Embed Size (px)
Citation preview

Once-Daily Liraglutide VersusLixisenatide as Add-on toMetformin in Type 2 Diabetes:A 26-Week RandomizedControlled Clinical TrialDiabetes Care 2016;39:1501–1509 | DOI: 10.2337/dc15-2479
OBJECTIVE
To compare the efficacy and safety of liraglutide versus lixisenatide as add-on tometformin in patients with type 2 diabetes not achieving adequate glycemiccontrol on metformin alone.
RESEARCH DESIGN AND METHODS
In this 26-week, randomized, parallel-group, open-label trial, 404 patients wererandomized 1:1 to liraglutide 1.8 mg or lixisenatide 20mg as add-on tometformin.Liraglutide was administered once daily at any time of the day. Lixisenatide wasadministered once daily within 1 h prior to the morning or evening meal.
RESULTS
At week 26, liraglutide reduced HbA1c (primary end point) more than lixisenatide(estimated treatment difference 20.62% [95% CI 20.8; 20.4]; P < 0.0001), withmore patients reaching HbA1c <7% (53 mmol/mol) and £6.5% (48 mmol/mol)versus lixisenatide (74.2% and 54.6% for liraglutide vs. 45.5% and 26.2% for lix-isenatide; P < 0.0001 for both). Liraglutide reduced fasting plasma glucosemore thanlixisenatide (estimated treatment difference21.15 mmol/L [95% CI21.5;20.8];P < 0.0001). Liraglutide provided greater reduction in mean 9-point self-measuredplasma glucose (P < 0.0001). However, postprandial glucose increments weresmaller with lixisenatide for the meal directly after injection compared with lira-glutide (P < 0.05), with no differences between treatments across all meals. Bothdrugs promoted similar body weight decrease (24.3 kg for liraglutide,23.7 kg forlixisenatide; P = 0.23). The most common adverse events in both groups weregastrointestinal disorders. Greater increases in pulse, lipase, and amylase wereobserved with liraglutide. Hypoglycemic episodes were rare and similar betweenthe two treatments.
CONCLUSIONS
At the dose levels studied, liraglutide was more effective than lixisenatide asadd-on to metformin in improving glycemic control. Body weight reductions weresimilar. Both treatments were well tolerated, with low risk of hypoglycemia andsimilar gastrointestinal adverse event profiles.
1Division of Diabetology, St. Josef Hospital, Ruhr-University Bochum, Bochum, Germany2Biomedical Department of Internal Medicineand Medical Specialties, University of Palermo,Palermo, Italy3Department of Diabetes and Endocrinology,Southmead Hospital, Bristol, U.K.4Novo Nordisk A/S, Søborg, Denmark5Department of Endocrinology, l’Institut du Thorax,Nantes University Hospital, Nantes, France
Corresponding author: Michael Nauck, [email protected].
Received 18 November 2015 and accepted 21May 2016.
Clinical trial reg. no. NCT01973231, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc15-2479/-/DC1.
© 2016 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More in-formation is available at http://diabetesjournals.org/site/license.
Michael Nauck,1 Manfredi Rizzo,2
Andrew Johnson,3 Heidrun Bosch-Traberg,4
Jesper Madsen,4 and Bertrand Cariou5
Diabetes Care Volume 39, September 2016 1501
CLIN
CARE/ED
UCATIO
N/N
UTR
ITION/PSYC
HOSO
CIAL

Glucagon-like peptide 1 (GLP-1) is a gut-derived incretin hormone that stimu-lates insulin and suppresses glucagonsecretion, inhibits gastric emptying, andreduces appetite and food intake (1).A number of GLP-1 receptor agonists
(GLP-1 RAs) have been approved byhealth authorities and have been com-mercially available for the treatment oftype 2 diabetes since 2005 (exenatide,liraglutide, exenatide extended release,lixisenatide, albiglutide, and dulaglutide).The current joint American Diabetes As-sociation (ADA)/European Association forthe Study of Diabetes position state-ment recommends the addition of aGLP-1 RA as a possible second step fortreatment when glycemic control withmetformin is insufficient, and GLP-1 RAsoffer the advantages of body weightloss and low risk of hypoglycemia (2).GLP-1 RAs differ with respect to phar-macokinetics, pharmacodynamics (PD),timing and frequency of administration,and immunogenicity (1,3–5). Based ontheir half-lives and 24-h plasma cover-age, they are usually categorized intoshort acting (half-life: 2–5 h) and long act-ing (half-life: 12 h to several days) (6). Thehalf-life of liraglutide is ;13 h comparedwith;3 h for lixisenatide (7,8).Compared with native human GLP-1,
liraglutide has a C16 fatty (palmitic) acidchain attached at position 26 (lysine) ofthe peptide, and lysine at position 34 re-placed by arginine, resulting in a pro-tracted pharmacokinetic profile suitablefor once-daily administration (8). In long-term trials, as monotherapy or combinedwith one or two oral antidiabetes drugs,including metformin, sulfonylurea (SU),thiazolidinedione, or combined with in-sulin in patients with type 2 diabetes, theaverage decrease in HbA1c with liraglu-tide was up to 1.5% (9–20). In addition,improvements in fasting and postpran-dial plasma glucose excursions wereseen with liraglutide. Liraglutide hasconsistently demonstrated weight re-ductions in clinical trials (9–20). Gastroin-testinal adverse events (AEs), includingtransient events of nausea, diarrhea,and vomiting, were the most commonAEs reported in liraglutide trials. A pulseincrease of 2–3 bpm from baseline wasnoted with liraglutide versus placebo(9). The incidence of hypoglycemia waslow, reflecting the glucose-dependentaction of liraglutide.Major hypoglycemicepisodes were rare, and most of these
major episodes were reported when lir-aglutide was used in combination withSU or insulin (9).
Lixisenatide is based on the structureof exendin-4, with ;50% homology tohuman GLP-1. It differs from exendin-4by the deletion of a proline residue andaddition of six lysine residues at theCOOH-terminal (21). HbA1c reductionsof up to 1%were observed with lixisena-tide 20 mg once daily after 24 weeks’treatment in addition to oral antidiabe-tes drugs or basal insulin (22,23). Further,lixisenatide has a pronounced effect onpostprandial plasma glucose for the mealafter injection, probably due to a delay ingastric emptying. The most common sideeffects are nausea, vomiting, and diar-rhea. Similar to other GLP-1 RAs, the riskof hypoglycemia is low except when lixi-senatide is used in combination with anSU or a basal insulin (7).
The objectives of this 26-week head-to-head trial (clinicaltrials.gov reg. no.NCT01973231) were to compare liraglu-tide and lixisenatide as add-on to met-formin with respect to glycemic control,HOMA of b-cell function (HOMA-B),weight loss, and other efficacy parametersas well as to compare the safety profile ofthe two drugs.
RESEARCH DESIGN AND METHODS
Trial DesignThis was a 26-week, randomized, two-armed, open-label, active-controlled, mul-ticenter, multinational, parallel-group trialinvestigating the efficacy and safety of lir-aglutide 1.8 mg and lixisenatide 20 mg asadd-on to metformin in patients withtype 2 diabetes who had not achievedadequate glycemic control onmetformin(Supplementary Figure 1).
The trial was conducted from 24 Oc-tober 2013 to 19 November 2014 at56 sites in nine countries of the Euro-pean Union (Czech Republic, Finland,France, Germany, Hungary, Italy, Latvia,Lithuania, and U.K.) in accordance withthe Declaration of Helsinki and GoodClinical Practice (24,25). The protocolwas approved by an independent ethicscommittee or institutional review board.Informed consent was obtained in writingprior to any trial-related activities.
PatientsEnrolled patientsweremales and femaleswith type 2 diabetes, age $18 years,HbA1c 7.5210.5% (58291 mmol/mol),
and BMI $20 kg/m2, who were on un-changed metformin treatment at themaximum tolerated dose (1,000 to3,000 mg/day) for at least 90 days priorto screening.
Main exclusions included the follow-ing: female patients of child-bearing po-tential whowaspregnant, breast-feeding,or intending to become pregnant or notusing adequate contraception and pa-tients who were previously treatedwith a GLP-1 RA, who were treated withglucose-lowering agents other than met-forminwithin 90 days of screening or whohad a history of chronic pancreatitis oridiopathic acute pancreatitis, a screeningcalcitonin value $50 ng/L, personal orfamily history of medullary thyroid carci-noma or multiple endocrine neoplasiasyndrome type 2, impaired liver function(alanine aminotransferase $2.5 timesthe upper normal limit [UNL]), impairedrenal function (estimated glomerular fil-tration rate ,60 mL/min/1.73 m2 perMDRD formula), or any chronic disorderor severe disease that in the opinion ofthe investigator might jeopardize thepatient’s safety or compliance with theprotocol.
TreatmentEligible patients were randomized 1:1 us-ing the interactive voice/web responsesystem to receive liraglutide 1.8 mg orlixisenatide 20 mgdboth combined withmetformin. Liraglutide (Victoza, NovoNordisk A/S) and lixisenatide (Lyxumia,Sanofi) were both administered once dailysubcutaneously. Liraglutide was injectedat any time of day irrespective of meals,but time of injection was to be consis-tent throughout the trial. Liraglutide wasstarted at 0.6 mg/day, with weekly doseescalations of 0.6 mg/day until the main-tenance dose of 1.8 mg/day was reached.Lixisenatide was administered within thehour prior to the first meal of the day orthe evening meal in accordance with theapproved label at the time of trial con-duct. After a starting dose of 10 mg, thelixisenatide dose was escalated to 20 mgfrom day 15. If patients could not toleratethe dose of liraglutide 1.8 mg or lixisena-tide 20 mg, they were to discontinue thetrial product.
Patients meeting predefined hypergly-cemia criteria were offered rescue treat-ment (suitable marketed products orattempt to further increase metformindose) at the discretion of the investigator
1502 Liraglutide or Lixisenatide in Type 2 Diabetes Diabetes Care Volume 39, September 2016

as add-on to the trial product during theremainder of the trial.
AssessmentsBlood samples were drawn at specifiedtime points and analyzed at the centrallaboratory (ICON Central Laboratories,Dublin, Ireland) to determine levels ofHbA1c, fasting plasma glucose (FPG), en-docrine pancreatic function (fastingplasma glucagon, proinsulin, C-peptide,proinsulin–to–C-peptide ratio, insulin,and HOMA-B), and fasting plasma lipidprofile (triglycerides, total cholesterol,LDL, HDL, VLDL cholesterol, and freefatty acids). Patients were instructed toperform a 9-point self-measured plasmaglucose (SMPG) profile (before break-fast, 90 min after the start of breakfast,before lunch, 90 min after the startof lunch, before dinner, 90 min afterthe start of dinner, at bedtime, at04:00 A.M., and before breakfast the fol-lowing day) within 1 week prior to sitevisits when the 9-point SMPG profiledata were collected. Body weight, bloodpressure, and pulse were measured fol-lowing the standard clinical practice.All AEs were coded using the Medical
Dictionary for Regulatory Activities (ver-sion 17.1). A medical event of specialinterest was defined as pancreatitis orclinical suspicion of pancreatitis, malig-nant neoplasms, and medication errorsconcerning trial products. PredefinedMedical Dictionary for Regulatory Activ-ities searches were performed on all re-ported AEs to capture medical events ofspecial interest. Hypoglycemic episodeswere defined using the ADA classificationof hypoglycemia (26) and the additionalcategory of confirmed hypoglycemia (pa-tients unable to treat themselves [severehypoglycemic episode] and/or have aplasma glucose reading ,3.1 mmol/L[56 mg/dL]). Clinical laboratory tests in-cluded standard hematology, biochem-istry, urinalysis, amylase, lipase, andcalcitonin at the central laboratory. De-tection of anti-drug antibodies and char-acterization of cross-reactivity to GLP-1was performed at a special laboratory(Celerion Switzerland AG) with a radio-immunoassay using a radioactively la-beled drug in the absence or presenceof an unlabeled drug or GLP-1. Antidrugantibodies were characterized for in vitroneutralizing effect by Novo Nordisk A/Susing a baby hamster kidney cell line trans-fected with the human GLP-1 receptor
and a reporter luciferase gene with lumi-nescence as read out (27).
Statistical MethodsThe sample size was determined in or-der to demonstrate noninferiority of lir-aglutide versus lixisenatide as add-on tometformin with regard to change frombaseline in HbA1c after 26 weeks of treat-ment. Basedon the assumptions of ameandifference of20.1% for change in HbA1cfor liraglutide versus lixisenatide (bothas add-on to metformin), an SD of 1.1%,and a noninferiority margin of 0.3%, thesample size required in order to achieve90% power was 160 in each arm.With anassumed dropout rate of 20%, 200 pa-tients were needed for each arm.
The full analysis set (FAS) included allrandomized patients. The safety analy-sis set (SAS) included all patients receiv-ing at least one dose of any of the trialproducts. All efficacy end points weresummarized and analyzed using theFAS, and all safety end points were sum-marized and analyzed using the SAS.
The statistical analyseswere performedwith a significance level of 5% (two-sidedtests). In the primary analysis, missing val-ues were handled by a mixed model forrepeated measurements (MMRM). Datacollected after initiation of rescue treat-ment or after discontinuation of the ran-domized treatment were consideredmissing in the primary efficacy analyses.For safety variables, all data for patientsreceiving rescue treatment while on ran-domized treatment were included.
The primary end point was the HbA1cchange from baseline to week 26. HbA1cchanges from baseline to measurementsat 6, 12, 16, 20, and 26 weeks were ana-lyzedusinganMMRM,with the treatmentand country as factors and baseline HbA1cas a covariate, all nested within week as afactor. From the MMRMmodel the treat-ment difference atweek26was estimatedand the corresponding two-sided 95% CIwas calculated. Noninferiority of liraglu-tide versus lixisenatide was assessed bycomparing the upper limit of the 95% CIfor the treatment differencewith the non-inferiority limit of 0.3%. Similarly, superi-ority of liraglutide versus lixisenatide wastobe concluded if the95%CI excluded0%.
Secondary efficacy end points, severalsafety end points (pulse, lipase, and amy-lase), and the post hoc analyses were an-alyzed with a method similar to that usedfor the primary end point. If data were log
transformed, the ratios of themeanswereestimated instead of themean difference.The dichotomous end points were ana-lyzed by a logistic regression model. Ef-fects in the model were treatment andcountry as factors and baseline HbA1cas a covariate. Results are presented in-cluding the 95% CI for the odds ratio (OR)(liraglutide over lixisenatide).
Mean9-point SMPGprofilewas definedas the area under the profile (calculatedusing the trapezoidal method) divided bythe measurement time. Mean postpran-dial increment for all meals was calculatedas themeanof the increments frombeforemeal to 90 min after breakfast, lunch, anddinner, respectively. The four-meal incre-ment end points derived from the 9-pointSMPG profiles were analyzed with amethod similar to that used for the pri-mary end point but with three treatmentgroups (liraglutide-treated patients, lixi-senatide-treated patients injecting in themorning, and lixisenatide-treated pa-tients injecting in the evening).
RESULTS
A total of 619 patients were screened,404 patients (202 in each group) wererandomized and exposed, and 340 pa-tients (178 [88.1%] patients for lira-glutide and 162 [80.2%] patients forlixisenatide) completed the 26-weektreatment period without discontinua-tion of trial product and without rescuemedication. Patient disposition is shownin Supplementary Fig. 2. Twenty-ninepatients (7.2%) discontinued trialproduct prematurely: 13 (6.4%) for lira-glutide and 16 (7.9%) for lixisenatide.More patients received rescue medica-tion in the lixisenatide group (16 [7.9%])compared with the liraglutide group(5 [2.5%]). All 404 patients were includedin the FAS and SAS.
There were fewer females (40%) thanmales (60%) in the trial. Mean 6 SD agewas 56.2 6 10.3 years and BMI 34.7 66.7 kg/m2. Mean baseline HbA1c was8.4 6 0.8% (68 6 9 mmol/mmol), meanbaseline FPG was 10.4 6 2.3 mmol/L(186.76 41.7mg/dL), andmean durationof diabetes was 6.46 5.1 years (Table 1).
Primary End Point: HbA1c ChangeFrom Baseline to Week 26From weeks 0 to 26, mean HbA1c valuesdecreased in both treatment groups butto a greater extent with liraglutide (Fig.1A). The estimated change in HbA1c from
care.diabetesjournals.org Nauck and Associates 1503

baseline to week 26 was 21.8% (220.0mmol/mol) for liraglutide and 21.2%(213.3mmol/mol) for lixisenatide. The es-timated treatment difference was 20.6%(95% CI 20.8; 20.4) (26.7 mmol/mol[28.7; 24.8]); P , 0.0001. Based on thepredefined noninferiority margin of 0.3%,noninferiority of liraglutide to lixisenatidewas confirmed. Furthermore, as the 95%CI excluded 0, superiority of liraglutide tolixisenatide was concluded.At week 26, a greater proportion of
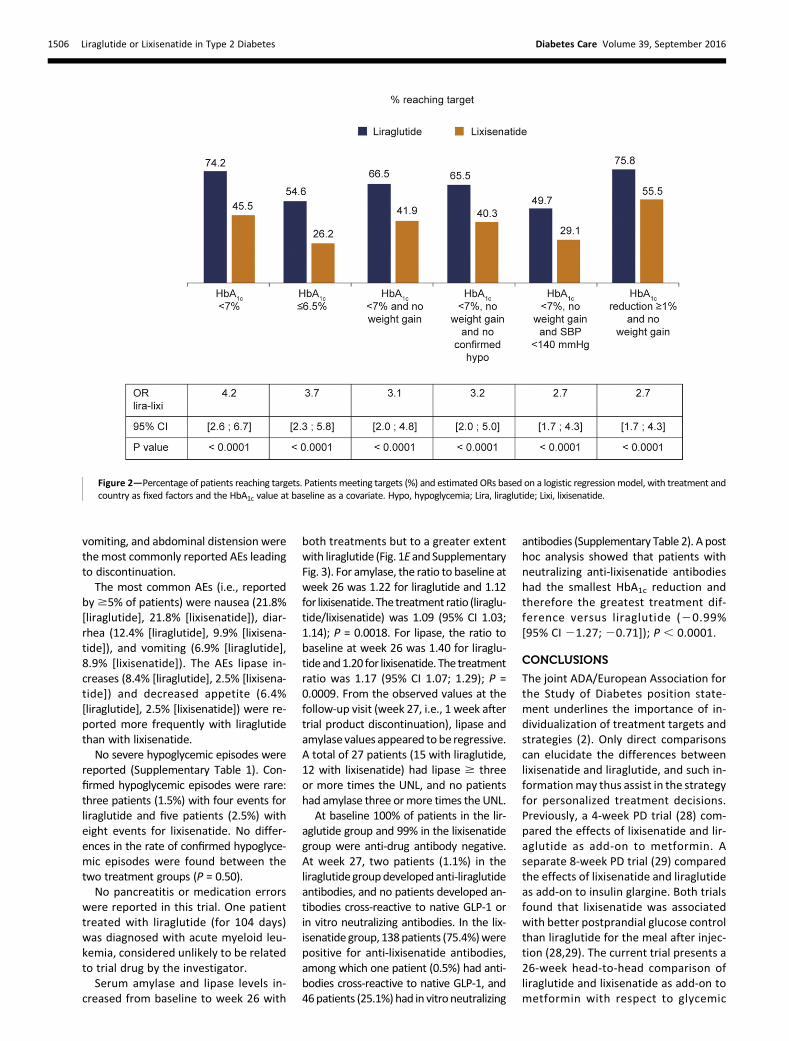
patients reached the HbA1c goals of,7% (53 mmol/mol) with liraglutide(74.2%) than with lixisenatide (45.5%).The OR was 4.2 (95% CI 2.6; 6.7); P ,0.0001. Similarly, more patients achievedthe HbA1c #6.5% (48 mmol/mol) targetwith liraglutide (54.6%) than with lixise-natide (26.2%); P , 0.0001. More pa-tients also achieved the prespecifiedcomposite end points (HbA1c ,7.0%and no weight gain, HbA1c ,7.0% withno weight gain and no confirmed hy-poglycemia, HbA1c ,7.0% with noweight gain and systolic blood pres-sure [SBP] ,140 mmHg, and HbA1c
reduction $1.0% and no weight gain)with liraglutide compared with lixise-natide (Fig. 2).
Fasting Plasma Glucose and Nine-Point Self-measured Plasma Glucose
At week 26, FPG was reduced more withliraglutide (22.9 mmol/L [251.4 mg/dL])than with lixisenatide (21.7 mmol/L[230.6 mg/dL]). The estimated treat-ment difference was 21.2 mmol/L (95%CI 21.5; 20.8) (220.8 mg/dL [95%CI227.2;214.4]); P , 0.0001 (Fig. 1B).
At week 0, the 9-point SMPG profilesfor the liraglutide and lixisenatidegroups were similar. After 26 weeks oftreatment, the two profiles separated,with liraglutide showing lower SMPGvalues at most of the time points (Fig.1D). Liraglutide provided greater reduc-tion in the mean of 9-point SMPG com-pared with lixisenatide. The estimatedchange in the mean of 9-point SMPG frombaseline to week 26 was 22.6 mmol/L(247.5 mg/dL) for liraglutide and 21.9mmol/L (234.0 mg/dL) for lixisenatide.The estimated treatment differencewas 20.8 mmol/L (95% CI 21.1; 20.4)(213.5 mg/dL [95% CI 219.4; 27.6]);P , 0.0001 (Table 2).
Four postprandial increment endpoints (breakfast, lunch, dinner, andmean postprandial increments acrossall 3 meals) from the 9-point SMPG profile
were analyzed by lixisenatide injectiontime (135 patients with morning injectionand 45 patients with evening injection)versus all liraglutide patients. It was foundthat the lixisenatide morning injectiongroup had a lower after-breakfast incre-ment compared with liraglutide (esti-mated treatment difference 1.2 mmol/L[21.6mg/dL]; P, 0.0001); the lixisenatideevening injection group had a lower after-dinner increment compared with liraglu-tide (estimated treatment difference1.3 mmol/L [24.1 mg/dL]; P = 0.0037)(Table 2). However, the mean postpran-dial increments across all meals showedno statistically significant differencesbetween the two treatments.
Body WeightBody weight decreased fromweek 0 to 26in both treatment groups (Fig. 1C). Theestimated change in body weight frombaseline to week 26 was 24.3 kg for lira-glutide and23.7 kg for lixisenatide. Theestimated treatment difference was20.6 kg (95% CI 21.6; 0.4); P = 0.23.
Endocrine Pancreatic FunctionBased on the ratio to baseline, thechanges in fasting state endocrine pan-creatic function after 26 weeks of treat-ment with liraglutide or lixisenatide werein the same direction: decrease in proin-sulin and proinsulin–to–C-peptide ratio,increase in C-peptide and HOMA-B, andminimal changes in fasting insulin andglucagon levels (Table 2). The resultsshowed that after 26weeks of treatment,liraglutide increased fasting C-peptide by7%more and HOMA-B by 28%more thanlixisenatide, and liraglutide decreasedfasting proinsulin by 16% more and fast-ing proinsulin–to–C-peptide ratio by 22%more than lixisenatide (P , 0.05 for all).
Lipid ProfileFor the liraglutide group, HDL cholesterolwas slight increased (2%) compared withbaseline, and all the other lipid parameterswere 4215% decreased based on ratio tobaseline (Table 2). For the lixisenatidegroup, slight increases for HDL (4%) andLDL (1%) were noted, whereas the rest ofthe lipid parameters decreased by 129%.There were no statistically significant dif-ferences between the two treatments.
Blood Pressure and PulseAt week 26, SBP decreased to a similarextent in both treatment groups (Table2). The estimated change in SBP from
Table 1—Demographic and baseline characteristics
Liraglutide Lixisenatide Total
Patients randomized (N) 202 202 404
Female; male (%) 35; 65 45; 55 40; 60
Age (years)Mean (SD) 56.3 (10.6) 56.1 (10.0) 56.2 (10.3)Median (range) 57.5 (24.0; 85.0) 57.5 (23.0; 80.0) 57.5 (23.0; 85.0)
Duration of diabetes (years)Mean (SD) 6.5 (5.3) 6.3 (5.0) 6.4 (5.1)Median (range) 5.4 (0.3; 33.4) 5.4 (0.3; 28.5) 5.4 (0.3; 33.4)
HbA1c (%)Mean (SD) 8.4 (0.7) 8.4 (0.8) 8.4 (0.8)Median (range) 8.3 (7.0; 10.6) 8.3 (7.0; 10.5) 8.3 (7.0; 10.6)
HbA1c (mmol/mol)Mean (SD) 68.3 (7.9) 68.6 (8.6) 68.5 (8.2)Median (range) 67.2 (53; 92) 67.2 (53; 91) 67.2 (53; 92)
FPG (mg/dL)Mean (SD) 188.7 (42.7) 184.7 (40.6) 186.7 (41.7)Median (range) 179.3 (100.9; 367.6) 179.3 (81.1; 293.7) 179.3 (81.1; 367.6)
FPG (mmol/L)Mean (SD) 10.5 (2.4) 10.3 (2.3) 10.4 (2.3)Median (range) 10.0 (5.6; 20.4) 10.0 (4.5; 16.3) 10.0 (4.5; 20.4)
Weight (kg)Mean (SD) 101.9 (23.3) 100.6 (19.9) 101.2 (21.7)Median (range) 99.0 (54.6; 189.0) 98.1 (66.0; 165.7) 98.6 (54.6; 189.0)
BMI (kg/m2)Mean (SD) 34.5 (6.8) 34.9 (6.6) 34.7 (6.7)Median (range) 33.7 (22.5; 58.6) 33.8 (23.8; 63.9) 33.7 (22.5; 63.9)
1504 Liraglutide or Lixisenatide in Type 2 Diabetes Diabetes Care Volume 39, September 2016

baseline to week 26 was24.7 mmHg forliraglutide and 23.5 mmHg for lixisena-tide. The estimated treatment differ-ence for SBP was 21.2 mmHg (95%CI 23.9; 1.5); P = 0.37. Diastolic bloodpressure also decreased, with no differ-ence between treatments.Pulse increased by 2.5 bpm with lira-
glutide from baseline to week 26 and
decreased by21.1 bpm with lixisenatide.The estimated treatment difference was3.6 bpm (95% CI 1.8; 5.4); P = 0.0001.
SafetyThe proportion of patients reporting AEswas 71.8% for liraglutide and 63.9% forlixisenatide (Supplementary Table 1).Twelve patients (5.9%) reported 13 serious
AEs (SAEs) with liraglutide, and seven pa-tients (3.5%) reported seven SAEs withlixisenatide. There was no clustering inthe type of SAEs (Supplementary Table1). The proportions of patients with AEsleading to discontinuation of trial prod-ucts were similar between the twogroups (liraglutide: 13 patients [6.4%];lixisenatide: 15 patients [7.4%]). Nausea,
Figure 1—Time course of HbA1c (A), FPG (B), body weight (C), SMPG (D), and lipase (E) fromweek 0 to week 26. Values are mean estimates (6SEM).These end points were analyzed using a mixedmodel for repeated measurements, with treatment and country as fixed factors and baseline value ascovariate, all nestedwithin visit. Groupmean estimates are adjusted according to the observed baseline distribution. Normal range for lipase: 16–63units/L. ETD, estimated treatment difference after 26 weeks.
care.diabetesjournals.org Nauck and Associates 1505
vomiting, and abdominal distension werethemost commonly reported AEs leadingto discontinuation.The most common AEs (i.e., reported
by$5% of patients) were nausea (21.8%[liraglutide], 21.8% [lixisenatide]), diar-rhea (12.4% [liraglutide], 9.9% [lixisena-tide]), and vomiting (6.9% [liraglutide],8.9% [lixisenatide]). The AEs lipase in-creases (8.4% [liraglutide], 2.5% [lixisena-tide]) and decreased appetite (6.4%[liraglutide], 2.5% [lixisenatide]) were re-ported more frequently with liraglutidethan with lixisenatide.No severe hypoglycemic episodes were
reported (Supplementary Table 1). Con-firmed hypoglycemic episodes were rare:three patients (1.5%) with four events forliraglutide and five patients (2.5%) witheight events for lixisenatide. No differ-ences in the rate of confirmed hypoglyce-mic episodes were found between thetwo treatment groups (P = 0.50).No pancreatitis or medication errors
were reported in this trial. One patienttreated with liraglutide (for 104 days)was diagnosed with acute myeloid leu-kemia, considered unlikely to be relatedto trial drug by the investigator.Serum amylase and lipase levels in-
creased from baseline to week 26 with
both treatments but to a greater extentwith liraglutide (Fig. 1E andSupplementaryFig. 3). For amylase, the ratio to baseline atweek 26 was 1.22 for liraglutide and 1.12for lixisenatide. The treatment ratio (liraglu-tide/lixisenatide) was 1.09 (95% CI 1.03;1.14); P = 0.0018. For lipase, the ratio tobaseline at week 26 was 1.40 for liraglu-tideand1.20 for lixisenatide. The treatmentratio was 1.17 (95% CI 1.07; 1.29); P =0.0009. From the observed values at thefollow-up visit (week 27, i.e., 1 week aftertrial product discontinuation), lipase andamylase values appeared to be regressive.A total of 27 patients (15 with liraglutide,12 with lixisenatide) had lipase $ threeor more times the UNL, and no patientshad amylase three ormore times the UNL.
At baseline 100% of patients in the lir-aglutide group and 99% in the lixisenatidegroup were anti-drug antibody negative.At week 27, two patients (1.1%) in theliraglutidegroupdevelopedanti-liraglutideantibodies, and no patients developed an-tibodies cross-reactive to native GLP-1 orin vitro neutralizing antibodies. In the lix-isenatide group, 138patients (75.4%)werepositive for anti-lixisenatide antibodies,among which one patient (0.5%) had anti-bodies cross-reactive to native GLP-1, and46patients (25.1%)had in vitroneutralizing
antibodies (Supplementary Table 2). A posthoc analysis showed that patients withneutralizing anti-lixisenatide antibodieshad the smallest HbA1c reduction andtherefore the greatest treatment dif-ference versus liraglutide (20.99%[95% CI 21.27; 20.71]); P , 0.0001.
CONCLUSIONS
The joint ADA/European Association forthe Study of Diabetes position state-ment underlines the importance of in-dividualization of treatment targets andstrategies (2). Only direct comparisonscan elucidate the differences betweenlixisenatide and liraglutide, and such in-formationmay thus assist in the strategyfor personalized treatment decisions.Previously, a 4-week PD trial (28) com-pared the effects of lixisenatide and lir-aglutide as add-on to metformin. Aseparate 8-week PD trial (29) comparedthe effects of lixisenatide and liraglutideas add-on to insulin glargine. Both trialsfound that lixisenatide was associatedwith better postprandial glucose controlthan liraglutide for the meal after injec-tion (28,29). The current trial presents a26-week head-to-head comparison ofliraglutide and lixisenatide as add-on tometformin with respect to glycemic
Figure 2—Percentage of patients reaching targets. Patients meeting targets (%) and estimated ORs based on a logistic regressionmodel, with treatment andcountry as fixed factors and the HbA1c value at baseline as a covariate. Hypo, hypoglycemia; Lira, liraglutide; Lixi, lixisenatide.
1506 Liraglutide or Lixisenatide in Type 2 Diabetes Diabetes Care Volume 39, September 2016

control, body weight, b-cell function (asmeasured by HOMA-B), and safety profile.While clinically relevant HbA1c reduc-
tions were seen with both drugs in thistrial, a greater HbA1c reduction was ob-served for liraglutide compared with lixise-natide, with an estimated treatmentdifference of20.6% (95% CI20.8;20.4);P, 0.0001. Larger proportions of patientstreated with liraglutide achieved the HbA1ctargets of ,7% and #6.5%. In line withprevious experience of long-acting versusshort-acting GLP-1 RAs (6), the FPG reduc-tion was greater with liraglutide than withlixisenatide. Also, the mean 9-point SMPG
profile was lower with liraglutide versuslixisenatide. Lixisenatide treatment re-sulted in lower postprandial glucose incre-ments only for the meal after the druginjection compared with liraglutide (no sig-nificant differences for the mean across allmeals), which is consistent with the find-ings from the PD trials (28,29).
Regarding any preferential reductionsin postprandial glycemic increments infavor of lixisenatide (a representativeof the short-acting GLP-1 RAs), this wasonly seen for themeal immediately afterthe injection (Table 2). In the currentstudy, like with previous comparisons
of short-acting (e.g., lixisenatide) andlong-acting (e.g., liraglutide) GLP-1 RAsused on a background of oral glucose-lowering agents, liraglutide was supe-rior with respect to glycemic control(fasting and overall) (10,30–32).
In addition to the effects on glycemiccontrol, clinically relevant body weightreductions were observed in this trial inboth treatment groups, with no differ-ence between the treatment groups.
Clinically relevant reductions in SBPand diastolic blood pressure were ob-served in both groups, with no differ-ences between the groups. No marked
Table 2—Secondary end points after 26 weeks of treatment
Lira (n = 202):change from baselineor ratio to baseline
Lixi (n = 202):change from baselineor ratio to baseline
Lira-Lixi
ETD or ETR 95% CI P*
SMPG*Mean of 9-point SMPG (mmol/L) 22.64 21.89 20.75 21.08; 20.42 ,0.0001Mean of 9-point SMPG (mg/dL) 247.5 234.0 213.5 219.4; 27.6 ,0.0001
Postprandial increments (mmol/L)*All liraglutide patients (n = 202) vs.
lixisenatide patients injecting inthe morning (n = 135)
Postbreakfast 20.86 22.06 1.20 0.65; 1.75 ,0.0001Postlunch 20.60 20.44 20.17 20.69; 0.35 0.53Postdinner 20.67 20.39 20.29 20.89; 0.31 0.34Mean of all 3 meals 20.71 20.94 0.22 20.14; 0.58 0.23
All liraglutide patients (n = 202) vs.lixisenatide patients injecting inthe evening (n = 45)
Postbreakfast 20.86 20.97 0.11 20.72; 0.94 0.80Postlunch 20.60 20.47 20.13 20.92; 0.66 0.74Postdinner 20.67 22.02 1.34 0.44; 2.25 0.0037Mean of all 3 meals 20.71 21.16 0.44 20.10; 0.99 0.11
Endocrine pancreatic function†Fasting insulin 0.95 0.92 1.03 0.91; 1.15 0.65Fasting C-peptide 1.08 1.01 1.07 1.00; 1.15 0.04Fasting proinsulin 0.67 0.80 0.84 0.73; 0.96 0.01Fasting proinsulin–to–C-peptide ratio 0.62 0.80 0.78 0.71; 0.86 ,0.0001Fasting glucagon 0.97 1.00 0.97 0.92; 1.02 0.28HOMA-B 1.67 1.30 1.28 1.14; 1.45 ,0.0001
Lipid profile†Total cholesterol 0.96 0.99 0.97 0.93; 1.00 0.08LDL cholesterol 0.96 1.01 0.95 0.89; 1.01 0.11VLDL cholesterol 0.87 0.92 0.95 0.88; 1.02 0.17HDL cholesterol 1.02 1.04 0.99 0.96; 1.02 0.46Triglycerides 0.85 0.91 0.93 0.86; 1.01 0.10Free fatty acids 0.93 0.93 1.00 0.92; 1.09 0.92
Vital signs*SBP (mmHg) 24.70 23.49 21.21 23.87; 1.45 0.37Diastolic blood pressure (mmHg) 22.62 22.69 0.07 21.53; 1.67 0.93Pulse (bpm) 2.50 21.10 3.60 1.78; 5.43 0.0001
ETD, estimated treatment difference; ETR, estimated treatment ratio; HOMA-B, HOMA-b-cell function; Lira, liraglutide; Lixi, lixisenatide. *These endpoints were analyzed usingmixedmodel for repeatedmeasurement with visit, treatment, and country as fixed factors and baseline as a covariate, allnested within visit. Estimated change from baseline and estimated treatment difference are presented. †These end points were log transformed andthen analyzed using a mixed model with treatment and country as fixed factors and log-transformed baseline value as covariate. Estimated ratio tobaseline and estimated treatment ratio are presented. Postprandial increment analyses included all liraglutide-treated patients regardless ofinjection time (n = 202) and all lixisenatide patients injecting in the morning (n = 135) or in the evening (n = 45), respectively. For the remaining22 patients, the lixisenatide injection time was unknown.
care.diabetesjournals.org Nauck and Associates 1507

differences in lipid profiles were notedbetween the two drugs. Greater im-provements in fasting C-peptide, proin-sulin, proinsulin–to–C-peptide ratio,and HOMA-B were shown for liraglutideversus lixisenatide. As these parameterswere, however, measured in the fastingstate, the improvement was potentiallypartially affected by the differences inglycemic control and by the differencesin drug exposure owing to different half-lives of liraglutide and lixisenatide.Regarding safety, both liraglutide and
lixisenatide were well tolerated, withsimilar gastrointestinal side effects al-ready known to be associated withGLP-1 RA treatment. The most com-mon AEs were nausea, diarrhea, andvomiting. The proportions of patientsreporting AEs and SAEs, respectively,appeared comparable between thegroups. No clustering of SAEs was ob-served in either group. Confirmed hypo-glycemic episodes were rare with bothtreatments, and no severe hypoglycemicepisodes were reported.A pulse increasewas seen in the current
trial with liraglutide (2.5 bpm), the magni-tude of which was in accordance with pre-vious trials (33). Pulse decreased slightlywith lixisenatide (21.1 bpm). The time ofthe pulse measurement in relation to lix-isenatide injection was not prespecified(i.e., depending on the time of visit, pa-tients could have had the pulse mea-surement at trough concentrations oflixisenatide). In a previous study, pulse in-crease of 3 bpm has been described withlixisenatide compared with 9 bpm for lira-glutide using 24-h monitoring (29). Whilethe long-termcardiovascular outcome trial(CVOT) Evaluation of Cardiovascular Out-comes in Patients With Type 2 DiabetesAfter Acute Coronary Syndrome DuringTreatment With AVE0010 (Lixisenatide)(ELIXA) (34) recently confirmed the cardio-vascular safety of lixisenatide (35), resultsfrom the liraglutideCVOT Liraglutide Effectand Action in Diabetes: Evaluation of car-diovascular outcome Results (LEADER) areexpected to be available in 2016 (36–38).Lipase and amylase increases have also
been seen with other GLP-1 RAs and di-peptidyl peptidase-4 inhibitors (31,39,40),and therefore routine monitoring of pan-creatic enzymes is implemented in trialswith liraglutide. The mechanism underly-ing the GLP-1–mediated increase of amy-lase and lipase is still unclear. Increases inpancreatic enzymes were seen with both
liraglutide and lixisenatide in this trial butwere higher with liraglutide. No cases ofpancreatitis occurred in the present trial,and the clinical relevance of these obser-vations is uncertain.
A low incidence of anti-drug antibodydevelopment was seen with liraglutide(two patients [1.1%]) compared with lix-isenatide (138 patients [75.4%]). WhileHbA1c did not seem to be impacted byanti-drug antibody status overall, the sub-group of patients with neutralizing anti-bodies to lixisenatide seemed to have theleast HbA1c reduction (post hoc analysis).
Potential limitations of this trial includethe relatively short 6-month duration,open-label nature, and impossibility of adouble-dummy design. We did not studythe effect of liraglutide 1.2 mg versus lix-isenatide in the current trial. In previoustrials (11,15) using both doses of liraglu-tide as add-on tometformin, minor differ-ences in HbA1c reduction were observedbetween 1.8 mg and 1.2 mg. Thereforethe estimated treatment difference of lir-aglutide 1.2 mg versus lixisenatide wouldmost likely be similar to that between lir-aglutide 1.8 mg and lixisenatide.
In conclusion, at the dose levels stud-ied, liraglutide was more effective thanlixisenatide as add-on to metformin in im-proving glycemic control. Body weight re-ductions were similar. Both treatmentswere well tolerated, with low risk of hypo-glycemia and similar gastrointestinal ad-verse events profiles; however, increasesin pulse, lipase, and amylase were greaterfor liraglutide.
Acknowledgments. The authors thank all ofthe investigators and their staff. The full list ofinvestigators is provided in SupplementaryData.Duality of Interest. This clinical trial was spon-sored by Novo Nordisk A/S. Dongmei Zhangfrom Novo Nordisk, Inc., provided editorial as-sistance for the manuscript. Watermeadow(Witney, U.K.) assisted with proofreading, for-matting, and accuracy checks, supported byNovo Nordisk. M.N. served on advisory panelsfor AstraZeneca/Bristol-Myers Squibb, Berlin-Chemie AG, Boehringer Ingelheim GmbH, Intar-cia Therapeutics, Inc., Janssen PharmaceuticalCompanies of Johnson & Johnson, Merck Sharp& Dohme, Novartis Pharma GmbH, Novo Nor-disk A/S, Profil Institute for Clinical Research,Inc., Sanofi Pasteur SA, and Versartis, Inc.; hasreceived research support from AstraZeneca/Bristol-Myers Squibb, Intarcia Therapeutics,Inc., Merck Sharp & Dohme, Novartis Pharma-ceuticals Corporation, Novo Nordisk A/S; and hasserved on the speaker’s bureau for AstraZeneca/Bristol-MyersSquibb,Berlin-ChemieAG,BoehringerIngelheim GmbH, Eli Lil ly and Company,
GlaxoSmithKline, Janssen Pharmaceutical Com-panies of Johnson & Johnson, Merck Sharp &Dohme, and Sanofi Pasteur SA. M.R. served onadvisory panels for AstraZeneca PharmaceuticalsLP, Eli Lilly and Company/Boehringer IngelheimPharmaceuticals, Inc., Kowa Pharmaceuticals,and Novo Nordisk, Inc.; on the speaker’s bu-reau for AstraZeneca, Bristol-Myers Squibb,Boehringer Ingelheim Pharmaceuticals, Inc.,Merck Sharp & Dohme, and Novo Nordisk, Inc.;and has participated in conferences sponsoredby Eli Lilly and Company, Novartis PharmaGmbH,NovoNordisk, Inc., and Servier. A.J. servedon advisory panels for Novo Nordisk and Sanofiand performs commercial research, which isundertaken on behalf of the North BristolNHS Trust, for Janssen, AstraZeneca, Eli Lilly,Novo Nordisk, Bayer, and Sanofi. H.B.-T. and J.M.are Novo Nordisk employees. B.C. has served asa board member for Amgen Inc., AstraZeneca/Bristol-Myers Squibb, Eli Lilly and Company,Janssen Pharmaceutical Companies of Johnson &Johnson, Novo Nordisk A/S, Regeneron Pharma-ceuticals, Inc., Sanofi Pasteur SA, and Takeda Phar-maceutical Company and as a consultant forGenfit. No other potential conflicts of interest rel-evant to this article were reported.Author Contributions. M.N. and B.C. are sig-natory investigators for the trialandwere involvedin interpreting data and contributing to the con-tent of the manuscript. M.R. was a main investiga-tor for the trial,was involved indata interpretation,and contributed to the content of the manu-script. A.J. contributed to the content of themanuscript. H.B.-T. contributed to trial design,data interpretation, and content of the manu-script. J.M. contributed to data analysis and thecontent of the manuscript. All authors approvedthe manuscript before submission. M.N. is theguarantor of this work and, as such, had full accessto all the data in the study and takes responsibil-ity for the integrity of the data and the accuracyof the data analysis.Prior Presentation. Parts of this study werepresented in abstract form at the 51st AnnualMeeting of the European Association for theStudy of Diabetes, Stockholm, Sweden, 14–18September 2015.
References1. Drucker DJ, Nauck MA. The incretin system:glucagon-like peptide-1 receptor agonists anddipeptidyl peptidase-4 inhibitors in type 2 dia-betes. Lancet 2006;368:1696–17052. Inzucchi SE, Bergenstal RM, Buse JB, et al.Management of hyperglycemia in type 2 diabe-tes, 2015: a patient-centered approach: updateto a position statement of the American Diabe-tes Association and the European Associationfor the Study of Diabetes. Diabetes Care 2015;38:140–1493. JespersenMJ, Knop FK, ChristensenM. GLP-1agonists for type 2 diabetes: pharmacokineticand toxicological considerations. Expert OpinDrug Metab Toxicol 2013;9:17–294. Nauck MA. Incretin-based therapies fortype 2 diabetes mellitus: properties, functions,and clinical implications. Am J Med 2011;124(Suppl.):S3–S185. RyanD, Acosta A. GLP-1 receptor agonists: Non-glycemic clinical effects in weight loss and beyond.Obesity (Silver Spring) 2015;23:1119–1129
1508 Liraglutide or Lixisenatide in Type 2 Diabetes Diabetes Care Volume 39, September 2016

6. Meier JJ. GLP-1 receptor agonists for individ-ualized treatment of type 2 diabetes mellitus.Nat Rev Endocrinol 2012;8:728–7427. Annex I: summary of product characteristics[Internet], 2014. Available from http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002445/WC500140401.pdf. Accessed 5 November 20158. Knudsen LB, Nielsen PF, Huusfeldt PO, et al.Potent derivatives of glucagon-like peptide-1with pharmacokinetic properties suitable foronce daily administration. J Med Chem 2000;43:1664–16699. Liraglutide (NN2211). Abbreviated Investigator’sBrochure. Edition 16. Bagsværd, Denmark, NovoNordisk A/S, 201410. Buse JB, Rosenstock J, Sesti G, et al.; LEAD-6Study Group. Liraglutide once a day versus exena-tide twice a day for type 2 diabetes: a 26-weekrandomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet 2009;374:39–4711. Pratley RE, Nauck MA, Bailey T, et al.; 1860-LIRA-DPP-4 Study Group. Efficacy and safety ofswitching from the DPP-4 inhibitor sitagliptin tothe human GLP-1 analog liraglutide after52 weeks in metformin-treated patients withtype 2 diabetes: a randomized, open-label trial.Diabetes Care 2012;35:1986–199312. Garber A, Henry R, Ratner R, et al.; LEAD-3(Mono) Study Group. Liraglutide versus glime-piride monotherapy for type 2 diabetes (LEAD-3Mono): a randomised, 52-week, phase III, dou-ble-blind, parallel-treatment trial. Lancet 2009;373:473–48113. Garber A, Henry RR, Ratner R, Hale P, ChangCT, Bode B; LEAD-3 (Mono) Study Group.Liraglutide, a once-daily human glucagon-likepeptide 1 analogue, provides sustained im-provements in glycaemic control and weightfor 2 years as monotherapy compared with gli-mepiride in patients with type 2 diabetes. Di-abetes Obes Metab 2011;13:348–35614. Marre M, Shaw J, Brandle M, et al.; LEAD-1SU study group. Liraglutide, a once-daily humanGLP-1 analogue, added to a sulphonylurea over26 weeks produces greater improvements inglycaemic and weight control compared withadding rosiglitazone or placebo in subjectswith Type 2 diabetes (LEAD-1 SU). Diabet Med2009;26:268–27815. NauckM, Frid A, Hermansen K, et al.; LEAD-2Study Group. Efficacy and safety comparison ofliraglutide, glimepiride, and placebo, all in combi-nation with metformin, in type 2 diabetes: theLEAD (Liraglutide Effect and Action in Diabetes)-2study. Diabetes Care 2009;32:84–9016. Nauck M, Frid A, Hermansen K, et al. Long-term efficacy and safety comparison of liraglu-tide, glimepiride and placebo, all in combinationwith metformin in type 2 diabetes: 2-year re-sults from the LEAD-2 study. Diabetes ObesMetab 2013;15:204–21217. Pratley RE, Nauck M, Bailey T, et al.; 1860-LIRA-DPP-4 Study Group. Liraglutide versus sita-gliptin for patients with type 2 diabetes who didnot have adequate glycaemic control with met-formin: a 26-week, randomised, parallel-group,open-label trial. Lancet 2010;375:1447–145618. Pratley R, Nauck M, Bailey T, et al.; 1860-LIRA-DPP-4 Study Group. One year of liraglutidetreatment offers sustained and more effec-tive glycaemic control and weight reduction
compared with sitagliptin, both in combina-tion with metformin, in patients with type 2diabetes: a randomised, parallel-group, open-label trial. Int J Clin Pract 2011;65:397–40719. Russell-Jones D, Vaag A, Schmitz O, et al.;Liraglutide Effect and Action in Diabetes 5(LEAD-5) met+SU Study Group. Liraglutide vsinsulin glargine and placebo in combinationwith metformin and sulfonylurea therapy intype 2 diabetes mellitus (LEAD-5 met+SU): arandomised controlled trial. Diabetologia2009;52:2046–205520. Zinman B, Gerich J, Buse JB, et al.; LEAD-4Study Investigators. Efficacy and safety of thehuman glucagon-like peptide-1 analog liraglu-tide in combination with metformin and thiazo-lidinedione in patients with type 2 diabetes(LEAD-4 Met+TZD). Diabetes Care 2009;32:1224–123021. Werner U, Haschke G, Herling AW, KramerW. Pharmacological profile of lixisenatide: Anew GLP-1 receptor agonist for the treatmentof type 2 diabetes. Regul Pept 2010;164:58–6422. Charbonnel B, Bertolini M, Tinahones FJ,Domingo MP, Davies M. Lixisenatide plus basalinsulin in patients with type 2 diabetes mellitus:a meta-analysis. J Diabetes Complications 2014;28:880–88623. Raccah D, Gourdy P, Sagnard L, Ceriello A.Lixisenatide as add-on to oral anti-diabetic ther-apy: an effective treatment for glycaemic con-trol with body weight benefits in type 2diabetes. Diabetes Metab Res Rev 2014;30:742–74824. International Conference on Harmonisa-tion of Technical Requirements for Registrationof Pharmaceuticals for Human Use. ICHharmonised tripartite guideline. Guidelinefor good clinical practice E6(R1) [Internet],1996. Available from http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E6/E6_R1_Guideline.pdf.Accessed 5 November 201525. World Medical Association. WMA Declara-tion of Helsinki. Ethical principles for medicalresearch involving human subjects [Internet],2008. Available from http://www.wma.net/en/30publications/10policies/b3/. Accessed5 November 201526. Workgroup on Hypoglycemia, AmericanDiabetes Association. Defining and reportinghypoglycemia in diabetes: a report from theAmerican Diabetes Association Workgroup onHypoglycemia. Diabetes Care 2005;28:1245–124927. Buse JB, Garber A, Rosenstock J, et al. Lir-aglutide treatment is associated with a low fre-quency and magnitude of antibody formationwith no apparent impact on glycemic responseor increased frequency of adverse events: re-sults from the Liraglutide Effect and Action inDiabetes (LEAD) trials. J Clin Endocrinol Metab2011;96:1695–170228. Kapitza C, Forst T, Coester HV, Poitiers F,Ruus P, Hincelin-Mery A. Pharmacodynamiccharacteristics of lixisenatide once daily versusliraglutide once daily in patients with type 2 di-abetes insufficiently controlled on metformin.Diabetes Obes Metab 2013;15:642–64929. Meier JJ, Rosenstock J, Hincelin-Mery A,et al. Contrasting effects of lixisenatide and
liraglutide on postprandial glycemic control,gastric emptying, and safety parameters in pa-tients with type 2 diabetes on optimized insulinglargine with or without metformin: a random-ized, open-label trial. Diabetes Care 2015;38:1263–127330. Buse JB, Nauck M, Forst T, et al. Exenatideonce weekly versus liraglutide once daily in pa-tients with type 2 diabetes (DURATION-6): arandomised, open-label study. Lancet 2013;381:117–12431. Dungan KM, Povedano ST, Forst T, et al.Once-weekly dulaglutide versus once-daily lira-glutide in metformin-treated patients withtype 2 diabetes (AWARD-6): a randomised,open-label, phase 3, non-inferiority trial. Lancet2014;384:1349–135732. Pratley RE, Nauck MA, Barnett AH, et al.;HARMONY 7 study group. Once-weekly albiglu-tide versus once-daily liraglutide in patientswith type 2 diabetes inadequately controlledon oral drugs (HARMONY 7): a randomised,open-label, multicentre, non-inferiority phase3 study. Lancet Diabetes Endocrinol 2014;2:289–29733. Fonseca VA, Devries JH, Henry RR,Donsmark M, Thomsen HF, Plutzky J. Reduc-tions in systolic blood pressure with liraglutidein patients with type 2 diabetes: insights from apatient-level pooled analysis of six randomizedclinical trials. J Diabetes Complications 2014;28:399–40534. Bentley-Lewis R, Aguilar D, Riddle MC,et al.; ELIXA Investigators. Rationale, design,and baseline characteristics in Evaluation ofLIXisenatide in Acute Coronary Syndrome, along-term cardiovascular end point trial of lix-isenatide versus placebo. Am Heart J 2015;169:631–638.e735. Pfeffer MA, Claggett B, Diaz R, et al.; ELIXAInvestigators. Lixisenatide in patients withtype 2 diabetes and acute coronary syndrome.N Engl J Med 2015;373:2247–225736. Marso SP, Poulter NR, Nissen SE, et al. De-sign of the Liraglutide Effect and Action in Di-abetes: Evaluation of cardiovascular outcomeResults (LEADER) trial. Am Heart J 2013;166:823–30.e537. Steinberg WM, Nauck MA, Zinman B, et al.;LEADER Trial investigators. LEADER 3--lipaseand amylase activity in subjects with type 2diabetes: baseline data from over 9000 sub-jects in the LEADER Trial. Pancreas 2014;43:1223–123138. Daniels GH, Hegedus L, Marso SP, et al.;LEADER Trial Investigators. LEADER 2: baselinecalcitonin in 9340 people with type 2 diabetesenrolled in the Liraglutide Effect and Action inDiabetes: Evaluation of cardiovascular out-come Results (LEADER) trial: preliminary ob-servations. Diabetes Obes Metab 2015;17:477–48639. Lando HM, Alattar M, Dua AP. Elevatedamylase and lipase levels in patients using glu-cagonlike peptide-1 receptor agonists or dipeptidyl-peptidase-4 inhibitors in the outpatient setting.Endocr Pract 2012;18:472–47740. Tokuyama H, Kawamura H, Fujimoto M,et al. A low-grade increase of serum pancreaticexocrine enzyme levels by dipeptidyl peptidase-4inhibitor in patients with type 2 diabetes. Diabe-tes Res Clin Pract 2013;100:e66–e69
care.diabetesjournals.org Nauck and Associates 1509





























