Embed Size (px)
Citation preview

S p e c i a l R e p o r t
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med nejm.org 1
Zika Virus and Birth Defects — Reviewing the Evidence for Causality
Sonja A. Rasmussen, M.D., Denise J. Jamieson, M.D., M.P.H., Margaret A. Honein, Ph.D., M.P.H., and Lyle R. Petersen, M.D., M.P.H.
Summary
The Zika virus has spread rapidly in the Americas since its first identification in Brazil in early 2015. Prenatal Zika virus infection has been linked to adverse pregnancy and birth outcomes, most no-tably microcephaly and other serious brain anom-alies. To determine whether Zika virus infection during pregnancy causes these adverse out-comes, we evaluated available data using criteria that have been proposed for the assessment of potential teratogens. On the basis of this review, we conclude that a causal relationship exists be-tween prenatal Zika virus infection and micro-cephaly and other serious brain anomalies. Evi-dence that was used to support this causal relationship included Zika virus infection at times during prenatal development that were consis-tent with the defects observed; a specific, rare phenotype involving microcephaly and associated brain anomalies in fetuses or infants with pre-sumed or confirmed congenital Zika virus infec-tion; and data that strongly support biologic plausibility, including the identification of Zika virus in the brain tissue of affected fetuses and infants. Given the recognition of this causal rela-tionship, we need to intensify our efforts toward the prevention of adverse outcomes caused by congenital Zika virus infection. However, many questions that are critical to our prevention ef-forts remain, including the spectrum of defects caused by prenatal Zika virus infection, the de-gree of relative and absolute risks of adverse out-comes among fetuses whose mothers were in-fected at different times during pregnancy, and factors that might affect a woman’s risk of ad-verse pregnancy or birth outcomes. Addressing these questions will improve our ability to reduce the burden of the effects of Zika virus infection during pregnancy.
Potential Rel ationship bet ween Zik a Virus Infec tion and Birth
Defec ts
Since the identification of the Zika virus in Bra-zil in early 2015, the virus has spread rapidly throughout the Americas (www . cdc . gov/ zika/ geo/ active-countries . html). An increase in the number of infants with microcephaly in Brazil was first noted in September 2015, after the recognition of Zika virus transmission in the country earlier in the year1; this was followed by the recognition of a similar increase in French Polynesia after an outbreak there in 2013 and 2014.2 Despite accumulating evidence that sup-ports the link between Zika virus infection and microcephaly, most experts have taken care not to state that Zika virus infection is causally re-lated to these adverse outcomes.3 This cautious approach toward ascribing Zika virus as a cause of birth defects is not surprising, given that the last time an infectious pathogen (rubella virus) caused an epidemic of congenital defects was more than 50 years ago, no flavivirus has ever been shown definitively to cause birth defects in humans,4 and no reports of adverse pregnancy or birth outcomes were noted during previous outbreaks of Zika virus disease in the Pacific Islands.5,6
On the basis of the available evidence, the public health response to the outbreak of Zika virus disease has moved forward, with the dis-tribution of health messages about the impor-tance of mosquito-bite prevention, recommenda-tions by public health authorities in some of the most severely affected countries to delay preg-nancy, and advisories that pregnant women avoid travel to areas with active Zika virus transmission.7 However, communications regarding Zika virus have been challenging: a recent survey showed
The New England Journal of Medicine Downloaded from nejm.org on April 13, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med nejm.org 2
low levels of knowledge and concern about Zika virus in the United States.8 The recognition of Zika virus as a cause of microcephaly and other serious brain anomalies would allow for more direct communication, which might lead to im-proved understanding of and adherence to public health recommendations. Therefore, a review of the evidence linking Zika virus infection and ad-verse pregnancy and birth outcomes is needed.
As is typically the case in epidemiology and medicine, no “smoking gun” (a single definitive piece of evidence that confirms Zika virus as a cause of congenital defects) should have been an-ticipated. Instead, the determination of a causal relationship would be expected to emerge from various lines of evidence, each of which suggests, but does not on its own prove, that prenatal Zika virus infection can cause adverse outcomes. Two approaches have been used to identify potential teratogens (exposures to a mother during preg-nancy that have a harmful effect on her embryo or fetus)9: first, the identification of a combination of a rare exposure and a rare defect (sometimes referred to as the astute clinician approach),10 and second, the use of epidemiologic data to confirm an association. Many teratogens were first iden-tified by means of the rare exposure–rare defect approach, including rubella virus, which was iden-tified after an ophthalmologist noted a character-istic form of cataracts in infants whose mothers had rubella during pregnancy,11 and heavy alcohol use, which was identified as a teratogen after the recognition of a characteristic pattern of malfor-mations that became known as the fetal alcohol syndrome.12 In contrast, some teratogens have been identified on the basis of epidemiologic studies (e.g., valproic acid was identified as a teratogen after a case–control study showed an odds ratio of 20 for the association of spina bifida with use of this drug during the first trimester of pregnancy).13
Shepard’s Criteria
In 1994, Thomas Shepard, a pioneer in the field of teratology, proposed a set of seven criteria for “proof” of human teratogenicity (Table 1) that incorporated both approaches.9 These criteria were an amalgamation of criteria developed by other teratologists and guided by methods that were used to identify previous teratogens. These criteria have been used to guide discussions
about causation in teratology-related litigation30 and to assess other potential teratogens.10 We used Shepard’s criteria9 as a framework to evaluate whether the currently available evidence supports the hypothesis that prenatal Zika virus infection is a cause of microcephaly and other brain anom-alies (Table 1).
According to these criteria, causality is estab-lished when either criteria 1, 3, and 4 (rare ex-posure–rare defect approach) or criteria 1, 2, and 3 (epidemiologic approach) are fulfilled. The first criterion states that a proven exposure to an agent must occur at a critical time during prenatal de-velopment. The severe microcephaly and other brain anomalies that have been observed in many infants are consistent with an infection occurring in the first or early second trimester of pregnan-cy. Several case reports and studies have shown that women who had fetuses or infants with congenital brain anomalies that were believed, on the basis of the mother’s symptoms or labo-ratory confirmation, to be due to Zika virus in-fection were infected in the first or early second trimester of pregnancy, as determined either according to the timing of the symptoms or ac-cording to the timing of travel to an area where Zika virus is endemic.14-20 An analysis of the tim-ing of laboratory-confirmed Zika virus transmis-sion in certain states in Brazil and of the in-crease in the cases of microcephaly identified the first trimester as the critical time period for infection.1 Zika virus infections that occur later in pregnancy have been associated with poor in-trauterine growth, fetal death, or in some preg-nancies, defects on prenatal imaging that have not yet been confirmed postnatally because the pregnancies are ongoing.14 We conclude that Shepard’s first criterion has been met.
Shepard’s second criterion requires that two epidemiologic studies of high quality support the association. Although ecologic data do not neces-sarily qualify as an epidemiologic study, data from Brazil regarding the temporal and geographic association between Zika virus infection and the later appearance of infants with congenital mi-crocephaly are compelling.1,31,32 Two epidemio-logic studies also provide support.2,14 In a study conducted during the outbreak in Brazil, 88 preg-nant women who had had an onset of rash in the previous 5 days were tested for Zika virus RNA. Among the 72 women who had positive tests, 42 underwent prenatal ultrasonography, and fe-
The New England Journal of Medicine Downloaded from nejm.org on April 13, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

Special Report
n engl j med nejm.org 3
tal abnormalities were observed in 12 (29%); none of the 16 women with negative tests had fetal abnormalities. The abnormalities that were ob-served on ultrasonography varied widely, and some findings lacked postnatal confirmation because the pregnancies were ongoing.14
A retrospective analysis after the 2013–2014
outbreak of Zika virus disease in French Polyne-sia identified eight cases of microcephaly; the authors used serologic and statistical data and mathematical modeling to estimate that 1% of the fetuses and neonates who were born to mothers who had been infected with Zika virus in the first trimester had microcephaly2 — a prevalence
Criterion No. Criterion Evidence Criterion Met?
1 Proven exposure to the agent at one or more critical times during prenatal development
On the basis of case reports, case series, and epidemiologic studies of microcephaly that are associated with laboratory-confirmed or pre-sumed Zika virus infection, the timing of Zika virus infection associ-ated with severe microcephaly and intracranial calcifications appears to be in the late first or early second trimester.14-20
Yes
2 Consistent findings by ≥2 high-quality epidemiologic studies, with con-trol of confounding factors, suffi-cient numbers, exclusion of posi-tive and negative bias factors, pro-spective studies if possible, and relative risk ≥6
On the basis of data from Brazil, the temporal and geographic associa-tion between Zika virus illness and cases of microcephaly is strong.1
Two epidemiologic studies have been published. In a study in Brazil14 that used a prospective cohort design, 29% of women with Zika virus infection at any time during pregnancy had abnormalities on prenatal ultrasonography, some of which have not been confirmed postnatal-ly, In a study in French Polynesia,2 retrospective identification of eight cases of microcephaly and the use of serologic and statistical data and mathematical modeling suggested that 1% of fetuses and infants born to women with Zika virus infection during the first trimester had microcephaly; the risk ratio in this analysis was approximately 50, as compared with the baseline prevalence of microcephaly.
No other epidemiologic studies have examined this association to date.
Partially
3 Careful delineation of clinical cases; a specific defect or syndrome, if present, is very helpful
The phenotype has been well characterized in fetuses and infants with presumed congenital Zika virus infection, including microcephaly and other serious brain anomalies, redundant scalp skin, eye findings, ar-throgryposis, and clubfoot.15,20-23
The phenotype in some infants appears to be consistent with the fetal brain disruption sequence,20,22 which has been observed after infec-tion with other viral teratogens.24
Yes
4 Rare environmental exposure that is associated with rare defect
Reports of fetuses and infants with microcephaly who are born to women with brief periods of travel to countries with active Zika virus trans-mission are consistent with Zika virus being a rare exposure.16,18,19
The defect, congenital microcephaly, is rare, with a birth prevalence of approximately 6 cases per 10,000 liveborn infants, according to data from birth-defects surveillance systems in the United States.25
Yes
5 Teratogenicity in experimental animals important but not essential
No results of an animal model with Zika virus infection during pregnancy and fetal effects have yet been published.
No
6 Association should make biologic sense
Findings are similar to those seen after prenatal infection with some oth-er viral teratogens (e.g., cytomegalovirus, rubella virus).26
Animal models have shown that Zika virus is neurotropic,27,28 which sup-ports biologic plausibility.
Evidence that Zika virus infects neural progenitor cells and produces cell death and abnormal growth,29 along with evidence of Zika virus in brains of fetuses and infants with microcephaly, on the basis of im-munohistochemical staining and identification of Zika virus RNA and live virus,16,17,19 provides strong biologic plausibility.
Yes
7 Proof in an experimental system that the agent acts in an unaltered state
This criterion applies to a medication or chemical exposure, not to infec-tious agents.
NA
* The criteria listed here were proposed by Shepard.9 Criteria 1, 2, and 3 or criteria 1, 3, and 4 are considered to be essential, whereas criteria 5, 6, and 7 are helpful but not essential. Partial evidence is insufficient to meet a criterion. NA denotes not applicable.
Table 1. Shepard’s Criteria for Proof of Teratogenicity in Humans as Applied to the Relationship between Zika Virus Infection and Microcephaly and Other Brain Anomalies.*
The New England Journal of Medicine Downloaded from nejm.org on April 13, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med nejm.org 4
that was approximately 50 times as high as the estimated baseline prevalence. However, this esti-mate was based on small numbers, confidence intervals were wide, and the risk of other adverse outcomes (e.g., other brain anomalies) was not assessed.2 Although these studies provide im-portant evidence in support of a causal relation-ship between Zika virus and microcephaly and other brain anomalies, both have limitations as noted by their authors, such as a lack of control for confounding factors and relatively small num-bers of cases, and therefore they do not meet the stringent criteria set by Shepard. Thus, we con-clude that Shepard’s second criterion has not yet been satisfied.
The third criterion, careful delineation of clinical cases with the finding of a specific de-fect or syndrome, appears to be met. Previous teratogens have caused specific birth defects or syndromes rather than a broad range of birth defects.33 Many fetuses and infants with presumed congenital Zika virus infection have had a typical pattern, including severe microcephaly, intracra-nial calcifications, and other brain anomalies, sometimes accompanied by eye findings, redun-dant scalp skin, arthrogryposis, and clubfoot15,20-23; such findings have led authors to use the term “congenital Zika syndrome.”22,34,35 On the basis of clinical details from a limited number of cases, some infants with presumed congenital Zika vi-rus infection have had features that were consis-tent with fetal brain disruption sequence,24 a phe-notype involving the brain that is characterized by severe microcephaly, overlapping cranial sutures, prominent occipital bone, redundant scalp skin, and considerable neurologic impairment.20,22 For example, 11 of 35 infants (31%) with microceph-aly whose cases were reported to a Brazil Minis-try of Health registry had excessive and redundant scalp skin,20 a finding that is not typically seen in other forms of microcephaly.36 These findings sug-gest an interruption of cerebral growth, but not in that of the scalp skin, after an injury (e.g., viral infection, hyperthermia, or vascular disruption) that occurred after the initial formation of brain structures, followed by partial collapse of the skull. The fetal brain disruption sequence is rare; only 20 cases were identified in a literature review in 2001.24
Shepard’s fourth criterion refers to the asso-ciation between a rare exposure and a rare de-fect; we conclude that this criterion also has
been met. The concept behind this criterion is that a rare defect occurring after a rare exposure during pregnancy implies causation because of the unlikelihood of the two rare events occur-ring together.10 Microcephaly is a rare defect that is estimated to occur in 6 infants per 10,000 live-born infants in the United States.25 Zika virus would not be a rare exposure among women living in Brazil during the Zika virus outbreak. However, reports of adverse birth outcomes among travelers who spent only a limited time period in an area where there is active Zika virus transmission are consistent with Zika virus being a rare expo-sure.16,18,19
A recent report is illustrative: a pregnant wom-an traveled for 7 days to Mexico, Guatemala, and Belize during her 11th week of gestation and had a positive test for Zika virus immunoglobu-lin M (IgM) antibodies 4 weeks later. On fetal ultrasonography and magnetic resonance imag-ing performed at 19 to 20 weeks of gestation, se-vere brain anomalies were diagnosed in the fetus, and the pregnancy was terminated at 21 weeks of gestation. Microcephaly was not present at the time of pregnancy termination, but the head cir-cumference had decreased from the 47th percen-tile at 16 weeks of gestation to the 24th percen-tile at 20 weeks of gestation (a finding that is consistent with the timing of diminishing head sizes in previous cases),14 which suggests that microcephaly would have developed in the fetus had the pregnancy continued.16 In this woman, Zika virus would be considered a rare exposure, and her fetus had a rare outcome.
The last three criteria are helpful if they are present, but they are not considered to be essen-tial. The fifth criterion, the need for an animal model that shows teratogenicity, has not been met. Although animal models have shown that Zika virus is neurotropic,27,28 no studies that test-ed for teratogenicity in an animal model have been published, although studies are under way. The sixth criterion, that the association should make biologic sense, is clearly met here. Other viral infections have had similar effects (micro-cephaly and eye problems).24,26 In addition, patho-logic evidence supports this association: Zika vi-rus RNA has been seen in damaged mononuclear cells (presumably glial cells and neurons) in the brains of newborns with microcephaly,17 and the virus appears to be neurotropic.17,19 Live Zika vi-rus has been cultured from the brain of a fetus
The New England Journal of Medicine Downloaded from nejm.org on April 13, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

Special Report
n engl j med nejm.org 5
with severe brain anomalies after maternal infec-tion at 11 weeks of gestation.16 Furthermore, Zika virus efficiently infects neural progenitor cells and produces cell death and abnormal growth, thus providing a possible mechanism for micro-
cephaly.29 The seventh criterion, proof in an ex-perimental system that the agent acts in an un-altered state, is aimed at medications or chemical exposures and does not apply to infectious agents. Thus, given Shepard’s criteria as a framework,
Criterion Evidence Criterion Met?
Strength of association A recent epidemiologic study from French Polynesia suggests a strong asso-ciation between prenatal Zika virus infection and microcephaly (estimat-ed risk ratio, approximately 50).2
The substantial increase in the number of cases of microcephaly and other brain anomalies that have been associated with the Zika virus outbreak in Brazil suggests a strong association.1,2
Yes
Consistency Two epidemiologic studies, one from Brazil and one from French Poly-nesia,2,14 support the association between prenatal Zika virus infection and microcephaly and other serious brain anomalies.
The observed increase in the number of cases of microcephaly after out-breaks of Zika virus infection in Brazil and French Polynesia, as well as preliminary reports of cases in Colombia, support consistency.1,2,42
Case reports of Zika virus infection in fetuses or infants with microcephaly or other brain anomalies who were born to mothers who traveled to areas of active Zika virus transmission support consistency.16,18,19
Yes
Specificity Other causes of microcephaly exist; however, on the basis of clinical descrip-tions that are available for a small number of infants with presumed con-genital Zika virus infection,20 the clinical phenotype linked to the Zika vi-rus appears to be an unusual form of microcephaly that is consistent with the fetal brain disruption sequence.
Yes
Temporality Zika virus infection in mothers during pregnancy precedes the finding of mi-crocephaly or other brain anomalies in fetuses or infants.14-20
Zika virus outbreaks in Brazil and French Polynesia preceded the increase in the number of cases of microcephaly.1,2
Yes
Biologic gradient Infection is a phenomenon that is either present or absent; there is no dose–response relationship.
No data are available regarding whether women with an increased viral load have a higher risk of adverse pregnancy or birth outcomes.
NA
Plausibility Findings are similar to those seen after prenatal infection with some other vi-ral teratogens (e.g., cytomegalovirus and rubella virus).26
Evidence that Zika virus infects neural progenitor cells and produces cell death and abnormal growth,29 along with evidence of Zika virus in brains of fetuses and infants with microcephaly, on the basis of on immunohis-tochemical staining and identification of Zika virus RNA and live vi-rus,16,17,19 provides strong biologic plausibility.
Yes
Coherence No results in an animal model of effects of Zika virus on pregnancy have yet been published, but animal models have shown that Zika virus is neuro-tropic,27,28 a finding that is consistent with prenatal Zika virus infection causing microcephaly and other brain anomalies.
Zika virus infects neural progenitor cells and produces cell death and abnor-mal growth,29 a finding that is consistent with a causal relationship be-tween Zika virus infection and microcephaly.
Yes
Experiment No experimental animal model of Zika virus teratogenicity is available. No
Analogy No other flavivirus has been shown to definitively cause birth defects in hu-mans,4 but flaviviruses, Wesselsbron and Japanese encephalitis viruses, have been shown to cause stillbirth and brain anomalies in animals.43
Findings are similar to those seen after prenatal infection with other viral te-ratogens (e.g., cytomegalovirus, rubella virus).26
Yes
* The criteria listed here were proposed by Hill.40 We have updated a recent analysis by Frank et al.41
Table 2. Bradford Hill Criteria for Evidence of Causation as Applied to the Relationship between Zika Virus Infection and Microcephaly and Other Brain Anomalies*
The New England Journal of Medicine Downloaded from nejm.org on April 13, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med nejm.org 6
criteria 1, 3, and 4 have been satisfied — evidence that is considered sufficient to identify an agent as a teratogen.
Other Criteria
Other criteria can also be used to assess this relationship. Koch’s postulates, developed in the late 19th century, are often cited as necessary to show causation in infectious disease; however, many authors have noted the need for Koch’s postulates to be updated to accommodate mod-ern technologies.37-39 The Bradford Hill criteria40 provide another framework to assess causation; Frank et al. recently used these criteria to assess the relationship between prenatal Zika virus in-fection and microcephaly and concluded that additional information was needed to assume that the relationship was causal.41 However, sev-eral key pieces of evidence have become available since they performed their analysis, including two epidemiologic studies,2,14 a study of the ef-fects of Zika virus on neural progenitor cells,29 and a case report of a fetus with brain anomalies and decreasing head size from whose brain live Zika virus was isolated.16 On the basis of our up-date of their analysis, which incorporates newly available evidence (Table 2), nearly all the rele-vant criteria have been met, with the exception of the presence of experimental evidence. How-ever, Hill emphasizes that meeting all nine crite-ria is not necessary40; instead, the criteria should serve as a framework to assess when the most likely interpretation of a relationship is causation.
Assessment of Criteria
Thus, on the basis of a review of the available evidence, using both criteria that are specific for the evaluation of potential teratogens9 and the Bradford Hill criteria40 as frameworks, we sug-gest that sufficient evidence has accumulated to infer a causal relationship between prenatal Zika virus infection and microcephaly and other se-vere brain anomalies. Also supportive of a causal relationship is the absence of an alterna-tive explanation; despite the extensive consider-ation of possible causes, researchers have been unable to identify alternative hypotheses that could explain the increase in cases of microcepha-ly that were observed first in Brazil and then retrospectively in French Polynesia, and now in
preliminary reports that are being investigated in Colombia.1,2,42
Moving from a hypothesis that Zika virus is linked to certain adverse outcomes to a state-ment that Zika virus is a cause of certain adverse outcomes allows for direct communications re-garding risk, both in clinical care settings and in public health guidance, and an intensified focus on prevention efforts, such as the imple-mentation of vector control, the identification of improved diagnostic methods, and the develop-ment of a Zika virus vaccine.44 In addition, after recognizing a causal relationship between Zika virus infection and adverse pregnancy and birth outcomes, we can focus research efforts on other critical issues: First, understanding the full spec-trum of defects caused by congenital Zika virus infection; if Zika virus is similar to other terato-gens, an expansion of the phenotype would be expected (e.g., with the congenital rubella syn-drome, the phenotype was expanded from cata-racts to include other findings such as hearing loss, congenital heart defects, and microcepha-ly).11 Second, quantifying the relative and abso-lute risks among infants who are born to women who were infected at different times during preg-nancy. Third, identifying factors that modify the risk of an adverse pregnancy or birth outcome (e.g., coinfection with another virus, preexisting immune response to another flavivirus, genetic background of the mother or fetus, and severity of infection). Addressing these issues will im-prove our efforts to minimize the burden of the effects of Zika virus infection during pregnancy.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
From the Division of Public Health Information Dissemination, Center for Surveillance, Epidemiology, and Laboratory Services (S.A.R.), Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion (D.J.J.), and Division of Congenital and Developmental Disorders, National Center on Birth Defects and Developmental Disabilities (M.A.H.), Centers for Disease Control and Prevention, Atlanta; and the Division of Vector-Borne Diseases, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Dis-ease Control and Prevention, Fort Collins, CO (L.R.P.). Address reprint requests to Dr. Rasmussen at the Centers for Disease Control and Prevention, 1600 Clifton Rd., MS E-33, Atlanta, GA 30329, or at skr9@ cdc . gov.
This article was published on April 13, 2016, at NEJM.org.
1. Kleber de Oliveira W, Cortez-Escalante J, De Oliveira WT, et al. Increase in reported prevalence of microcephaly in infants born to women living in areas with confirmed Zika virus trans-mission during the first trimester of pregnancy — Brazil, 2015. MMWR Morb Mortal Wkly Rep 2016; 65: 242-7.
The New England Journal of Medicine Downloaded from nejm.org on April 13, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

Special Report
n engl j med nejm.org 7
2. Cauchemez S, Besnard M, Bompard P, et al. Association be-tween Zika virus and microcephaly in French Polynesia, 2013-15: a retrospective study. Lancet 2016 March 15 (Epub ahead of print).3. Petersen LR, Jamieson DJ, Powers AM, Honein MA. Zika vi-rus. N Engl J Med 2016; 374: 1552-63.4. O’Leary DR, Kuhn S, Kniss KL, et al. Birth outcomes follow-ing West Nile Virus infection of pregnant women in the United States: 2003-2004. Pediatrics 2006; 117(3): e537-45.5. Duffy MR, Chen T-H, Hancock WT, et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N Engl J Med 2009; 360: 2536-43.6. Ioos S, Mallet HP, Leparc Goffart I, Gauthier V, Cardoso T, Herida M. Current Zika virus epidemiology and recent epidem-ics. Med Mal Infect 2014; 44: 302-7.7. Chang C, Ortiz K, Ansari A, Gershwin ME. The Zika out-break of the 21st century. J Autoimmun 2016; 68: 1-13.8. Associated Press-NORC Center for Public Affairs Research. The Zika virus: Americans’ awareness and opinions of the U.S. response. April 2016 (http://www .apnorc .org/ PDFs/ Zika/ 2016-04%20Zika%20Virus%20Issue%20Brief%20DTPB_v1r5 .pdf).9. Shepard TH. “Proof” of human teratogenicity. Teratology 1994; 50: 97-8.10. Carey JC, Martinez L, Balken E, Leen-Mitchell M, Robertson J. Determination of human teratogenicity by the astute clinician method: review of illustrative agents and a proposal of guide-lines. Birth Defects Res A Clin Mol Teratol 2009; 85: 63-8.11. Webster WS. Teratogen update: congenital rubella. Teratol-ogy 1998; 58: 13-23.12. Jones KL, Smith DW. Recognition of the fetal alcohol syn-drome in early infancy. Lancet 1973; 302: 999-1001.13. Lammer EJ, Sever LE, Oakley GP Jr. Teratogen update: val-proic acid. Teratology 1987; 35: 465-73.14. Brasil P, Pereira JP Jr, Raja Gabaglia C, et al. Zika virus infec-tion in pregnant women in Rio de Janeiro — preliminary report. N Engl J Med. DOI: 10.1056/NEJMoa1602412.15. Calvet G, Aguiar RS, Melo AS, et al. Detection and sequenc-ing of Zika virus from amniotic fluid of fetuses with micro-cephaly in Brazil: a case study. Lancet Infect Dis 2016 February 17 (Epub ahead of print).16. Driggers RW, Ho CY, Korhonen EM, et al. Zika virus infec-tion with prolonged maternal viremia and fetal brain abnor-malities. N Engl J Med. DOI: 10.1056/NEJMoa1601824.17. Martines RB, Bhatnagar J, Keating MK, et al. Notes from the field: evidence of Zika virus infection in brain and placental tissues from two congenitally infected newborns and two fetal losses — Brazil, 2015. MMWR Morb Mortal Wkly Rep 2016; 65: 159-60.18. Meaney-Delman D, Hills SL, Williams C, et al. Zika virus infection among U.S. pregnant travelers — August 2015–Febru-ary 2016. MMWR Morb Mortal Wkly Rep 2016; 65: 211-4.19. Mlakar J, Korva M, Tul N, et al. Zika virus associated with microcephaly. N Engl J Med 2016; 374: 951-8.20. Schuler-Faccini L, Ribeiro EM, Feitosa IM, et al. Possible as-sociation between Zika virus infection and microcephaly — Bra-zil, 2015. MMWR Morb Mortal Wkly Rep 2016; 65: 59-62.21. Ventura CV, Maia M, Bravo-Filho V, Góis AL, Belfort R Jr. Zika virus in Brazil and macular atrophy in a child with micro-cephaly. Lancet 2016; 387: 228.22. Miranda-Filho Dde B, Martelli CM, Ximenes RA, et al. Initial description of the presumed congenital Zika syndrome. Am J Public Health 2016; 106: 598-600.23. Oliveira Melo AS, Malinger G, Ximenes R, Szejnfeld PO, Alves Sampaio S, Bispo de Filippis AM. Zika virus intrauterine infection causes fetal brain abnormality and microcephaly: tip of the iceberg? Ultrasound Obstet Gynecol 2016; 47: 6-7.
24. Corona-Rivera JR, Corona-Rivera E, Romero-Velarde E, Hernández-Rocha J, Bobadilla-Morales L, Corona-Rivera A. Re-port and review of the fetal brain disruption sequence. Eur J Pediatr 2001; 160: 664-7.25. National Birth Defects Prevention Network. Major birth de-fects data from population-based birth defects surveillance pro-grams in the United States, 2006-2010. August 2013 (http://www .nbdpn .org/ docs/ DataDirectory2013_NBDPN_AR .pdf).26. Bale JF Jr. Fetal infections and brain development. Clin Peri-natol 2009; 36: 639-53.27. Dick GW. Zika virus. II. Pathogenicity and physical proper-ties. Trans R Soc Trop Med Hyg 1952; 46: 521-34.28. Bell TM, Field EJ, Narang HK. Zika virus infection of the central nervous system of mice. Arch Gesamte Virusforsch 1971; 35: 183-93.29. Tang H, Hammack C, Ogden SC, et al. Zika virus infects human cortical neural progenitors and attenuates their growth. Cell Stem Cell 2016 March 4 (Epub ahead of print).30. Public Affairs Committee of the Teratology Society. Causa-tion in teratology-related litigation. Birth Defects Res A Clin Mol Teratol 2005; 73: 421-3.31. Teixeira MG, da Conceição N Costa M, de Oliveira WK, Nunes ML, Rodrigues LC. The epidemic of Zika virus-related microcephaly in Brazil: detection, control, etiology, and future scenarios. Am J Public Health 2016; 106: 601-5.32. Reefhuis J, Gilboa SM, Johansson MA, et al. Projecting month of birth for at-risk infants after Zika virus disease out-breaks. Emerg Infect Dis (in press).33. Mitchell AA. Proton-pump inhibitors and birth defects — some reassurance, but more needed. N Engl J Med 2010; 363: 2161-3.34. Costa F, Sarno M, Khouri R, et al. Emergence of congenital Zika syndrome: viewpoint from the front lines. Ann Intern Med 2016 February 24 (Epub ahead of print).35. Chan JF, Choi GK, Yip CC, Cheng VC, Yuen KY. Zika fever and congenital Zika syndrome: an unexpected emerging arbovi-ral disease. J Infect 2016 March 3 (Epub ahead of print).36. Abuelo D. Microcephaly syndromes. Semin Pediatr Neurol 2007; 14: 118-27.37. Byrd AL, Segre JA. Infectious disease: adapting Koch’s pos-tulates. Science 2016; 351: 224-6.38. Fredricks DN, Relman DA. Sequence-based identification of microbial pathogens: a reconsideration of Koch’s postulates. Clin Microbiol Rev 1996; 9: 18-33.39. Williams JV. Déjà vu all over again: Koch’s postulates and virology in the 21st century. J Infect Dis 2010; 201: 1611-4.40. Hill AB. The environment and disease: association or causa-tion? Proc R Soc Med 1965; 58: 295-300.41. Frank C, Faber M, Stark K. Causal or not: applying the Brad-ford Hill aspects of evidence to the association between Zika virus and microcephaly. EMBO Mol Med 2016 March 14 (Epub ahead of print).42. Instituto Nacional de Salud. Boletin Epidemiologico Se-manal. April 2016 (http://www .ins .gov .co/ boletin-epidemiologico/ Boletn%20Epidemiolgico/ 2016%20Boletín%20epidemiológico %20semana%2012 .pdf).43. Hubálek Z, Rudolf I, Nowotny N. Arborviruses pathogenic for domestic and wild animals. Adv Virus Res 2014; 89: 201-75.44. Palacios R, Poland GA, Kalil J. Another emerging arbovirus, another emerging vaccine: targeting Zika virus. Vaccine 2016 March 23 (Epub ahead of print).
DOI: 10.1056/NEJMsr1604338Copyright © 2016 Massachusetts Medical Society.
The New England Journal of Medicine Downloaded from nejm.org on April 13, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

REPORTS
Cite as: Garcez et al., Science 10.1126/science.aaf6116 (2016).
Primary microcephaly is a severe brain malformation char-acterized by the reduction of the head circumference. Pa-tients display a heterogeneous range of brain impairments, compromising motor, visual, hearing and cognitive func-tions (1).
Microcephaly is associated with decreased neuronal pro-duction as a consequence of proliferative defects and death of cortical progenitor cells (2). During pregnancy, the pri-mary etiology of microcephaly varies from genetic muta-tions to external insults. The so-called TORCHS factors (Toxoplasmosis, Rubella, Cytomegalovirus, Herpes virus, Syphilis) are the main congenital infections that compro-mise brain development in utero (3).
The increase in the rate of microcephaly in Brazil has been associated with the recent outbreak of Zika virus (ZIKV) (4, 5), a flavivirus that is transmitted by mosquitoes (6) and sexually (7–9). So far, ZIKV has been described in the placenta and amniotic fluid of microcephalic fetuses (10–13), and in the blood of microcephalic newborns (11, 14). ZIKV had also been detected within the brain of a microce-phalic fetus (13, 14), and recently, there is direct evidence that ZIKV is able to infect and cause death of neural stem cells (15).
Here, we used human induced pluripotent stem (iPS) cells cultured as neural stem cells (NSC), neurospheres and brain organoids to explore the consequences of ZIKV infec-tion during neurogenesis and growth with 3D culture mod-els. Human iPS-derived NSCs were exposed to ZIKV (MOI 0.25 to 0.0025). After 24 hours, ZIKV was detected in NSCs (Fig. 1, A to D), when viral envelope protein was shown in 10.10% (MOI 0.025) and 21.7% (MOI 0.25) of cells exposed to ZIKV (Fig. 1E). Viral RNA was also detected in the superna-
tant of infected NSCs (MOI 0.0025) by qRT-PCR (Fig. 1F), supporting productive infection.
To investigate the effects of ZIKV during neural differen-tiation, mock- and ZIKV-infected NSCs were cultured as neurospheres. After 3 days in vitro, mock NSCs generated round neurospheres. However, ZIKV-infected NSCs generat-ed neurospheres with morphological abnormalities and cell detachment (Fig. 2B). After 6 days in vitro (DIV), hundreds of neurospheres grew under mock conditions (Fig. 2, C and E). Strikingly, in ZIKV-infected NSCs (MOI 2.5 to 0.025) only a few neurospheres survived (Fig. 2, D and E).
Mock neurospheres presented expected ultrastructural morphology of nucleus and mitochondria (Fig. 3A). ZIKV-infected neurospheres revealed the presence of viral parti-cles, similarly to those observed in murine glial and neu-ronal cells (16). ZIKV was bound to the membranes and observed in mitochondria and vesicles of cells within infect-ed neurospheres (Fig. 3, B and F, arrows). Apoptotic nuclei, a hallmark of cell death, were observed in all ZIKV-infected neurospheres analyzed (Fig. 3B). Of note, ZIKV-infected cells in neurospheres presented smooth membrane struc-tures (SMS) (Fig. 3, B and F), similarly to those previously described in other cell types infected with dengue virus (17). These results suggest that ZIKV induces cell death in human neural stem cells and thus impairs the formation of neuro-spheres.
To further investigate the impact of ZIKV infection dur-ing neurogenesis, human iPS-derived brain organoids (18) were exposed with ZIKV, and followed for 11 days in vitro (Fig. 4). The growth rate of 12 individual organoids (6 per condition) was measured during this period (Fig. 4, A and D). As a result of ZIKV infection, the average growth area of
Zika virus impairs growth in human neurospheres and brain organoids Patricia P. Garcez,1,2* Erick Correia Loiola,2† Rodrigo Madeiro da Costa,2† Luiza M. Higa,3† Pablo Trindade,2† Rodrigo Delvecchio,3 Juliana Minardi Nascimento,2,4 Rodrigo Brindeiro,3 Amilcar Tanuri,3 Stevens K. Rehen2,1* 1Institute of Biomedical Sciences, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil. 2D'Or Institute for Research and Education (IDOR), Rio de Janeiro, Brazil. 3Institute of Biology, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil. 4Institute of Biology, State University of Campinas, Campinas, Brazil.
*Corresponding author. Email: [email protected] (P.P.G.); [email protected] (S.K.R.)
†These authors contributed equally to this work.
Since the emergence of Zika virus (ZIKV), reports of microcephaly have increased significantly in Brazil; however, causality between the viral epidemic and malformations in fetal brains needs further confirmation. Here, we examine the effects of ZIKV infection in human neural stem cells growing as neurospheres and brain organoids. Using immunocytochemistry and electron microscopy, we show that ZIKV targets human brain cells, reducing their viability and growth as neurospheres and brain organoids. These results suggest that ZIKV abrogates neurogenesis during human brain development.
First release: 14 April 2016 www.sciencemag.org (Page numbers not final at time of first release) 1
on
Apr
il 22
, 201
6ht
tp://
scie
nce.
scie
ncem
ag.o
rg/
Dow
nloa
ded
from

ZIKV-exposed organoids was reduced by 40% when com-pared to brain organoids under mock conditions (0.624 mm2 ± 0.064 ZIKV-exposed organoids versus 1.051 mm2 ± 0.1084 mock-infected organoids normalized, Fig. 4E).
In addition to MOCK infection, we used dengue virus 2 (DENV2), a flavivirus with genetic similarities to ZIKV (11, 19), as an additional control group. One day after viral expo-sure, DENV2 infected human NSCs with a similar rate as ZIKV (fig. S1, A and B). However, after 3 days in vitro, there was no increase in caspase 3/7 mediated cell death induced by DENV2 with the same 0.025 MOI adopted for ZIKV in-fection (fig. S1, C and D). On the other hand, ZIKV induced caspase 3/7 mediated cell death in NSCs, similarly to the results described by Tang and colleagues (15). After 6 days in vitro, there is a significant difference in cell viability be-tween ZIKV-exposed NSCs compared to DENV2-exposed NSCs (fig. S1, E and F). In addition, neurospheres exposed to DENV2 display a round morphology such as uninfected neurospheres after 6 days in vitro (fig. S1G). Finally, there was no reduction of growth in brain organoids exposed to DENV2 for 11 days compared to MOCK (1.023 mm2 ± 0.1308 DENV2-infected organoids versus 1.011 mm2 ± 0.2471 mock-infected organoids normalized, fig. S1, H and I). These re-sults suggest that the deleterious consequences of ZIKV in-fection in human NSCs, neurospheres and brain organoids are not a general feature of the flavivirus family. Neuro-spheres and brain organoids are complementary models to study embryonic brain development in vitro (20, 21). While neurospheres present the very early characteristics of neu-rogenesis, brain organoids recapitulate the orchestrated cellular and molecular early events comparable to the first trimester fetal neocortex, including gene expression and cortical layering (18, 22). Our results demonstrate that ZIKV induces cell death in human iPS-derived neural stem cells, disrupts the formation of neurospheres and reduces the growth of organoids (fig. S2), indicating that ZIKV infection in models that mimics the first trimester of brain develop-ment may result in severe damage. Other studies are neces-sary to further characterize the consequences of ZIKV infection during different stages of fetal development.
Cell death impairing brain enlargement, calcification and microcephaly is well described in congenital infections with TORCHS (3, 23, 24). Our results, together with recent reports showing brain calcification in microcephalic fetuses and newborns infected with ZIKV (10, 14) reinforce the growing body of evidence connecting congenital ZIKV out-break to the increased number of reports of brain malfor-mations in Brazil.
REFERENCES AND NOTES 1. E. C. Gilmore, C. A. Walsh, Genetic causes of microcephaly and lessons for
neuronal development. WIREs Dev. Biol. 2, 461–478 (2013). Medline doi:10.1002/wdev.89
2. C. G. Woods, J. Bond, W. Enard, Autosomal recessive primary microcephaly
(MCPH): A review of clinical, molecular, and evolutionary findings. Am. J. Hum. Genet. 76, 717–728 (2005). Medline doi:10.1086/429930
3. N. Neu, J. Duchon, P. Zachariah, TORCH infections. Clin. Perinatol. 42, 77–103 (2015). Medline doi:10.1016/j.clp.2014.11.001
4. C. Zanluca, V. C. Melo, A. L. Mosimann, G. I. Santos, C. N. Santos, K. Luz, First report of autochthonous transmission of Zika virus in Brazil. Mem. Inst. Oswaldo Cruz 110, 569–572 (2015). Medline doi:10.1590/0074-02760150192
5. G. S. Campos, A. C. Bandeira, S. I. Sardi, Zika virus outbreak, Bahia, Brazil. Emerg. Infect. Dis. 21, 1885–1886 (2015). Medline doi:10.3201/eid2110.150847
6. E. B. Hayes, Zika virus outside Africa. Emerg. Infect. Dis. 15, 1347–1350 (2009). Medline doi:10.3201/eid1509.090442
7. G. W. A. Dick, Zika virus. II. Pathogenicity and physical properties. Trans. R. Soc. Trop. Med. Hyg. 46, 521–534 (1952). Medline doi:10.1016/0035-9203(52)90043-6
8. D. Musso, C. Roche, E. Robin, T. Nhan, A. Teissier, V. M. Cao-Lormeau, Potential sexual transmission of Zika virus. Emerg. Infect. Dis. 21, 359–361 (2015). Medline doi:10.3201/eid2102.141363
9. B. D. Foy, K. C. Kobylinski, J. L. Chilson Foy, B. J. Blitvich, A. Travassos da Rosa, A. D. Haddow, R. S. Lanciotti, R. B. Tesh, Probable non-vector-borne transmission of Zika virus, Colorado, USA. Emerg. Infect. Dis. 17, 880–882 (2011). Medline doi:10.3201/eid1705.101939
10. M. Sarno, G. A. Sacramento, R. Khouri, M. S. do Rosário, F. Costa, G. Archanjo, L. A. Santos, N. Nery Jr., N. Vasilakis, A. I. Ko, A. R. de Almeida, Zika virus infection and stillbirths: A case of hydrops fetalis, hydranencephaly and fetal demise. PLOS Negl. Trop. Dis. 10, e0004517 (2016). Medline doi:10.1371/journal.pntd.0004517
11. G. Calvet, R. S. Aguiar, A. S. Melo, S. A. Sampaio, I. de Filippis, A. Fabri, E. S. Araujo, P. C. de Sequeira, M. C. de Mendonça, L. de Oliveira, D. A. Tschoeke, C. G. Schrago, F. L. Thompson, P. Brasil, F. B. Dos Santos, R. M. Nogueira, A. Tanuri, A. M. de Filippis, Detection and sequencing of Zika virus from amniotic fluid of fetuses with microcephaly in Brazil: A case study. Lancet Infect. Dis. 10.1016/S1473-3099(16)00095-5 (2016). Medline
12. A. S. Oliveira Melo, G. Malinger, R. Ximenes, P. O. Szejnfeld, S. Alves Sampaio, A. M. Bispo de Filippis, Zika virus intrauterine infection causes fetal brain abnormality and microcephaly: Tip of the iceberg? Ultrasound Obstet. Gynecol. 47, 6–7 (2016). Medline doi:10.1002/uog.15831
13. R. B. Martines, J. Bhatnagar, M. K. Keating, L. Silva-Flannery, A. Muehlenbachs, J. Gary, C. Goldsmith, G. Hale, J. Ritter, D. Rollin, W. J. Shieh, K. G. Luz, A. M. Ramos, H. P. Davi, W. Kleber de Oliveria, R. Lanciotti, A. Lambert, S. Zaki, Notes from the field: Evidence of Zika virus infection in brain and placental tissues from two congenitally infected newborns and two fetal losses - Brazil, 2015. MMWR Morb. Mortal. Wkly. Rep. 65, 159–160 (2016). Medline doi:10.15585/mmwr.mm6506e1
14. J. Mlakar, M. Korva, N. Tul, M. Popović, M. Poljšak-Prijatelj, J. Mraz, M. Kolenc, K. Resman Rus, T. Vesnaver Vipotnik, V. Fabjan Vodušek, A. Vizjak, J. Pižem, M. Petrovec, T. Avšič Županc, Zika virus associated with microcephaly. N. Engl. J. Med. 374, 951–958 (2016). Medline doi:10.1056/NEJMoa1600651
15. H. Tang, C. Hammack, S. C. Ogden, Z. Wen, X. Qian, Y. Li, B. Yao, J. Shin, F. Zhang, E. M. Lee, K. M. Christian, R. A. Didier, P. Jin, H. Song, G. L. Ming, Zika virus infects human cortical neural progenitors and attenuates their growth. Cell Stem Cell 18, 1–4 (2016). Medline
16. T. M. Bell, E. J. Field, H. K. Narang, Zika virus infection of the central nervous system of mice. Arch. Gesamte Virusforsch. 35, 183–193 (1971). Medline doi:10.1007/BF01249709
17. C. Grief, R. Galler, L. M. C. Côrtes, O. M. Barth, Intracellular localisation of dengue-2 RNA in mosquito cell culture using electron microscopic in situ hybridisation. Arch. Virol. 142, 2347–2357 (1997). Medline doi:10.1007/s007050050247
18. M. A. Lancaster, M. Renner, C. A. Martin, D. Wenzel, L. S. Bicknell, M. E. Hurles, T. Homfray, J. M. Penninger, A. P. Jackson, J. A. Knoblich, Cerebral organoids model human brain development and microcephaly. Nature 501, 373–379 (2013). Medline doi:10.1038/nature12517
19. R. S. Lanciotti, O. L. Kosoy, J. J. Laven, J. O. Velez, A. J. Lambert, A. J. Johnson, S. M. Stanfield, M. R. Duffy, Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 14, 1232–1239 (2008). Medline doi:10.3201/eid1408.080287
First release: 14 April 2016 www.sciencemag.org (Page numbers not final at time of first release) 2
on
Apr
il 22
, 201
6ht
tp://
scie
nce.
scie
ncem
ag.o
rg/
Dow
nloa
ded
from

20. B. A. Reynolds, S. Weiss, Generation of neurons and astrocytes from isolated cells of the adult mammalian central nervous system. Science 255, 1707–1710 (1992). Medline doi:10.1126/science.1553558
21. M. A. Lancaster, J. A. Knoblich, Generation of cerebral organoids from human pluripotent stem cells. Nat. Protoc. 9, 2329–2340 (2014). Medline doi:10.1038/nprot.2014.158
22. J. G. Camp, F. Badsha, M. Florio, S. Kanton, T. Gerber, M. Wilsch-Bräuninger, E. Lewitus, A. Sykes, W. Hevers, M. Lancaster, J. A. Knoblich, R. Lachmann, S. Pääbo, W. B. Huttner, B. Treutlein, Human cerebral organoids recapitulate gene expression programs of fetal neocortex development. Proc. Natl. Acad. Sci. U.S.A. 112, 15672–15677 (2015). Medline
23. Z. W. Naing, G. M. Scott, A. Shand, S. T. Hamilton, W. J. van Zuylen, J. Basha, B. Hall, M. E. Craig, W. D. Rawlinson, Congenital cytomegalovirus infection in pregnancy: A review of prevalence, clinical features, diagnosis and prevention. Aust. N. Z. J. Obstet. Gynaecol. 56, 9–18 (2016). Medline doi:10.1111/ajo.12408
24. D. V. Vasconcelos-Santos, D. O. Machado Azevedo, W. R. Campos, F. Oréfice, G. M. Queiroz-Andrade, E. V. Carellos, R. M. Castro Romanelli, J. N. Januário, L. M. Resende, O. A. Martins-Filho, A. C. de Aguiar Vasconcelos Carneiro, R. W. Almeida Vitor, W. T. Caiaffa, UFMG Congenital Toxoplasmosis Brazilian Group, Congenital toxoplasmosis in southeastern Brazil: Results of early ophthalmologic examination of a large cohort of neonates. Ophthalmology 116, 2199–205.e1 (2009). Medline doi:10.1016/j.ophtha.2009.04.042
25. B. S. Paulsen, C. S. Souza, L. Chicaybam, M. H. Bonamino, M. Bahia, S. L. Costa, H. L. Borges, S. K. Rehen, Agathisflavone enhances retinoic acid-induced neurogenesis and its receptors α and β in pluripotent stem cells. Stem Cells Dev. 20, 1711–1721 (2011). Medline doi:10.1089/scd.2010.0446
26. Y. Yan, S. Shin, B. S. Jha, Q. Liu, J. Sheng, F. Li, M. Zhan, J. Davis, K. Bharti, X. Zeng, M. Rao, N. Malik, M. C. Vemuri, Efficient and rapid derivation of primitive neural stem cells and generation of brain subtype neurons from human pluripotent stem cells. Stem Cells Transl. Med. 2, 862–870 (2013). Medline doi:10.5966/sctm.2013-0080
27. E. A. Henchal, M. K. Gentry, J. M. McCown, W. E. Brandt, Dengue virus-specific and flavivirus group determinants identified with monoclonal antibodies by indirect immunofluorescence. Am. J. Trop. Med. Hyg. 31, 830–836 (1982). Medline
ACKNOWLEDGMENTS
The authors thank the lab-crew members Marcelo Costa, Ismael Gomes, Gabriela Vitória, Jarek Sochacki and Matías Alloati for providing technical support, cultures of human iPS cells and brain organoids. We acknowledge Dr. Ortrud Monika Barth for comments on the electron micrographs. We also thank Dr Fabricio Pamplona for Mind the Graph assistance and Centro Nacional de Biologia Estrutural e Bioimagem (CENABIO) for the use of the Electron Microscopy. Funds (not specifically for Zika virus studies) were provided by the Brazilian Development Bank (BNDES); Funding Authority for Studies and Projects (FINEP); National Council of Scientific and Technological Development (CNPq); Foundation for Research Support in the State of Rio de Janeiro (FAPERJ); and fellowships from the São Paulo Research Foundation (FAPESP, grant #2014/21035-0) and Coordination for the Improvement of Higher Education Personnel (CAPES). All protocols and procedures were approved by the institutional research ethics committee of Hospital Copa D'Or (CEPCOPADOR) under # 727.269. The authors declare no competing financial interests.
SUPPLEMENTARY MATERIALS www.sciencemag.org/cgi/content/full/science.aaf6116/DC1 Materials and Methods Figs. S1 and S2 References (25–27) 2 March 2016; accepted 4 April 2016 Published online 14 April 2016 10.1126/science.aaf6116
First release: 14 April 2016 www.sciencemag.org (Page numbers not final at time of first release) 3
on
Apr
il 22
, 201
6ht
tp://
scie
nce.
scie
ncem
ag.o
rg/
Dow
nloa
ded
from

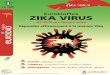
Fig. 1. ZIKV infects human neural stem cells. Confocal microscopy images of iPS-derived NSCs double stained for (A) ZIKV in the cytoplasm, and (B) SOX2 in nuclei, one day after virus infection. (C) DAPI staining, (D) merged channels show perinuclear localization of ZIKV. Bar = 100 μm. (E) Percentage of ZIKV infected SOX2 positive cells (MOI 0.25 and 0.025). (F) RT-PCR analysis of ZIKV RNA extracted from supernatants of mock and ZIKV-infected neurospheres (MOI 0.0025) after 3 DIV, showing amplification only in infected cells. RNA was extracted, qPCR performed and virus production normalized to 12h post-infection controls. Data presented as mean ± SEM, n=5, Student’s t test, *p < 0.05, **p < 0.01.
First release: 14 April 2016 www.sciencemag.org (Page numbers not final at time of first release) 4
on
Apr
il 22
, 201
6ht
tp://
scie
nce.
scie
ncem
ag.o
rg/
Dow
nloa
ded
from

Fig. 2. ZIKV alters morphology and halts the growth of human neurospheres. (A) Control neurosphere displays spherical morphology after 3 DIV. (B) Infected neurosphere showed morphological abnormalities and cell detachment after 3 DIV. (C) Culture well-plate containing hundreds of mock neurospheres after 6 DIV. (D) ZIKV-infected well-plate (MOI 2.5-0.025) containing few neurospheres after 6 DIV. Bar = 250 μm in (A) and (B), and 1 cm in (C) and (D). (E) Quantification of the number of neurospheres in different MOI. Data presented as mean ± SEM, n=3, Student’s t test, ***p < 0.01.
First release: 14 April 2016 www.sciencemag.org (Page numbers not final at time of first release) 5
on
Apr
il 22
, 201
6ht
tp://
scie
nce.
scie
ncem
ag.o
rg/
Dow
nloa
ded
from

Fig. 3. ZIKV induces death in human neurospheres. Ultrastructure of mock- and ZIKV-infected neurospheres after 6 days in vitro. (A) Mock-infected neurosphere showing cell processes and organelles, (B) ZIKV-infected neurosphere shows pyknotic nucleus, swollen mitochondria, smooth membrane structures and viral envelopes (arrow). Arrows point viral envelopes on cell surface (C), inside mitochondria (D), endoplasmic reticulum (E) and close to smooth membrane structures (F). Bar = 1 μm in (A) and (B) and 0.2 μm in (C) to (F). m = mitochondria; n = nucleus; sms = smooth membrane structures.
First release: 14 April 2016 www.sciencemag.org (Page numbers not final at time of first release) 6
on
Apr
il 22
, 201
6ht
tp://
scie
nce.
scie
ncem
ag.o
rg/
Dow
nloa
ded
from

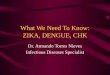
Fig. 4. ZIKV reduces the growth rate of human brain organoids. 35 days old brain organoids were infected with (A) MOCK and (B) ZIKV for 11 days in vitro. ZIKV-infected brain organoids show reduction in growth compared with MOCK. Arrows point to detached cells. Organoid area was measured before and after 11 days exposure with (C) MOCK and (D) ZIKV in vitro. Plotted quantification represent the growth rate. (E) Quantification of the average of mock- and ZIKV-infected organoid area 11 days after infection in vitro. Data presented as mean ± SEM, n=6, Student’s t test, *p < 0.05.
First release: 14 April 2016 www.sciencemag.org (Page numbers not final at time of first release) 7
on
Apr
il 22
, 201
6ht
tp://
scie
nce.
scie
ncem
ag.o
rg/
Dow
nloa
ded
from

published online April 10, 2016(April 10, 2016) Nascimento, Rodrigo Brindeiro, Amilcar Tanuri and Stevens K. RehenLuiza M. Higa, Pablo Trindade, Rodrigo Delvecchio, Juliana Minardi Patricia P. Garcez, Erick Correia Loiola, Rodrigo Madeiro da Costa,organoidsZika virus impairs growth in human neurospheres and brain
Editor's Summary
This copy is for your personal, non-commercial use only.
Article Tools
http://science.sciencemag.org/content/early/2016/04/08/science.aaf6116tools: Visit the online version of this article to access the personalization and article
Permissionshttp://www.sciencemag.org/about/permissions.dtlObtain information about reproducing this article:
is a registered trademark of AAAS. Scienceall rights reserved. The title Washington, DC 20005. Copyright 2016 by the American Association for the Advancement of Science;December, by the American Association for the Advancement of Science, 1200 New York Avenue NW,
(print ISSN 0036-8075; online ISSN 1095-9203) is published weekly, except the last week inScience
on
Apr
il 22
, 201
6ht
tp://
scie
nce.
scie
ncem
ag.o
rg/
Dow
nloa
ded
from

Brief Report
Zika Virus Infects HumanCortical Neural Progenitorsand Attenuates Their Growth
Graphical Abstract
Highlights
d Zika virus (ZIKV) infects human embryonic cortical neural
progenitor cells (hNPCs)
d ZIKV-infected hNPCs produce infectious ZIKV particles
d ZIKV infection leads to increased cell death of hNPCs
d ZIKV infection dysregulates cell cycle and transcription in
hNPCs
Authors
Hengli Tang, Christy Hammack,
Sarah C. Ogden, ..., Peng Jin,
Hongjun Song, Guo-li Ming
[email protected] (H.T.),[email protected] (H.S.),[email protected] (G.-l.M.)
In Brief
The suspected link between ZIKV
infection and microcephaly is an urgent
global health concern. Tang et al. report
that ZIKV virus directly infects human
cortical neural progenitor cells with high
efficiency, resulting in stunted growth of
this cell population and transcriptional
dysregulation.
Accession Numbers
GSE78711
Tang et al., 2016, Cell Stem Cell 18, 1–4June 2, 2016 ª2016 Elsevier Inc.http://dx.doi.org/10.1016/j.stem.2016.02.016

Cell Stem Cell
Brief Report
Zika Virus Infects Human Cortical NeuralProgenitors and Attenuates Their GrowthHengli Tang,1,11,* Christy Hammack,1,11 Sarah C. Ogden,1,11 Zhexing Wen,2,3,11 Xuyu Qian,2,4,11 Yujing Li,9 Bing Yao,9
Jaehoon Shin,2,5 Feiran Zhang,9 Emily M. Lee,1 Kimberly M. Christian,2,3 Ruth A. Didier,10 Peng Jin,9
Hongjun Song,2,3,5,6,7,* and Guo-li Ming2,3,5,6,7,8,*1Department of Biological Science, Florida State University, Tallahassee, FL 32306, USA2Institute for Cell Engineering3Department of Neurology4Biomedical Engineering Graduate Program5Cellular and Molecular Medicine Graduate Program6Solomon Snyder Department of Neuroscience7Kavli Neuroscience Discovery Institute8Department of Psychiatry and Behavioral Sciences
Johns Hopkins University School of Medicine, Baltimore, MD 21025, USA9Department of Human Genetics, Emory University School of Medicine, Atlanta, GA 30322, USA10College of Medicine, Florida State University, Tallahassee, FL 32306, USA11Co-first author*Correspondence: [email protected] (H.T.), [email protected] (H.S.), [email protected] (G.-l.M.)
http://dx.doi.org/10.1016/j.stem.2016.02.016
SUMMARY
The suspected link between infection by Zika virus(ZIKV), a re-emerging flavivirus, and microcephalyis an urgent global health concern. The direct targetcells of ZIKV in the developing human fetus are notclear. Here we show that a strain of the ZIKV,MR766, serially passaged in monkey and mosquitocells efficiently infects human neural progenitor cells(hNPCs) derived from induced pluripotent stem cells.Infected hNPCs further release infectious ZIKV parti-cles. Importantly, ZIKV infection increases cell deathand dysregulates cell-cycle progression, resulting inattenuated hNPC growth. Global gene expressionanalysis of infected hNPCs reveals transcriptionaldysregulation, notably of cell-cycle-related path-ways. Our results identify hNPCs as a direct ZIKVtarget. In addition, we establish a tractable experi-mental model system to investigate the impact andmechanism of ZIKV on human brain developmentand provide a platform to screen therapeutic com-pounds.
Zika virus (ZIKV), a mosquito-borne flavivirus, is now reported to
be circulating in 26 countries and territories in Latin America and
the Caribbean (Petersen et al., 2016). While infected individuals
can often be asymptomatic or have only mild symptoms, of
mounting concern are reports linking ZIKV infection to fetal
and newborn microcephaly and serious neurological complica-
tions, such as Guillain-Barre syndrome (Petersen et al., 2016).
The World Health Organization declared a Public Health Emer-
gency of International Concern on February 1 of 2016 (Heymann
et al., 2016). ZIKV infects human skin cells, consistent with its
major transmission route (Hamel et al., 2015). ZIKVwas detected
in the amniotic fluid of two pregnant women whose fetuses had
been diagnosedwithmicrocephaly (Calvet et al., 2016), suggest-
ing that ZIKV can cross the placental barrier. ZIKV was also
found in microcephalic fetal brain tissue (Mlakar et al., 2016).
Because so little is known about direct cell targets and mecha-
nisms of ZIKV, and because access to fetal human brain tissue
is limited, there is an urgent need to develop a new strategy to
determine whether there is a causal relationship between ZIKV
infection and microcephaly. Here we used human induced
pluripotent stem cells (hiPSCs) as an in vitro model to investigate
whether ZIKV directly infects human neural cells and the nature
of its impact.
We obtained a ZIKV stock from the infected rhesus Macaca
cell line LLC-MK2. We passaged the virus in the mosquito C6/
C36 cell line and titered collected ZIKV on Vero cells, an inter-
feron-deficient monkey cell line commonly used to titer viruses.
Sequences of multiple RT-PCR fragments generated from
this stock (Figure S1A) matched the sequence of MR766, the
original ZIKV strain that likely passed from an infected rhesus
monkey to mosquitos (Dick et al., 1952). We first tested several
human cell lines and found varying levels of susceptibility to
ZIKV infection (Table S1). Notably, the human embryonic kidney
cell line HEK293T showed low permissiveness for ZIKV infection
(Figure S1C).
To identify direct target cells of ZIKV in the human neural line-
age, we used a highly efficient protocol to differentiate hiPSCs
into forebrain-specific human neural progenitor cells (hNPCs),
which can be further differentiated into cortical neurons (Wen
et al., 2014). The titer of ZIKV in the infected humans is currently
unknown. We performed infections at a low multiplicity of infec-
tion (MOI < 0.1) and the medium containing virus inoculum was
removed after a 2 hr incubation period. Infection rates were
then quantified 56 hr later with RT-PCR using MR766-specific
primers (Figure S1A) and with immunocytochemistry using an
anti-ZIKV envelope antibody (Figures 1A and 1B). The hNPCs
Cell Stem Cell 18, 1–4, June 2, 2016 ª2016 Elsevier Inc. 1
Please cite this article in press as: Tang et al., Zika Virus Infects Human Cortical Neural Progenitors and Attenuates Their Growth, Cell Stem Cell (2016),http://dx.doi.org/10.1016/j.stem.2016.02.016

were readily infected by ZIKV in vitro, with the infection
spreading to 65%–90% of the cells within 3 days of inoculation
(Figures 1A and 1C). Quantitative analysis showed similar results
for hNPCs derived from hiPSC lines of two different subjects
(Figure 1C). As a control, we also exposed human embryonic
stem cells (hESCs), hiPSCs, and immature cortical neurons to
ZIKV under the same conditions. hESCs and hiPSCs could
also be infected by ZIKV, but the infection was limited to a few
cells at the colony edge with reduced expression of the pluripo-
tent marker NANOG (Figures 1C and S1D; Table S1). Immature
neurons differentiated from hNPCs also exhibited lower levels
of infection under our conditions (Figures 1B and 1C). Together,
these results establish that hNPCs, a constitutive population of
the developing embryonic brain, are a direct cell target of ZIKV.
ZIKV envelope immunostaining exhibited the characteristic
intracellular ‘‘virus factory’’ pattern of flaviviruses (Romero-
Brey and Bartenschlager, 2014) (Figure 1A). We therefore tested
infectivity using supernatant from infected hNPCs and observed
robust infection of Vero cells (Figure 1D), indicating that produc-
tive infection of hNPCs leads to efficient secretion of infectious
ZIKV particles.
We next determined the potential impact of ZIKV infection on
hNPCs. We found a 29.9% ± 6.6% reduction in the total number
of viable cells 66–72 hr after ZIKV infection, as compared to the
mock infection (n = 3). Interestingly, ZIKV infection led to signif-
icantly higher caspase-3 activation in hNPCs 3 days after infec-
tion, as compared to the mock infection, suggesting increased
cell death (Figures 2A and 2B). Furthermore, analysis of DNA
content by flow cytometry suggested cell-cycle perturbation of
infected hNPCs (Figures 2C and S2A). Therefore, ZIKV infection
of hNPCs leads to attenuated growth of this cell population that
is due, at least partly, to both increased cell death and cell-cycle
dysregulation.
To investigate the impact of ZIKV infection on hNPCs at the
molecular level, we employed global transcriptome analyses
(RNA-seq). Our genome-wide analyses identified a large number
of differentially expressed genes upon viral infection (Figure S2B
and Table S2). Gene Ontology analyses revealed a particular
A BZIKVE DAPI+
ZIK
VM
ock
+ ZI
KV
Moc
k
ZIKVE DAPI
C D
hNPC neuron
VeroZIKVE DAPI
hESC hiPSC hNPCC line
hNPCD line
NeuronDay 1
NeuronDay 9
0
20
40
60
80
100
Infe
ctio
n ra
te (%
)
* *
5 5 5 566
*
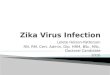
Figure 1. ZIKV Infects hiPSC-Derived Neural Progenitor Cells with High Efficiency
(A and B) Sample confocal images of forebrain-specific hNPCs (A) and immature neurons (B) 56 hr after infection with ZIKV supernatant, immunostained for ZIKV
envelop protein (ZIKVE; green) and DAPI (gray). Cells were differentiated from the C1-2 hiPSC line. Scale bars, 20 mm.
(C) Quantification of infection efficiency for different cell types, including hESCs, hiPSCs, hNPCS derived from two different hiPSCs, and immature neurons 1 or
9 days after differentiation from hNPCs. Both hESCs and hiPSCs were analyzed 72 hr after infection, whereas all other cells were analyzed 56 hr after infection.
Numbers associated with bar graphs indicate numbers of independent experiments. Values represent mean ± SD (*p < 0.01; Student’s t test).
(D) Production of infectious ZIKV particles by infected hNPCs. Supernatant from hNPC cultures 72 hr after ZIKV infectionwas collected and added to Vero cells for
2 hr. The Vero cells were further cultured for 48 hr. Shown are sample images of ZIKVE immunostaining (green) and DAPI (gray). Scale bars, 20 mm.
See also Figure S1 and Table S1.
2 Cell Stem Cell 18, 1–4, June 2, 2016 ª2016 Elsevier Inc.
Please cite this article in press as: Tang et al., Zika Virus Infects Human Cortical Neural Progenitors and Attenuates Their Growth, Cell Stem Cell (2016),http://dx.doi.org/10.1016/j.stem.2016.02.016

enrichment of downregulated genes in cell-cycle-related path-
ways (Figure 2D), which is consistent with our flow cytometry
findings (Figure 2C). Upregulated genes were primarily enriched
in transcription, protein transport, and catabolic processes
(Figure 2E). Consistent with increased caspase-3 activation
observed by immunocytochemistry (Figures 2A and 2B), RNA-
seq analysis revealed upregulation of genes, including cas-
pase-3, involved in the regulation of the apoptotic pathway
(Figure 2E). These global transcriptome datasets not only sup-
port our cell biology findings but also provide a valuable resource
for the field.
It is not known whether specific strains of ZIKV circulating in
geographically diverse parts of the world differ in their ability to
impact neural development, and the stain we used had been
discovered prior to the current reports of a potential epidemio-
logic link between ZIKV and microcephaly. Nevertheless, our re-
sults clearly demonstrate that ZIKV can directly infect hNPCs
in vitro with high efficiency and that infection of hNPCs leads
to attenuated population growth through virally induced
caspase-3-mediated apoptosis and cell-cycle dysregulation.
Infected hNPCs also release infectious viral particles, which pre-
sents a significant clinical challenge for developing effective
therapeutics to arrest or block the impact of infection. Future
studies using the hiPSC/hNPC model can determine whether
various ZIKV strains impact hNPCs differently and, conversely,
whether a single ZIKV strain differentially affects hNPCs from
hiPSCs of various human populations.
Flaviviruses tend to have broad cellular tropisms and multiple
factors contribute to pathogenic outcomes, including specific
cellular response and tissue accessibility. Dengue virus infects
cells of several lineages and hematopoietic cells play an essen-
tial role in the associated pathogenesis (Pham et al., 2012). West
Nile virus infects epithelial cells of multiple tissues and can be
neuroinvasive (Suthar et al., 2013).We note that ZIKV also infects
other human cell types, including skin cells and fibroblasts
(Hamel et al., 2015), and it remains unknown how ZIKV may
gain access to the fetal brain (Mlakar et al., 2016). The capacity
of ZIKV to infect hNPCs and attenuate their growth underscores
the urgent need for more research into the role of these cells in
putative ZIKV-related neuropathology. The finding that ZIKV
also infects immature neurons raises critical questions about
pathological effects on neurons and other neural cell types in
+ ZIKV Mock0
5
10
15
20
Cas
3+ cel
ls (%
)
A CZIKVE Cas3 DAPI+
ZIK
VM
ock
Mock
Infected
Mixture
0
2000
4000
0
500
1000
0
300
600
25000 50000 75000 100000
25000 50000 75000 100000
25000 50000 75000 100000
D ECell cycle
Cell cycle phaseM phase
Nuclear divisionMitosis
M phase of mitotic cell cycle
Cell cycle processOrganelle fission
DNA metabolic processMitotic cell cycle
TranscriptionRegulation of transcription
Protein localizationProtein transport
Establishment of protein localization
Intracellular transportRegulation of transcription, DNA-dependent
Modification-dependent macromolecule catabolic processModification-dependent protein catabolic process
Regulation of cell death
0 10 20 300 10 20 30-log10 Pvalue
B 2N 4N
*
-log10 Pvalue
Figure 2. ZIKV-Infected hNPCs Exhibit Increased Cell Death and Dysregulated Cell-Cycle Progression and Gene Expression
(A and B) Increased cell death of ZIKV-infected hNPCs. Shown in (A) are sample images of immunostaining of hNPCs for ZIKVE (green) and cleaved-caspase-3
(Cas3; red) and DAPI (gray) 72 hr after ZIKV infection. Scale bars, 20 mm. Shown in (B) is the quantification. Values represent mean ± SEM (n = 6; *p < 0.01;
Student’s t test).
(C) Cell-cycle perturbation of hNPCs infected by ZIKV. Shown are sample flow cytometry analyses of distributions of hNPCs (from the C1-2 line) at different
phases of the cell cycle 72 hr after ZIKV or mock infection. For the mixture sample, mock and infected hNPCs were mixed at a ratio of 1:1 following propidium
iodide staining of each sample.
(D and E) RNA-seq analysis of hNPCs (C1-2 line) 56 hr after ZIKV or mock infection. Genes with significant differences in expression between infected and
uninfected hNPCs were subjected to GO analyses. The top 10 most significant terms are shown for downregulated (D) and upregulated (E) genes, respectively.
The �log10 p values are indicated by bar plots. An additional term of regulation of programmed cell death is also shown for upregulated genes (E).
See also Figure S2 and Table S2.
Cell Stem Cell 18, 1–4, June 2, 2016 ª2016 Elsevier Inc. 3
Please cite this article in press as: Tang et al., Zika Virus Infects Human Cortical Neural Progenitors and Attenuates Their Growth, Cell Stem Cell (2016),http://dx.doi.org/10.1016/j.stem.2016.02.016

the brain, as well as potential long-term consequences. Intrigu-
ingly, an early animal study showed ZIKV infection of neurons
and astrocytes in mice and observed enlarged astrocytes (Bell
et al., 1971). Our study also raises the question of whether
ZIKV infects neural stem cells in adult humans (Bond et al., 2015).
In summary, our results fill a major gap in our knowledge about
ZIKV biology and serve as an entry point to establish a mecha-
nistic link between ZIKV and microcephaly. Our study also pro-
vides a tractable experimental system for modeling the impact
of ZIKV on neural development and for investigating underlying
cellular and molecular mechanisms. Of equal importance, our
hNPC model and robust cellular phenotype comprise a readily
scalable platform for high-throughput screens to prevent ZIKV
infection of hNPCs and to ameliorate its pathological effects dur-
ing neural development.
ACCESSION NUMBERS
The accession number for RNA-seq data reported in this paper is GEO:
GSE78711.
SUPPLEMENTAL INFORMATION
Supplemental Information for this article includes two figures, two tables, and
Supplemental Experimental Procedures and can be found with this article on-
line at http://dx.doi.org/10.1016/j.stem.2016.02.016.
AUTHOR CONTRIBUTIONS
H.T., H.S., and G.-l.M. conceived of the research, designed the study, and
wrote the manuscript. C.H., S.C.O., Z.W., and X.Q. performed experiments,
analyzed data, and contributed equally to this study. Y.L., B.Y., J.S., F.Z.,
and P.J. performed RNA-seq analysis, and E.M.L., K.M.C., and R.A.D. contrib-
uted to additional data collection. All authors commented on the manuscript.
ACKNOWLEDGMENTS
We thank Yichen Cheng, Taylor Lee, and Jianshe Lang of the Tang laboratory,
Lihong Liu and Yuan Cai of the Ming and Song laboratories, Luoxiu Huang of
the Jin laboratory for technical assistance, Zhiheng Xu and additional labora-
tory members for suggestions, and Timothy Megraw for assistance with
confocal imaging. H.T. thanks the College of Arts and Sciences and the
Department of Biological Science at Florida State University for seed funding.
This work was partially supported by NIH (AI119530/AI111250 to H.T.,
NS047344 to H.S., NS048271/NS095348 to G-l.M., and NS051630/
NS079625/MH102690 to P.J.), MSCRF (to H.S.), and start-up funding (to H.S.).
Received: February 24, 2016
Revised: February 28, 2016
Accepted: February 29, 2016
Published: March 4, 2016
REFERENCES
Bell, T.M., Field, E.J., and Narang, H.K. (1971). Zika virus infection of the cen-
tral nervous system of mice. Arch. Gesamte Virusforsch. 35, 183–193.
Bond, A.M., Ming, G.L., and Song, H. (2015). Adult mammalian neural stem
cells and neurogenesis: Five decades later. Cell Stem Cell 17, 385–395.
Calvet, G., Aguiar, R.S., Melo, A.S., Sampaio, S.A., de Filippis, I., Fabri, A.,
Araujo, E.S., de Sequeira, P.C., de Mendonca, M.C., de Oliveira, L., et al.
(2016). Detection and sequencing of Zika virus from amniotic fluid of fetuses
with microcephaly in Brazil: a case study. Lancet Infect. Dis. S1473-3099(16)
00095-5. http://dx.doi.org/10.1016/S1473-3099(16)00095-5.
Dick, G.W., Kitchen, S.F., and Haddow, A.J. (1952). Zika virus. I. Isolations and
serological specificity. Trans. R. Soc. Trop. Med. Hyg. 46, 509–520.
Hamel, R., Dejarnac, O.,Wichit, S., Ekchariyawat, P., Neyret, A., Luplertlop, N.,
Perera-Lecoin, M., Surasombatpattana, P., Talignani, L., Thomas, F., et al.
(2015). Biology of Zika virus infection in human skin cells. J. Virol. 89, 8880–
8896.
Heymann, D.L., Hodgson, A., Sall, A.A., Freedman, D.O., Staples, J.E.,
Althabe, F., Baruah, K., Mahmud, G., Kandun, N., Vasconcelos, P.F., et al.
(2016). Zika virus and microcephaly: why is this situation a PHEIC? Lancet
387, 719–721.
Mlakar, J., Korva, M., Tul, N., Popovi�c, M., Polj�sak-Prijatelj, M., Mraz, J.,
Kolenc, M., Resman Rus, K., Vesnaver Vipotnik, T., Fabjan Vodu�sek, V.,
et al. (2016). Zika virus associated with microcephaly. N. Engl. J. Med.
http://dx.doi.org/10.1056/NEJMoa1600651.
Petersen, E., Wilson, M.E., Touch, S., McCloskey, B., Mwaba, P., Bates, M.,
Dar, O., Mattes, F., Kidd, M., Ippolito, G., et al. (2016). Rapid spread of Zika
virus in the Americas - Implications for public health preparedness for
mass gatherings at the 2016 Brazil Olympic Games. Int. J. Infect. Dis. 44,
11–15.
Pham, A.M., Langlois, R.A., and TenOever, B.R. (2012). Replication in cells of
hematopoietic origin is necessary for Dengue virus dissemination. PLoS
Pathog. 8, e1002465.
Romero-Brey, I., and Bartenschlager, R. (2014). Membranous replication fac-
tories induced by plus-strand RNA viruses. Viruses 6, 2826–2857.
Suthar, M.S., Diamond, M.S., and Gale, M., Jr. (2013). West Nile virus infection
and immunity. Nat. Rev. Microbiol. 11, 115–128.
Wen, Z., Nguyen, H.N., Guo, Z., Lalli, M.A., Wang, X., Su, Y., Kim, N.S., Yoon,
K.J., Shin, J., Zhang, C., et al. (2014). Synaptic dysregulation in a human iPS
cell model of mental disorders. Nature 515, 414–418.
4 Cell Stem Cell 18, 1–4, June 2, 2016 ª2016 Elsevier Inc.
Please cite this article in press as: Tang et al., Zika Virus Infects Human Cortical Neural Progenitors and Attenuates Their Growth, Cell Stem Cell (2016),http://dx.doi.org/10.1016/j.stem.2016.02.016