-
Thyroid & Parathyroid Gland
-
Regulasi Aksis TiroidPENDREDSYNDROME
-
Iodine +Tyrosil ResiduesIodidePeroxidasePLASMAFOLLICULAR
CELLCOLLOIDIodideDietary IodideTraping Iodine + Tyrosil ResiduesMIT
+ DITT4 + T3 Thyroglobulin Deiodo- TyrosinaseMIT + DITT4 + T3T4 +
T3 ThyroglobulinT4 T3MIT DITProtease
-
Thyroid Disease Can Have Widespread EffectsThyroidIncreased LDL
CholesterolElevated TriglyceridesLiverConstipationDecreased GI
Activity IntestinesDecreased FertilityMenstrual AbnormalitiesMay
Harm Development of Infant
ReproductiveSystemDepressionDecreased ConcentrationGeneral Lack
of InterestBrainDecreased Heart RateIncreased/Decreased Blood
PressureDecreased Cardiac OutputHeartDecreased FunctionFluid
Retention and EdemaKidneysHypohyroidism AffectsMany Body Systems
and Overall Health
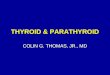
- Prevalence of Elevated Serum TSH by Decade of Age and
GenderAt
-
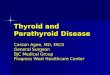
Prevalence of Abnormal Thyroid FunctionThe Colorado Thyroid
Disease Prevalence study Used thyroid stimulating hormone (TSH)
levels as a measure of thyroid functionPrevalence of elevated TSH
levels (hypothyroidism) was 9.5% and the prevalence of decreased
TSH levels (hyperthyroidism) was 2.2%Lipid levels increased as
thyroid function declined40% of patients taking thyroid medications
had abnormal TSH levelsCanaris GJ, et al. Arch Intern Med.
2000;160:526-534.
-
McDermot MT and Ridgway EC. J Clin Endocrinol Metab
86:4585-4590
-
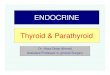
1%10%1%13%NHANES* (2002)NA12%Rotterdam (1993)3%16%4%21%Colorado*
(2000)2.3%5.9%Framingham (1987)3%8%Whickham follow-up
(1995)MenWomenStudySawin CT, et al. Arch Intern Med.
1985;145:1386-1388.Vanderpump MP et al. Clin Endocrinol (Oxf).
1995;43:55-68. Canaris GJ, et al. Arch Intern Med. 2000;
160:526-534.Hak AE, et al. Ann Intern Med.
2000;132:270-278.Hollowell JG, et al. J Clin Endocrinol Metab.
2002;87:489-499.Prevalence of Elevated TSH by Gender*Percentage
calculated by decade of life.
-
Thyroid-Stimulating Hormone (TSH) AssaysKey test for diagnosis
of hypothyroidism and hyperthyroidismTSH assay sensitivity has
improved with subsequent test generationsFirst generation: RIA
Sensitivity: 1.0 IU/mLSecond generation: IRMASensitivity: 0.1
IU/mLThird generation: ELISASensitivity: 0.03 IU/mLLadenson PW, et
al. Arch Intern Med. 2000;160:1573-1575.Braverman LE, et al. Werner
& Ingbars The Thyroid. A Fundamental and Clinical Text. 8th ed.
2000.Zophel K, et al. Nuklearmedizin. 1999;38:150-155.
- Thyroid Disease Spectrum0105TSH, IU/mLMild Thyroid FailureTSH
>4.0 IU/mL, Free T4 NormalOvert HypothyroidismTSH >4.0 IU/mL,
Free T4 LowEuthyroidTSH 0.4-4.0 IU/mL, Free T4
NormalThyrotoxicosisTSH
-
Screening for Thyroid Dysfunction Recommendations for
Asymptomatic AdultsOrganizationAmerican Thyroid Association
American Association ofClinical Endocrinologists
American College ofPhysiciansScreening RecommendationWomen and
men >35 years of age should be screened and every 5 years
later
Older patients, especially women, should be screened
Women >50 years of age with an incidental finding suggestive
of symptomatic thyroid disease should be evaluatedLadenson PW, et
al. Arch Intern Med. 2000;160:1573-1575.Cooper DS. N Engl J Med.
2001;345:260-265.Ann Intern Med. 1998;129:141-143.
-
Additional Laboratory Tests for Thyroid FunctionTestNormal
LevelsWhen to UseSerum total T45-11 g/dLBound and free T4; use with
TSH for diagnosis
Free T40.7-1.8 ng/dLUse with TSH to assess degree of
hypothyroidism
TPOAb, TgAbNegativeIn combination with TSH, predictor of disease
progressionEndocr Pract. 2002;8:457-469.Braverman LE, et al. Werner
& Ingbars The Thyroid. A Fundamental and Clinical Text. 8th ed.
2000.Demers LM, Spencer CA, eds. The National Academy of Clinical
Biochemistry Web site. Available at:
http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed July 1,
2003.
-
Goals for Treating Thyroid DiseaseHypothyroidismRestore thyroid
hormones to normal levelsLevothyroxine sodium is the treatment of
choice HyperthyroidismRestore a eumetabolic state3 treatments
available: antithyroid drugs, radioactive iodine (131I), and
thyroid surgerySinger PA, et al. JAMA. 1995;273:808-812.
-
Types of HypothyroidismPrimary hypothyroidism: caused by
decreased production of T4 and T3 due to thyroid
dysfunctionSecondary hypothyroidism: caused by decreased thyroidal
stimulation by TSH; may be caused by pituitary (TSH) or
hypothalamic (TRH) diseaseBraverman LE, et al. Werner & Ingbars
The Thyroid. A Fundamental and Clinical Text. 8th ed. 2000.
-
Causes of primary hypothyroidismCommonAutoimmune lymphocytic
thyroiditis (Hahimoto)RadioiodineThyroid surgeryDrugs: antithyroid
drugs (PTU,Crbimazole),amiodarone,
lithium.RareInfiltrationDysgensisThyroid hormone resistanceIodine
deficiencyIodine excess (Wolff-Chaikoff effect)Chew and Leslie.
Clinical Endocrinology and Daiabetes,2006
-
Clinical Manifestations of HypothyroidismFatigueWeight gain Dry
skin and cold intolerance Yellowing or yellow hue of the skin
Coarseness or loss of hair HoarsenessGoiterDelayed relaxation of
deeptendon reflexesAtaxia Braverman LE, et al. Werner & Ingbars
The Thyroid. A Fundamental and Clinical Text. 8th ed.
2000.ConstipationMemory and mental impairment Decreased
concentration Depression Irregular or heavy menses and
infertilityMyalgiasHyperlipidemiaBradycardia and
hypothermiaMyxedema
-
Cholesterol Levels Elevate With Increasing TSH LevelsCanaris GJ,
et al. Arch Intern Med.
2000;160:526-534.209216223226229238239270267200210220230240250260270280Mean
Total Cholesterol Level,
mg/dL5.1-10>10-15>15-20>20-40>40-60>60-80>80TSH,
IU/mLAbnormalEuthyroid
- Correlation of Serum TSH and Cholesterol in Hypothyroid
PatientsPatients (n)TSH Range (IU/mLMean Cholesterol (mg/dL)390 1.1
to 5.0231130 5.1 to 10.0244*13010.1 to 15.0252* 8115.1 to
20.0248*11520.1 to 40.0260* 9940.1 to 80.0310* 73
>80.0347**Statistically significantly (P
-
Hypothyroidism and DepressionHave Many Common
FeaturesDepressionHypothyroidism Sleep decrease Suicidal ideation
Weight loss Appetite increase/ decreaseNemeroff CB, J Clin
Psychiatry. 1989;50(suppl):13-20. Bradycardia Cardiac and
lipidabnormalities Cold intolerance Delayed reflexes Goiter Hair
and skin changes Constipation Appetite decrease Decreased
concentration Decreased libido Delusions Depressed mood Diminished
interest Sleep increase Weight increase Fatigue
-
Hypothyroidism Treatment Goal EuthyroidismThe goal of
hypothyroidism therapy is to replace thyroxine to mimic normal,
physiologic levels and alleviate signs, symptoms, and biochemical
abnormalities
Braverman LE, et al. Werner & Ingbars The Thyroid. A
Fundamental and Clinical Text. 8th ed. 2000.
-
Treatment of Hypothyroidism Thyroid Hormone ReplacementTreatment
of choice: levothyroxine (synthetic levothyroxine, LT4)Chemically
stableT4 converted to T3 in peripheryOther therapies (T3 or T3 and
T4 mixtures)Thyroid USP, liothyronine, liotrix, thyroglobulinSome
disadvantages, no advantages versus levothyroxineSinger PA, et al.
JAMA. 1995;273:808-812.Endocr Pract. 2002;8:457-469.Braverman LE,
et al. Werner & Ingbars The Thyroid. A Fundamental and Clinical
Text. 8th ed. 2000.
-
Recommendations for Treatment of HypothyroidismAACE
guidelines:AACE advocates the use of a high-quality brand
preparation of levothyroxine. It is preferable to maintain the
patient on the same brand of levothyroxine throughout
treatment.Importantly, patients should be reevaluated and
retitrated after an interval of at least 6 weeks following any
change in levothyroxine brand or dose.American Thyroid Association
recommendations:For patients who have recently started receiving
levothyroxine or who have had their dosage, type, or brand of
thyroid preparation changed, the TSH concentration should be
measured after 8 to 12 weeks.Endocr Pract. 2002;8:457-469.Singer
PA, et al. JAMA. 1995;273:808-812.
-
Diagnosis Algorithm for Hypothyroidism TSH0.4 to 4.0
IU/mLPatientEuthyroidTSH4.0 IU/mLGo to Next StepSinger PA, et al.
JAMA. 1995;273:808-812.Demers LM, Spencer CA, eds. The National
Academy of Clinical Biochemistry Web site. Available at:
http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed July 1,
2003.SuspectHypothyroid?Test TSH
-
Primary Hypothyroidism Diagnosis AlgorithmTSH >4.0 IU/mLTest
FT4 *Free T4 estimateDemers LM, Spencer CA, eds. The National
Academy of Clinical Biochemistry Web site. Available at:
http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed July 1,
2003.Ayala AR, et al. Cleve Clin J Med. 2002;69:313-320.Ayala AR,
et al. The Endocrinologist. 1997;7:44-50.Endocr Pract.
2002;8:457-469.
- Hypothyroidism TreatmentLevothyroxine sodium is the treatment
of choice for the routine management of hypothyroidismAdults: about
1.7 g/kg of body weight/dChildren up to 4.0 g/kg of body
weight/dElderly
- Primary Hypothyroidism Treatment AlgorithmTSH >4
IU/mLTSH
-
Therapy Initiation and TitrationTherapy with levothyroxine
sodium products requires individualized patient dosingCareful
titration: use a formulation with consistent dosesClinical
evaluation: symptoms resolve more slowly than TSH
responseLaboratory monitoring: need consistent, sensitive TSH
measurements
Individualized patient dosing is influenced byAge and
weightCardiovascular healthSeverity and duration of
hypothyroidismConcomitant disease states and treatmentEndocr Pract.
2002;8:457-469.Singer PA, et al. JAMA. 1995;273:808-812.
-
Therapy MonitoringClinical and laboratory monitoring
enableEvaluation of the clinical responseAssessment of patient
complianceAssessment of drug interactions, if applicableAdjustment
of dosage, as neededClinical and laboratory evaluations should be
performed At 6- to 8-week intervals while titratingAnnually once a
euthyroid state is establishedSinger PA, et al. JAMA.
1995;273:808-812. Demers LM, Spencer CA, eds.Demers LM, Spencer CA,
eds. The National Academy of Clinical Biochemistry Web site.
Available at: http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed
July 1, 2003.
-
Special Considerations Elderly PatientsHigher prevalence of
hypothyroidism compared with younger personsAppropriate dose
selection and monitoring critical for elderly patients with cardiac
abnormalitiesPoor patient compliance, adherence, and persistence
may be an issueFelicetta JV. Consultant. 2002;1597-1606. Available
at: www.consultantlive.com. Accessed July 1, 2003.
- Caution in Patients With Underlying Cardiac DiseaseUsing LT4 in
those with ischemic heart disease increases the risk of MI,
aggravation of angina, or cardiac arrhythmiasFor patients
-
Impact of Maternal Hypothyroidism on Subsequent
Neuropsychological Development of OffspringUndiagnosed
hypothyroidism in pregnant women may adversely affect
fetusesTreating maternal hypothyroidism during pregnancy appears to
be beneficial, even when treatment falls short of euthyroid
statusScreening for hypothyroidism before or very early in
pregnancy may be warrantedHaddow JE, et al. N Engl J Med.
1999;341:549-555.
-
Special Considerations Levothyroxine Therapy With Other
PopulationsPregnant womenThyroid failure may impede the
intellectual development of the childIncreased LT4 doses may be
necessaryTSH levels should be monitored each trimesterPostpartum
thyroiditisCan lead to symptomatic thyrotoxicosis and/or
hypothyroidismReported prevalence varies from 2% to 21%Has been
associated with postpartum depressionCan lead to chronic
hypothyroidismSynthroid [package insert]. Abbott Laboratories;
2003.Braverman LE, et al. Werner & Ingbars The Thyroid. A
Fundamental and Clinical Text. 8th ed. 2000.
-
Treating Hypothyroidism Before and During PregnancyEncourage
adherence with levothyroxine replacement therapy before
conceptionMonitor TSH levels before conception and during first
trimesterIncrease the levothyroxine dosage in athyreotic patients
by 25%-50% when pregnancy is confirmedMonitor TSH levels every 6 to
8 weeks throughout pregnancyReinstate prepregnancy levothyroxine
dosage immediately following deliveryGharib H, et al. Endocr Pract.
1999;5:367-368.Mandel SJ, et al. N Engl J Med. 1990;323:91-96.
-
Subclinical HypothyroidismTreatments
-
Subclinical HypothyroidismPrevalenceWorldwide prevalence between
1% and 10%Highest rates are in women older than 60 years of ageOver
the age of 74, 16% of men and 21% of women have the disorderCooper
DS. N Engl J Med. 2001;345:260-264.
-
Prevalence and Incidence of Subclinical
HypothyroidismPrevalence4% to 10% in large population screening
surveysIncreases with increasing ageIs more common in women than in
menIncidence2.1% to 3.8% per year in thyroid antibody-positive
patients0.3% per year in thyroid antibody-negative patients
McDermott MT, et al. J Clin Endocrinol Metab.
2001;86:4585-4590.Caraccio N, et al. J Clin Endocrinol Metab.
2002;87:1533-1538.Biondi B, et al. Ann Intern Med.
2002;137:904-914.
-
Definition of Subclinical HypothyroidismElevated TSH level
(>4.0 IU/mL)Normal total or free serum T4 and T3 levelsFew or no
signs or symptoms of hypothyroidismMcDermott MT, et al. J Clin
Endocrinol Metab. 2001;86:4585-4590.Braverman LE, Utiger RD, eds.
The Thyroid: A Fundamental and Clinical Text. 8th ed. Philadelphia,
Pa: Lippincott, Williams & Wilkins; 2000;1001.
-
50403020100Participants, %01234Number of SymptomsEuthyroidMild
Thyroid FailureHypothyroid>35%>25%Many Patients With
Hypothyroidism Report No Symptoms Canaris GJ, et al. Arch Intern
Med. 2000;160:526-534.Ladenson PW, et al. Arch Intern Med.
2000;160:1573-1575.
-
Causes of Subclinical HypothyroidismExogenous
factorsLevothyroxine underreplacementMedications, such as lithium,
cytokines, or iodine-containing agents (eg, amiodarone)Antithyroid
medications131I therapy or thyroidectomyEndogenous factorsPrevious
subacute or silent thyroiditis Hashimoto thyroiditisBiondi B, et
al. Ann Intern Med. 2002;137:904-914.
-
Subclinical Hypothyroidism and Cardiovascular DiseaseCardiac
manifestationsLeft ventricular systolic and diastolic
dysfunctionIncreased systolic time intervalMyocardial
infarctionCoronary artery diseaseElevated total cholesterol levels,
LDL-C levels, and triglyceride levelsAortic
atherosclerosisHyperhomocysteinemiaBiondi B, et al. Ann Intern Med.
2002;137:904-914.Ayala AR, et al. Cleve Clin J Med.
2002;69:313-320.Aldin V, et al. Am Fam Physician.
1998;57:776-780.
-
Subclinical Hypothyroidism and Aortic Atherosclerosis in
WomenPresence of Aortic AtherosclerosisHak AE, et al. Ann Intern
Med. 2000;132:270-278.Women With Mild Thyroid
FailureEuthyroidWomenWomen With Mild Thyroid Failure and Antibodies
to Thyroid PeroxidaseEuthyroid Women Without Antibodies to Thyroid
Peroxidase
-
Subclinical Hypothyroidism Affects Cardiac FunctionCardiac
function is subtly impaired in patients with mild thyroid
failureAbnormalities can include Subtle abnormalities in systolic
time intervals and myocardial contractilityDiastolic dysfunction at
rest or with exerciseReduction of exercise-related stroke volume,
cardiac index, and maximal aortic flow velocityThe clinical
significance of the changes is unclearMcDermott MT, et al. J Clin
Endocrinol Metab. 2001;86:4585-4590.Braverman LE, Utiger RD, eds.
The Thyroid: A Fundamental and Clinical Text. 8th ed. Philadelphia,
Pa: Lippincott, Williams & Wilkins; 2000:1004.
-
Subclinical Hypothyroidism May Increase Cardiovascular Disease
RiskMild thyroid failure has been evaluated as a cardiovascular
risk factor associated withIncreased serum levels of total
cholesterol and low-density lipoprotein cholesterol (LDL-C)
levelsReduced high-density lipoprotein cholesterol (HDL-C)
levelsIncreased prevalence of aortic atherosclerosisIncreased
incidence of myocardial infarction
-
The Rotterdam Study Design and ObjectivesA population-based
cross-sectional cohort study conducted in a district of Rotterdam,
the NetherlandsCohort included 3105 men and 4878 women aged 55 and
olderThyroid status was determined from a random sample of 1149
elderly women (mean age 69 7.5 years) selected from the studyThe
study's objective was to investigate whether mild thyroid failure
and thyroid autoimmunity are associated with aortic atherosclerosis
and myocardial infarction
-
Subclinical Hypothyroidism Increases Risk of Myocardial
Infarction (MI)Findings from the Rotterdam StudySubclinical
Hypothyroidism contributed to 60% of MI cases in patients with
diagnosed subclinical hypothyroidism, and 14% of all MI instances
in the study populationSubclinical Hypothyroidism appeared to be a
strong indicator of risk for aortic atherosclerosis and MI in older
womenThyroid autoimmunity by itself was not associated with aortic
atherosclerosis or MIHak AE, et al. Ann Intern Med.
2000;132:270-278.
-
Subclinical Hypothyroidism Elevates Serum Lipid LevelsCanaris
GJ, et al. Arch Intern Med. 2000;160:526-534.*Total-C indicates
total cholesterol; LDL-C, LDL-Cholesterol; HDL-C,
HDL-Cholesterol050100150200250300Lipid Levels, mg/dLTotal-C*
LDL-C*HDL-C*Triglycerides
-
Potential benefits from treatmentPrevent progression to overt
hypothyroidismImprove serum lipid profile, which may reduce the
risk of death from cardiovascular causesReduce symptoms, including
psychiatric and cognitive abnormalitiesCooper DS. N Engl J Med.
2001;345:260-264.Rationale for Treating Mild Thyroid Failure
-
Mild Thyroid Failure Treated With Levothyroxine Therapy: Effects
on Total Cholesterol-40-35-30-25-20-15-10-50Gorman etal, 1979Elder
et al,1990Wiseman et al,1993 Change in Total Cholesterol (mg/dL),
%Tanis BC, et al. Clin Endocrinol. 1996;44:643-649.
-
Levothyroxine Therapy Reduces Cholesterol in Subclinical
HypothyroidismTSHTotal CholesterolLDL-C02468101214TSH
(IU/mL)LT4Placebo230240250PlaceboTC (mg/dL)140145150155LDL-C
(mg/dL)Meier C, et al. J Clin Endocrinol Metab.
2001;86:4860-4866.Basel Thyroid Study (N=63)PlaceboLT4LT4
-
The Rate of Progression of Subclinical Hypothyroidism to Overt
HypothyroidismSubclinical Hypothyroidism is a common disorder that
frequently progresses to overt hypothyroidismProgression has been
reported in about 3% to 18% of affected patients per
yearProgression may take years or may rapidly occurThe rate is
greater if TSH is higher or if there are positive antithyroid
antibodiesThe rate may also be greater in patients who were
previously treated with radioiodine or surgery
-
Treatment of subclinical hypothyroidism Whether to treat
subclinical hypothyroidism remains a dilemma.Most clinicians treat
subclinical hypothyroidism who have a serum TSH > 10 mIU/L.
Whereas opinions differ about the management of mild disease in
which TSH ranges between 4.5 10 mIU/L especially in elderly
asymptomatic patients
Biondi and Cooper Endocrine Reviews. 2008 ; 29:76-131
-
Factors That May Reduce Levothyroxine EffectivenessMalabsorption
SyndromesPostjejunoileal bypass surgeryShort bowel syndromeCeliac
diseaseReduced AbsorptionColestipol hydrochloride SucralfateFerrous
sulfateFood (eg, soybean formula)Aluminum
hydroxideCholestyramineSodium polystyrene sulfonateDrugs That
Increase ClearanceRifampinCarbamazepinePhenytoinFactors That
Reduced T4 to T3 ClearanceAmiodaroneSelenium deficiencyOther
MechanismsLovastatinSertraline Braverman LE, Utiger RD, eds. The
Thyroid: A Fundamental and Clinical Text. 8th ed. 2000.Synthroid
[package insert]. Abbott Laboratories; 2003.
-
Thyroid Status of Treated PatientsCanaris GJ, et al. Arch Intern
Med. 2000;160:526-534.020406080100Participants,
%HyperthyroidSubclinicalHyperthyroid 0.9
20.7>20%SubclinicalHypothyroidHypothyroid 17.6
0.7Undertreated>18%Colorado Thyroid Disease Prevalence Study
-
Under-Replacement RisksSwitching between different levothyroxine
formulations can lead to under-replacementUnder-replacement risk
(TSH >5.0 IU/mL)Continued hypothyroid
stateHyperlipidemiaDecreased heart rate and ventricular
contractilityIncreased peripheral vascular resistance and diastolic
pressureMemory loss, fatigue, and weight gainDepression
- Over-Replacement RisksSwitching a narrow therapeutic index
drug, such as LT4, without retesting and retitrating can cause
inconsistent TSH control, resulting in over-replacement
Over-replacement risks (TSH
-
SummaryHypothyroidism increases in prevalence and incidence
among the elderly.Autoimmune thyroiditis is the most common cause
of hypothyroidism Levothyroxine sodium is the treatment of choice
for the routine management of hypothyroidismTreatment and
management of subclinical hypothyroidism and population screening
are still controversialSpecial considerations may apply in planning
treatment due to changes in the metabolic clearance of thyroid
hormone, drug interactions and potential adverse reaction
-
Parathyroid Hormone (PTH)Is an 84 aminoacid chain, but its
biologically activity resides in the first 34 residues.In the
parathyroid gland, a Pre-Pro-PTH are synthesizedPre-Pro-PTH is
converted to Pro-PTH and Pro-PTH converted to PTH.When serum
Calcium level falls, signal is transduced through calcium sensing
receptors, and secretion of PTH increased.
-
Principles of Human Anatomy and Physiology, 11e*PARATHYROID
GLANDSThe parathyroid glands are embedded on the posterior surfaces
of the lateral lobes of the thyroid principal cells produce
parathyroid hormoneoxyphil cells function is unknown Parathyroid
hormone (PTH) regulates the homeostasis of calcium and phosphate
increase blood calcium leveldecrease blood phosphate levelincreases
the number and activity of osteoclastsincreases the rate of Ca+2
and Mg+2 from reabsorption from urine and inhibits the reabsorption
of HPO4-2 so more is secreted in the urinepromotes formation of
calcitriol, which increases the absorption of Ca+2, Mg+2,and HPO4-2
from the GI tract
-
Principles of Human Anatomy and Physiology, 11e*Histology of
Parathyroid GlandPrincipal cells produce parathyroid hormone
(PTH)Oxyphil cell function is unknown
-
Biologic Effects of PTH The central function of PTH is to
regulate ionized ( Ca2+) levels by concerted effects on three
principal target organ :BoneIntestinal mucosa KidneyThe effect of
PTH on intestinal calcium absorpsion is indirect, resulting from
increased renal production of the intestinally active vitamin D
metabolite 1,25(OH)2D. By its integrated effects on kidney, gut and
bone PTH acts to increased the flow of calcium into the
extracellular fluid and thus defend against hypocalcemia. Removal
of the parathyroid glands results in profound hypocalcemia and
ultimately in tetani and death
Principles of Human Anatomy and Physiology, 11e*
-
Figure 1813
-
Principles of Human Anatomy and Physiology, 11e*Regulation of
Calcium Blood LevelsHigh or low blood levels of Ca+2 stimulate the
release of different hormones --- PTH or Calcitonin
-
Biosynthesis, Storage & Secretion of PTH PTH is synthesized
as the preprohormone (Preproparathyroid Hormone) by parathyroid
gland chief cells The active form of PTH is cleaved from the
preprohormone before release from the gland PTH is synthesized
continously (it is either released from the gland or degraded)PTH
is released by exocytosis in response to reduced plasma
calciumVitamin D feeds back to reduce PTH secretion as a secondary
mechanism
-
Biological Activity of PTHBONE PTH stimulates bone osteoblasts
to increase growth & metabolic activityPTH stimulated bone
resorption releases calcium & phosphate into bloodKIDNEYPTH
increases reabsorption of calcium & reduces reabsorption of
phosphateNet effect of its action is increased calcium &
reduced phosphate in plasmaINTESTINEIncreases calcium reabsorption
via vitamin D
-
CalcitoninCalcitonin is a peptide hormone secreted by the
parafollicular or C cells of the thyroid glandIt is synthesized as
the preprohormone & released in response to high plasma
calciumCalcitonin acts on bone osteoclasts to reduce bone
resorption. Net result of its action is a decline in plasma calcium
& phosphate
-
Synthesis, Release & Activity of Active Vitamin DVitamin D3
is may be obtained from the diet or made in the skinIt is converted
to the active form (1,25-OH-D3 by sequential enzymatic reactions in
the liver and kidney (stimulated by PTH)Vitamin D3 stimulates
intestinal calcium uptake, increased bone calcium resorption &
increased kidney phosphate uptake
-
Calcium Metabolism:Figure 23-20: Calcium balance in the body
-
Hormonal Regulation of Calcium and Phosphate Balance Decreased
Plasma Calcium Causes:Increased PTH Resulting in mobilization of
bone Ca & phosphate, increased renal phosphate excretion &
Ca retention and increased Vitamin D3 synthesisThe outcome is a
rise in plasma Ca levels & maintenance of normal phosphate
levels
-
*Alterations of Parathyroid FunctionHyperparathyroidismPrimary
hyperparathyroidismExcess secretion of PTH from one or more
parathyroid glandsSecondary hyperparathyroidismIncrease in PTH
secondary to a chronic diseaseHypoparathyroidismAbnormally low PTH
levelsUsually caused by parathyroid damage in thyroid surgery
-
Hyperparathyroidism The incidence of the disease increases
dramatically after the age of 50 and it is 2-4 folds more common in
women.A single adenoma occurs in about 80% of patients with primary
hyperparathyroidism. Four glands hyprplasia account for 15-20% of
cases. A parathyroid carcinoma could be the etiology in a rare
incidence of less then 1%.
-
Clinical Feature of HyperparathyroidismIn skeleton a condition
called osteitis fibrosa cystica could occur with subperiosteal
resorption of the distal phalanges, distal tappering of the
clavicles, a salt and pepper appearance of the skull as well as
bone cysts and brown tumors of the long bones. Such overt bone
disease even though typical of primary hyperparathyroidism is very
rarely encountered.
-
Clinical Feature of HyperparathyroidismThe two major sites of
potential complications are the bones and the kidneys.The kidneys
may have renal stones (nephrolithiasis) or diffuse deposition of
calcium-phosphate complexes in the parachyma (nephrocalcinosis).
Now a days such complications are seen less commonly and around 20%
of patients or less show such complications.Clinical Features:
-
HypoparathyroidismIn the absence of renal failure the presence
of hypocalcaemia with hyperphosphataemia is virtually diagnostic of
hypoparathyroidism. Undetectable serum iPTH confirms the diagnosis
or it can be detectable if the assay is very sensitive.
Diagnosis:
-
HypoparathyroidismNeuromuscularParathesiaTetanyHyperventilationAdrenergic
symptomsConvulsion (More common in young people and it can take the
form of either generalized tetany followed by prolonged tonic
spasms or the typical epileptiform seizures.Signs of latent tetany
Chvostek sign,Trousseau sign and extrapyramidal signs (due to basal
ganglia calcification)Clinical Features:
-
HypoparathyroidismOther clinical manifestationPosterio
lenticular cataractCardiac manifestation:Prolonged QT interval in
the ECGResistance to digitalisHypotensionRefractory heart failure
with cardiomegally can occur.
Clinical Features:
-
HypoparathyroidismOther clinical manifestationDental
ManifestationAbnormal enamel formation with delayed or absent
dental eruption and defective dental root formation.Malabsorption
syndromePresumably secondary to decreased calcium level and may
lead to steatorrhoea with long standing untreated disease.Clinical
Features:
-
Treating HypoparathyroidismIt seems logical that PTH would be
beneficial in treating hypoparathyroidism. However few studies are
available that have looked at this traetment possibility. Study
among patients with hypoparathyroidism to PTH twice a day or
calcium and calcitriol to attain normal calcium concentration.
Calcium, phosphorus and magnesium levels did not differ between the
group. No significant BMD between the group. PTH however does not
have the FDA indication for hypoparathyroidism (Painter and
Camacho,2007)*
-
HypoparathyroidismThe mainstay of treatment is a combination of
oral calcium with pharmacological doses of vitamin D or its potent
analogues. Phosphate restriction in diet may also be useful with or
without aluminum hydroxide gel to lower serum phosphate
level.Treatment:
-
Emergency Treatment for HypocalcaemicCalcium should be given
parenterally till adequate serum calcium level is obtained and then
vitamin D supplementation with oral calcium should be
initiated.Tetany:
-
Osteoporosis: Disease of Bone Growth & Calcium
MetabolismFigure 23-21: Osteoclasts are responsible for bone
resorptionBone reabsorption exceeds depositionOsteoclasts mobilize
Ca++ to plasmaFactors: inadequate Ca++ intake, genes, hormones,
smoking
*
a systemic skeletal disease characterized by low bone mass and
micro-architectural deterioration of bone tissue, leading to
enhanced bone fragility and a consequent increase in fracture risk.
Definition of osteoporosisWorld Health Organization (WHO), 1994
-
World Health Organization (WHO)guidelines for osteoporosis
OsteoporosisOsteopeniaNormalPeak Bone MassT-Score
Mosby items and derived items 2006 by Mosby, Inc.
**Prevalence of Elevated Serum TSH by Decade of Age and Gender.
The National Health and Nutrition Examination Survey III (NHANES
III) was a large, prospective study to ascertain the prevalence of
thyroid disease in the United States.1 Hollowell et al measured
serum TSH, total serum T4, antithyroperoxidase (TPOAb), and
antithyroglobulin (TgAb) antibodies from a sample of 17 353 people,
12 years of age or older. The investigators found serum TSH
concentrations to be greater in females than males and to increase
with age, with the greatest increases starting at age 35.In
addition, the NHANES III study showed a higher prevalence of
antithyroid hormones in women than in men, a phenomenon that
increased with age.
Reference1. Hollowell JG, et al. J Clin Endocrinol Metab.
2002;87:489-499.
*Prevalence of Abnormal Thyroid Function.The Colorado Thyroid
Disease Prevalence study examined the prevalence of abnormal
thyroid function in the United States.1 The investigators studied
25 862 participants in a statewide health fair in Colorado in 1995.
The main outcome measures were serum thyrotropin
(thyroid-stimulating hormone [TSH]) and total thyroxine (T4)
concentrations. They also measured serum lipid levels and responses
to a hypothyroid symptoms questionnaire. The researchers defined
normal TSH levels as between 0.3 and 5.1 IU/mL.They found that the
prevalence of elevated TSH in their study population was 9.5%.
Lipid levels were reported to increase as thyroid function
declined. They also reported that the mean total cholesterol and
low-density lipoprotein cholesterol (LDL-C) levels of subjects with
TSH values between 5.1 and 10 IU/mL were significantly higher than
the mean lipid levels in subjects who were euthyroid.The prevalence
of decreased TSH levels was 2.2%. Another finding was that 40% of
patients taking thyroid medications had abnormal TSH levels.
Reference1. Canaris GJ, et al. Arch Intern Med.
2000;160:526-534.*Prevalence of Elevated TSH by Gender.Five large
prevalence studies of thyroid disease placed hypothyroidism among
the conditions for which population screening is justified. In each
of the studies, there were clear differentials between women and
men, with higher rates consistently found in women.1-5The highest
prevalence rates were among older individuals, which was true for
both women and men.
References1. Sawin CT, et al. Arch Intern Med.
1985;145:1386-1388.2. Vanderpump MP, et al. Clin Endocrinol (Oxf).
1995;43:55-68. 3. Canaris GJ, et al. Arch Intern Med.
2000;160:526-534.4. Hak AE, et al. Ann Intern Med.
2000;132:270-278.5. Hollowell JG, et al. J Clin Endocrinol Metab.
2002;87:489-499.*Thyroid-Stimulating Hormone (TSH) Assays.TSH
measurement is the most reliable test to diagnose common forms of
hypothyroidism and hyperthyroidism.1 In both overt and mild
hypothyroidism, serum TSH is elevated and its measurement can
identify a patient with primary hypothyroidism.1 In secondary
hypothyroidism, TSH concentrations may be low, normal, or mildly
elevated. Therefore, TSH measurement cannot reliably identify
patients with central (secondary) hypothyroidism.1 Typically,
hyperthyroidism is accompanied by suppressed TSH concentrations
>0.1 IU/mL.1 In order to diagnose hyperthyroidism, the lowest
reliably measured TSH concentration (assay sensitivity) must be
0.02 IU/mL or less.1The first generation assay used for measuring
TSH was the radioimmunoassay (RIA).2 It has a functional
sensitivity of 1.0 IU/mL.2 The sensitivity of tests has improved
with subsequent generations. The second generation
immunoradiometric assay (IRMA) has a sensitivity of 0.1 IU/mL, and
the third generation enzyme-linked immunosorbent assay (ELISA) has
a sensitivity of 0.03 IU/mL.2,3
References Ladenson PW, et al. Arch Intern Med.
2000;160:1573-1575. Braverman LE, et al. Werner & Ingbars The
Thyroid. A Fundamental and Clinical Text. 8th ed. 2000. Zophel K,
et al. Nuklearmedizin. 1999;38:150-155.*Thyroid Disease
Spectrum.Hyperthyroidism is characterized by sustained increases in
thyroid hormone biosynthesis and secretion.1 Hypothyroidism is
associated with decreases in thyroid hormone production.1Overt
hypothyroidism is defined as the triad of classical signs and
symptoms of hypothyroidism, elevated serum TSH, and abnormally low
free T4.1Mild thyroid failure is less often associated with the
classical signs and symptoms of hypothyroidism.1 Serum TSH levels
are elevated, but to a lesser extent than in overt hypothyroidism.1
Unlike overt disease, the serum free T4 concentration is typically
in the normal range. Mild thyroid failure is associated with health
consequences (eg, unhealthy changes in lipid profiles).2 If
untreated, it has been estimated that 3% to 18% of patients with
mild thyroid failure will progress to overt hypothyroidism.3
References1. Braverman LE, et al. Werner & Ingbars The
Thyroid. A Fundamental and Clinical Text. 8th ed. 2000.2. Canaris
GJ, et al. Arch Intern Med. 2000;160:526-534.3. Vanderpump MP, et
al. Clin Endocrinol (Oxf). 1995;43:55-68.*Screening for Thyroid
Dysfunction. Recommendations for Asymptomatic Adults.The following
recommendations are from 3 organizations that endorsed the use of
screening to detect thyroid dysfunction in asymptomatic
adults.1-3American Thyroid Association (ATA): women and men >35
years of age should be screened every 5 years.American Association
of Clinical Endocrinologists (AACE): older patients, especially
women, should be screened.American College of Physicians: women
>50 years of age with an incidental finding suggestive of
symptomatic thyroid disease should be evaluated.3
References1. Ladenson PW, et al. Arch Intern Med.
2000;160:1573-1575.2. Cooper DS. N Engl J Med. 2001;345:260-265.3.
Ann Intern Med. 1998;129:141-143.*Additional Laboratory Tests for
Thyroid Function.Sensitive immunometric assays have become the
mainstay of thyroid testing.1 Thyroid disease is a graded
phenomenon and changes in serum T4 and especially TSH
concentrations can be detected before any clinical evidence of
hypothyroidism appears.1,2 These laboratory findings are
particularly valuable in diagnosing the spectrum of thyroid
dysfunction as well as for monitoring thyroid hormone replacement
therapy.2 However, patients with subclinical and milder forms of
the disorder have shifts in other measures of thyroid disease. For
this reason, TSH assays combined with other measurements, such as
free and bound T3 and T4, are useful indicators of disease state.2
Serum total T3 or T4 tests measure the total serum concentration of
T3 or T4 using RIA techniques.1,3 Free T4 and T3 measures the
quantity of free or unbound serum T4 and T3.3 Free hormones are
measured by immunometric assay or by equilibrium dialysis.3 TPOAb
and TgAb detection measures antimicrosomal antibodies that are
predictors of disease progression. Normal ranges for these tests
may vary from laboratory to laboratory, depending on test
methodologies and laboratory differences.2 References1. Endocr
Pract. 2002;8:457-469.2. Braverman LE, et al. Werner & Ingbars
The Thyroid. A Fundamental and Clinical Text. 8th ed. 2000.3.
Demers LM, Spencer CA, eds. The National Academy of Clinical
Biochemistry Web site. Available at:
http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed July 1,
2003.*Goals for Treating Thyroid Disease.The goal for managing
patients with thyroid disease is to restore the patient to a normal
state.For hypothyroidism, the goal is to restore thyroid hormones
to normal levels. Levothyroxine sodium is the treatment of choice
for managing patients with hypothyroidism.1 For hyperthyroidism,
treatment is directed toward lowering the serum concentrations of
thyroid hormones in patients to restore a eumetabolic state. The 3
treatments available for achieving this goal are antithyroid drugs,
radioactive iodine (131I), and thyroid surgery.1
Reference1. Singer PA, et al. JAMA. 1995;273:808-812.
*Types of Hypothyroidism.Hypothyroidism is the most common type
of thyroid function disorder.1 There are 2 types: primary and
secondary (or central) hypothyroidism.Primary hypothyroidism is
caused by a condition affecting the thyroid gland that leads to
decreased production of T4 and T3. Primary hypothyroidism is
usually accompanied by increased secretion of TSH. Secondary
hypothyroidism is caused by decreased thyroidal stimulation by TSH.
Secondary hypothyroidism may be caused by pituitary or hypothalamic
disease, the latter associated with decreased thyrotropin-releasing
hormone (TRH).
Reference1. Braverman LE, et al. Werner & Ingbars The
Thyroid. A Fundamental and Clinical Text. 8th ed. 2000.
*Clinical Manifestations of Hypothyroidism.The symptoms of
hypothyroidism are usually related to the age of the patient, the
rapidity of onset, and the presence of other disorders.1 The number
of potential signs and symptoms is large, but most patients will
experience some of the following: fatigue, weight gain, dry skin,
cold intolerance, yellow skin, coarseness or loss of hair,
hoarseness, goiter, delayed relaxation of deep tendon reflexes,
ataxia, constipation, memory and mental impairment, decreased
concentration, depression, irregular or heavy menses and
infertility, myalgias, hyperlipidemia, bradycardia, hypothermia,
and myxedema.1Because the symptoms are varied and not unusual, they
can be misdiagnosed.2Although hypothyroidism is usually associated
with a normal-sized gland, goiter may occur.1 Physical examination
of the thyroid gland is best accomplished by an experienced
clinical endocrinologist.3
References1. Braverman LE, et al. Werner & Ingbars The
Thyroid. A Fundamental and Clinical Text. 8th ed. 2000.2. Canaris
GJ, et al. Arch Intern Med. 2000; 160(4):526-534.3. Hardman JG,
Limbird LE, eds. Goodman and Gilmans The Pharmacological Basis of
Therapeutics. 9th ed. 1996.*Cholesterol Levels Elevate With
Increasing TSH Levels.In the Colorado Thyroid Disease Prevalence
study, Canaris et al studied 25 862 participants at a statewide
health fair in Colorado.1 As part of the study, the total study
population was divided by investigators according to TSH levels to
determine the relationship between declining thyroid function and
serum lipid concentrations. The investigators found that total
cholesterol and LDL-C concentrations progressively and
statistically significantly (P4.0 IU/mL, measuring free thyroxine
(FT4) is the second step.1,2 A normal free T4 value in the face of
an elevated TSH defines mild thyroid failure.1,3 A low FT4 in the
face of an elevated TSH defines overt hypothyroidism.4
References1. Demers LM, Spencer CA, eds. The National Academy of
Clinical Biochemistry Web site. Available at:
http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed July 1, 2003.2.
Ayala AR, et al. Cleve Clin J Med. 2002;69:313-320.3. Ayala AR, et
al. The Endocrinologist. 1997;7:44-50.4. Endocr Pract.
2002;8:457-469.*Hypothyroidism Treatment.According to the American
Thyroid Association1 and the American College of Endocrinology,2
levothyroxine is the treatment of choice for the routine management
of hypothyroidism. Levothyroxine preparations are manufactured in
many different dosages and allow for the precise titration of an
individual patients requirements.1Adults with hypothyroidism
require approximately 1.7 g/kg of body weight/d for full
replacement.1 Children may require up to 4 g/kg of body weight/d.
Older patients may need less than 1 g/kg of body weight/d because
of a decrease in their rate of clearance of thyroxine.1 For
patients who are older than 50 years of age, or in younger patients
with a history of cardiac disease, a lower initial dosage is
recommended, starting with .025 mg to .05 mg of levothyroxine
daily.1The Standards of Care Committee of the American Thyroid
Association also recommends that patients be evaluated at 6- to
8-week intervals until the serum TSH concentration is normalized.1
It is important to remember that patients with exceptionally high
levels of TSH may progress to equilibrium slower than those with
lower TSH values.2 Given the narrow and precise treatment range for
levothyroxine therapy, the AACE recommends that patients should be
maintained on the same brand of levothyroxine through the course of
treatment.2References1. Singer PA, et al. JAMA. 1995;273:808-812.
2. Endocr Pract. 2002;8:457-469.
*Primary Hypothyroidism Treatment Algorithm.This slide shows a
treatment algorithm for primary hypothyroidism. After an initial
dose, the patient should receive a repeat TSH measurement after 6
to 8 weeks.1 If the TSH level is low (4 IU/mL), then the dose of
levothyroxine should be increased by 12.5 to 25 g/d.2 If the TSH
level is in the normal range of 0.5 to 2.0 IU/mL and symptoms are
resolved, then the levothyroxine dose should be continued and the
patients TSH level should be measured after 6 months, then
annually, unless he or she develops symptoms suggestive of thyroid
disease.1,2
References1. Singer PA, et al. JAMA. 1995;273:808-812. 2. Demers
LM, Spencer CA, eds. The National Academy of Clinical Biochemistry
Web site. Available at: http://www.nacb.org/lmpg/thyroid_lmpg.stm.
Accessed July 1, 2003.*Therapy Initiation and Titration.Therapy
with levothyroxine sodium products requires individualized patient
dosing using careful titration, clinical evaluation, and laboratory
monitoring.1 Individualized titration should be based on both
clinical evaluation and laboratory monitoring in order to optimize
serum thyroxine levels, alleviate signs and symptoms of the
disorder, and avoid adverse events.2For each patient, the starting
dose, the frequency of dose titration, and the optimal full
replacement dose must be carefully determined.1 These parameters
will be influenced by patient age, weight, cardiovascular status,
general health, and the severity and duration of
hypothyroidism.1
References1. Endocr Pract. 2002;8:457-469.2. Singer PA, et al.
JAMA. 1995;273:808-812.*Therapy Monitoring.Periodic monitoring of
patients receiving levothyroxine therapy is essential for effective
management.1 Clinical evaluations and laboratory monitoring of
serum TSH levels permit evaluation of the clinical response to the
medication, assessment of patient compliance, assessment of drug
interactions (if applicable), and adjustment of dosage as required
in response to changes in patient lifestyle or circumstances.1It is
recommended that clinical and laboratory evaluations be performed
at 6- to 8-week intervals (2 to 3 weeks in severely hypothyroid
patients).2 The levothyroxine dosage should be adjusted by 12.5 to
25 g increments until serum TSH concentration is normalized and
signs and symptoms resolve.2 Annual testing is recommended after a
euthyroid state is established.2
References1. Singer PA, et al. JAMA. 1995;273:808-812. Demers
LM, Spencer CA, eds.2. Demers LM, Spencer CA, eds. The National
Academy of Clinical Biochemistry Web site. Available at:
http://www.nacb.org/lmpg/thyroid_lmpg.stm. Accessed July 1,
2003.*Special Considerations. Elderly Patients.The prevalence of
hypothyroidism is higher in the elderly compared with younger
persons.1 The symptoms of hypothyroidism in the elderly may be
subtle and include hoarseness, deafness, confusion, dementia,
ataxia, depression, dry skin, and hair loss.Appropriate dose
selection is critical in the elderly as this patient population is
at greater risk for cardiac disorders, and over-replacement with
levothyroxine therapy can exacerbate cardiac abnormalities. Poor
adherence can be an issue with elderly patients, particularly if
they do not have a family or other support system. Furthermore,
elderly patients are often taking multiple medications. Therefore,
careful monitoring of serum TSH levels and adequate patient
education is required to ensure that the patient is given the
appropriate dosage and is complying with the dosing regimen.
Reference1. Felicetta JV. Consultant. 2002;1597-1606. Available
at: www.consultantlive.com. Accessed July 1, 2003.*Caution in
Patients With Underlying Cardiac Disease.Caution should be used
when administering levothyroxine to patients who have ischemic
heart disease in order to prevent possible MI, aggravation of
angina, or cardiac arrhythmias.1,2When administering levothyroxine
to patients