Embed Size (px)
Citation preview
ARTICLE IN PRESS
0020-7489/$ - se
doi:10.1016/j.ijn
�CorrespondCollege of Tec
Hualien, 970 T
fax: +886 3857
E-mail addr
International Journal of Nursing Studies 44 (2007) 1371–1378
www.elsevier.com/locate/ijnurstu
Taiwanese nurses’ attitudes towards and useof complementary and alternative medicine in nursing practice:
A cross-sectional survey
Fang-Ying Chua,b,�, Marianne Wallisb,c
aNursing Department, Tzu Chi College of Technology, Taiwan, ROCbSchool of Nursing and Midwifery, Griffith University, Australia
cResearch Centre for Practice Innovation, Griffith University and Gold Coast Health Service District, Queensland, Australia
Received 18 October 2005; received in revised form 10 July 2006; accepted 13 July 2006
Abstract
Background: Increasingly, nurses in Western countries express positive attitudes to complementary and alternative
medicine (CAM) but lack knowledge, access to education and organisational policy to guide practice. It is unclear
whether nurses in developed Asian countries mirror or differ from this profile.
Objectives: To determine the attitudes towards and use of CAM by registered nurses in Taiwan.
Design: Cross sectional survey.
Setting: A Nursing College in eastern Taiwan.
Participants: Registered nurses (N ¼ 170) working in various clinical settings who were studying a post registration
Bachelor of Nursing conversion course.
Methods: Questionnaire distributed to nurses during class time.
Results: Most nurses had positive attitudes to CAM and most used therapies, like massage, occasionally in practice.
However, none had formal qualifications in CAM and most perceived that there were insufficient resources or
organisational policy to facilitate practice.
Conclusions: Taiwanese nurses need more formal education about CAM and require access to clear policies regarding
the safe use of CAM in nursing practice.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Attitudes; Complementary and alternative medicine; Registered nurses; Utilisation
e front matter r 2006 Elsevier Ltd. All rights reserve
urstu.2006.07.001
ing author. Nursing Department, Tzu Chi
hnology 880, Section 2, Chien Kuo Road,
aiwan, ROC. Tel.: +886 38572158;
7962.
ess: [email protected] (F.-Y. Chu).
What is already known about the topic?
�
d.
CAMs are increasingly being used by the general
public and hospitalised patients across the developed
world.
�
Nurses are increasingly becoming interested inadopting some CAM into nursing practice but often
lack knowledge related to these therapies.

ARTICLE IN PRESSF.-Y. Chu, M. Wallis / International Journal of Nursing Studies 44 (2007) 1371–13781372
�
In countries such as the UK and Australia studieshave revealed positive attitudes but poor education in
nurses and a lack of organisational policies related to
the administration of CAM.
What this paper adds
�
Despite high rates of CAM use by patients inTaiwan, nurses have received little formal education
about CAM.
�
Taiwanese nurses have positive attitudes to manyCAM but rarely include them in their practice.
�
As found in English-speaking countries nursesperceive a lack of organisational policies and
organisational resources related to the administration
of CAM, in acute care in-patient facilities, in Taiwan.
1. Introduction
Complementary and alternative medicine (CAM) has
gained increasing popularity worldwide during the past
decade (Cassileth and Deng, 2004). The rates of use
of CAM in the USA range from 30% to 50% (Baldwin
et al., 2002; Leung et al., 2001). Thomas et al. (2001)
estimated that 46.6% of the population in England
have used some form of CAM in their lifetime. In
Australia, those in the 25–54 year-old age group are
more likely to consider CAM than the other age groups
(Wilkinson and Simpson, 2002). In Taiwan, the rate of
use ranges from 51% to 82%, a much higher rate than
that of the English-speaking world (Lin, 1999; Chang
and Li, 2004).
As CAM use increases worldwide, especially in
Taiwan, more people who are admitted to hospitals
are likely to be using some form of CAM. It is important
for nurses who work in the health care setting to have an
understanding of how these therapies work, and the
potential for adverse interactions between complemen-
tary therapy modalities and conventional medical
treatment. However, there is little information available
about Taiwanese nurses’ attitudes toward CAM and
there are little data to indicate which CAMs are used.
Also, there is scant information about which formal or
informal qualifications in CAM Taiwanese nurses have
obtained from accredited institutions, or which policies
related to CAM practice guide Taiwanese nurses. The
purpose of this study was to explore Taiwanese nurses’
attitudes towards CAM and current utilisation of CAMs
in nursing practice. The educational preparation of
nurses, with respect to CAM, and nurses’ knowledge of
policy and procedures to guide the practice of CAM,
were also investigated.
2. Literature review
The National Centre for Complementary and Alter-
native Medicine (2002), in the USA, classifies CAM into
five categories. These include: (1) alternative medical
systems, such as traditional Chinese medicine (including
acupuncture), naturopathic medicine, ayurvedic medi-
cine and homoeopathy; (2) mind–body interventions
such as meditation, prayer, hypnotherapy, yoga, Tai
Chi, art dance, music therapy; (3) biologically based
therapies including foods, herbs, vitamins, dietary
supplements, aromatherapy; (4) manipulative and
body-based methods, for example, chiropractic or
osteopathic manipulation, and massage; and (5) energy
therapies such as Gi Gong, therapeutic touch and
magnet therapy. CAM includes non-conventional heal-
ing methods and in relation to nursing, refers to any
approaches used in nursing practice to promote healing
and mental and physical well-being which are congruent
with the tenets of holistic nursing practice and are not
necessarily prescribed by a medical officer (Cassileth and
Deng, 2004).
Most of the studies reviewed showed that health
professionals have a positive attitude toward CAM, but
lack knowledge related to clear definitions, correct usage
and adverse reactions (Botting and Cook, 2000;
Brolinson et al., 2001; Frenkel and Borkan, 2003; Hayes
and Alexander, 2000; Hessig et al., 2004; Risberg et al.,
2004). Nurses’ attitudes towards CAM are reported less
frequently than physicians’ attitudes. In general, nurses
from Western countries and other countries have been
open-minded toward CAM (DeKeyser et al., 2001; King
et al., 2000; McDowell and Burman, 2004; Risberg et al.,
2004; Tracy et al., 2003).
As the general public increases its use of CAM, it
becomes necessary for accurate sources of information
about these therapies to be readily available. One of the
largest groups of health professionals that are in regular
contact with the public are nurses, and it seems logical to
have nurses take a significant role in assisting patients in
making informed decisions regarding CAM. Thus,
nurses need to become well informed regarding the
efficacy and safety of CAM. Lindquist et al. (2005)
conducted a statewide survey in America. The results
showed that critical care nurses’ knowledge about a
therapy was highly associated with their perceptions of
the efficacy of that therapy. The therapies most
frequently used in nursing practice were similar to those
that nurses used personally. Frequently used therapies
included massage, music, exercise, diet, prayer, and
counselling. These results are consistent with the other
studies (Fearon, 2003; King et al., 2000; McDowell and
Burman, 2004; Sohn and Loveland Cook, 2002; Tracy
et al., 2003).
However, a qualitative study conducted in Canada by
McDowell and Burman (2004) indicated that personal

ARTICLE IN PRESSF.-Y. Chu, M. Wallis / International Journal of Nursing Studies 44 (2007) 1371–1378 1373
positive perceptions were inconsistent with what nurses
said about their professional practice. Despite the
overall feeling that CAM could be useful and beneficial
in the acute setting, most of the participants admitted to
not asking about their patients’ use of CAM or their
preferences for therapies while in the hospital, and did
not actively recommend CAM to their patients. The
reasons may have been as simple as a reluctance to offer
therapies that require extra time, or the perception that
clients were not interested.
In an Australian pilot study, Wallis et al. (2004) found
that registered nurses (RNs) engaged in some form of
complementary therapy on a regular basis. This study
also revealed a small number were engaging in CAM
outside of the scope of nursing practice. It is of concern
that some of these nurses may not have had appropriate
training, accreditation or indemnity insurance and that
they were not supported by appropriate institutional
policies (Wallis et al., 2004). This may be similar to the
situation in Taiwan; however, there are no data
available. There have been studies in a number of
Western countries related to nurses’ attitudes to and the
use of CAM and their referral patterns, but no
information on Taiwanese nurses was found in a search
of the literature.
3. Research questions
There are three main research questions that directed
this study.
1.
What are the attitudes of nurses registered in Taiwantowards CAM?
2.
To what extent do nurses in Taiwan use CAM duringtheir day-to-day nursing practice?
3.
What factors influence nurses’ use of CAM innursing practice in Taiwan?
4. Methods
4.1. Sample and setting
The population sampled for this study was RNs
undertaking a course designed to convert their college
acquired certificate or diploma to a Bachelor of Nursing.
This population was chosen as representing a large
proportion of Taiwanese nurses with a range of
experience but not being within the first year of working
as a registered nurse. All the current nurses at one
Technology College, in the east of Taiwan, were invited
to participate in this study. This accessed a convenience
sample of 265 students. In total, 265 questionnaires were
distributed to the nurses who attended classes over a 6-
week period. At the end of this period 170 completed
surveys were returned, giving a response rate of 64%.
4.2. Instrument
The instrument was based on the one developed by
Wallis et al. (2004). In this study a modified and
extended form of the Wallis et al. (2004) questionnaire
was translated into Chinese by the researcher and then
used to survey the participants. This questionnaire takes
10–15min to complete. It included 25 questions and
consisted of four sections. The first section included
multiple choice items related to socio-demographic and
professional characteristics. The second and third
sections asked about attitudes to and use of CAM,
respectively. Fifteen specific CAMs were referred to in
sections 2 and 3: Acupuncture, Aromatherapy, Art
therapy, Colour therapy, Feng Shui, Herbalism, homo-
eopathy, Hypnotherapy, Massage, Meditation, Music
therapy, Naturopathy, Osteopathy, Relaxation thera-
pies and Therapeutic touch. In addition in the ‘‘Other’’
category the respondents were prompted to include
other therapies such as Tai Chi, Gi Gong, and Yoga. In
the attitude section of the survey the respondents were
asked how strongly they agreed or disagreed with the
statement ‘‘this therapy can be helpful to clients involved
in mainstream healthcare’’. They were scored on a five
point Likert scale ranging from ‘‘Strongly agree’’ to
‘‘Strongly disagree’’. In the section of the survey that
dealt with use of CAM in practice the respondents were
asked to ‘‘circle the number that best describes the
frequency with which you would employ any of these
activities’’. This was scored on a six-point Likert scale
from ‘‘Never’’ to ‘‘More than once a day’’. There was
one open-ended question that asked respondents to
describe a typical activity that they might undertake
while doing any of these CAM practices. In section four
respondents were asked about organisational factors
and professional issues that influenced their use of CAM
in the workplace. They could select any number of
options from an extensive list and include their own
additional items.
This translation was then pilot tested with 5 Taiwa-
nese nurses. The pilot study data were not added to the
study results. Analysis of the pilot study indicated no
amendments were required.
4.3. Procedures
This study was approved by the administration of the
Taiwanese College. The data collectors negotiated with
lecturers from the College in Taiwan to arrange times
when they could attend classes to recruit nurses for the
study and to collect the data. They then met with the
nurses and described the study, at the beginning of a
lecture. The questionnaires were distributed and the
ARTICLE IN PRESS
Table 1
Demographic characteristics of nurses (N ¼ 170)
Characteristic Frequency Percent (%)
Gender
Males 2 1.2
Females 168 98.8
Age
25–30 76 44.7
31–35 52 30.6
36–40 29 17.1
41–45 8 4.7
46–50 3 1.7
51–55 2 1.2
Current appointed position
General registered nurse 79 46.5
Clinical nurse specialist 42 24.7
Nurse manager 33 19.4
Other 16 9.4
Year(s) in this position
0–5 82 48.2
5–10 58 34.2
10–15 24 14
15–20 3 1.8
20–25 2 1.2
F.-Y. Chu, M. Wallis / International Journal of Nursing Studies 44 (2007) 1371–13781374
nurses were given time to complete the questionnaire, in
the classroom. The questionnaires were then returned to
the data collectors. The nurses were advised that
participation was voluntary and that no member of
the college staff was involved with the research. In a
covering letter accompanying the self-report question-
naire, the participants were informed of their anonymity
if they participated and that completion of the
questionnaire implied consent. The subjects were ad-
vised to respond to the questions as openly as possible.
4.4. Data analysis
Descriptive statistics were used to describe the sample
characteristics and the study results. These included
frequencies, percentages, measures of central tendency
and ranges. Cross tabulations and the w2-test for
comparison of proportions were used to determine the
significance of differences in the use of CAM between
different groups of nurses. The Statistical Package for
the Social Sciences (SPSS version 11.0) was the
statistical package used for the analyses. The data, from
the open-ended question, were entered into a word-
processing program and the research team grouped the
descriptors related to each specific therapy.
25–30 0 0
30–35 1 0.6
Table 2
Frequencies and percentages of nurses working in different
settings (N ¼ 170)
Clinical setting Frequency Percent (%)
Medical/surgical 56 32.9
Critical /emergency care 30 17.7
Mental health 22 12.9
Community health 18 10.6
Paediatrics 11 6.5
Maternity (women’s health) 9 5.3
Pre and post operative 7 4.1
Aged care 5 2.9
Other 12 7.1
Total 170 100.0
5. Results
5.1. Demographic characteristics of sample
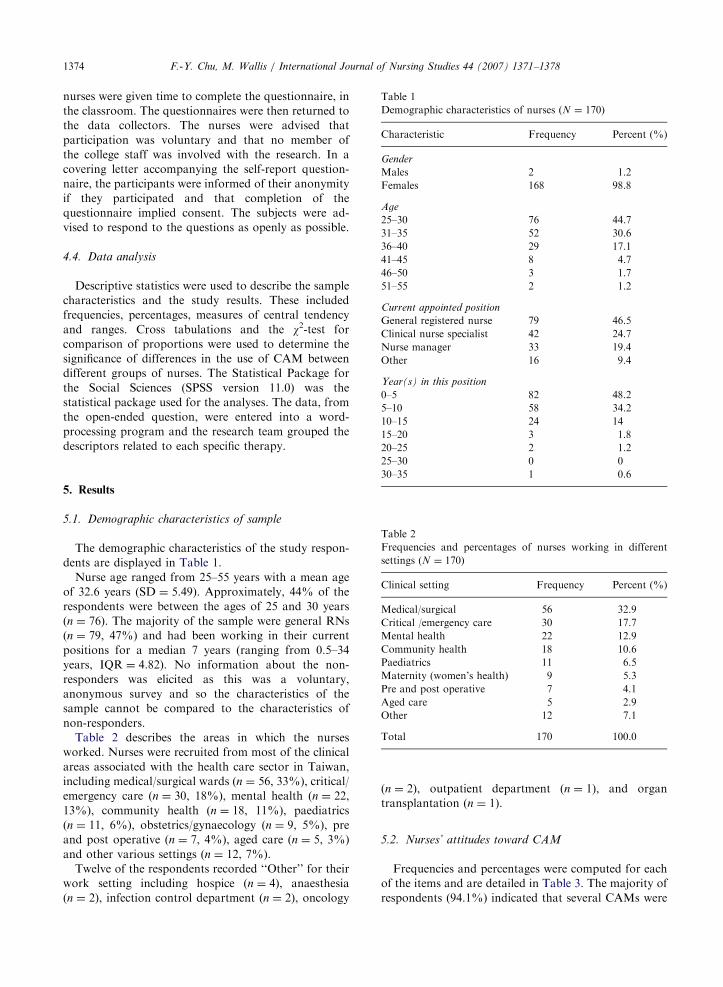
The demographic characteristics of the study respon-
dents are displayed in Table 1.
Nurse age ranged from 25–55 years with a mean age
of 32.6 years (SD ¼ 5.49). Approximately, 44% of the
respondents were between the ages of 25 and 30 years
(n ¼ 76). The majority of the sample were general RNs
(n ¼ 79, 47%) and had been working in their current
positions for a median 7 years (ranging from 0.5–34
years, IQR ¼ 4.82). No information about the non-
responders was elicited as this was a voluntary,
anonymous survey and so the characteristics of the
sample cannot be compared to the characteristics of
non-responders.
Table 2 describes the areas in which the nurses
worked. Nurses were recruited from most of the clinical
areas associated with the health care sector in Taiwan,
including medical/surgical wards (n ¼ 56, 33%), critical/
emergency care (n ¼ 30, 18%), mental health (n ¼ 22,
13%), community health (n ¼ 18, 11%), paediatrics
(n ¼ 11, 6%), obstetrics/gynaecology (n ¼ 9, 5%), pre
and post operative (n ¼ 7, 4%), aged care (n ¼ 5, 3%)
and other various settings (n ¼ 12, 7%).
Twelve of the respondents recorded ‘‘Other’’ for their
work setting including hospice (n ¼ 4), anaesthesia
(n ¼ 2), infection control department (n ¼ 2), oncology
(n ¼ 2), outpatient department (n ¼ 1), and organ
transplantation (n ¼ 1).
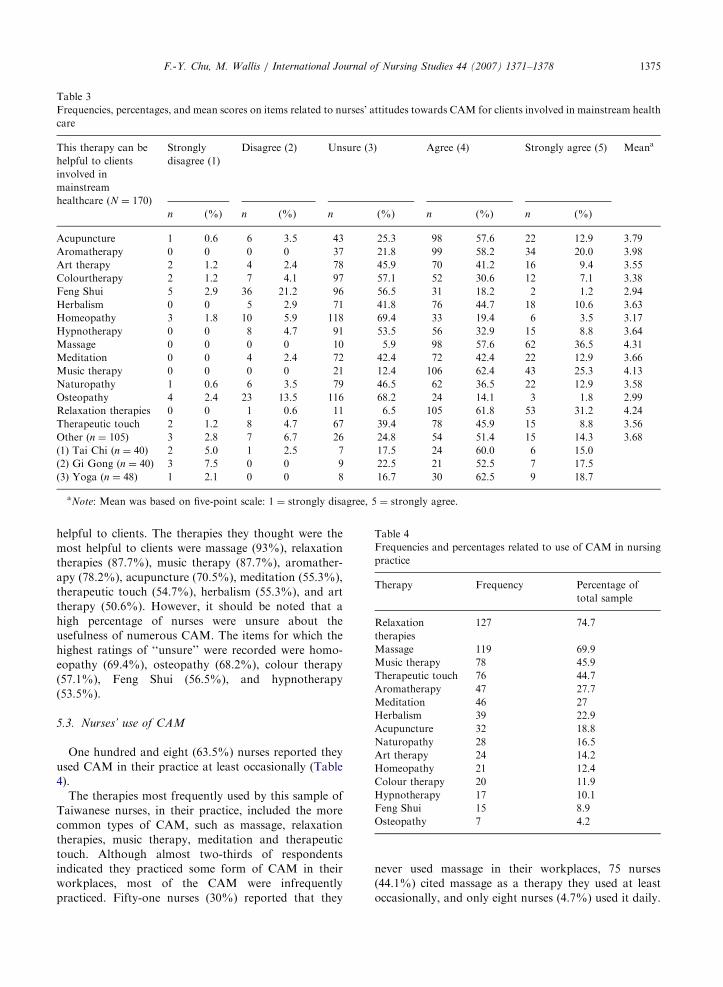
5.2. Nurses’ attitudes toward CAM
Frequencies and percentages were computed for each
of the items and are detailed in Table 3. The majority of
respondents (94.1%) indicated that several CAMs were
ARTICLE IN PRESS
Table 3
Frequencies, percentages, and mean scores on items related to nurses’ attitudes towards CAM for clients involved in mainstream health
care
This therapy can be
helpful to clients
involved in
mainstream
healthcare (N ¼ 170)
Strongly
disagree (1)
Disagree (2) Unsure (3) Agree (4) Strongly agree (5) Meana
n (%) n (%) n (%) n (%) n (%)
Acupuncture 1 0.6 6 3.5 43 25.3 98 57.6 22 12.9 3.79
Aromatherapy 0 0 0 0 37 21.8 99 58.2 34 20.0 3.98
Art therapy 2 1.2 4 2.4 78 45.9 70 41.2 16 9.4 3.55
Colourtherapy 2 1.2 7 4.1 97 57.1 52 30.6 12 7.1 3.38
Feng Shui 5 2.9 36 21.2 96 56.5 31 18.2 2 1.2 2.94
Herbalism 0 0 5 2.9 71 41.8 76 44.7 18 10.6 3.63
Homeopathy 3 1.8 10 5.9 118 69.4 33 19.4 6 3.5 3.17
Hypnotherapy 0 0 8 4.7 91 53.5 56 32.9 15 8.8 3.64
Massage 0 0 0 0 10 5.9 98 57.6 62 36.5 4.31
Meditation 0 0 4 2.4 72 42.4 72 42.4 22 12.9 3.66
Music therapy 0 0 0 0 21 12.4 106 62.4 43 25.3 4.13
Naturopathy 1 0.6 6 3.5 79 46.5 62 36.5 22 12.9 3.58
Osteopathy 4 2.4 23 13.5 116 68.2 24 14.1 3 1.8 2.99
Relaxation therapies 0 0 1 0.6 11 6.5 105 61.8 53 31.2 4.24
Therapeutic touch 2 1.2 8 4.7 67 39.4 78 45.9 15 8.8 3.56
Other (n ¼ 105) 3 2.8 7 6.7 26 24.8 54 51.4 15 14.3 3.68
(1) Tai Chi (n ¼ 40) 2 5.0 1 2.5 7 17.5 24 60.0 6 15.0
(2) Gi Gong (n ¼ 40) 3 7.5 0 0 9 22.5 21 52.5 7 17.5
(3) Yoga (n ¼ 48) 1 2.1 0 0 8 16.7 30 62.5 9 18.7
aNote: Mean was based on five-point scale: 1 ¼ strongly disagree, 5 ¼ strongly agree.
Table 4
Frequencies and percentages related to use of CAM in nursing
practice
Therapy Frequency Percentage of
total sample
Relaxation
therapies
127 74.7
Massage 119 69.9
Music therapy 78 45.9
Therapeutic touch 76 44.7
Aromatherapy 47 27.7
Meditation 46 27
Herbalism 39 22.9
Acupuncture 32 18.8
Naturopathy 28 16.5
Art therapy 24 14.2
Homeopathy 21 12.4
Colour therapy 20 11.9
Hypnotherapy 17 10.1
Feng Shui 15 8.9
Osteopathy 7 4.2
F.-Y. Chu, M. Wallis / International Journal of Nursing Studies 44 (2007) 1371–1378 1375
helpful to clients. The therapies they thought were the
most helpful to clients were massage (93%), relaxation
therapies (87.7%), music therapy (87.7%), aromather-
apy (78.2%), acupuncture (70.5%), meditation (55.3%),
therapeutic touch (54.7%), herbalism (55.3%), and art
therapy (50.6%). However, it should be noted that a
high percentage of nurses were unsure about the
usefulness of numerous CAM. The items for which the
highest ratings of ‘‘unsure’’ were recorded were homo-
eopathy (69.4%), osteopathy (68.2%), colour therapy
(57.1%), Feng Shui (56.5%), and hypnotherapy
(53.5%).
5.3. Nurses’ use of CAM
One hundred and eight (63.5%) nurses reported they
used CAM in their practice at least occasionally (Table
4).
The therapies most frequently used by this sample of
Taiwanese nurses, in their practice, included the more
common types of CAM, such as massage, relaxation
therapies, music therapy, meditation and therapeutic
touch. Although almost two-thirds of respondents
indicated they practiced some form of CAM in their
workplaces, most of the CAM were infrequently
practiced. Fifty-one nurses (30%) reported that they
never used massage in their workplaces, 75 nurses
(44.1%) cited massage as a therapy they used at least
occasionally, and only eight nurses (4.7%) used it daily.

ARTICLE IN PRESSF.-Y. Chu, M. Wallis / International Journal of Nursing Studies 44 (2007) 1371–13781376
Nevertheless, the most frequent daily use was related to
relaxation therapy (12.4%) and therapeutic touch
(11.8%).
The data from the open-ended question gave some
indication what nurses did when they engaged in the
CAM they reported using in practice. Forty-six respon-
dents (n ¼ 46=108, 42.5%) completed this question. The
activities they described included massage, relaxation
therapy, music therapy, and therapeutic touch. Nurses’
descriptions of massage included relieving symptoms
and providing comfort. For example: ‘stroking the
patient’s abdomen when the patient feels distended’,
‘stroking the infant’s body after bathing the baby’,
‘stroking the patient’s shoulder when the patient feels
sore’, ‘patient feels wound pain, stroking patient’s hands
and shoulder, let patient feel comfortable’. Another
description of relaxation therapies was very broad and
included such activities as ‘helping the patient take a
deep breath when patient feels pain and is uncomfor-
table’ and ‘holding patients’ hands and shoulder, told
patient to take a deep breath slowly’. The other
description of activities as music therapy were ‘turn on
the radio in the ward’, ‘provide Buddhist music if patient
requests’, and ‘encourage family to provide music’.
5.4. Factors influencing nurses’ use of CAM in practice
Although 63.5% (n ¼ 108) of the respondents re-
ported that they used CAM in their workplaces, 36.5%
(n ¼ 62) of nurses indicated they do not practice these
CAM in their workplaces. As shown in Table 5, there
were multiple reasons cited by nurses for not being able
to practice complementary therapy.
Table 5
Frequencies and percentages of reasons cited for not using
CAM (N ¼ 170)
Reason for not using
CAM
Frequencies (n) Percentage of
total sample
(%)
No organisational
resources
58 34.1
No organisational
policies
47 27.6
Never had access to
learning about CT
40 23.5
Not relevant 24 14.1
Lack confidence 21 12.4
Unsure 20 11.8
Unable to 19 11.2
Never wanted to learn 10 5.9
Don’t want to 8 4.7
NB: Using all data available from respondents (N ¼ 170),
recognising that multiple responses were permitted.
The most frequent reasons were lack of organisational
resources (34.1%), lack of organisational polices
(27.6%) and never having had access to learning about
CAM (23.5%). In addition, the majority of respondents
(41%) reported that they did not know whether there
were policies and procedures in their workplaces. One-
third of nurses in this study did not make any referrals
for clients related to their use of CAM.
5.5. Analysis of sub-group data
The sub-groups consisted of different age groups
(25–35, 36–45, and 46+), different work places (acute
versus non-acute settings—the acute care units in this
sample included medical/surgical ward, critical care,
paediatric, and maternity; the non-acute care units
included aged care, community health, and mental
health) and groups of different lengths of work
experience (o10 versus 10+ years). The results of these
analyses found there were no statistically significant
differences in the number of CAM used by nurses
working in acute care units versus chronic care units (w2
(df) ¼ 25.24 (1), p ¼ 0.113). Moreover, there were no
statistically significant differences in the use of comple-
mentary therapy by nurses’ age group (w2 (df) ¼ 3.87(2),
p ¼ 0.144). No association was found between work
experience and use of CAM. Nurses in this sample with
10 or more years of work experience compared to those
with less than 10 years of experience had no statistically
significant differences in the use of CAM (w2 (df) ¼ 1.06
(2), p ¼ 0.588).
6. Discussion
The nurses in this study reported that relaxation
therapies, massage, music therapy, therapeutic touch,
and aromatherapy were the therapies most often used in
their practice. These findings were similar to the findings
of Wallis et al. (2004), in Australia. While some studies
found that a considerable percentage of nurses use CAM
in their daily practice (Brolinson et al., 2001; King et al.,
2000; Wilkinson and Simpson, 2002), Taiwanese RNs in
this study, did not. Although 16.5% of nurses indicated
they used relaxation therapies at least daily or more than
daily, no nurses reported that they had completed
formal training or an accredited course in relaxation
therapies. These findings indicate that there is a lack of
formal training and /or inadequate foundation of
scientific knowledge provided by professional educa-
tional institutions. It should be noted that most nursing
schools in Taiwan do not include courses in CAM and
those that do frequently offer them on an elective basis
only. Thus, it is not surprising for the respondents of this
current study to indicate that they had difficulty ans-
wering questions about their professional responsibil-

ARTICLE IN PRESSF.-Y. Chu, M. Wallis / International Journal of Nursing Studies 44 (2007) 1371–1378 1377
ities related to CAM practice with the different
perspectives on use of CAM. These findings were also
consistent with the findings of Wallis et al. (2004).
While some CAM, such as massage, are within the
scope of practice of nurses in Taiwan, therapies such as
homoeopathy and naturopathy would be outside of the
scope of practice and nurses would need to be qualified,
have patient consent and be covered by health facility
policy before they could practice these therapies. Most
of the nurses in this study reported that they did not get
written, informed consent from their clients when
engaging in CAM. Only one nurse reported she got
verbal, informed consent from patients when practicing
CAM. Accordingly, providing CAM to patients without
informed consent may jeopardise patient care and
conflict with practice regulations. In this current study,
only one nurse reported membership of a professional
association related to a complementary therapy (Ar-
omatherapy Association of Taiwan). However, even this
nurse did not have an accredited qualification for
aromatherapy.
CAM is generally not available to patients in
Taiwanese hospitals, except acupuncture. In the Taiwa-
nese health care system, acupuncture therapy is a part of
Traditional Chinese Medicine and is provided by
professional Chinese Medicine doctors. It is not
legitimate for nurses to provide acupuncture therapy in
Taiwan, because acupuncture therapy is viewed as an
invasive therapy. Providing such a service raises
indemnity, legal and ethical issues and there should be
explicit policy direction (Wallis et al., 2004).
In previous studies (DeKeyser et al., 2001; Fearon,
2003; Munstedt et al., 2000; Risberg et al., 2004), age
and gender were found to be associated with attitudes
towards CAM. However, age and gender sub-group
analysis in this study revealed no such differences. This
is probably due to the fact that the majority of nurses in
this study were female and aged between 25 and 35
years. This demographic reflects the general population
of nurses in Taiwan but the lack of variability
compromises sub-group analysis. Accordingly, the
homogeneity of this sample in this study could not be
used to determine whether these demographic data were
associated with differences in attitudes towards CAM.
7. Limitations of the study
Although this current study achieved a good response
rate (64%), a few limitations of the study must be
considered when interpreting its findings. First, the
study used a small convenience sample of nurses from
one participating Nursing College, and therefore, does
not represent the general nursing population in Taiwan.
Second, the study was cross-sectional in design, thus no
cause and effect relationship can be drawn from the
results. Sampling bias may also have occurred as nurses
who were positive in their attitudes to CAM may have
self-selected into the study. Third, the questionnaire did
not cover all aspects of attitude towards CAM, focusing
specifically on the helpfulness of therapies for clients in
mainstream health care. Other constructs related to
safety, efficacy and appropriateness were not covered in
this study. This limits the interpretation of the results to
the individual items, rather than reporting on a
psychometric instrument measuring all dimensions of
the construct of attitude. In addition, only a few of the
possible socio-demographic variables that could affect
attitude were included in this study. Future studies could
look at cross-cultural factors and religion as possible
mediators of attitude to CAM.
8. Conclusion and recommendations
This study demonstrated that Taiwanese nurses
engaged in further education have a positive attitude
toward CAM. Since there has been a lack of previous
studies performed in Taiwan with Registered Nurses
related to CAM, the results of this study provide
information for nursing practice and nursing education.
The results of this study suggest that while most
Taiwanese nurses believed CAM were a valuable adjunct
to conventional therapies and help to provide holistic
care for patients, few used CAM in their daily practice
because of a lack of organisational policies, resources
and professional education.
With the increasing rate of CAM use in Taiwan,
further research should continue to focus on important
issues in CAM practice and nursing education. More-
over, the efficacy and safety of various CAM used in
nursing practice needs to be investigated through an
evidenced-based approach.
Acknowledgments
We gratefully acknowledge the nurses who partici-
pated in the study. Special thanks are given to
Ms Pei-Ying Tan, Ms Chu-Yan Chen, and Ms Jiu-
Hua Huang for their assistance with questionnaire
distribution.
References
Baldwin, C.M., Long, K., Kroesen, K., Brooks, A.J., Bell, I.R.,
2002. A profile of military veterans in the southwestern
United States who use complementary and alternative
medicine: implications for integrated care. Archives of
Internal Medicine 162 (15), 1697–1704.

ARTICLE IN PRESSF.-Y. Chu, M. Wallis / International Journal of Nursing Studies 44 (2007) 1371–13781378
Botting, D.A., Cook, R., 2000. Complementary medicine:
knowledge, use and attitudes of doctors. Complementary
Therapies in Nursing and Midwifery 6 (1), 41–47.
Brolinson, P.G., Price, J.H., Ditmyer, M., Reis, D., 2001.
Nurses’ perceptions of complementary and alternative
medical therapies. Journal of Community Health 26 (3),
175–189.
Cassileth, B.R., Deng, G., 2004. Complementary and alter-
native therapies for cancer. Oncologist 9 (1), 80–89.
Chang, L.C., Li, I.C., 2004. Patterns of complementary therapy
use by homebound cancer. Applied Nursing Research 17
(1), 41–47.
DeKeyser, F.G., Bar Cohen, B., Wagner, N., 2001. Knowledge
levels and attitudes of staff nurses in Israel towards
complementary and alternative medicine. Journal of Ad-
vanced Nursing 36 (1), 41–48.
Fearon, J., 2003. Complementary therapies: knowledge and
attitudes of health professionals. Paediatric Nursing 15 (6),
31–35.
Frenkel, M.A., Borkan, J.M., 2003. An approach for integrat-
ing complementary-alternative medicine into primary care.
Family Practitioner 20 (3), 324–332.
Hayes, K.M., Alexander, I.M., 2000. Alternative therapies and
nurse practitioners: Knowledge, professional experience,
and personal use. Holistic Nursing Practice 14 (3), 49–58.
Hessig, R.E., Arcand, L.L., Frost, M.H., 2004. The effects of an
educational intervention on oncology nurses’ attitude,
perceived knowledge, and self-reported application of
complementary therapies. Oncology Nurses Forum 31 (1),
71–78.
King, M.O., Pettigrew, A.C., Reed, F.C., 2000. Complemen-
tary, alternative, integrative: have nurses kept pace with
their clients? Dermatology Nursing 12 (1), 41–44, 47–50.
Leung, J.M., Dzankic, S., Manku, K., Yuan, S., 2001. The
prevalence and predictors of the use of alternative medicine
in presurgical patients in five California hospitals. Anesthe-
sia and Analgesia 93 (4), 1062–1068.
Lin, S.C., 1999. Alternative medicine in hospice care. Taiwan
Journal of Hospice Palliative 11, 43–50.
Lindquist, R., Tracy, M.F., Savik, K., Watanuki, S.,
2005. Regional use of complementary and alternative
therapies by critical care nurses. Critical Care Nurse 25
(2), 63–75.
McDowell, J.E., Burman, M.E., 2004. Complementary and
alternative medicine: a qualitative study of beliefs of a small
sample of Rocky Mountain area nurses. Medsurg Nursing:
Official Journal of the Academy of Medical-Surgical Nurses
13 (6), 383–390.
Munstedt, K., Entezami, A., Wartenberg, A., Kullmer, U.,
2000. The attitudes of physicians and oncologists towards
unconventional cancer therapies (UCT). European Journal
of Cancer 36 (16), 2090–2095.
National Centre for Complementary and Alternative Medicine,
2002. Get the facts: what is complementary and alternative
medicine ? Retrieved May 12, 2005 from http://www.
nccam.nih.gov/health/whatiscam/index.htm
Risberg, T., Kolstad, A., Bremnes, Y., Holte, H., Wist, E.A.,
Mella, O., Klepp, O., Wilsgaard, T., Cassileth, B.R., 2004.
Knowledge of and attitudes toward complementary and
alternative therapies: a national multicentre study of
oncology professionals in Norway. European Journal of
Cancer 40 (4), 529–535.
Sohn, P.M., Loveland Cook, C.A., 2002. Nurse practitioner
knowledge of complementary alternative health care:
foundation for practice. Journal of Advanced Nursing 39
(1), 9–16.
Thomas, K.J., Nicholl, J.P., Coleman, P., 2001. Use and
expenditure on complementary medicine in England: a
population based survey. Complementary Therapy in
Medicine 9 (1), 2–11.
Tracy, M.F., Lindquist, R., Watanuki, S., Sendelbach, S.,
Kreitzer, M.J., Berman, B., Savik, K., 2003. Nurse attitudes
towards the use of complementary and alternative therapies
in critical care. Heart & Lung: Journal of Acute and Critical
Care 32 (3), 197–209.
Wallis, M., Peerson, A., Young, J., Parkinson, S., Grant, S.,
2004. Nurses’ utilisation of complementary therapies: a pilot
study exploring scope of practice. Collegian 11 (4), 19–25.
Wilkinson, J.M., Simpson, M.D., 2002. Personal and profes-
sional use of complementary therapies by nurses in NSW,
Australia. Complementary Therapies in Nursing and Mid-
wifery 8, 142–147.