FIT – Laboratory update
Sally C Benton
Consultant Clinical Biochemist, Berkshire and Surrey
Pathology Services (BSPS)
Director, Bowel Cancer Screening Southern Hub
Date: 26th February 2019
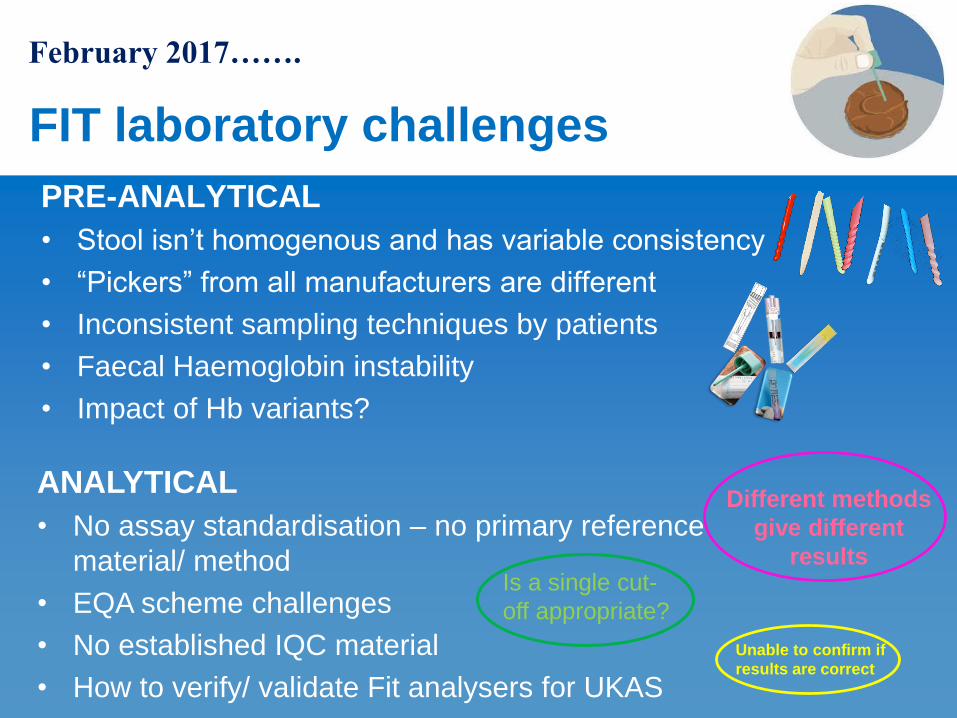
FIT laboratory challenges
PRE-ANALYTICAL
• Stool isn’t homogenous and has variable consistency
• “Pickers” from all manufacturers are different
• Inconsistent sampling techniques by patients
• Faecal Haemoglobin instability
• Impact of Hb variants?
February 2017…….
ANALYTICAL
• No assay standardisation – no primary reference
material/ method
• EQA scheme challenges
• No established IQC material
• How to verify/ validate Fit analysers for UKAS
Different methods
give different
results
Unable to confirm if
results are correct
Is a single cut-
off appropriate?

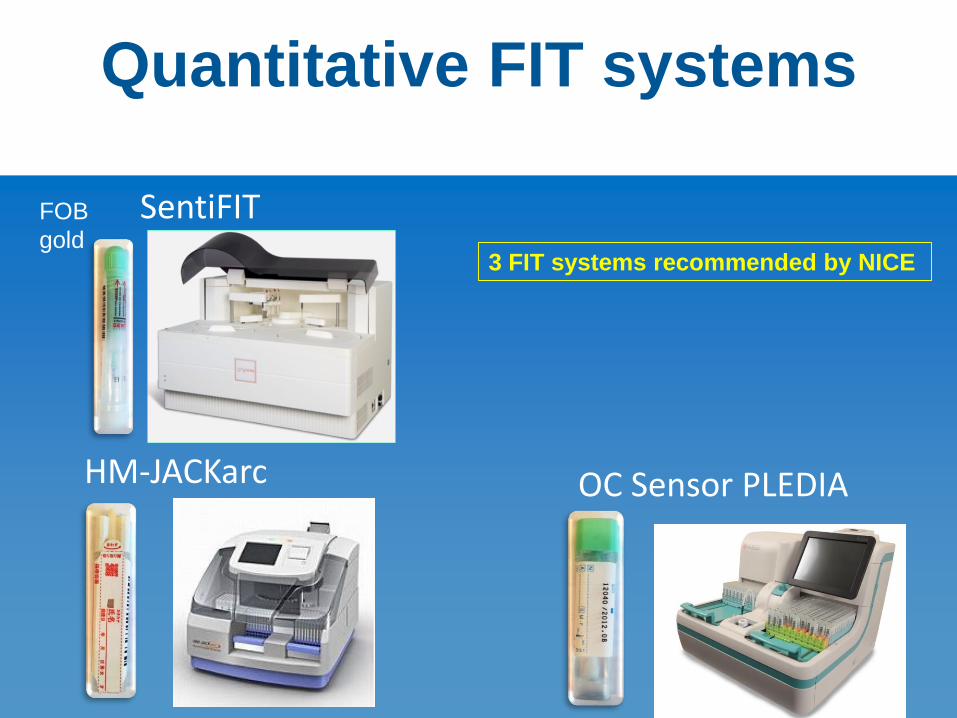
Quantitative FIT systems
SentiFIT
HM-JACKarc OC Sensor PLEDIA
NS Prime FOB
gold
Quantitative FIT systems
SentiFIT
HM-JACKarc OC Sensor PLEDIA
FOB
gold3 FIT systems recommended by NICE
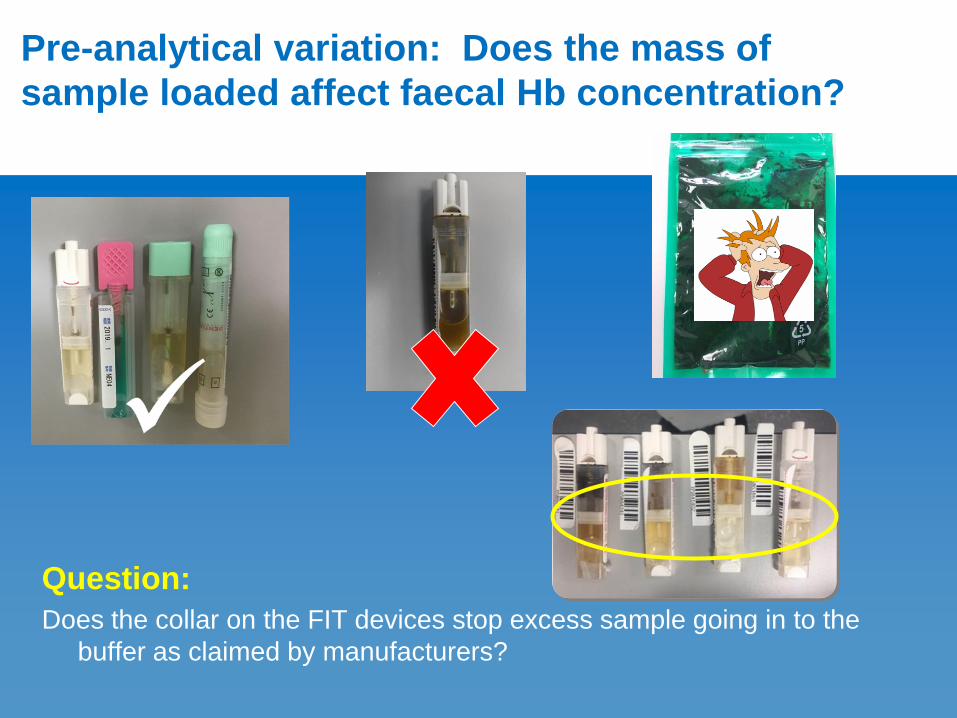
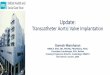
Question:
Does the collar on the FIT devices stop excess sample going in to the
buffer as claimed by manufacturers?
Pre-analytical variation: Does the mass of
sample loaded affect faecal Hb concentration?
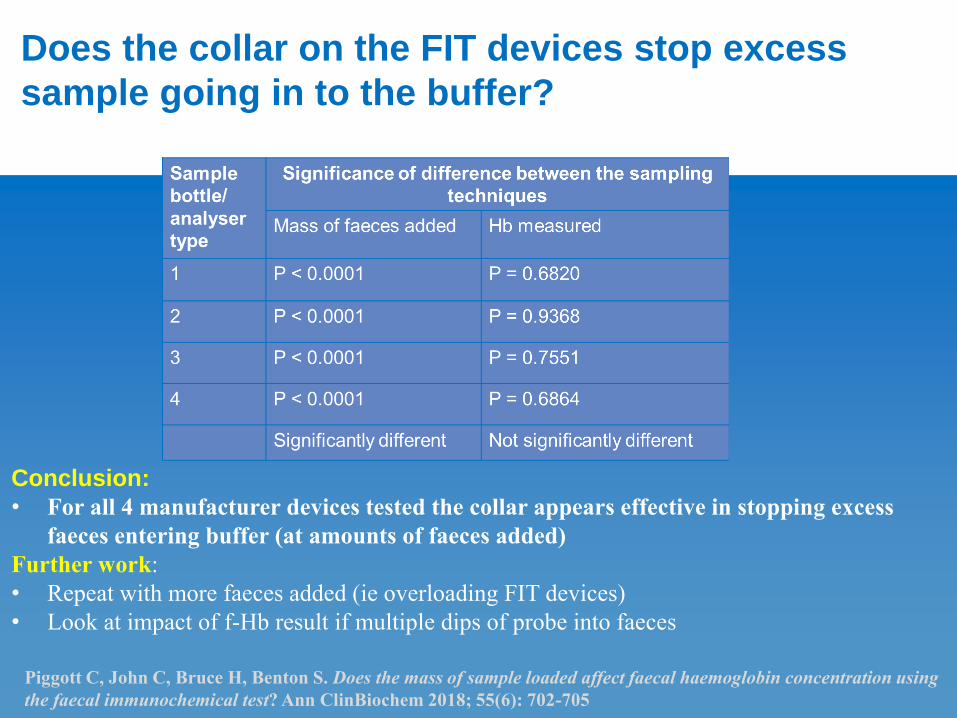
Conclusion:
• For all 4 manufacturer devices tested the collar appears effective in stopping excess
faeces entering buffer (at amounts of faeces added)
Further work:
• Repeat with more faeces added (ie overloading FIT devices)
• Look at impact of f-Hb result if multiple dips of probe into faeces
Does the collar on the FIT devices stop excess
sample going in to the buffer?
Piggott C, John C, Bruce H, Benton S. Does the mass of sample loaded affect faecal haemoglobin concentration using
the faecal immunochemical test? Ann ClinBiochem 2018; 55(6): 702-705
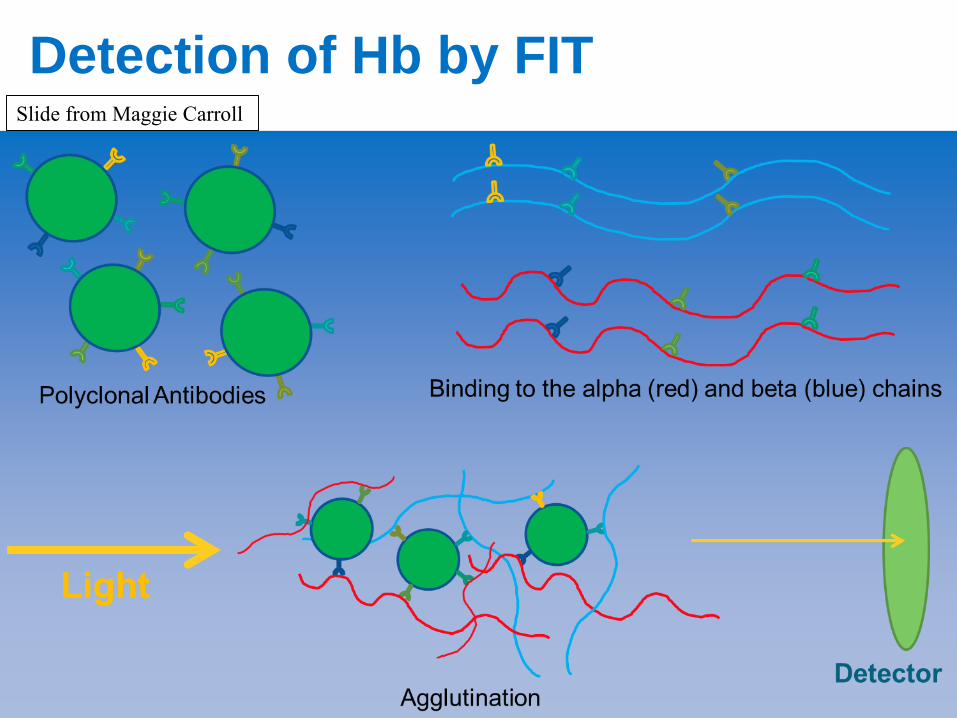
Detection of Hb by FITSlide from Maggie Carroll
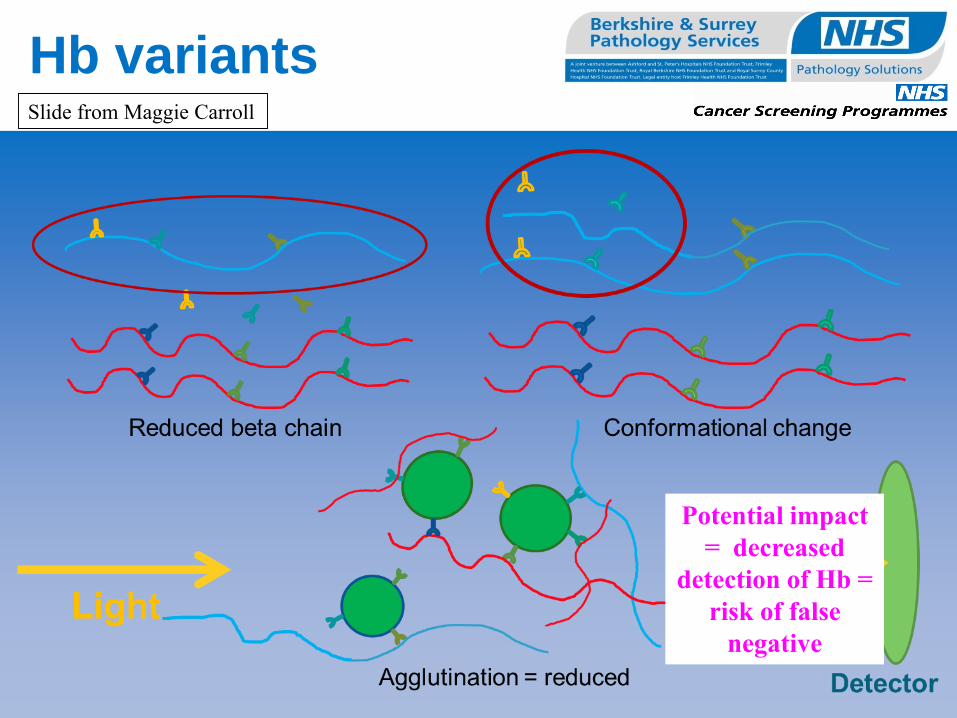
Hb variants
Potential impact
= decreased
detection of Hb =
risk of false
negative
Slide from Maggie Carroll
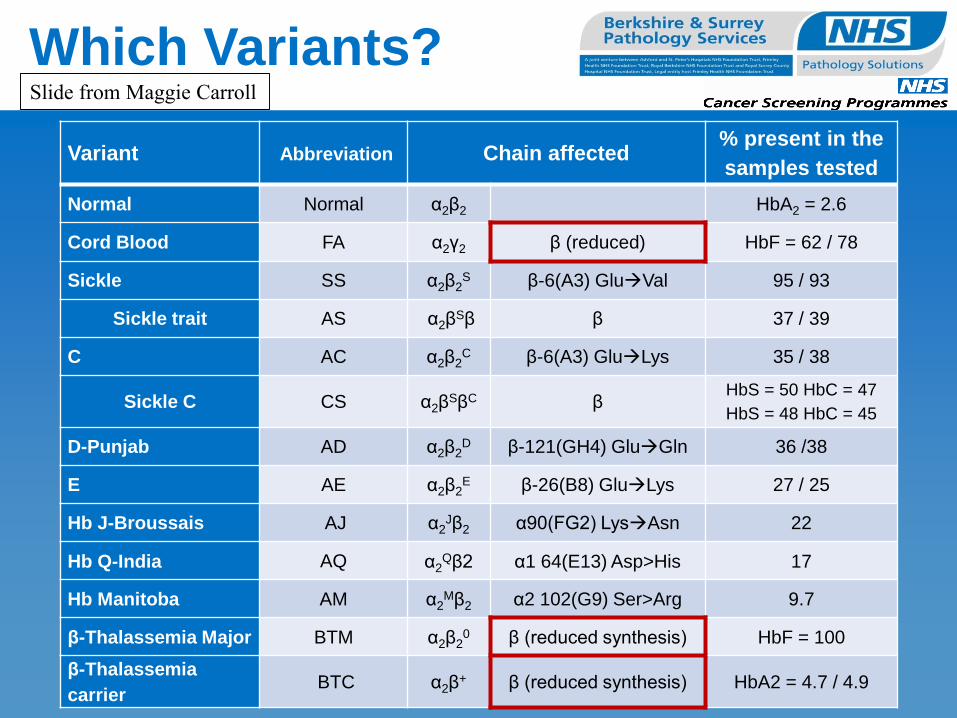
Which Variants?
Variant Abbreviation Chain affected% present in the
samples tested
Normal Normal α2β2 HbA2 = 2.6
Cord Blood FA α2γ2 β (reduced) HbF = 62 / 78
Sickle SS α2β2S β-6(A3) GluVal 95 / 93
Sickle trait AS α2βSβ β 37 / 39
C AC α2β2C β-6(A3) GluLys 35 / 38
Sickle C CS α2βSβC β
HbS = 50 HbC = 47
HbS = 48 HbC = 45
D-Punjab AD α2β2D β-121(GH4) GluGln 36 /38
E AE α2β2E β-26(B8) GluLys 27 / 25
Hb J-Broussais AJ α2Jβ2 α90(FG2) LysAsn 22
Hb Q-India AQ α2Qβ2 α1 64(E13) Asp>His 17
Hb Manitoba AM α2Mβ2 α2 102(G9) Ser>Arg 9.7
β-Thalassemia Major BTM α2β20 β (reduced synthesis) HbF = 100
β-Thalassemia
carrierBTC α2β
+ β (reduced synthesis) HbA2 = 4.7 / 4.9
Slide from Maggie Carroll
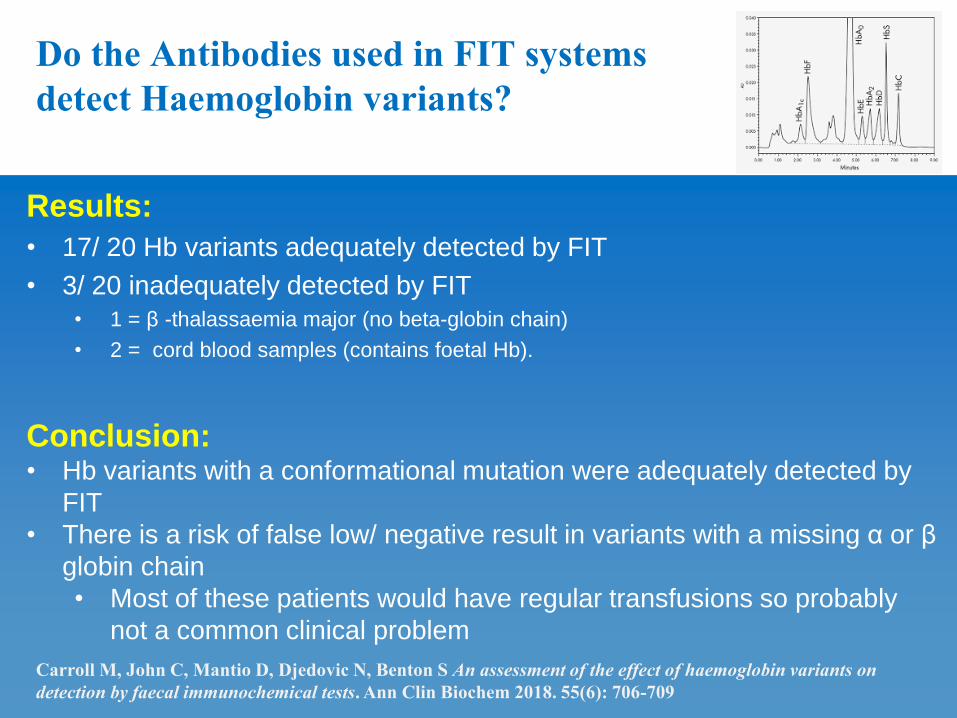
Results:
• 17/ 20 Hb variants adequately detected by FIT
• 3/ 20 inadequately detected by FIT
• 1 = β -thalassaemia major (no beta-globin chain)
• 2 = cord blood samples (contains foetal Hb).
Conclusion:• Hb variants with a conformational mutation were adequately detected by
FIT
• There is a risk of false low/ negative result in variants with a missing α or β
globin chain
• Most of these patients would have regular transfusions so probably
not a common clinical problem
Do the Antibodies used in FIT systems
detect Haemoglobin variants?
Carroll M, John C, Mantio D, Djedovic N, Benton S An assessment of the effect of haemoglobin variants on
detection by faecal immunochemical tests. Ann Clin Biochem 2018. 55(6): 706-709
Specimen collection
• Hb is unstable in faeces
• Recommendation from all FIT suppliers and international
experts is to collect samples straight in to FIT tube NOT in
to a poo pot for lab to transfer in to FIT tube
• Laboratories have had to adapt sample collection
processes
• Some give GP’s FIT tubes to hand out
• Some offer a FIT postal service
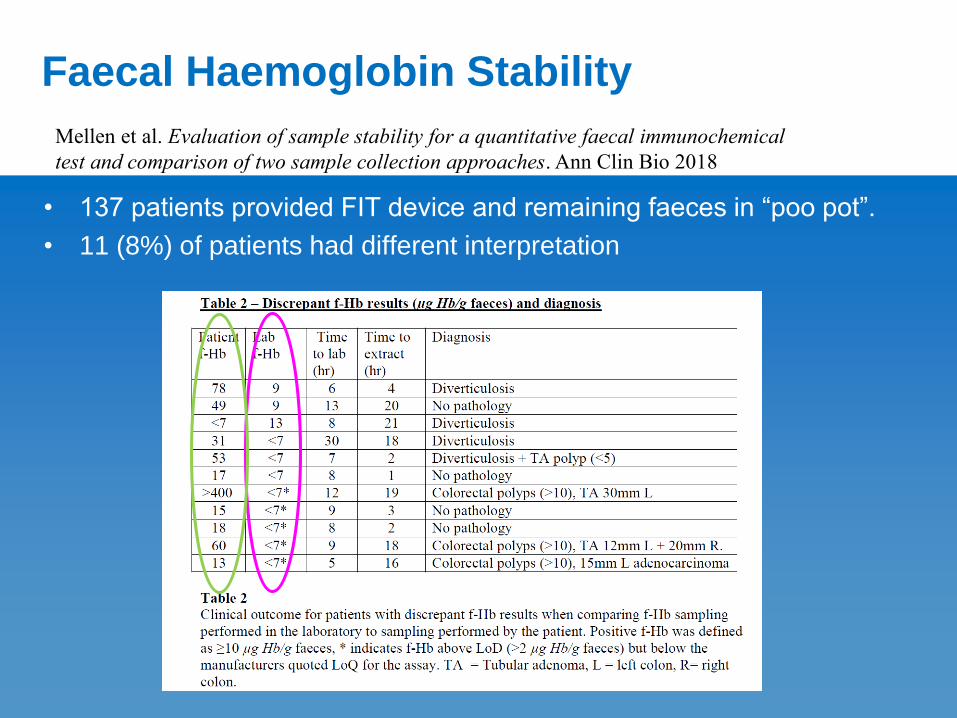
Faecal Haemoglobin Stability
• 137 patients provided FIT device and remaining faeces in “poo pot”.
• 11 (8%) of patients had different interpretation
Mellen et al. Evaluation of sample stability for a quantitative faecal immunochemical
test and comparison of two sample collection approaches. Ann Clin Bio 2018
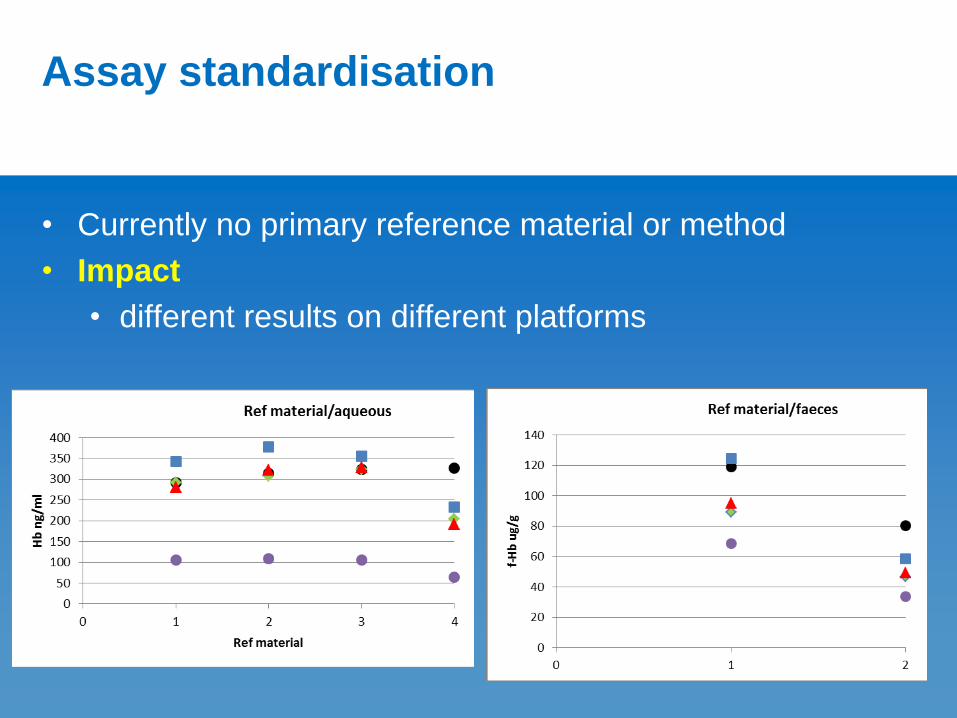
Assay standardisation
• Currently no primary reference material or method
• Impact
• different results on different platforms
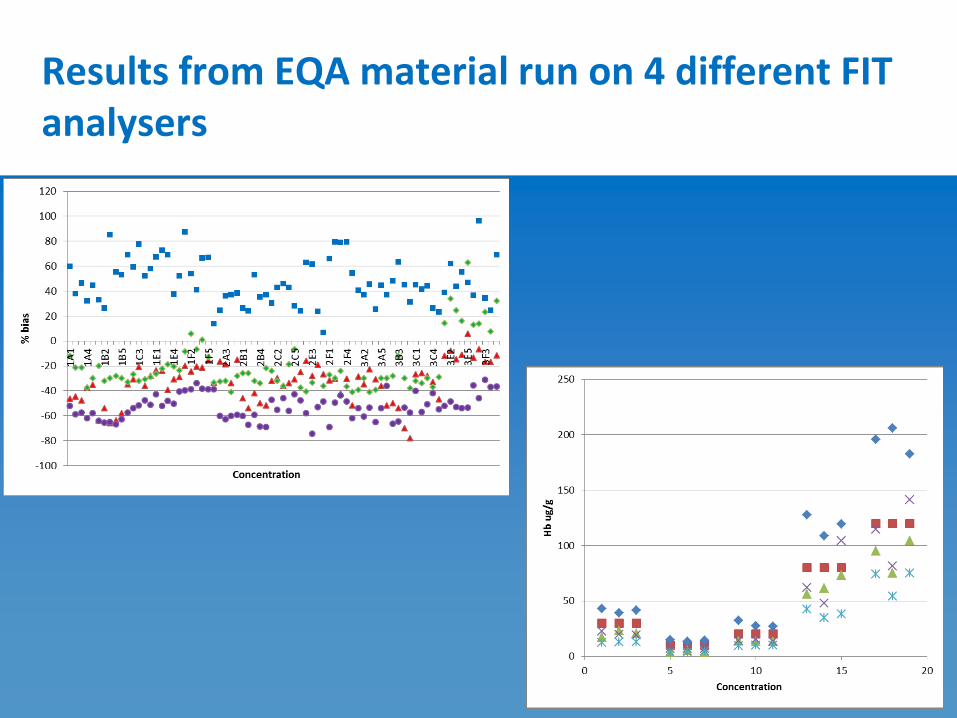
Results from EQA material run on 4 different FIT analysers
IFCC FIT Working Group(International Federation of Clinical Chemistry & laboratory
medicine)
Chair
Sally C. Benton UK
Group Members
Marieke Fasa NL
Barcey Levy USA
Han Mo Chiu Taiwan
Josep-Maria Auge Spain
Erin Symonds Australia
Petr Kocna Czech Republic
Natasha Djedovic UK
Judith Strachan UK
Ingrid Zegers Belgium
Shizuka Takehara Japan
Samantha Jones UK
Corporate members
Maurizio Gramegna Italy Sentinel
Michael Zacherl Italy Sentinel
Hideyuki Hayashi Japan Eiken
Takuo Ichiyanagi Japan Eiken
Tsuyoshi Fukuda Japan Kyowa
Yasunobu Masuda Japan Kyowa
Mr Yosuke Doi Japan Alfresa
Dr Tetsuya Kosaka Japan Alfresa
Motohito Fujimura Japan Wako
Terms of Reference
• To attempt to standardize analysis of haemoglobin in faecal samples by immunochemistry
(FIT)
• To identify all sources of pre-analytical variation and standardise if possible
• To establish external quality assurance and third party internal quality control programmes
• To determine impact of assay interference of Hb variants and other factors
First meeting held in
Athens in June 2017
2nd meeting held in
Barcelona in October
2017
3rd meeting held in Geel
in May 2018
4th meeting held in
Vienna in June 2018
Assay standardisation
progress
• Southern hub collaborating with Reference lab in Belgium
and all suppliers to identify a suitable reference material
• There will always be slight differences but we aim to align
results as much as we can between suppliers
• NICE FIT sub study
• collecting samples from patients using all 4 FIT
devices to see if same/ different diagnostic accuracy
with different FIT kits
EQA schemes update
• 2 schemes in the UK
• UKNEQAS
• WEQAS – starting in April
• Multiple schemes globally (>15)
• Varying approaches by EQA schemes
• Lyophilised samples
• Pre-loaded FIT devices
• Faecal like material sent to labs to load in to devices
• Analytical evaluation of 5 schemes being carried out by the Southern
Hub research team. 11 more schemes being contacted
• Challenge – ensuring EQA scheme assesses analytical accuracy
IQC material update
• No established 3rd party IQC material commercially
available
• Labs have to use manufacturers IQC
What should be the reporting threshold for
symptomatic FIT…..?
• Considerations;
Analytical performance characteristics
• Manufacturers recommendations
• Laboratory verification/ validation
NICE guidance
Diagnostic accuracy
• NPV and PPV/ clinical specificity and sensitivity
Impact on referral/ endoscopy capacity
Analytical performance characteristics
• Limit of detection (LOD)
• The lowest concentration at which f-Hb can be detected 95% of
the time
• The concentration where f-Hb can be reliably distinguished from a
blank sample
• Limit of quantification (LOQ)
• The lowest amount of f-Hb than can be reliably measured
according to pre-defined analytical perfomance characteristics
(CV <10%)
• Labs should not report a numerical value less than LOQ
• If f-Hb is greater than LOD but less than LOQ, lab could report
“Hb detected at very low concentrations”
Fraser CG & Benton SC. Detection capability of quantitative faecal immunochemical tests for haemoglobin (FIT)
and reporting of low faecal haemoglobin concentrations. Clin Chem Lab Med 2018.
What are labs reporting?
• Email sent on ACB mailbase for information on labs
offering symptomatic FIT
• 10 labs in England responded
• 9 labs use 10ug/g as threshold
• 1 lab uses 7ug/g
• Only 2 labs had worked out LOD and LOQ of their
instruments
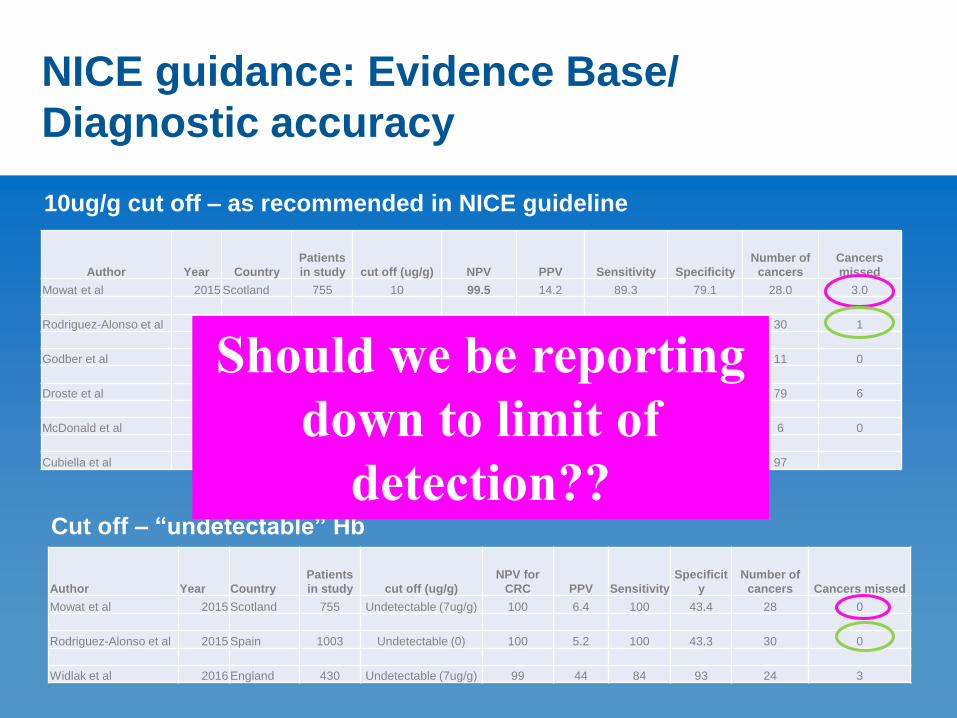
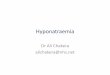
NICE guidance: Evidence Base/
Diagnostic accuracy
Author Year Country
Patients
in study cut off (ug/g) NPV PPV Sensitivity Specificity
Number of
cancers
Cancers
missed
Mowat et al 2015 Scotland 755 10 99.5 14.2 89.3 79.1 28.0 3.0
Rodriguez-Alonso et al 2015 Spain 1003 10 99.9 12.8 96.7 79.8 30 1
Godber et al 2015 Scotland 484 10 100 100 11 0
Droste et al 2011 Netherlands 2145 10 92.4 86.4 79 6
McDonald et al 2012 Scotland 280 10 100 7.6 100 93.9 6 0
Cubiella et al 2014 Spain 787 20 97.8 35.3 87.6 77.4 97
Author Year Country
Patients
in study cut off (ug/g)
NPV for
CRC PPV Sensitivity
Specificit
y
Number of
cancers Cancers missed
Mowat et al 2015 Scotland 755 Undetectable (7ug/g) 100 6.4 100 43.4 28 0
Rodriguez-Alonso et al 2015 Spain 1003 Undetectable (0) 100 5.2 100 43.3 30 0
Widlak et al 2016 England 430 Undetectable (7ug/g) 99 44 84 93 24 3
10ug/g cut off – as recommended in NICE guideline
Cut off – “undetectable” Hb
Should we be reporting
down to limit of
detection??
Impact on endoscopy
• Threshold to use is a local decision
• Local lab, endoscopy services CCG to jointly decide
• Currently no published evidence to demonstrate impact of
symptomatic FIT on endoscopy
• Lower the concentration that is reported = more people
referred = pressure on endoscopy = more cancers/ pre-
cancers likely to be detected

FIT laboratory current status
PRE-ANALYTICAL
• Hb variants likely to have very minimal impact
• Collars on FIT tubes effective – more work on-going
• Samples should be collected straight in to FIT devices
• Symptomatic FIT testing is now available across much of
England
February 2019…….
ANALYTICAL
• Identification of a primary reference material/ method underway
• There are a number of EQA schemes now available. The most fit
for purpose still to be confirmed
• Guidance is available on how to verify/ validate FIT analysers
• Still no established IQC material
FIT laboratory current statusPRE-ANALYTICAL
• Hb variants likely to have very minimal impact
• Collars on FIT tubes effective – more work on-going
• Samples should be collected straight in to FIT devices
• Symptomatic FIT testing is now available across much of England
February 2019…….
ANALYTICAL
• Identification of a primary reference material/ method underway
• There are a number of EQA schemes now available. The most fit for purpose still to be
confirmed
• Guidance is available on how to verify/ validate FIT analysers
• Still no established IQC material
POST-ANALYTICAL
• What threshold should be actually be used…….?
• LOD/ LOQ??
Berkshire & Surrey Pathology Services A joint venture between Frimley Park Hospital, Royal Surrey County
Hospital, Royal Berkshire Hospital, Wexham Park Hospital and Ashford
and St. Peter’s Hospitals NHS Foundation Trusts
Recommended