Embed Size (px)
Citation preview

SGLT2 Inhibitors andCardiovascular Risk: LessonsLearned From the EMPA-REGOUTCOME StudyDiabetes Care 2016;39:717–725 | DOI: 10.2337/dc16-0041
Although cardiovascular (CV) mortality is the principal cause of death in individualswith type 2 diabetes (T2DM), reduction of plasma glucose concentration has littleeffect on CV disease (CVD) risk. Thus, novel strategies to reduce CVD risk in T2DMpatients are needed. The recently published BI 10773 (Empagliflozin) CardiovascularOutcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME)study demonstrated that in T2DMpatients with high CVD risk empagliflozin reducedthe primary major adverse cardiac event end point (CV death, nonfatal myocardialinfarction, nonfatal stroke) by 14%. This beneficial effect was driven by a 38%reduction in CV mortality with no significant decrease in nonfatal myocardialinfarction or stroke. Empagliflozin also caused a 35% reduction in hospitalization forheart failurewithout affecting hospitalization for unstable angina. Although sodium–
glucose cotransporter 2 inhibitors exert multiple metabolic benefits (decreases inHbA1c, body weight, and blood pressure and an increase in HDL cholesterol), all ofwhich could reduce CVD risk, it is unlikely that the reduction in CV mortality can beexplained by empagliflozin’s metabolic effects. More likely, hemodynamic effects,specifically reduced blood pressure and decreased extracellular volume, are respon-sible for the reduction in CV mortality and heart failure hospitalization. In thisPerspective, we will discuss possible mechanisms for these beneficial effects ofempagliflozin and their implications for the care of T2DM patients.
The BI 10773 (Empagliflozin) Cardiovascular Outcome Event Trial in Type 2 DiabetesMellitus Patients (EMPA-REG OUTCOME) study (1) provided evidence that empagliflozinreduces cardiovascular (CV) mortality and heart failure in high-risk patients with type 2diabetes (T2DM) with a previous CV event (myocardial infarction [MI], stroke, amputa-tion, multivessel coronary artery disease, or coronary artery bypass graft). Although theresults have important clinical implications for the care of T2DM patients, they raise anumber of questions with regard to 1) mechanism of action, 2) generalizability, and 3)class effect. In this Perspective,we discuss the results of the EMPA-REGOUTCOME study,their implications for the care of T2DM patients, and future directions.
CV RISK AND T2DM
T2DM individuals manifest a two- to threefold greater risk of CV events comparedwith counterparts without diabetes, and CV mortality is responsible for ;80% ofthe mortality (2). In T2DM patients without MI, risk of CV death is similar to indi-viduals without diabetes with prior MI (2). Although hyperglycemia is the principalrisk factor formicrovascular complications, it is a weak risk factor for CV disease (CVD),and interventional studies focused on reducing plasma glucose in T2DM have only a
1Division of Diabetes, University of Texas HealthScience Center at San Antonio, San Antonio, TX2Diabetes and Obesity Clinical Research Center,Department of Medicine, Hamad General Hospi-tal, Doha, Qatar3Department of Clinical and Experimental Med-icine, University of Pisa School of Medicine, Pisa,Italy4Division of Cardiology, University of TexasHealth Science Center at San Antonio and SouthTexas Veterans Health Care System, San Antonio,TX
Correspondingauthors:MuhammadAbdul-Ghani,[email protected], and Ralph A. DeFronzo,[email protected].
Received 8 January 2016 and accepted 24February 2016.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc16-0041/-/DC1.
© 2016 by the American Diabetes Association.Readersmayuse this article as longas thework isproperly cited, the use is educational and not forprofit, and the work is not altered.
Seeaccompanyingarticles, pp. 664, 668,677, 686, 694, 701, 709, 726, 735, and738.
Muhammad Abdul-Ghani,1,2
Stefano Del Prato,3 Robert Chilton,4
and Ralph A. DeFronzo1
Diabetes Care Volume 39, May 2016 717
CARDIOVASCULA
RDISEA
SEANDDIABETES
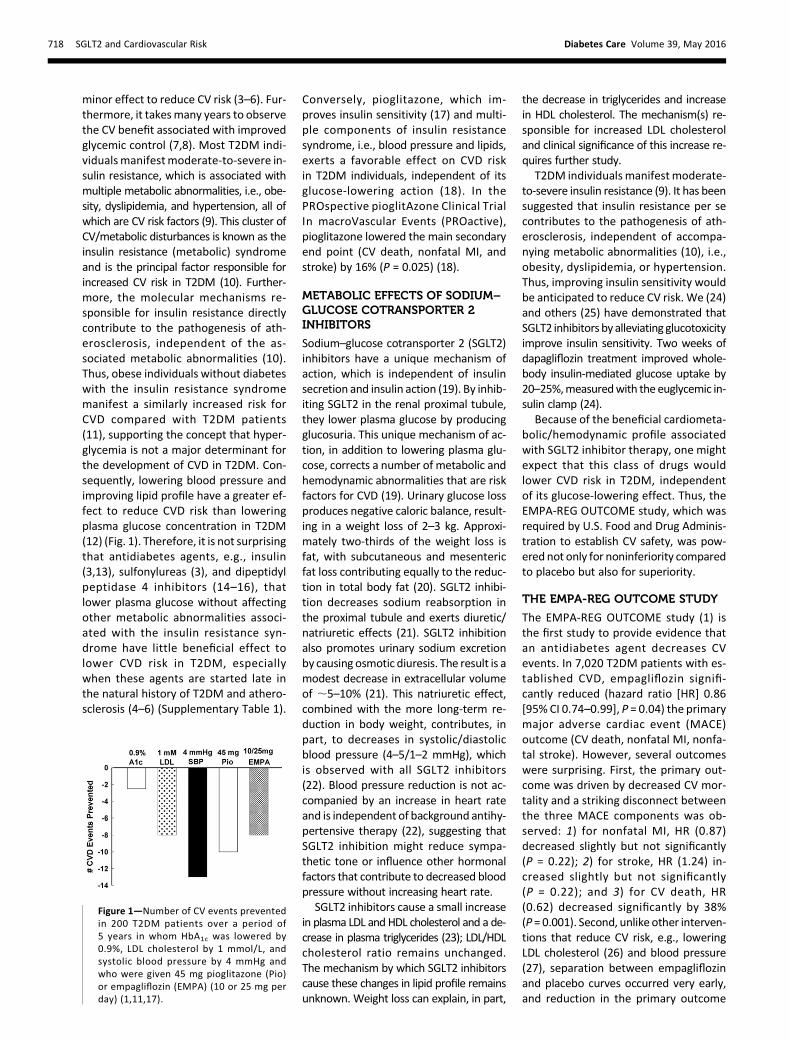
minor effect to reduce CV risk (3–6). Fur-thermore, it takesmany years to observethe CV benefit associated with improvedglycemic control (7,8). Most T2DM indi-vidualsmanifestmoderate-to-severe in-sulin resistance, which is associated withmultiple metabolic abnormalities, i.e., obe-sity, dyslipidemia, and hypertension, all ofwhich are CV risk factors (9). This cluster ofCV/metabolic disturbances is known as theinsulin resistance (metabolic) syndromeand is the principal factor responsible forincreased CV risk in T2DM (10). Further-more, the molecular mechanisms re-sponsible for insulin resistance directlycontribute to the pathogenesis of ath-erosclerosis, independent of the as-sociated metabolic abnormalities (10).Thus, obese individuals without diabeteswith the insulin resistance syndromemanifest a similarly increased risk forCVD compared with T2DM patients(11), supporting the concept that hyper-glycemia is not a major determinant forthe development of CVD in T2DM. Con-sequently, lowering blood pressure andimproving lipid profile have a greater ef-fect to reduce CVD risk than loweringplasma glucose concentration in T2DM(12) (Fig. 1). Therefore, it is not surprisingthat antidiabetes agents, e.g., insulin(3,13), sulfonylureas (3), and dipeptidylpeptidase 4 inhibitors (14–16), thatlower plasma glucose without affectingother metabolic abnormalities associ-ated with the insulin resistance syn-drome have little beneficial effect tolower CVD risk in T2DM, especiallywhen these agents are started late inthe natural history of T2DM and athero-sclerosis (4–6) (Supplementary Table 1).
Conversely, pioglitazone, which im-proves insulin sensitivity (17) and multi-ple components of insulin resistancesyndrome, i.e., blood pressure and lipids,exerts a favorable effect on CVD riskin T2DM individuals, independent of itsglucose-lowering action (18). In thePROspective pioglitAzone Clinical TrialIn macroVascular Events (PROactive),pioglitazone lowered the main secondaryend point (CV death, nonfatal MI, andstroke) by 16% (P = 0.025) (18).
METABOLIC EFFECTS OF SODIUM–
GLUCOSE COTRANSPORTER 2INHIBITORS
Sodium–glucose cotransporter 2 (SGLT2)inhibitors have a unique mechanism ofaction, which is independent of insulinsecretion and insulin action (19). By inhib-iting SGLT2 in the renal proximal tubule,they lower plasma glucose by producingglucosuria. This unique mechanism of ac-tion, in addition to lowering plasma glu-cose, corrects a number of metabolic andhemodynamic abnormalities that are riskfactors for CVD (19). Urinary glucose lossproduces negative caloric balance, result-ing in a weight loss of 2–3 kg. Approxi-mately two-thirds of the weight loss isfat, with subcutaneous and mesentericfat loss contributing equally to the reduc-tion in total body fat (20). SGLT2 inhibi-tion decreases sodium reabsorption inthe proximal tubule and exerts diuretic/natriuretic effects (21). SGLT2 inhibitionalso promotes urinary sodium excretionby causing osmotic diuresis. The result is amodest decrease in extracellular volumeof ;5–10% (21). This natriuretic effect,combined with the more long-term re-duction in body weight, contributes, inpart, to decreases in systolic/diastolicblood pressure (4–5/1–2 mmHg), whichis observed with all SGLT2 inhibitors(22). Blood pressure reduction is not ac-companied by an increase in heart rateand is independent of background antihy-pertensive therapy (22), suggesting thatSGLT2 inhibition might reduce sympa-thetic tone or influence other hormonalfactors that contribute to decreased bloodpressure without increasing heart rate.
SGLT2 inhibitors cause a small increasein plasma LDL and HDL cholesterol and a de-crease in plasma triglycerides (23); LDL/HDLcholesterol ratio remains unchanged.The mechanism by which SGLT2 inhibitorscause these changes in lipid profile remainsunknown. Weight loss can explain, in part,
the decrease in triglycerides and increasein HDL cholesterol. The mechanism(s) re-sponsible for increased LDL cholesteroland clinical significance of this increase re-quires further study.
T2DM individualsmanifestmoderate-to-severe insulin resistance (9). It has beensuggested that insulin resistance per secontributes to the pathogenesis of ath-erosclerosis, independent of accompa-nying metabolic abnormalities (10), i.e.,obesity, dyslipidemia, or hypertension.Thus, improving insulin sensitivity wouldbe anticipated to reduce CV risk. We (24)and others (25) have demonstrated thatSGLT2 inhibitors by alleviating glucotoxicityimprove insulin sensitivity. Two weeks ofdapagliflozin treatment improved whole-body insulin-mediated glucose uptake by20–25%,measuredwith the euglycemic in-sulin clamp (24).
Because of the beneficial cardiometa-bolic/hemodynamic profile associatedwith SGLT2 inhibitor therapy, one mightexpect that this class of drugs wouldlower CVD risk in T2DM, independentof its glucose-lowering effect. Thus, theEMPA-REG OUTCOME study, which wasrequired by U.S. Food and Drug Adminis-tration to establish CV safety, was pow-ered not only for noninferiority comparedto placebo but also for superiority.
THE EMPA-REG OUTCOME STUDY
The EMPA-REG OUTCOME study (1) isthe first study to provide evidence thatan antidiabetes agent decreases CVevents. In 7,020 T2DM patients with es-tablished CVD, empagliflozin signifi-cantly reduced (hazard ratio [HR] 0.86[95% CI 0.74–0.99], P = 0.04) the primarymajor adverse cardiac event (MACE)outcome (CV death, nonfatal MI, nonfa-tal stroke). However, several outcomeswere surprising. First, the primary out-come was driven by decreased CV mor-tality and a striking disconnect betweenthe three MACE components was ob-served: 1) for nonfatal MI, HR (0.87)decreased slightly but not significantly(P = 0.22); 2) for stroke, HR (1.24) in-creased slightly but not significantly(P = 0.22); and 3) for CV death, HR(0.62) decreased significantly by 38%(P = 0.001). Second, unlike other interven-tions that reduce CV risk, e.g., loweringLDL cholesterol (26) and blood pressure(27), separation between empagliflozinand placebo curves occurred very early,and reduction in the primary outcome
Figure 1—Number of CV events preventedin 200 T2DM patients over a period of5 years in whom HbA1c was lowered by0.9%, LDL cholesterol by 1 mmol/L, andsystolic blood pressure by 4 mmHg andwho were given 45 mg pioglitazone (Pio)or empagliflozin (EMPA) (10 or 25 mg perday) (1,11,17).
718 SGLT2 and Cardiovascular Risk Diabetes Care Volume 39, May 2016
was evident 3 months after starting em-pagliflozin. Third, the beneficial effect ofempagliflozin on mortality and hospitali-zation for heart failure widened progres-sively over the 3.1 years of treatment.Fourth, both empagliflozin doses (10and 25 mg) had a similar effect on out-come measures with no dose-responserelationship.
POSSIBLE MECHANISMS
Is It the Metabolic Actions ofEmpagliflozin?Inhibition of renal SGLT2 in T2DM exertsmultiple metabolic effects (e.g., reducedHbA1c, weight loss, increase in fat oxida-tion, and increase in glucagon secretion)that can affect cardiac function and po-tentially influence CV mortality. Reduc-tion in CV death without decrease in MIor stroke suggests that the beneficial ef-fect of empagliflozin is to improve sur-vival among patients experiencing a CVevent rather than to slow the atheroscle-rotic process and prevent atheroscleroticevents, i.e., MI and stroke. Reduction inCV death (5.9 to 3.6%, P , 0.001) wasobserved across all diagnostic categories(sudden death, 1.6 to 1.1%; worseningheart failure, 0.8 to 0.2%; acute MI, 0.5to 0.3%; stroke, 0.5 to 0.3%; other CVdeath, 2.4 to 1.6%). The latter categoryincludes deaths not explained by otherknown causes. The majority of suchcases result from acute MI and arrhyth-mias, and this category is not as diagnos-tically sound as the others. Empagliflozinfailed to reduce hospitalization from un-stable angina (HR 0.97, P = 0.97). Becauseof 1) the lack of beneficial effect of empa-gliflozin on nonfatal stroke and nonfatalMI, 2) the absence of reduction in unsta-ble angina, and 3) the rapidity of onset ofdecrease in CV mortality, it is highly un-likely that the decrease in MACE outcomein the EMPA-REG OUTCOME study resultsfrom slowing the atherosclerotic processby empagliflozin (Fig. 2).
Glycemic Control
It is unlikely that empagliflozin reducedmortality in the EMPA-REG OUTCOMEstudy by improving glucose control.First, hyperglycemia is weak risk factorfor CVD (12). Intensive glycemic controlfailed to decrease CV events in the UKProspective Diabetes Study (UKPDS) (3),Action to Control Cardiovascular Risk inDiabetes (ACCORD) study (4), Action inDiabetes and Vascular Disease: Preterax
and Diamicron MR Controlled Evalua-tion (ADVANCE) study (5), and VeteransAffairs Diabetes Trial (VADT) (6). Sec-ond, the difference in HbA1c betweenempagliflozin and placebo groups wasmodest: 0.45% at 90 weeks and 0.28%at 204 weeks. Third, it took;10 years inUKPDS (7) and VADT (8) to demonstrate asmall (;10%), though significant, reduc-tion in CV events by tight glycemic con-trol, while the effect of empagliflozin onCVmortality was evident at 3months andwell established at 6 months.
Shift in Fuel Metabolism
SGLT2 inhibitors shift whole-body metab-olism fromglucose to fat oxidation (24,25)(Fig. 3). Two and 4 weeks of treatmentwith dapagliflozin and empagliflozin, re-spectively, reduced the respiratory quo-tient (RQ) during fasting state, indicatinga decrease in glucose oxidation and in-crease in fatoxidation.Dapagliflozin causeda 14% increase in fat oxidation and 20%reduction in glucose oxidation (24). Duringa mixed meal, glucose oxidation decreased
by 60% and fat oxidation increased by 20%after 4weeks of empagliflozin. Because theamount of oxygen required to generate thesame amount of ATP is greater with fatcompared with glucose (28), the shiftfrom glucose to fat oxidation would in-crease myocardial oxygen demand, andthis would be expected toworsenmyocar-dial ischemia in T2DM patients. Thus, in-creasedmyocardial fat oxidation causedbyempagliflozin in the EMPA-REGOUTCOMEstudy cannot explain the reduction in CVmortality caused by the drug.
Ketones
SGLT2 inhibitors cause a shift from glu-cose to fat oxidation and the end prod-uct of fatty acid oxidation is acetyl CoA,which either can enter the tricarboxylicacid cycle or be converted to ketones,the latter being favored by the SGLT2inhibitor–induced stimulation of glucagonsecretion (24,25) (Fig. 3). The rise inplasma ketone concentration is small(0.3–0.6 meq/L) (24,25). Like free fatty
acids, the amount of oxygen required
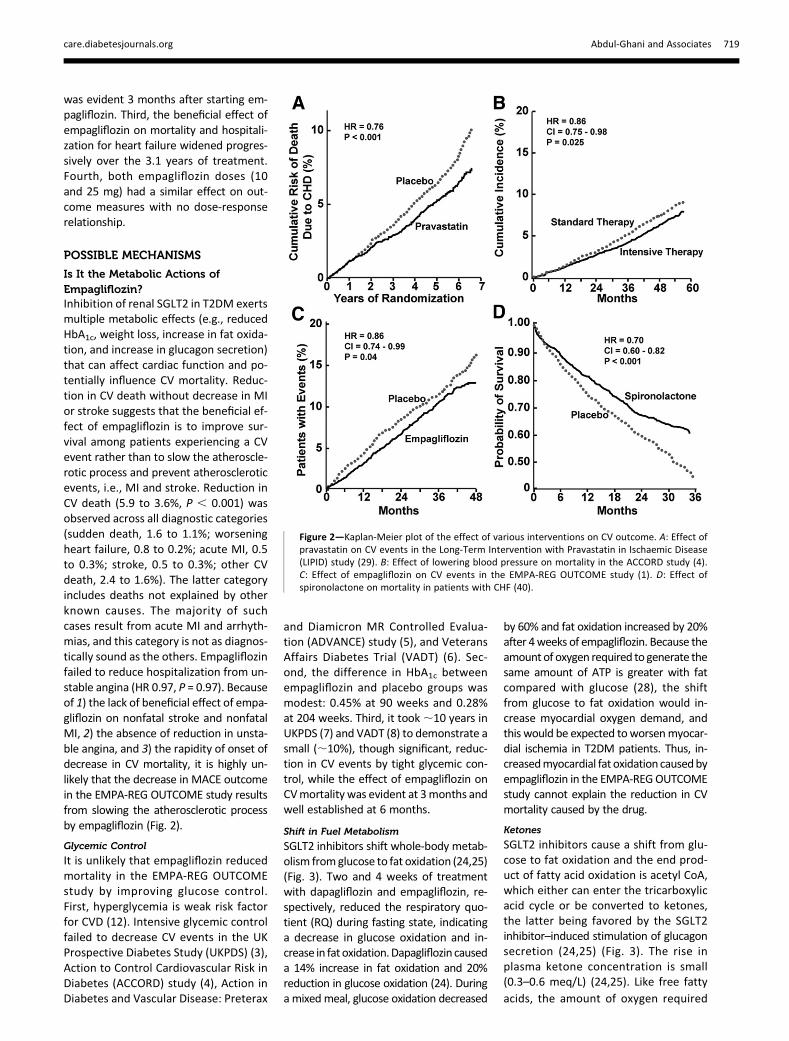
Figure 2—Kaplan-Meier plot of the effect of various interventions on CV outcome. A: Effect ofpravastatin on CV events in the Long-Term Intervention with Pravastatin in Ischaemic Disease(LIPID) study (29). B: Effect of lowering blood pressure on mortality in the ACCORD study (4).C: Effect of empagliflozin on CV events in the EMPA-REG OUTCOME study (1). D: Effect ofspironolactone on mortality in patients with CHF (40).
care.diabetesjournals.org Abdul-Ghani and Associates 719

to generate the same amount of ATP isgreater with ketones compared with glu-cose. However, the heart avidly extractsand consumes ketone bodies and ketonebody oxidation may improve cardiacmuscle efficiency (reviewed in 29). Fur-ther studies will be required to examinewhether the preferential oxidation of ke-tones by the heart (29) provides an ener-getic benefit to the failing myocardium.
Uric Acid
SGLT2 inhibitors promote uric acid excre-tion and reduce the plasma uric acid con-centration by ;0.7% mg/dL (Fig. 3).Increased uric acid levels long have beenassociated with increased CVD (30), but acausal link remains controversial. How-ever, accumulating evidence in both hu-mans and animals indicates that elevatedplasmauric acid levels can cause hyperten-sion, vascular damage, and impaired renalfunction (reviewed in 31). Although un-likely to explain the early reduction in CVmortality, the potential benefits of uricacid reduction to reduce blood pressureand prevent vascular damage may play arole in the progressive late separation inthemortality curves between empagliflozinand placebo. The reduction in plasma uricacid concentration also may contribute to
the impressive slowing of diabetic nephrop-
athy observed in the EMPA-REGOUTCOME
study.
Glucagon
SGLT2 is expressed in pancreatic a-cellsand plays an important role in regulating
glucagon secretion (32). Dapagliflozin
(24) and empagliflozin (25) cause a ro-
bust increase in plasma glucagon in
T2DM patients (Fig. 3). In experimental
animals, glucagon receptor activation
exerts a detrimental effect on myocar-
dial function (33), and glucagon infusion
in humans has no effect on left ventric-
ular (LV) function (34). Thus, it is unlikely
that an increase in plasma glucagon con-
tributed to reduced CV mortality or hospi-
talization for heart failure by empagliflozin.
Weight Loss
Glucosuria, produced by SGLT2 inhibitors,causes caloric loss and a decrease in body
weight. In the EMPA-REG OUTCOME
study, empagliflozin-treated subjects
lost;2 kg. Althoughpossible, it is unlikely
that this small amount of weight loss con-
tributed to the reduction in CV mortality
that was observed within 2–3 months af-
ter the start of empagliflozin.
Is It a Direct Effect of the Drug?Although SGLT2 is not expressed in car-diac myocytes, SGLT1 is present in myo-cardial tissue. Therefore, partial SGLT1inhibition by empagliflozin could affectcardiac function. However, half-maximaleffective concentration for SGLT1 inhibi-tion by empagliflozin is 8.3mmol/L, whichis ;2,600-fold greater than for SGLT2,and the peak plasma empagliflozin con-centration following the administrationof 10 and 25 mg/day doses is ;500and ;800 nmol/L. Moreover, most ofthe circulating drug is bound to plasmaproteins and free drug concentration ismuch lower. Therefore, the expectedplasma-free empagliflozin concentrationin the EMPA-REG OUTCOME study wouldbe very low, and it is very unlikely that thelow circulating free empagliflozin levelcould have any effect on SGLT1 function.Further, if SGLT1 were inhibited by empa-gliflozin, myocardial function would beexpected to decline, not improve. Con-sistent with this, SGLT1 inhibition byphlorizin (dual SGLT1/2 inhibitor) in ex-perimental animals exerts a detrimentaleffect on LV function (35). We are un-aware of any study that demonstratesthat empagliflozin has a direct beneficialeffect on the heart, unrelated to an effecton the SGLT2/SGLT1 transporters, al-though such an effect cannot be ex-cluded. In summary, direct myocardialeffects by empagliflozin are unlikely toexplain the beneficial effect of the drugon CV mortality.
Is It Change in Plasma ElectrolyteConcentration and/or Distribution?SGLT2 inhibition produces negative so-dium balance in the first 2–3 days afterstarting the drug without a change inplasma sodium concentration. Whatremains to be established is whether so-dium redistribution between the intra-and extracellular compartments mayhave occurred as a result of the natri-uretic effect of the drug. In animalmodelsof heart failure, an increase in intracellu-lar sodium has been reported. Preclinicalstudies also have reported heart tissueremodeling after the administration ofSGLT2 inhibitors in association with amarked reduction of interstitial fibrosis(36). The latter, however, requires timeand is unlikely to explain the early devia-tion of curves for CV mortality and heartfailure hospitalization.
Figure 3—Schematic representation of the possible metabolic and hemodynamic mechanismsvia which empagliflozin reduced mortality and hospitalization for heart failure in the EMPA-REGOUTCOME study. Because of the rapidity of onset of these beneficial effects and the known CVbenefits of blood pressure and volume reduction from previous trials with antihypertensiveagents and diuretics, it is likely that the hemodynamic and volume-depleting actions play apivotal role in the cardioprotective effects of empagliflozin. It seems less likely that the meta-bolic/hormonal effects (shift from glucose to fat/ketone oxidation, reduced plasma uric acidconcentration, weight loss, increased glucagon secretion, increased angiotensin [Ang] 1-7, andAT2 receptor activation) of empagliflozin therapy could play a role in the drug’s cardioprotectiveeffects (see text for a more detailed explanation). ECFV, extracellular fluid volume.
720 SGLT2 and Cardiovascular Risk Diabetes Care Volume 39, May 2016

A small increase in plasma potassiumconcentration has been observed withsome SGLT2 inhibitors, and hyperkale-mia can cause arrhythmias. However,this would increase, not decrease, CVmortality.No consistent changes inplasmachloride, bicarbonate, or calcium concen-trations have been reported with SGLT2inhibitors.Small increases in serum phosphate
(3–5%) and magnesium (7–9%) havebeen reported with SGLT2 inhibitors. Itis unlikely that such a small increase inserum phosphate could affect myocar-dial function, and serum magnesiumcorrelates poorly with tissue magne-sium levels.
Is It the Blood Pressure?Although most participants in the EMPA-REG OUTCOME study were hypertensiveand .90% received antihypertensivetherapy, starting blood pressure waswell controlled (135/77 mmHg). The de-crease in systolic/diastolic blood pressurein the EMPA-REG OUTCOME study was;5/2 mmHg, and was maintainedthroughout the 3.1-year study duration.Such a decrease in blood pressure couldcontribute to the reduction in CV eventsin the EMPA-REG OUTCOME study. How-ever, in studies that examined the effectof blood pressure reduction on CV events,the decrease became evident only after 1year (27,37) (Fig. 2). Moreover, loweringblood pressure generally has a greater im-pact on stroke reduction than on othercardiac events (27,37). In the EMPA-REGOUTCOME study there was a small, albeitnonsignificant, increase in nonfatal stroke.Thus, it is unlikely that the decrease in CVevents in empagliflozin-treated individu-als can beexplained solely by thedecreasein brachial artery blood pressure. How-ever, reduction in brachial artery bloodpressure may underestimate central aor-tic pressure and provides no informationabout aortic stiffness, both of which areindependent predictors of CV mortalityand LV function (38,39). Results from theConduit Artery Function Evaluation (CAFE)study (40) demonstrated that, despitesimilar brachial arterial blood pressures,subjects with hypertension and treatedwith amlodipine/perindopril had signifi-cantly lower central aortic blood pressurethan the group treated with atenolol/thiazide. Further, reduction in central aor-tic blood pressure was strongly associatedwith reduced CV events in a post hoc
analysis of 2,073 participants. If empagli-flozin caused a greater decrease in centralaortic pressure than evident by the de-crease in brachial artery blood pressureand reduced aortic stiffness, it couldhave greater impact on cardiac eventsandheart failure thanonstroke.Consistentwith this hypothesis, empagliflozin hasbeen shown to reduce aortic stiffness insubjects with diabetes, possibly by reduc-ing oxidative stress or suppressing inflam-mation (41). Changes in nitric oxide andsystemic renin-angiotensin-aldosteronesystem activity were unrelated to thedecline in aortic stiffness followingempagliflozin therapy (37). Further, thediuretic effect of empagliflozin and theaccompanying decrease in intravascularvolume could further decrease centralaortic pressure and produce an afterloadreduction effect that improves LV func-tion, reduces cardiac workload, anddecreases myocardial oxygen demand(Fig. 3). These hemodynamic effects ofempagliflozin would be expected to re-duce cardiac events, particularly in sub-jects with ischemic heart disease,impaired LV function, and congestiveheart failure (CHF). Consistent with thisscenario, participants with history ofheart disease benefitedmost from empa-gliflozin treatment. The HR for 3-pointMACE was 0.83 (95% CI 0.68–1.04) forpatients with history of coronary heartdisease only, 0.94 (0.47–1.88) for patientswith peripheral vascular disease only, and1.15 (0.74–1.78) for patients with strokeonly. Thus, it is possible that these hemo-dynamic effects of empagliflozin contrib-uted to its beneficial CV effect, particularlyin subjects with reduced LV function andCHF. Unfortunately, no information onbaseline LV function or change in LV func-tion in response to therapy is availablefrom the EMPA-REG OUTCOME study. Fu-ture studies examining the impact ofSGLT2 inhibitors on central aortic and bra-chial artery blood pressure, aortic stiff-ness, and LV function will add insightabout this hypothesis. Such hemodynamiceffects of empagliflozin also could explainlack of relationship between empagliflozindose and CV outcomes. As empagliflozin10 mg produces near-maximal glucosuric,natriuretic, and blood pressure–loweringeffects, the beneficial CV effect of 10 and25 mg doses would be expected to besimilar (42). Last, empagliflozin caused a5/2 mmHg decrease in systolic/diastolicblood pressure without any increase in
heart rate. This is consistent with the ac-tion of the drug to reduce sympathetictone, which could have favorable effectson CVmortality. However, previous studiesfrom our laboratory (24) suggest that theincrease in endogenous (hepatic) glucoseproduction observed with SGLT2 inhibi-tors is mediated by the stimulation of therenal sympathetic nerves. If this was asso-ciated with a generalized activation of thesympathetic nervous system, one wouldexpect heart rate to increase, not de-crease, as was observed in the EMPA-REG OUTCOME study. Further studies areneeded to examine the effect of SGLT2inhibitor therapy on the sympathetic ner-vous system.
Empagliflozin reduced hospitalizationfrom CHF by 35%. Thus, it is possiblethat empagliflozin reduced CV mortalityby improving survival specifically amongpatients with compromised LV functionand/or clinically symptomatic CHF. A re-cent subanalysis showed that empagli-flozin similarly reduced CV mortality insubjects with and without heart failureat time of entry into the EMPA-REGOUTCOME study. However, diagnosisof heart failure at baseline was basedon self-reporting rather than on mea-sured LV function. Further, subjectswho did not report a history of heartfailure and developed heart failure dur-ing the study were placed in the cate-gory without heart failure. Because thediagnosis of heart failure at baseline wasbased on self-reporting, it is possibledinfact likelydthat many individuals whodeveloped heart failure during the studyactually had heart failure at baseline and,thus, were misclassified. Last, the reduc-tion in CV mortality became evidentshortly after starting therapy. This timecourse is reminiscent of the effect of spi-ronolactone on survival in subjects withCHF (43) (Fig. 2). It is possible that theentire benefit of empagliflozin onCVmor-tality occurs secondary to the drug’sunique action to simultaneously reduceboth preload (reduction of plasma vol-ume) and afterload (improved bloodpressure and aortic stiffness) in patientswith reduced LV function and heart fail-ure (Fig. 3). Measurement of B-type na-triuretic peptide could have added insightabout this hypothesis and been helpful inidentifying this high-risk population. Ex-ploring this possibility not only wouldimprove our understanding of the mech-anism(s) by which empagliflozin reduces
care.diabetesjournals.org Abdul-Ghani and Associates 721

CV mortality but also would identify asubgroup of patients with diabetesand existing heart failure who wouldbenefit most from SGLT2 inhibitortreatment.Reduction in the intravascular volume
by empagliflozin could lead to activationof the renin-angiotensin-aldosteronesystem, leading to an exacerbation ofthe underlying CVD by stimulating thetype 1 angiotensin (AT1) receptor (44).However, 81% of patients with diabetesin the EMPA-REG OUTCOME study werereceiving ACE inhibitors or angiotensinreceptor blockers. This would favoractivation of the AT2 receptor and angio-tensin 1-7 pathway, resulting in vasodila-tion; antiproliferation; antihypertrophy;antiarrhythmic, anti-inflammatory, posi-tive inotropic effects; and reduction inmicroalbuminuria (45) (Fig. 3).Microalbu-minuria is a known risk factor for CVD,although a direct causal association hasyet to be established.
Does Empagliflozin Have an Effectto Slow Atherosclerosis?Empagliflozin-treated subjects experi-enced ;2 kg weight loss, 2 mg/dL in-crease in HDL cholesterol, and 5 mmHgdecrease in systolic blood pressurecompared with placebo-treated sub-jects. These benefits would be ex-pected to slow the atheroscleroticprocess and reduce nonfatal CV events.However, nonfatal CV events (MI andstroke)werenot affectedbyempagliflozin.It is possible that the study durationwas too short to observe the impactof these metabolic/hemodynamic ef-fects on atherosclerosis-related eventsor that the antiatherosclerotic effectof empagliflozin may have been ob-scured by the advanced atheroscleroticcondition of the participants. It is alsopossible that the increase in plasmaLDL, although small, negated somebeneficial effect of empagliflozin onCV risk factors. Last, there was an11% and 7% increase in insulin and sul-fonylurea use in the placebo group.These agents are associated withweight gain and adverse CV outcomes(8,46). It is possible that, in part, sep-aration in MACE outcome curvesbetween empagliflozin-treated andplacebo-treated patients is explainedby a detrimental impact of the hypogly-cemic agents used in the placebogroup.
Is There a Place for CombinationTherapy With Pioglitazone?Metformin long has been considered toexert some CV protection. Such an ef-fect, however, is based primarily on asmall group (n = 342) of obese T2DMpatients in the UKPDS. Pioglitazone isthe only other antidiabetes agent shownto lower CV events in T2DM (18). In thePROactive study, pioglitazone reducedthe main secondary end point, MACE,by 16% (HR 0.84 [95% CI 0.72–0.98],P = 0.027), although the primary endpoint (MACE plus peripheral vascular dis-ease) did not reach statistical signifi-cance due to an increase in the numberof leg revascularizations. Of note, eachcomponent of the MACE end point de-creased significantly with pioglitazone(death from 4.63 to 4.22%, MI from4.48 to 4.00%, and stroke from 3.64 to2.91%). Of particular note, recurrentstroke (HR 0.53, P = 0.008) and recurrentMI (HR 0.72, P = 0.045), which were notreduced in the EMPA-REG OUTCOMEstudy, were markedly decreased inPROactive study (47,48). In addition, pio-glitazone does not exert any negativeeffect on LV function and improves di-astolic dysfunction (49), improves thelipid profile (17), reduces blood pressure(afterload) (50), improves endothelialdysfunction, and slows atherosclerosis(51–53). Thus, it is possible that combinedpioglitazone/empagliflozin therapy wouldexert an additive, even synergistic, effectto reduce afterload and to improve CVevents. One could argue that fluid reten-tion with pioglitazone could offset someof the beneficial hemodynamic effects ofempagliflozin. Fluid retention with pio-glitazone is related to the drug’s sodiumretentive effect on the kidney; however,despite increased salt/water retention,pioglitazone significantly decreasedsystolic blood pressure (18,50). In thePROactive study, the incidence of “heartfailure” in pioglitazone-treated subjectswas increased; nonetheless, overall mor-tality and CV events in this group de-creased compared with the placebogroup, although the decrease was notas great as in pioglitazone-treated indi-viduals who did not experience “heartfailure” while on the thiazolidinedione(18). Thus, salt/water retention withpioglitazone does not negate the drug’sbeneficial CV effects in patients withheart failure. In a recent study involving3,876 patients with a recent stroke or
transient ischemic attack, pioglitazonereduced the primary outcome of fatalor nonfatal stroke and MI by 26% (P ,0.001) (54). Of note, there was no in-crease in the incidence of heart failurein pioglitazone-treated individuals in thishigh-risk population in this study (54).Given the natriuretic effect of SGLT2 in-hibitors, one might expect minimal fluidretention with combined pioglitazone/SGLT2 inhibitor therapy, especially if lowpioglitazone doses (15–30 mg/day) areused.
Is It a Class Effect?There are no significant differences inglucose lowering, body weight loss,and blood pressure reduction amongthe individual SGLT2 inhibitors. Usingthe Archimedes model, it has been pre-dicted that, over a period of 20 years,patients with diabetes treated with da-pagliflozin would experience a relativereduction of MI, stroke, CV death, andall-cause death (55). However, onlywell-designed CV intervention trialswill provide a true answer to the ques-tion. The CANagliflozin cardioVascularAssessment Study (CANVAS) andDECLAREstudy, which examine the effectof canagliflozin and dapagliflozin, re-spectively, on CV outcomes, may helpclarify whether the effect of empagliflo-zin to reduce CV events is a class effector represents a specific pharmacologicaleffect of empagliflozin. It is impossible atthis time to determine whether otherSGLT2 inhibitors will exert similar re-ductions in CV death and CHF hospitali-zation. Populations with diabetes inCANVAS and DECLARE differ signifi-cantly from those in the EMPA-REGOUTCOME study. Approximately 60–70% of patients in CANVAS and ;40%in DECLARE had a prior CV event and theremaining participants qualified basedon CV risk factor profile. Moreover, thesample size (4,339 patients) in CANVAS(56) is relatively small compared withthe EMPA-REG OUTCOME study. Asthe beneficial CV effects of empagliflo-zin most likely are mediated via its he-modynamic/volume depletion actions,one might expect other members ofthis class to have similar beneficial ef-fects on CV events. However, becauseof different selection criteria in CANVASand DECLARE, it is possible that a ben-eficial effect of canagliflozin and dapa-gliflozin to reduce CV mortality and CHF
722 SGLT2 and Cardiovascular Risk Diabetes Care Volume 39, May 2016

may not be observed even though thebeneficial hemodynamic (and meta-bolic) effects of all three SGLT2 inhibi-tors are similar.
WHAT IS THE IMPACT OF THEEMPA-REG OUTCOME STUDY ONPATIENT CARE?
The EMPA-REG OUTCOME study resultsdemonstrate that the addition of empa-gliflozin to the antidiabetes treatmentregimen in high-risk T2DM patientswith established CVD reduces CV mor-tality by 38%. We believe that such adramatic effect on CV mortality justifiesinclusion of empagliflozin in treatmentregimen of T2DM patients with similarclinical characteristics to those in theEMPA-REG OUTCOME study, i.e., withestablished CVD. If such a high-risk T2DMpatient is on another SGLT2 inhibitor,evidence-basedmedicinedictates a switchto empagliflozin. In T2DM patients whoare earlier in the natural history of thedisease and do not have well-establishedCVD, there are no data to support the useof one SGLT2 inhibitor over another. Cur-rently, there are no data that any of thethree SGLT2 inhibitors approved in theU.S. will have a CV protective effect inthis T2DM population without clinicallyevident CVD. Therefore, the physicianshould feel comfortable using any ofthe three SGLT2 inhibitors in patientswith diabetes without advanced cardiacdisease. All three SGLT2 inhibitors
similarly reduce HbA1c, blood pressure,and body weight and have a good safetyprofile.
WHAT IS NEXT?
As the results of the EMPA-REGOUTCOMEstudy suggest that the beneficial effectof empagliflozin to lower CV mortality inT2DM patients most likely results fromits hemodynamic rather than its meta-bolic effects, it is intriguing to examinethe impact of the drug specifically in sub-jects with and without diabetes with re-duced LV function (e.g., post-MI) and insubjects with existing CHF (Table 1). Wepostulate that the beneficial effect ofempagliflozin on CV mortality and CHFhospitalization in these patient popula-tions is likely to be quite robust. Addi-tional studies to examine this possibilityare indicated.
Funding. M.A.-G. receives grant support fromthe Qatar Foundation (NPRP 4-248-3-076). M.A.-G.(R01 DK097554-01) and R.A.D. (5R01DK24093)have received grant support from the NationalInstitutes ofHealth. The salaryof R.A.D. is partiallysupported by the South Texas Veterans HealthCare System.Duality of Interest. S.D.P. is on advisory panelsfor AstraZeneca, Boehringer Ingelheim, Eli Lillyand Co., GlaxoSmithKline, Hanmi Pharmaceuti-cals, Intarcia, Janssen, Merck & Co., NovartisPharmaceuticals, Novo Nordisk, Sanofi, andTakeda and has research support fromMerck & Co.and Novo Nordisk. R.C. is an advisory boardmember for Pfizer, Boehringer Ingelheim,
AstraZeneca, Boston Scientific, Merck Sharp &Dohme, and Takeda. R.A.D. is an advisory boardmember for AstraZeneca, Novo Nordisk, Jans-sen, Boehringer Ingelheim, and Intarcia; is onthe speaker’s bureau for AstraZeneca and NovoNordisk; and has grants from AstraZeneca, Jans-sen, and Boehringer Ingelheim. No other poten-tial conflicts of interest relevant to this articlewere reported.
References1. Zinman B,Wanner C, Lachin JM, et al.; EMPA-REG OUTCOME Investigators. Empagliflozin,cardiovascular outcomes, and mortality in type2 diabetes. N Engl J Med 2015;373:2117–21282. Di Angelantonio E, Kaptoge S, Wormser D,et al.; Emerging Risk Factors Collaboration. As-sociation of cardiometabolic multimorbiditywith mortality. JAMA 2015;314:52–603. UK Prospective Diabetes Study (UKPDS)Group. Intensive blood-glucose control with sul-phonylureas or insulin compared with conven-tional treatment and risk of complications inpatients with type 2 diabetes (UKPDS 33). Lan-cet 1998;352:837–8534. Gerstein HC, Miller ME, Byington RP, et al.;Action to Control Cardiovascular Risk in Diabe-tes Study Group. Effects of intensive glucoselowering in type 2 diabetes. N Engl J Med2008;358:2545–25595. Patel A, MacMahon S, Chalmers J, et al.;ADVANCE Collaborative Group. Intensive bloodglucose control and vascular outcomes in patientswith type 2 diabetes. N Engl J Med 2008;358:2560–25726. Duckworth W, Abraira C, Moritz T, et al.;VADT Investigators. Glucose control and vascu-lar complications in veterans with type 2 diabe-tes. N Engl J Med 2009;360:129–1397. Holman RR, Paul SK, Bethel MA, MatthewsDR, Neil HA. 10-year follow-up of intensive glu-cose control in type 2 diabetes. N Engl J Med2008;359:1577–1589
Table 1—Possible mechanisms that could contribute to the reduction of CV mortality by empagliflozin in the EMPA-REGOUTCOME study
Effect Likelihood Reason
Metabolic actionsLowered plasma glucose concentration Unlikely Hyperglycemia is a weak CV risk factor; benefit of HbA1c
reduction on CVD takes ;10 years to observeIncreased fax oxidation Unlikely Increased oxygen demand per ATP generatedIncreased plasma ketone concentration Unlikely Increased oxygen demand per ATP generatedIncreased plasma uric acid concentration Unlikely Causal association with CVD not establishedIncreased plasma glucagon concentration Unlikely Physiological increase in glucagon has no effect on CV functionWeight loss Unlikely Weight loss is modest but may contribute to long-term
reduction in blood pressureChange in plasma electrolyte concentration Unlikely No consistent changes observed
Hemodynamic actionsDecrease in blood pressure Likely Rapid reduction in blood pressure correlates with early CV
benefit; proven CV protection in prior studiesDiuretic effect and decrease in extracellular fluid volume Likely Rapid reduction in extracellular fluid volume correlates
with early CV benefit; proven protection against CHF inprior studies
Impaired arterial elasticity Possible Arterial stiffness is a CV risk factor; empagliflozin reducesarterial stiffness
Direct effect on the myocardium Unlikely No evidenceDecreased sympathetic tone Possible No increase in heart rate despite decrease in blood pressure
and extracellular fluid volume
care.diabetesjournals.org Abdul-Ghani and Associates 723

8. Hayward RA, Reaven PD, Wiitala WL, et al.;VADT Investigators. Follow-up of glycemiccontrol and cardiovascular outcomes in type2 diabetes. N Engl J Med 2015;372:2197–22069. DeFronzo RA. Insulin resistance: a multifac-eted syndrome responsible for NIDDM, obesity,hypertension, dyslipidaemia and atherosclero-sis. Neth J Med 1997;50:191–19710. DeFronzo RA. Insulin resistance, lipotoxic-ity, type 2 diabetes and atherosclerosis: themissing links. The Claude Bernard Lecture2009. Diabetologia 2010;53:1270–128711. Obunai K, Jani S, Dangas GD. Cardiovascu-lar morbidity and mortality of the metabolicsyndrome. Med Clin North Am 2007;91:1169–118412. Sattar N. Revisiting the links between gly-caemia, diabetes and cardiovascular disease. Di-abetologia 2013;56:686–69513. Gerstein HC, Bosch J, Dagenais GR, et al.;ORIGIN Trial Investigators. Basal insulin and car-diovascular and other outcomes in dysglycemia.N Engl J Med 2012;367:319–32814. Scirica BM, Bhatt DL, Braunwald E, et al.;SAVOR-TIMI 53 Steering Committee and Inves-tigators. Saxagliptin and cardiovascular out-comes in patients with type 2 diabetesmellitus. N Engl J Med 2013;369:1317–132615. White WB, Cannon CP, Heller SR, et al.;EXAMINE Investigators. Alogliptin after acutecoronary syndrome in patients with type 2 dia-betes. N Engl J Med 2013;369:1327–133516. Green JB, Bethel MA, Armstrong PW, et al.;TECOS Study Group. Effect of sitagliptin on car-diovascular outcomes in type 2 diabetes. N EnglJ Med 2015;373:232–24217. Miyazaki Y, Mahankali A, Matsuda M, et al.Improved glycemic control and enhanced insu-lin sensitivity in type 2 diabetic subjects treatedwith pioglitazone. Diabetes Care 2001;24:710–71918. Dormandy JA, Charbonnel B, Eckland DJ,et al.; PROactive Investigators. Secondary pre-vention of macrovascular events in patientswith type 2 diabetes in the PROactive Study(PROspective pioglitAzone Clinical Trial In mac-roVascular Events): a randomised controlled tri-al. Lancet 2005;366:1279–128919. Abdul-Ghani MA, Norton L, Defronzo RA.Role of sodium-glucose cotransporter 2 (SGLT 2)inhibitors in the treatment of type 2 diabetes.Endocr Rev 2011;32:515–53120. Bolinder J, Ljunggren O, Kullberg J, et al.Effects of dapagliflozin on body weight, totalfat mass, and regional adipose tissue distribu-tion in patients with type 2 diabetes mellituswith inadequate glycemic control on metfor-min. J Clin Endocrinol Metab 2012;97:1020–103121. Lambers Heerspink HJ, de Zeeuw D, Wie L,Leslie B, List J. Dapagliflozin a glucose-regulatingdrug with diuretic properties in subjects withtype 2 diabetes. Diabetes Obes Metab 2013;15:853–86222. Abdul-Ghani MA, Norton L, DeFronzo RA.Renal sodium-glucose cotransporter inhibitionin themanagement of type 2 diabetes mellitus.Am J Physiol Renal Physiol 2015;309:F889–F90023. Sinclair A, Bode B, Harris S, et al. Efficacyand safety of canagliflozin compared with
placebo in older patients with type 2 diabetesmellitus: a pooled analysis of clinical studies.BMC Endocr Disord 2014;14:3724. Merovci A, Solis-Herrera C, Daniele G, et al.Dapagliflozin improves muscle insulin sensitiv-ity but enhances endogenous glucose produc-tion. J Clin Invest 2014;124:509–51425. Ferrannini E, Muscelli E, Frascerra S, et al.Metabolic response to sodium-glucose cotrans-porter 2 inhibition in type 2 diabetic patients.J Clin Invest 2014;124:499–50826. The Long-Term Intervention with Prava-statin in Ischaemic Disease (LIPID) Study Group.Prevention of cardiovascular events and deathwith pravastatin in patients with coronary heartdisease and a broad range of initial cholesterollevels. N Engl J Med 1998;339:1349–135727. Patel A, MacMahon S, Chalmers J, et al.;ADVANCE Collaborative Group. Effects of a fixedcombination of perindopril and indapamide onmacrovascular and microvascular outcomes inpatients with type 2 diabetes mellitus (theADVANCE trial): a randomised controlled trial.Lancet 2007;370:829–84028. Ferrannini E. The theoretical bases of indi-rect calorimetry: a review.Metabolism 1988;37:287–30129. Cotter DG, Schugar RC, Crawford PA. Ke-tone body metabolism and cardiovascular dis-ease. Am J Physiol Heart Circ Physiol 2013;304:H1060–H107630. OddenMC,AmaduAR, Smit E, Lo L, Peralta CA.Uric acid levels, kidney function, and cardiovascularmortality in US adults: National Health and Nutri-tion Examination Survey (NHANES) 1988-1994 and1999-2002. Am J Kidney Dis 2014;64:550–55731. Feig DI, Kang DH, Johnson RJ. Uric acid andcardiovascular risk. N Engl J Med 2008;359:1811–182132. Bonner C, Kerr-Conte J, Gmyr V, et al. In-hibition of the glucose transporter SGLT2 withdapagliflozin in pancreatic alpha cells triggersglucagon secretion. Nat Med 2015;21:512–51733. Ali S,Ussher JR, Baggio LL, et al. Cardiomyocyteglucagon receptor signaling modulates outcomesin mice with experimental myocardial infarction.Mol Metab 2015;4:132–14334. Thuesen L, Christiansen JS, Sørensen KE,Orskov H, Henningsen P. Low-dose intravenousglucagon has no effect on myocardial contrac-tility in normal man. An echocardiographicstudy. Scand J Clin Lab Invest 1988;48:71–7535. Kashiwagi Y, Nagoshi T, Yoshino T, et al. Ex-pression of SGLT1 in human hearts and impair-ment of cardiac glucose uptake by phlorizinduring ischemia-reperfusion injury in mice. PLoSOne 2015;10:e013060536. Levelt E, Mahmod M, Piechnik SK, et al. Re-lationship between left ventricular structuraland metabolic remodeling in type 2 diabetes.Diabetes 2016;65:44–5237. Xie X, Atkins E, Lv J, et al. Effects of intensiveblood pressure lowering on cardiovascular andrenal outcomes: updated systematic review andmeta-analysis. Lancet 2016;387:435–44338. Cruickshank K, Riste L, Anderson SG, WrightJS, Dunn G, Gosling RG. Aortic pulse-wavevelocity and its relationship to mortality in di-abetes and glucose intolerance: an integratedindex of vascular function? Circulation 2002;106:2085–2090
39. Roman MJ, Devereux RB, Kizer JR, et al.Central pressure more strongly relates to vascu-lar disease and outcome than does brachialpressure: the Strong Heart Study. Hypertension2007;50:197–20340. Williams B, Lacy PS, Thom SM, et al.; CAFEInvestigators; Anglo-Scandinavian Cardiac Out-comes Trial Investigators; CAFE Steering Com-mittee and Writing Committee. Differentialimpact of blood pressure-lowering drugs oncentral aortic pressure and clinical outcomes:principal results of the Conduit Artery FunctionEvaluation (CAFE) study. Circulation 2006;113:1213–122541. Cherney DZ, Perkins BA, Soleymanlou N,et al. The effect of empagliflozin on arterial stiff-ness and heart rate variability in subjects withuncomplicated type 1 diabetes mellitus. Cardio-vasc Diabetol 2014;13:2842. Heise T, Seman L, Macha S, et al. Safety,tolerability, pharmacokinetics, and pharmaco-dynamics of multiple rising doses of empagliflo-zin in patients with type 2 diabetes mellitus.Diabetes Ther 2013;4:331–34543. Pitt B, Zannad F, Remme WJ, et al.; Ran-domized Aldactone Evaluation Study Investiga-tors. The effect of spironolactone on morbidityand mortality in patients with severe heart fail-ure. N Engl J Med 1999;341:709–71744. Jiang F, Yang J, Zhang Y, et al. Angiotensin-converting enzyme 2 and angiotensin 1-7: noveltherapeutic targets. Nat Rev Cardiol 2014;11:413–42645. Muskiet MH, van Raalte DH, van Bommel E,Smits MM, Tonneijck L. Understanding EMPA-REG OUTCOME. Lancet Diabetes Endocrinol2015;3:928–92946. Phung OJ, Schwartzman E, Allen RW, EngelSS, Rajpathak SN. Sulphonylureas and risk ofcardiovascular disease: systematic review andmeta-analysis. Diabet Med 2013;30:1160–117147. Erdmann E, Dormandy JA, Charbonnel B,Massi-Benedetti M, Moules IK, Skene AM; PRO-active Investigators. The effect of pioglitazoneon recurrent myocardial infarction in 2,445patients with type 2 diabetes and previous myo-cardial infarction: results from the PROactive(PROactive 05) Study. J Am Coll Cardiol 2007;49:1772–178048. Wilcox R, Bousser MG, Betteridge DJ, et al.;PROactive Investigators. Effects of pioglitazonein patients with type 2 diabetes with or withoutprevious stroke: results from PROactive(PROspective pioglitAzone Clinical Trial In mac-roVascular Events 04). Stroke 2007;38:865–87349. Clarke GD, Molina-Wilkins M, Martinez S,et al. Improved left ventricular diastolic function(LVDF) following pioglitazone therapy is stronglyrelated to increased myocardial insulin sensitivity[Abstract]. Diabetes 2014;63(Suppl. 1):A29850. Konrad T, Lubben G, Franzen C. Pioglitazonelowers blood pressure in hypertensive patientswith type 2 diabetes mellitus : an open, multi-centre, observational study. Clin Drug Investig2005;25:337–34051. Nissen SE, Nicholls SJ, Wolski K, et al.;PERISCOPE Investigators. Comparison of piogli-tazone vs glimepiride on progression of coro-nary atherosclerosis in patients with type 2diabetes: the PERISCOPE randomized controlledtrial. JAMA 2008;299:1561–1573
724 SGLT2 and Cardiovascular Risk Diabetes Care Volume 39, May 2016

52. Saremi A, Schwenke DC, Buchanan TA,et al. Pioglitazone slows progression of ath-erosclerosis in prediabetes independentof changes in cardiovascular risk factors.Arterioscler Thromb Vasc Biol 2013;33:393–39953. Rizza S, Cardellini M, Porzio O, et al. Piogli-tazone improves endothelial and adipose tissue
dysfunction in pre-diabetic CAD subjects. Ath-erosclerosis 2011;215:180–18354. Kernan WN, Viscoli CM, Furie KL, et al.; IRISTrial Investigators. Pioglitazone after ischemicstroke or transient ischemic attack. N Engl JMed. 17 February 2016 [Epub ahead of print]55. Dziuba J, Alperin P, Racketa J, et al. Model-ing effects of SGLT-2 inhibitor dapagliflozin
treatment versus standard diabetes therapyon cardiovascular and microvascular outcomes.Diabetes Obes Metab 2014;16:628–63556. Neal B, Perkovic V, de Zeeuw D, et al. Ratio-nale, design, and baseline characteristics of theCanagliflozin Cardiovascular Assessment Study(CANVAS)da randomized placebo-controlledtrial. Am Heart J 2013;166:217–223.e11
care.diabetesjournals.org Abdul-Ghani and Associates 725





























