Embed Size (px)
Citation preview

Towards a Complete Solution for Cost/Effectiveness in Oncology: Handling Heterogeneity, Variability and Censoring
Gerhardt PohlEli Lilly and Company

Objective
We view a “complete” solution to the problem of calculating the Incremental Cost Effectiveness Ratio (ICER) in oncology as one simultaneously addressing the key issues of (1) Heterogeneity (2) Variability and (3) Censoring.The talk will discuss a stratified, bootstrap approach and draw links to the concept of “local propensity.”

What is an ICER??
• Incremental Cost Effectiveness Ratio
• Ratio of difference in mean cost divided by difference in mean effectiveness.
where T denotes the new treatment and C the control

Impact
• ICER is the primary tool used in cost-effectiveness comparisons by HTA (Health Technology Assessment) bodies around the world.
• ICER’s allow comparisons of treatments between therapies and across disease states to allow appropriate choices in national health expenditures.

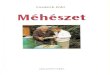
ICER Graphically
QALY
$
ICE Plane
Cheaper and BetterCheaper but Less Effective
More Expense for More Effectiveness
More Expensive and Less Effective
(Quality Adjusted Life Years)

NICE Thresholds
£50,000/QALY (E
nd of Life
Status)
£30,000/QALYNot Approvable
Approvable
“End of Life Status” is granted only for treatments which are life-extending (>3months) for patients (<7,000) with short life expectancy (<24 months)
National Institute for Health and Clinical Excellence

Analysis GoalCreate a bootstrapped display of variability in the ICE plane where each iteration is based on risk-adjusted and censored estimates of the cost and survival.
Frick KD, et al. “Modeled cost-effectiveness of the experience corps Baltimore based on a pilot randomized trial.” Journal of Urban Health 2004; 81:106-117.

Addressing Heterogeneity

Propensity Score Pictorially
Age
Com
orbi
ditie
s
Propensit
y Sco
re St
rata
More likely to receive red treatment
More likely to receive blue treatment

A Downside of Propensity Scoring
• Patients with the identical propensity score may have very different covariate levels.
Age
Com
orbi
ditie
s
Young and Sick
Old But Healthy

Blocking
• Grid the factor space into blocks (unordered strata) of similar patients.
• This may be thought of as a many-to-many matching directly in the covariate space.
Age
Com
orbi
ditie
s
Stratum 1 Stratum 2 Stratum 3
Stratum 4 Stratum 5 Stratum 6
Stratum 7 Stratum 8 Stratum 9

General Approach
• Whatever the original dimension of the covariate space, this reduces the problem to cross-classification of treatments versus strata.
Stratum 1 Stratum 2 Stratum 3
Stratum 4 Stratum 5 Stratum 6
Stratum 7 Stratum 8 Stratum 9
Stratum 1 Stratum 2 … TotalTreatment nT1 nT2 NT
Control nC1 nC2 NC
Total N1 N2 N

Calculate Within-Stratum Treatment Differences
Stratum 1 Stratum 2 Etc. TotalTreatment nT1 nT2 NT
Control nC1 nC2 NC
Total N1 N2 N
Cost:
Effectiveness:
How to pool across strata?

Stratum Weighting
For overall mean difference, pool relative to size of strata:
Definition of Stratified ICER:

Pros and Cons
Blocking• Non-parametric• Provides better matches of
underlying covariates• Able to capture complex
interactions of covariates and likelihood of treatment
Propensity Score Matching• Reduces complexity of
covariate space down to one dimension
• Can maintain structure/ordering of covariate levels
• Can borrow information across blocks
• Potentially uses full richness of continuous data

Addressing Variability

Variability in the ICER Estimate• Many methods have been proposed to incorporate variability into ICER
based inference:
– Univariate Sensitivity Analyses (Tornado Diagrams)– Confidence Intervals (Fieller’s Theorem, 2-dimensional boxes, ellipses, wedges,
bootstrapping…)– Simulation– Cost-Effectiveness Acceptability Curves– Net Monetary Benefit– And various combinations thereof…
• Fundamental technical issue is that the ratio of 2 normal variables is not normal. (Nor very tractable! For example, what if confidence interval for the denominator includes zero.)
• Evidence in literature suggests that Bootstrapping provides robust and consistent inference. Bootstrapping is also relatively assumption free and easily, explained heuristically .

Bootstrapping the Stratified ICER
• Pre-specify strata (factors and cutoff levels).• Sample individual patient cost/effectiveness pairs.• Draw samples with replacement proportional to the
size of the treatment groups -- Ignore stratification in drawing the samples.
• Use the fixed, pre-specified boundaries to divide each sample into strata.
• Calculate stratified difference in cost, stratified difference in effectiveness and stratified ICER for each sample.

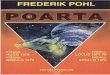
Interpreting the Bootstrap Samples
+Upper
95% Co
nf. In
t.
Lower 95% Conf. Int.
ICER
QALY
$
50.5%48.0%
0.5%1.0%
+
QALY
$
Windshield Wiper Regions Proportion in Each Quadrant of ICE Plane

Effects of Bootstrapping against Fixed Strata Boundaries
• The fraction of patients treated with one or the other treatment within a stratum changes from sample to sample.
• This captures (some of) the component of variability due to estimating the propensity.
• Fixed boundaries prevent technical issues that violate assumptions necessary to assure convergence of the bootstrap. (Abade and Imbens. “On the failure of the bootstrap fro Matching Estimators”. Econometrica, Vol. 76, Issue 6, pp. 1537-1557, Nov. 2008.)

Stratification Redux
• Whatever the original dimension of the covariate space, reduce the problem to cross-classification of treatments versus strata.
Stratum 1 Stratum 2 Stratum 3
Stratum 4 Stratum 5 Stratum 6
Stratum 7 Stratum 8 Stratum 9
Stratum 1 Stratum 2 … TotalTreatment nT1 nT2 NT
Control nC1 nC2 NC
Total N1 N2 N

Local Propensity Score
• Define the “Local Propensity Score” as the fraction of patients treated with treatment A within each stratum.
• Blocking can be thought of as fitting a step function for the estimated propensity.
Stratum 1 Stratum 2 … TotalTreatment nT1 nT2 NT
Control nC1 nC2 NC
Total N1 N2 N
Propensity pj = nT1/N1 nT2/N2

Inverse Propensity Weighting

A Curious Equivalence

Some Algebra
Sum by blocks
Within-block Average
Sum of Weights isTotal Sample Size

Consequences of Equivalence
• (For a class of statistics…)• Consider two individuals from different blocks but
with same propensity score. They enter IPW statistic identically with same weight.
• Therefore, even if matched via propensity score, the summary statistic remains the same.
• Stated another way, matching within strata then calculating local propensity is equivalent to deriving local propensity and then matching via that propensity.

The Downside of PS Does Not Apply to Stratified Local Propensity Scoring
• Underlying differences in covariates are irrelevant to the summary statistic.
Age
Com
orbi
ditie
s
Young and Sick
Old But Healthy

Three Possible WeightingsStratum 1 Stratum 2 Etc. Total
Treatment nT1 nT2 NT
Control nC1 nC2 NC
Total N1 N2 N
Marginal wrt Treatment:
Marginal wrt Control:
Marginal wrt Population:
Weighting Within-Stratum Differences

Three Possible WeightingsStratum 1 Stratum 2 Etc. Total
Treatment nT1 nT2 NT
Control nC1 nC2 NC
Total N1 N2 N
Marginal wrt Treatment:
Marginal wrt Control:
Marginal wrtPopulation:
Average Treatment Effect (ATE)
Average Treatment amongControls (ATT for Control Group)
Average Treatment amongTreated (ATT)
Weighting Within-Stratum Differences IPW/Causal Inference

Relationship among Weightings
Average Treatment Effect (ATE)
Average Treatment amongControls (ATT for Control Group)
Average Treatment amongTreated (ATT)
I.e., ATE is a convex combination of the ATT weightings for Treatment and Control proportional to the size of the groups.

Implications
ATT and ATE weightings are the same,
if and only if, there is uniform propensity to treat with regard to strata.
Therefore, differences under ATT and ATE weightings inform on the impact of directed prescribing (a.k.a. propensity).

Population-Based Weightings Are Not the Same as ANOVA Weightings
• SAS Type I:
• SAS Type II:
• SAS Type III:
Differ, so not collapsible to function of
Inversely proportional to variance of
Uniform across strata

Addressing Censoring

Censored Survival• A recent paper reviewed the survival component of 45 Health Technology
Assessments (HTA) submitted to National Institute for Health and Clinical Excellence (NICE) in the cancer disease area.
• Nicholas R. Latimer. “Survival Analysis for Economic Evaluations alongside Clinical Trials—Extrapolation with Patient-Level Data: Inconsistencies, Limitations, and a Practical Guide”. Medical Decision Making, published online 22 January 2013.
• A variety of methods were noted as having been used to estimate mean survival in the assessments– restricted means analyses, i.e., area under the K-M curve up until a certain point– parametric modeling (exponential, Weibull, Gompertz, etc.)– Partial Likelihood Regression/Proportional Hazards (which accounts for heterogeneity)– Reliance on estimates external to the study
• STRONG PREFERENCE of author for parametric modeling : “a lifetime horizon is usually advocated, particularly for interventions that affect survival. Therefore, in the presence of censoring, extrapolation is required to predict the complete survival impact of the new intervention, which may be summarized as the mean survival benefit.

Is Censoring Really So Bad?
• “In 17 (38%) [H]TAs, extrapolation was not performed, with the survival analysis based purely on the observed trial data (restricted means analysis). Appropriately, this was generally only the case when there was relatively little censoring in the survival data from the trial.”
• Consider a study with 1,000 patients followed until death. Now, add data from 1,000 more patients that have incomplete censored data. The supplemented data has 50% censoring but more information content. Is it really worse than a study one half the size with no censoring?

Our Approach
• The restricted K-M mean provides the advantage of using all data and being non-parametric. So long as time horizon is adequately long to fully characterize survival function, censoring should not be a problem.
• We calculate the K-M mean within each stratum as area under the curve up until the last death. This is conservative as regards the ICER as it tends to underestimate the denominator.

Censored Costs
• D. Y. Lin; E. J. Feuer; R. Etzioni; Y. Wax. “Estimating Medical Costs from Incomplete Follow-Up Data”. Biometrics, Vol. 53, No. 2. (Jun., 1997), pp. 419-434.
• Basic concept is to calculate expected cost via conditioning, i.e., as the sum all intervals of the probability of survival to start of an interval times the average cost incurred during the interval by patients alive at the start of the interval.

Calculation of Censored Cost
PatientEvent Time
Death or
Censor Cost1 Cost2 Cost3 …1 22 1 $1,533 $3,742 $4,899 2 18 1 $5,426 $2,538 $3,745 3 39 0 $6,792 $4,407 $3,890 …
Input Dataset
One Record per Patient
Time to Death or Censoring
Total Cost in Interval (E.g., Weekly Cost)

Calculation of Censored Cost
PatientEvent Time
Death or
Censor Cost1 Cost2 Cost3 …1 22 1 $1,533 $3,742 $4,899 2 18 1 $5,426 $2,538 $3,745 3 39 0 $6,792 $4,407 $3,890 …
Week S1 0.982 0.873 0.66…
Week Avg Cost1 $4,583 2 $3,562 3 $4,178 …
Kaplan-Meier Calculate Averages
Input Dataset
Probability ofSurvival untilTime Period
Average Period Cost among Patients Alive at
Start of Time Period
One Record per Time Interval
One Record per Patient

Calculation of Censored Cost
PatientEvent Time
Death or
Censor Cost1 Cost2 Cost3 …1 22 1 $1,533 $3,742 $4,899 2 18 1 $5,426 $2,538 $3,745 3 39 0 $6,792 $4,407 $3,890 …
Week S1 0.982 0.873 0.66…
Week Avg Cost1 $4,583 2 $3,562 3 $4,178 …
$10,348
Kaplan-Meier Calculate Averages
Input Dataset
Probability ofSurvival untilTime Period
Average Period Cost among Patients Alive at
Start of Time Period
One Record per Time Interval
One Record per Patient
Expected (Censoring-Adjusted) Cost

Pulling It All Together
• To adjust for heterogeneous risk stratify.• Address censoring by calculating censored mean
survival and expected cost within strata.• Pool strata relative to stratum size.• Bootstrap at individual patient level against the pre-
specified strata boundaries to incorporate variability arising from outcomes and propensity estimates.
• All together, this yields a complete method to calculate ICER in oncology.








![Gerhardt traite resistances[1]](https://img.pdfslide.net/doc/110x75/55ce3441bb61eb29628b457b/gerhardt-traite-resistances1.jpg)