Embed Size (px)
Citation preview

Respiratory system
Upper respiratory tract - nose, pharynx andassociated structures.Lower respiratory tract - larynx, trachea, bronchiand lungs.Study Oto-Rhino-Laryng-Ology - ENTPulmonologist - lung diseases.
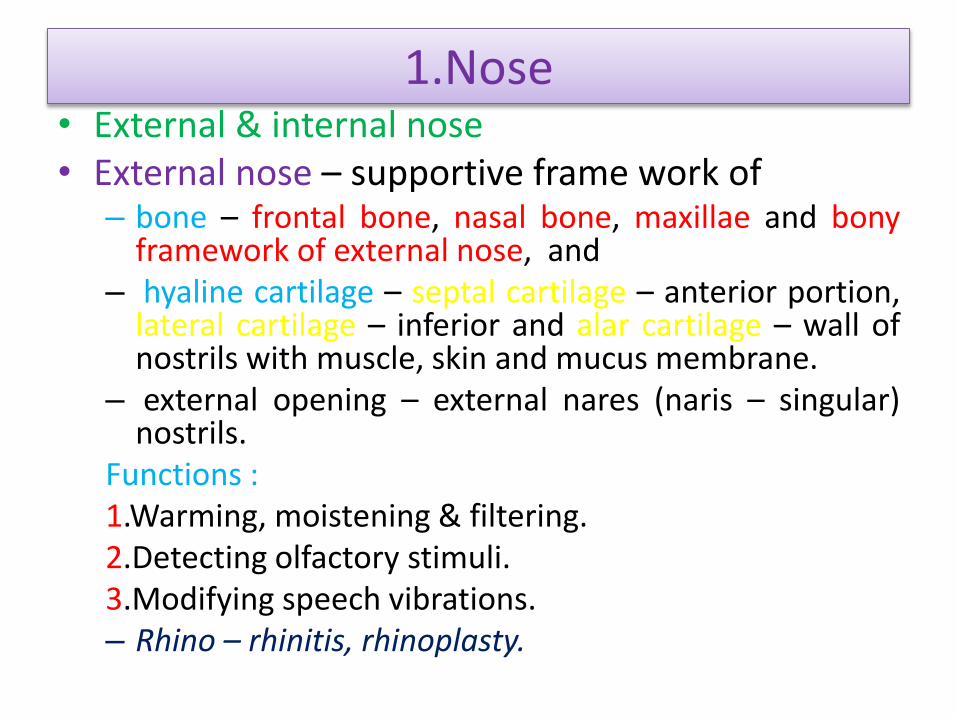
1.Nose• External & internal nose• External nose – supportive frame work of
– bone – frontal bone, nasal bone, maxillae and bonyframework of external nose, and
– hyaline cartilage – septal cartilage – anterior portion,lateral cartilage – inferior and alar cartilage – wall ofnostrils with muscle, skin and mucus membrane.
– external opening – external nares (naris – singular)nostrils.
Functions :1.Warming, moistening & filtering.2.Detecting olfactory stimuli.3.Modifying speech vibrations.– Rhino – rhinitis, rhinoplasty.


CONT….
• Internal nose – large cavity (nasal cavity) in theinterior aspect of skull lined with muscle andmucus
– Internal nares or choane – 2 openings forcommunication with pharynx (divided into series ofgroove like passages – superior, middle and inferiormeatuses)
– Paranasal sinus and nasolacrimal ducts opens intointernal nose
– lined with olfactory epithelium
– Nasal septum – divides nasal cavity into right & left.
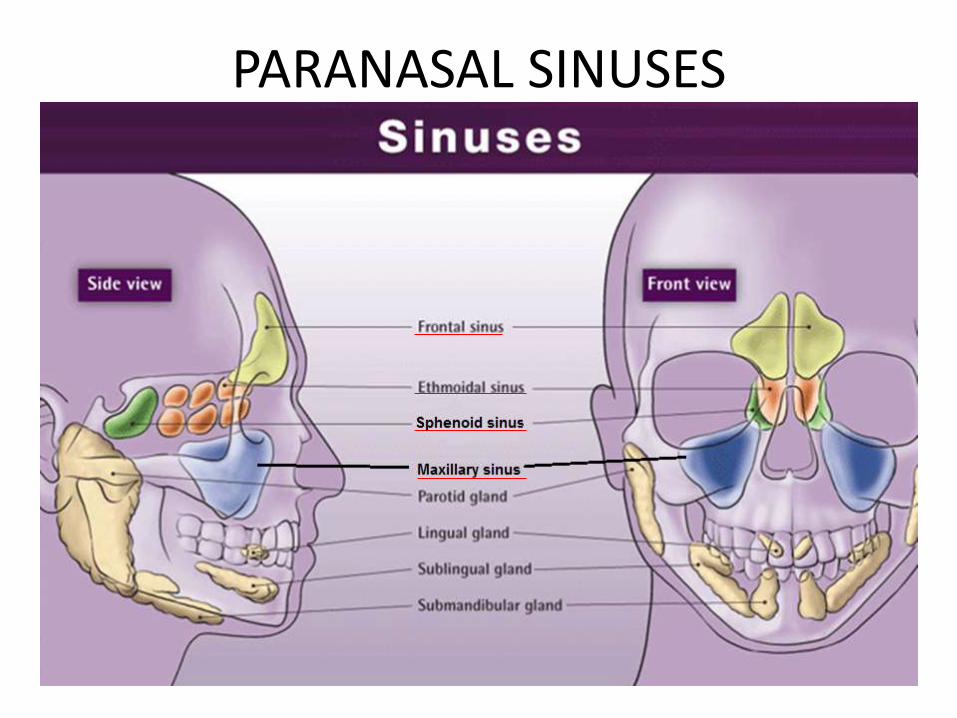
PARANASAL SINUSES
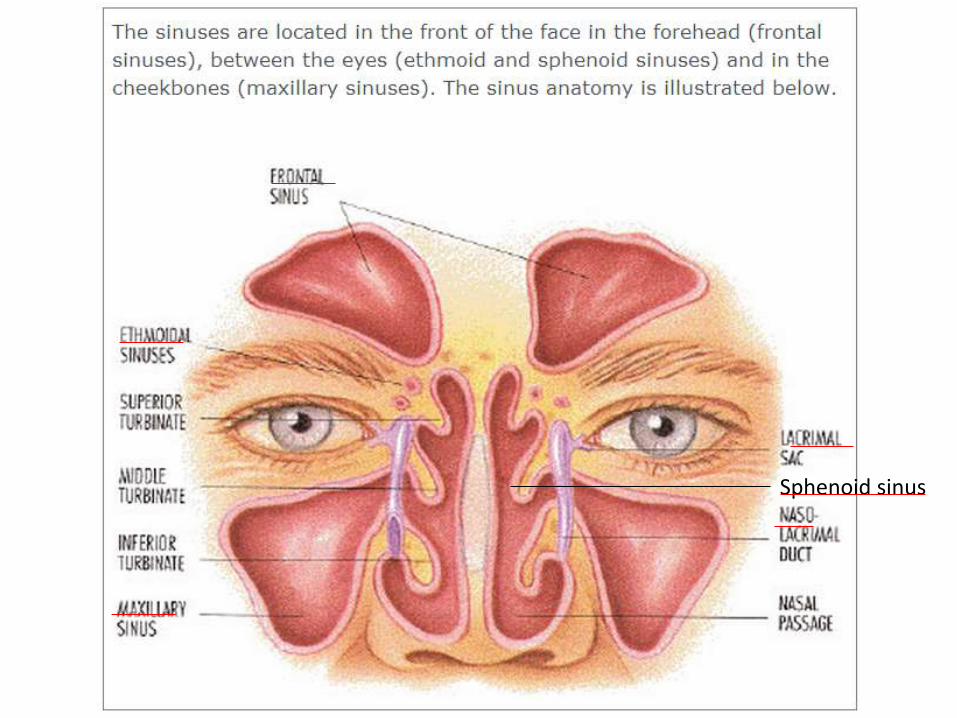
Sphenoid sinus
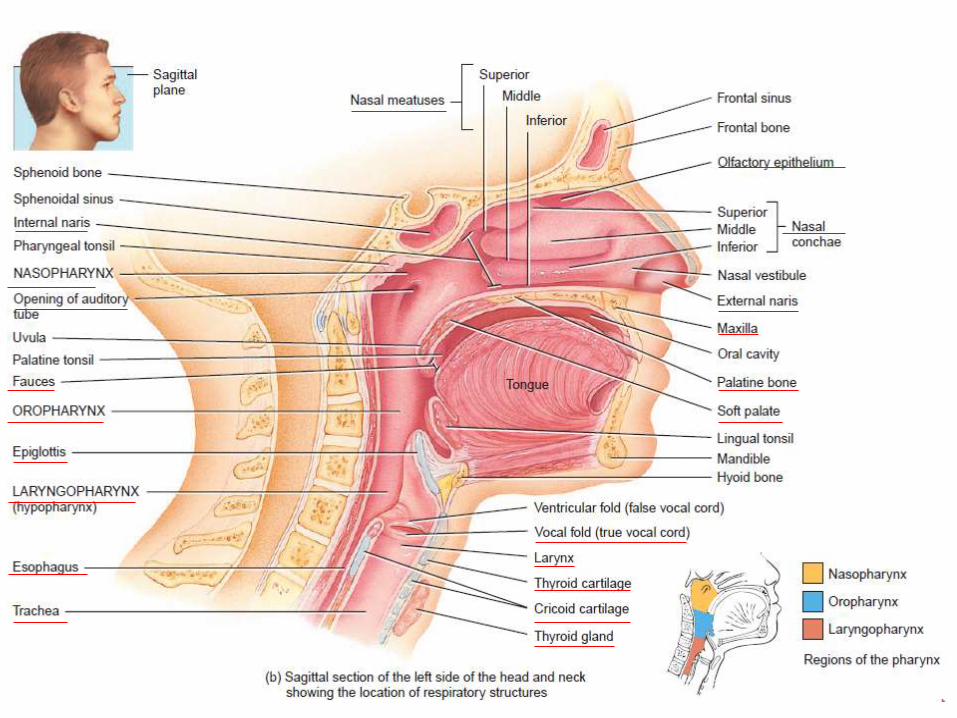
2. Pharynx (throat)• Funnel shaped tube approximately 13 cm long.• Starts at internal nares ends at larynx’s cricoid cartilage.• Anterior to cervical vertebrae and posterior to nasal/oral cavities.• Composed of skeletal muscles.• Functions
– as passage of air and food.– resonating chamber for sound.– house of tonsils in immunological reactions.
Anatomically 3 portions• 1. Nasopharynx – (helps to adjust pressure b/w pharynx and
middle ear) superior portion with openings to internal nares, earand oropharynx, contain pharyngeal tonsil.
• 2. Oropharynx – middle portion, opening called fauces to mouth-posses respiratory and digestive function, palatine and lingualtonsils found here.
• 3. Laryngopharynx – opens down to esophagus also hasrespiratory and digestive function.

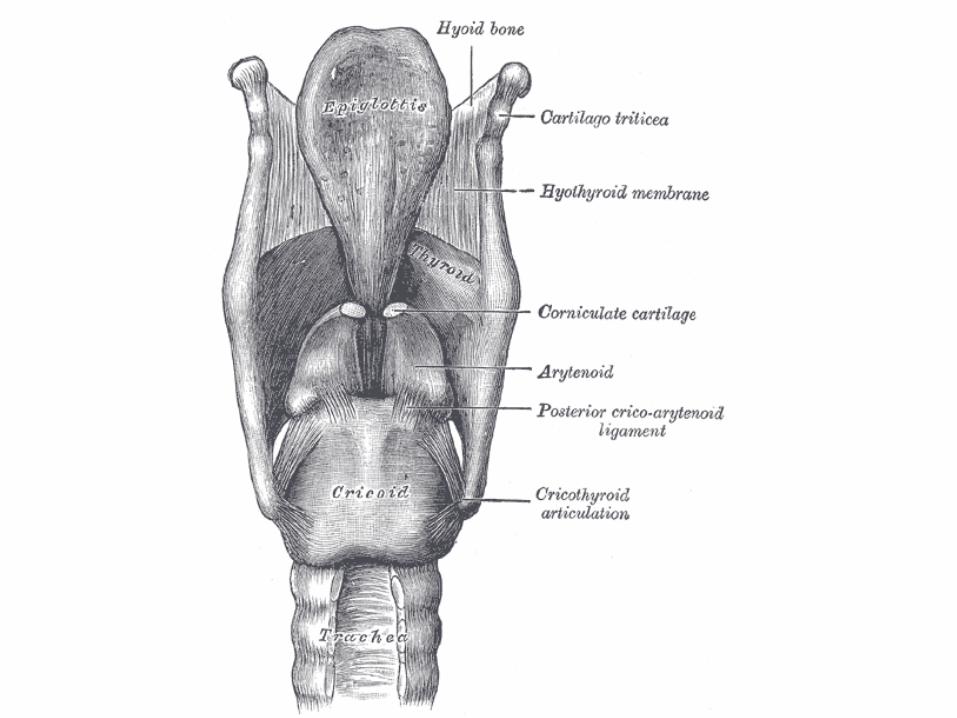
3. Larynx (voice box)• Connects pharynx and trachea, in the midline of neck anterior
to esophagusMade of nine piece of cartilage• 1. Thyroid cartilage – Adam’s apple- 2 fused cartilages in
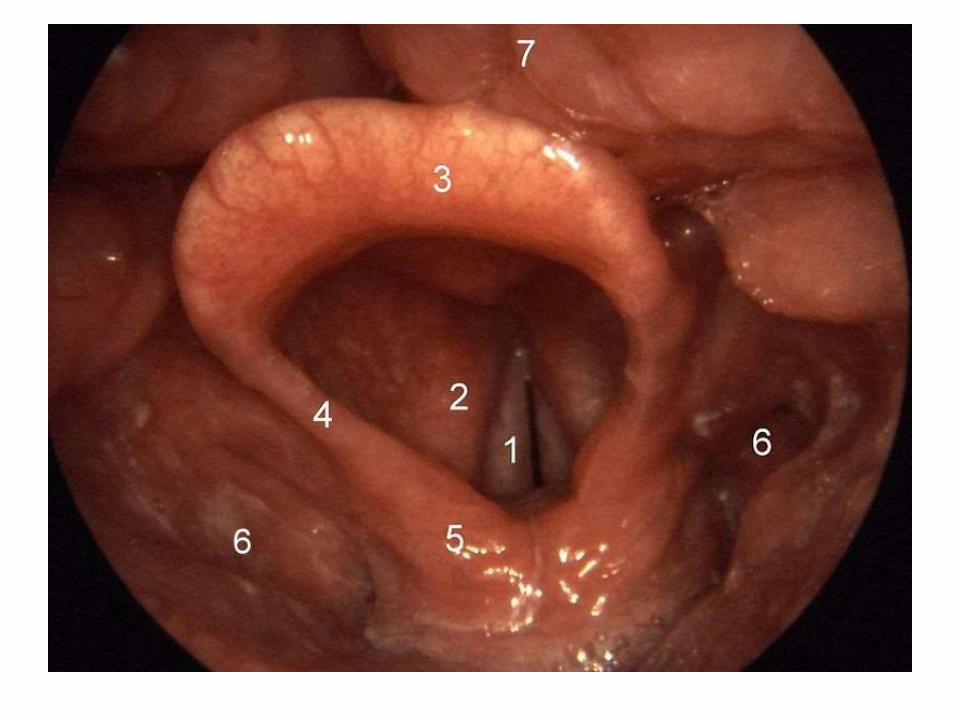
triangular shape, larger in male.• 2. Epiglottis (glottis- tongue)large leaf shaped with tapered stem and
broad superior leafy portion.– Glottis portion consists of pair of folds of mucus membrane called
vocal folds and space b/w them called Rima glottides.
• 3. Cricoid cartilage – ring of hyaline cartilage attaches withtrachea and thyroid cartilage by ligaments.
• 4. Arytenoid cartilage (paired) – triangular attached abovecricoid attached to vocal folds.
• 5. Corniculate cartilages – (paired) at the apex of arytenoidsupporting epiglottis.
• 6. Cuneiform cartilages – (paired) club shaped cartilages abovecuneiform support vocal folds.




4.Trachea (wind pipe)• Tubular passage for air, approximately 12 cm long &
2.5 cm diameter.
• Anterior to esophagus.
• Starts from larynx to 5th thoracic vertebra and dividesinto two primary bronchi.
• 4 layered –
– mucosa & sub mucosa - which provide protection fromdust and produce mucus.
– hyaline cartilage – 16-20 horizontal, incomplete C shapedrings stalked upon each other, open ends has trachealismuscle helps to adjust with esophagus expansion.
– adventitia connect trachea to other surrounding tissues.
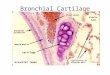
5.Bronchi (wind pipe)
• At 5th thoracic vertebra trachea divides into 2.• Right and left primary bronchi – right into right lung
and left into left lung.• Primary bronchi also has incomplete cartilages.• Internal ridge where right and left bronchi divides is
called carina – where mucus membrane is mostsensitive.
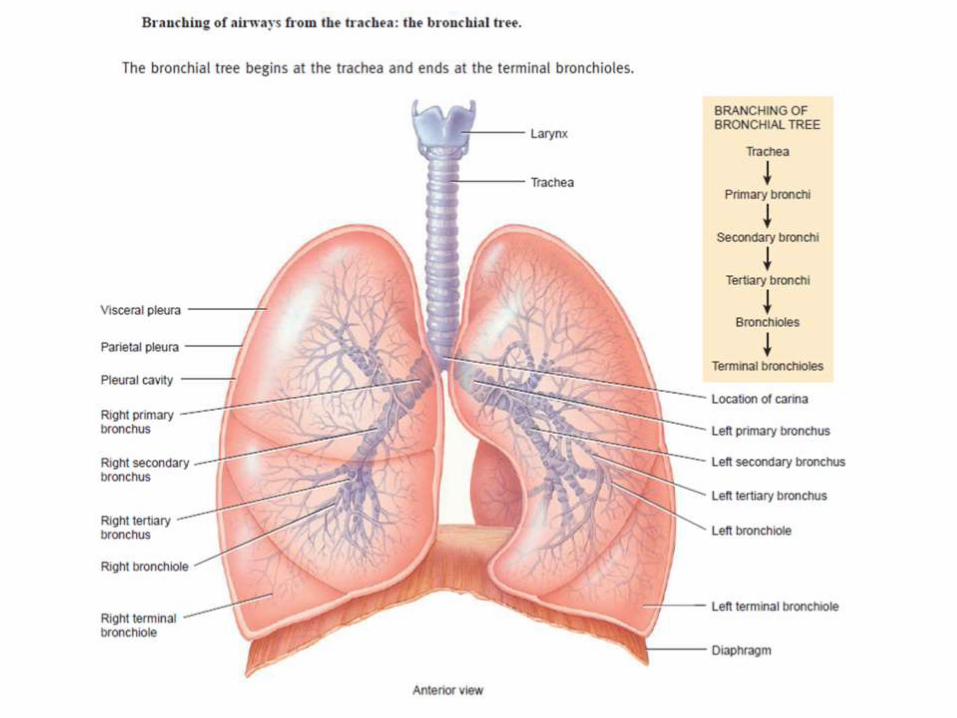
• Primary bronchi divides to secondary (lobar) and thento tertiary (segmental) to bronchioles and then toterminal bronchioles.
• This extensive branching called bronchial tree.

• Right pulmonary bronchus – more vertical,longer, wider, aspired air object more into rightlung.
• Right bronchi – 3 lobes.
• Bronchi to bronchioles – pseudostratifiedcuboidal. columnar becomes – non ciliatedsimple cuboidal.
• No Goblet cells.
• Incomplete rings to cartilages and cartilagedecreases replaced by more and more smoothmuscle - muscle spasm can occur.
Lungs – light weight• Paired, cone shaped, in the thoracic cavity.
• Heart lies in between.
• Lobes and fissures.
• Oblique fissure – on both lungs anteriorly andposteriorly - to superior and inferior lobes.
• Horizontal fissure – right lung - middle and inferiorlobes.
• Pleural membrane – 2 layers of serous membrane -enclose and protect lung.– Parietal pleura – superficial to thoracic wall.
– Visceral pleura – cover the lungs.
– Pleural cavity – b/w pleura – lubricates, reduce frictionand helps in breathing.
• Pneumothorax – if air inside, haemothorax if blood,atelectasis – collapse of lung.
• A hemothorax (or haemothorax/Haemorrhagicpleural effusion) is a condition that results fromblood accumulating in the pleural cavity. Atelectasis(from Greek: "incomplete" + "extension") is definedas the collapse or closure of the lung resulting inreduced or absent gas exchange.


• Position
– Above diaphragm, just inferior to clavicles.
– Base broad and concave.
– Apex – narrow superior.
– Coastal surface – surface against ribs.
– Hilum - where bronchi, pulmonary vessels, lymph, bloodvessels enters in to the lungs.
– Root - above structures, pleura, connective tissue heldtogether.
– Cardiac notch – concave cavity of left lung where the heart issituated.
• Right lung - shorter broader, thicker, due to liveraccommodation.
• Left lung - 10 % shorter than right.


• 10 bronchi – divides into 20 bronchi – right lung 3 lobesand left lung 2 lobes.
• 20 to 30 bronchi – one 20 to 10 – 30 30 bronchi.
• Bronchopulmonary segment - each 30 and segment oflung tissue.
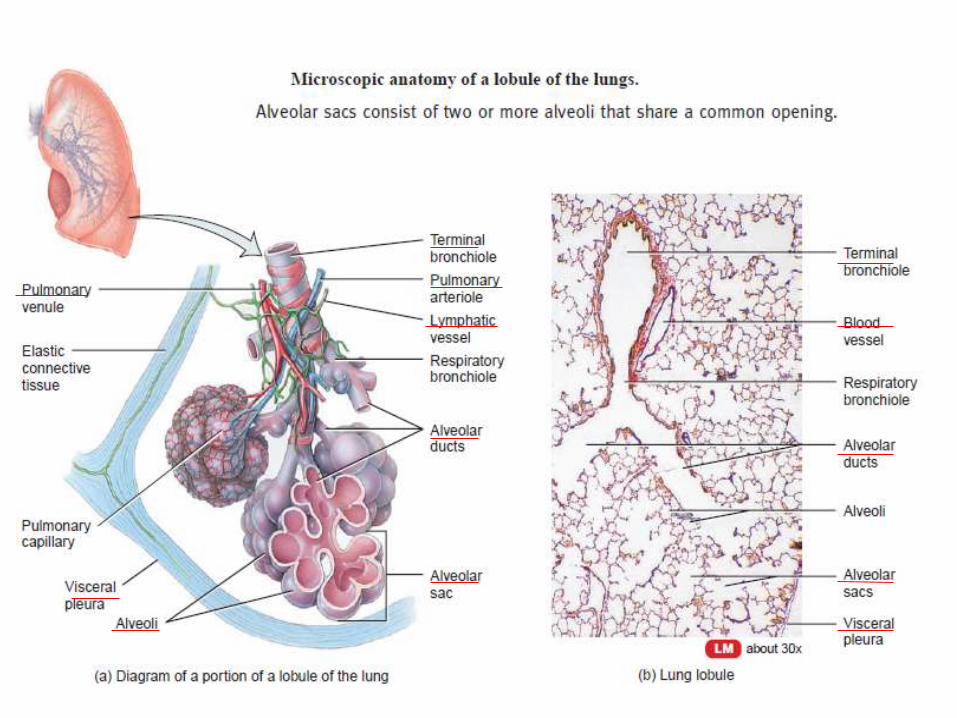
• Lobules – small compartment of Bronchopulmonarysegment with lymphatic vessels, arterioles, venules &terminal bronchiole.
• Terminal bronchiole – respiratory bronchiole divides into2-11 alveolar ducts.

ALVEOLI
• Around Alveolar ducts numerous alveoli and alveolar sacs.
• Alveolus – cup shaped pouches.
• Alveolar sac – 2 or more alveoli with common opening.
• Alveolar cells – type 1 – simple squamous for gasexchange, type 2 or septal cells - few, rounded secretealveolar fluid contain surfactant, a mixture of complexphospholipids and lipoproteins.
• Alveolar macrophages – remove dust particles.
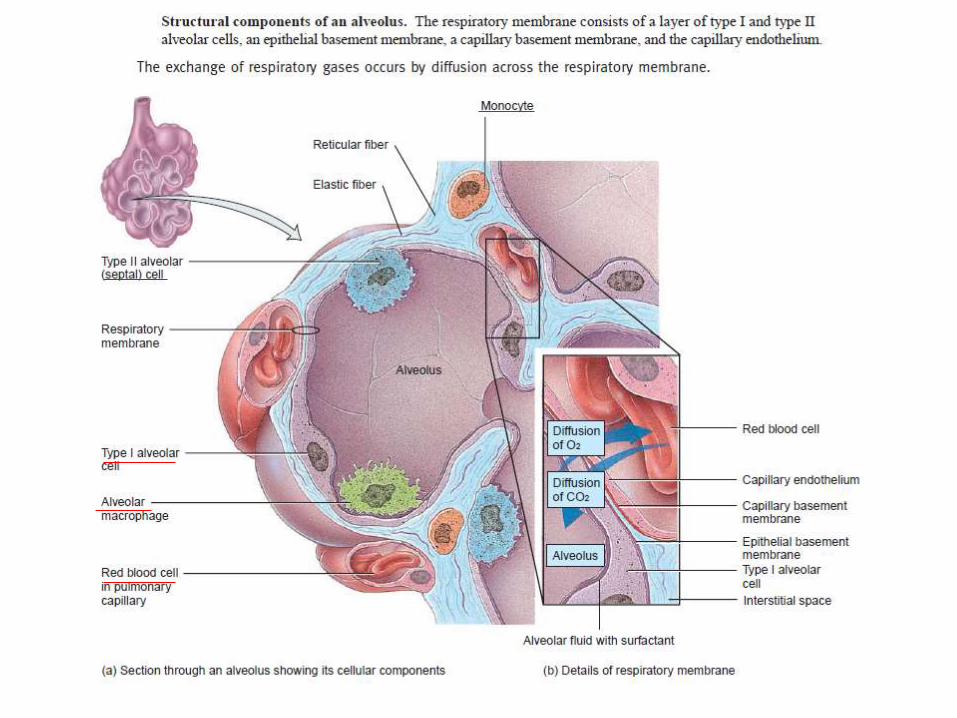

Respiratory membrane Membrane wall b/w alveolar and capillary wall, 0.5 micron as 4
layers.
• One layer of type 1 and type 2 cells, macrophages.
• Epithelial basement membrane of alveolar wall.
• Capillary basement fused to epithelial membrane.
• Capillary endothelium allows rapid diffusion of gases.
• 300 million alveoli – 70 m2 surface area for gas exchange.
Blood supply
• Receive via• Pulmonary Arteries – supply deoxygenated blood
from heart directly.• Bronchial Arteries – from aorta - oxygenated
blood.• Pulmonary Vein – oxygenated blood to heart.• Ventilation perfusion coupling – constriction of
arterioles in response to hypoxia, diverts bloodflow from poorly ventilated area to highlyventilated areas.

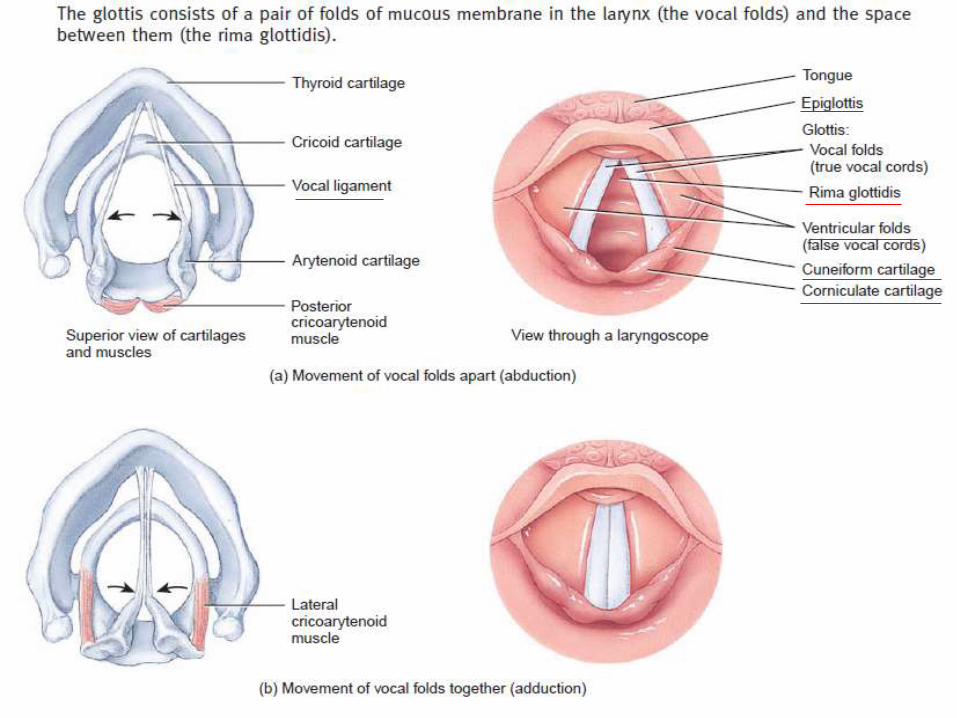
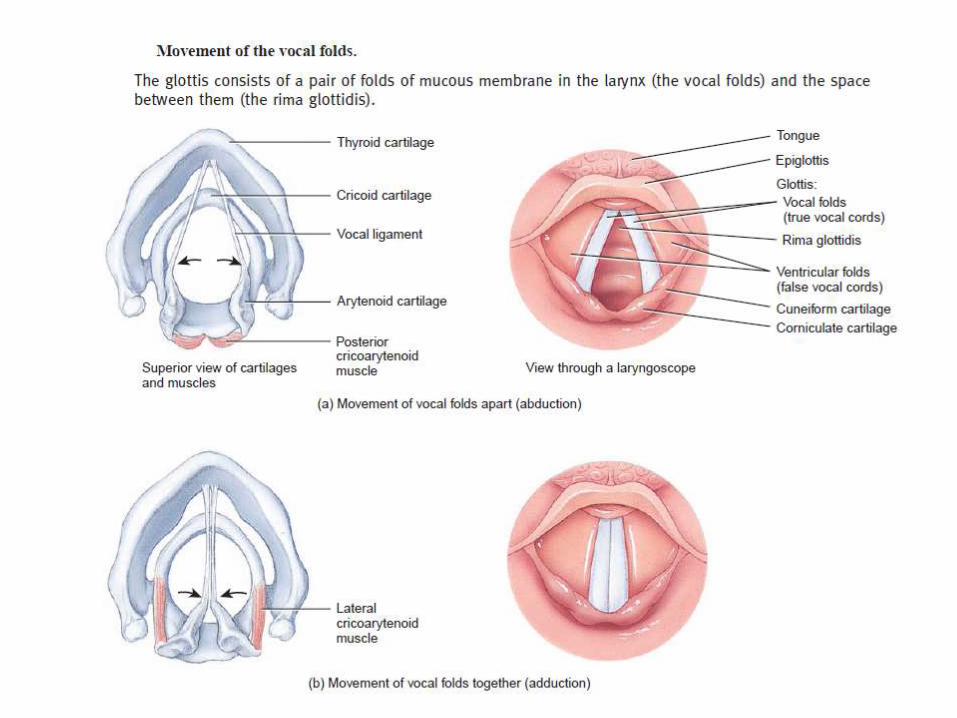
3.(a)Voice production Structures• glottis portion of larynx consists of pair of folds of mucus membrane• superior fold called ventricular or false vocal folds and• inferior pair called true vocal cords and• space b/w ventricular folds called rima glottidis• laryngeal muscles attached to cartilage and vocal foldsProcess• 1. When laryngeal muscles contracts they pull posterior cricoarytenoid
muscles and moves vocal folds apart (abduction) and rima glottidisbecomes open.
• 2. When lateral cricoarytenoid muscles contracts moves the vocal foldstogether and rima glottidis becomes narrow /closed (adduction).
• Other intrinsic muscles also can elongate or shorten vocal folds.• 3. Increased tension on vocal folds, cause folds vibrate rapidly and high
pitch and vice versa.• Androgens cause male vocal folds more thick, so vibrate slowly and has
low pitch in males.• Pharynx, mouth, nasal cavity, paranasal sinuses acts as resonating
chambers gives voice individual quality.

Pulmonary ventilation
• Respiration – process of gas exchange in our body.• 3 steps.• Pulmonary ventilation – breathing = inhalation (inflow)
+ exhalation (outflow) – b/w air of atmosphere andalveoli of lungs.
• External pulmonary respiration – exchange of gas b/walveoli of lungs and blood in pulmonary capillariesacross respiratory membrane – blood gains O2 andblood loses CO2.
• Internal tissue respiration – exchange of gas b/w bloodin capillaries and tissue cells – blood loses O2 and gainsCO2.

Inhalation
• An active process• Breathing in is called inhalation/inspiration• As per boyle’s law – when volume increases pressure
decreases• Before respiration Pressure inside the lungs = air
pressure of atmosphere = 760 mm of hg = 1atmosphere
• Then pressure inside the lung decreases by increasedlung volume cause air to flow to lungs
• For inhalations lungs must expand, this needscontraction of muscles of inspiration
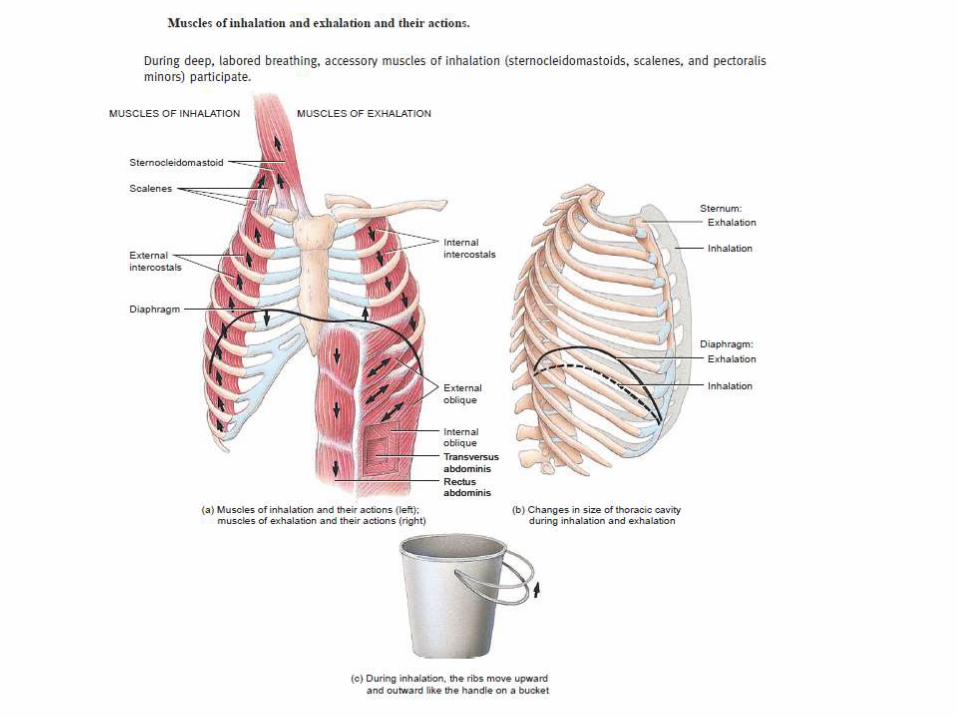
Muscles of inspiration1.Diaphragm – dome shaped skeletal muscle at the floor
of thoracic cavity innervated by phrenic nerve.– Contraction causes –flattening and lowering its dome– Increases vertical diameter of thoracic cavity– Descends –normal breath -1 cm, strenuous breath -10 cm,– Pressure difference – 1-3 mm of hg to 100 mm of hg.– Normal 500 ml, strenuous 2-3 L.– Responsible for 75 % of air entering.
2.External intercostal muscles – contraction causeelevation of ribs, increased anterio-posterior & lateraldiameter of chest cavity - responsible for 25 % of airthat enter
• Accessory muscles – during deep forceful inhalation– Sternocleidomastoid muscle – elevate sternum– Scalene muscle - elevate first 2 ribs
• Intra pleural pressure - during quiet inhalations –always sub atmospheric -756 mm of hg.
• Contraction of diaphragm and external intercoastal muscles – decreases to 754 mm of hg,expansion parietal and visceral – pulled alongthoracic cavity.
• Alveolar pressure - pressure 760 drops to 758.
• Pressure difference established air enters tolungs.

Exhalation or expiration• Breathing out is called exhalation.• Also due to pressure gradient in opposite direction,
pressure inside the lung more.• Normal exhalation - passive process, no muscle
contraction involved, results from elastic recoil ofchest wall and lungs.
• Recoil of elastic fibers stretched during inhalation,inward pull of surface tension due to fill of alveolarfluid.
• The relaxation of muscles of inhalation, diaphragm,external intercostal muscles decreases lung volume.
• Alveolar pressure increases 762 mm of hg• Air flows out

• During forceful exhalation - playing windinstruments, exercise – muscles of exhalation –rectus abdominus and other abdominal muscles- contract – moves inferior rib down wards,compress abdominal viscera forcing diaphragmsuperiorly
• Internal Intercostal muscles - contraction pullsrib anteriorly
Other factors affect pulmonary ventilation
• 1. Surface tension of alveolar fluid – cause alveolito assume smallest possible diameter.Also account for 2/3rd of elastic recoil of lungswhich decreases size of alveoli during exhalation.
• 2. Compliance of lungs – is the effort required tostretch the lung and chest wall, high compliance –expand rapidly, normal – high compliance, in TB,Pulmonary edema – intercostal muscle paralysisdecreased compliance.
• 3. Air way resistance - resistance to flow of airespecially by bronchioles, signals fromsympathetic system, relaxation of air wall, COPD,asthma, chronic bronchitis contracts air ways.

• Eupnoea – normal pattern of breathing
• Coastal breathing – shallow chest breathing
• Diaphragmatic breathing – deep abdominal breathing
• Modified respiratory movements - coughing, sneezing, sighing, yawning, sobbing, crying, laughing, hiccoughing, valsalua maneuer.

Lung volumes – 12 breath per minute.
• Tidal volume - volume of one breath = 500 ml• Minute ventilation – total volume in each minute = 12 x 500
= 6 L• Anatomic dead space - the conducting air ways with air
that does not undergoes respiratory exchange = 30% of air= 150 ml
• Alveolar ventilation rate - volume of air that reachesrespiratory zone per minute - 350x12 =4200 ml
• Inspiratory reserve volume - additional air that can beinhaled by taking a very deep breath - 3100 for male, 1900for female
• Expiratory reserve volume - inhale normally, exhale forciblyas far as possible – additional air that can be pushed out,1200 ml male, 700 ml female

Lung volumes
• Forced expiratory volume FEV 1.0 1 second - volumeof air that can be exhaled from the lungs in one secondwith maximal effort following a maximal inhalation
• Residual volume - even after expiratory reservevolume, considerable air remaining in lungs, cannot bemeasured by spirometer - 1200 male, 1100 female
• Minimal volume - if thoracic cavity opened,intrapleural pressure rises force out some residualvolume, the air remaining is called minimal volume
• Fetal lung – no air, so still born baby lung not float inwater

Lung capacities • Are combinations of various or specific lung volumes
• Inspiratory capacity – tidal volume + inspiratoryreserve volume = 500 + 3100/1900
• Functional residual capacity - residual volume +expiratory reserve volume = 1200+1200 / 1100+700
• Vital capacity - inspiratory reserve volume + tidalvolume + expiratory reserve volume =3100+500+1200/1900+500+700= 4800/3100
• Total lung capacity = vital capacity + residual volume =6000/4200

Spirometer – apparatus used to measure volume of air exchanged
Transport of gases Oxygen transport
• O2 not easily dissolve in water - only 1.5% inblood plasma, 98.5% bound with Hb in RBC
– 100 ml blood - 20 ml gaseous O2 - 19.7 ml-as Hb,0.3 ml in blood plasma
• Hb = haem + globulin
– Haem - 4 iron atoms – 1 O2 each
• So only 1.5 % diffused out of tissue capillariesinto tissue cells

Determinants / factors of O2 transport
1. partial pressure ofO2:
• more the partial pressure morebinding of O2 to Haem
• Hb+O2 – HbO2 (oxyheamoglobin)• Fully saturated – completely
bound• In pulmonary capillaries – PO2
high 100-105 mmHg - O2 bindsto Hb.
• In tissue capillaries – PO2 low –dissolved O2 is unloaded , diffuseto tissue cells – only 95 % isunloaded from Hb.
• If PO2– b/w – 60-100 – Hb is
90 % saturated with O2.
– 40-Hb is 75%.– 20-Hb saturation is
35%.
• So people still performat high altitudes.
• In active tissues PO2reaches 40 below. SoO2 unloaded fromHbO2, so more O2available for tissuerespiration.

Determinants / factors of O2 transport
2. Acidity & pH:• As the acidity increases -
the pH decreases.
• O2 dissociates more fromHb because affinity of Hbdecreases.
• Lactic acid, carbonic acidetc. increase duringexercise hence O2
dissociation.
• Bohr effect - when pHincreases Hb dissociationcurve shifts to right i.e.at given PO2 Hb is lesssaturated with O2.
• Due to high binding of Hbwith H+, when H+ binds toHb, O2 diffuses out fromHb.

Determinants /factors of O2 transport
3. Partial pressure ofCO2:
• Effect similar to H+
• PCO2 increases, Hb releases O2more readily, because CO2also binds to Hb
• CO2 also increases acidity• CO2 enters to blood –
temporarily converted tocarbonic acid, by enzymecarbonic anhydrase, soincreased H+, decreases O2affinity
• CO2 + H2O H2CO3 H+
+HCO3
4. Temperature:• Increased temperature
increased O2 releasefrom Hb, heatbyproduct of allmetabolic reactions
• Metabolically activecells release acid + heat– increased O2 release
• Hypothermia - less O2released, so more O2binds to Hb
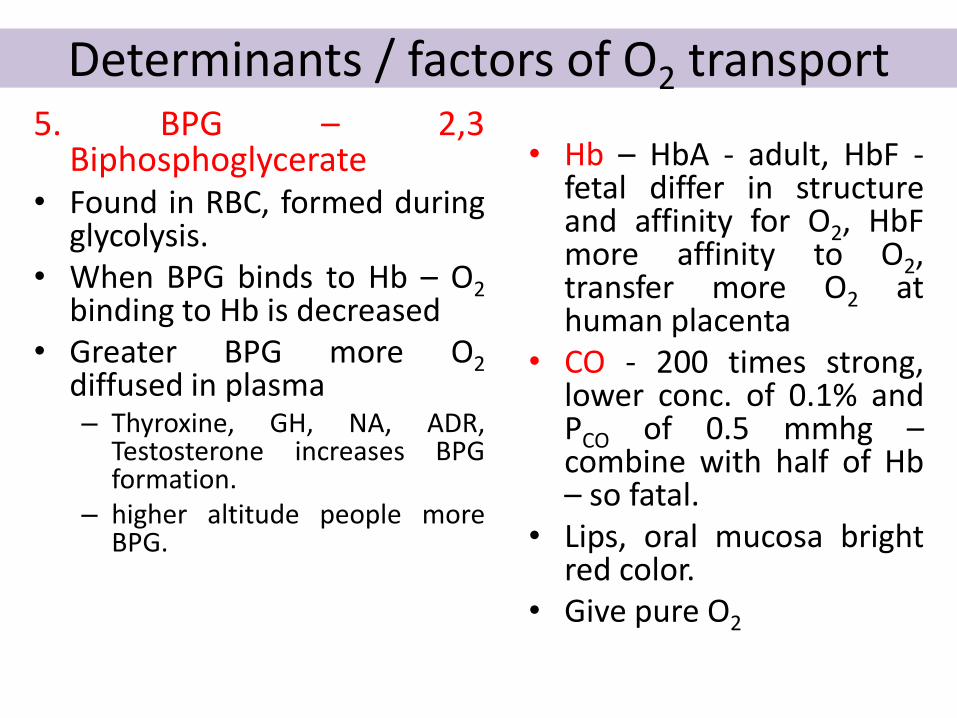
Determinants / factors of O2 transport 5. BPG – 2,3
Biphosphoglycerate• Found in RBC, formed during
glycolysis.• When BPG binds to Hb – O2
binding to Hb is decreased• Greater BPG more O2
diffused in plasma– Thyroxine, GH, NA, ADR,
Testosterone increases BPGformation.
– higher altitude people moreBPG.
• Hb – HbA - adult, HbF -fetal differ in structureand affinity for O2, HbFmore affinity to O2,transfer more O2 athuman placenta
• CO - 200 times strong,lower conc. of 0.1% andPCO of 0.5 mmhg –combine with half of Hb– so fatal.
• Lips, oral mucosa brightred color.
• Give pure O2
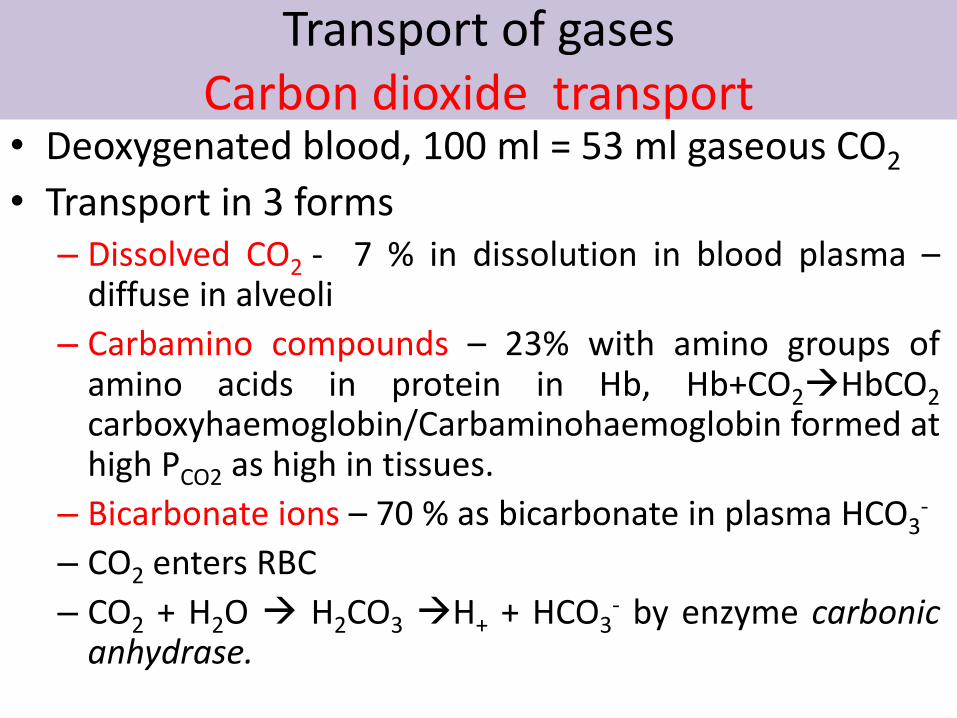
Transport of gases Carbon dioxide transport
• Deoxygenated blood, 100 ml = 53 ml gaseous CO2
• Transport in 3 forms– Dissolved CO2 - 7 % in dissolution in blood plasma –
diffuse in alveoli
– Carbamino compounds – 23% with amino groups ofamino acids in protein in Hb, Hb+CO2HbCO2carboxyhaemoglobin/Carbaminohaemoglobin formed athigh PCO2 as high in tissues.
– Bicarbonate ions – 70 % as bicarbonate in plasma HCO3-
– CO2 enters RBC
– CO2 + H2O H2CO3 H+ + HCO3- by enzyme carbonic
anhydrase.


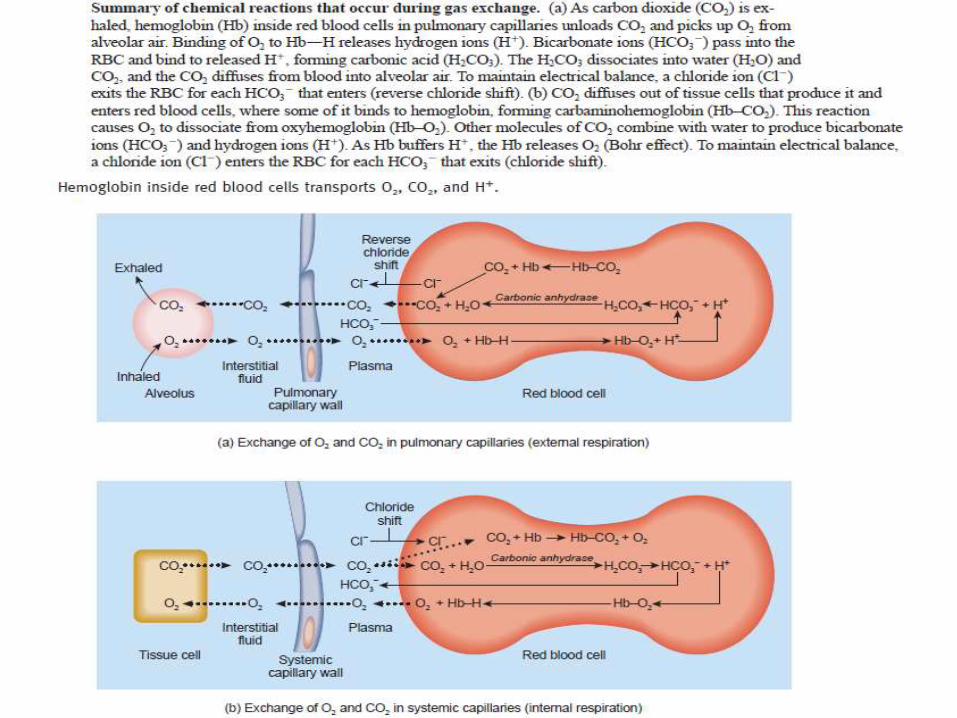
• HCO3- diffuses out of RBC
down the concentrationgradient and in exchange –Cl- enters the cell.
• This exchange maintainsthe electrical balance b/wplasma & RBC – calledchloride shift.
• HCO3- in blood plasma
reaches lungs, reactionreverses CO2 out.
• Haldane effect – It is therelationship b/w CO2transport and CO2 carryingcapacity.
• Lower theoxyhaemoglobin higherthe CO2 carrying capacity.
• Deoxy-Hb binds to CO2
transport more CO2.
• Deoxy-Hb buffers H+ morethan O2, so remove H+ ionsfrom solution andpromote CO2H2CO3

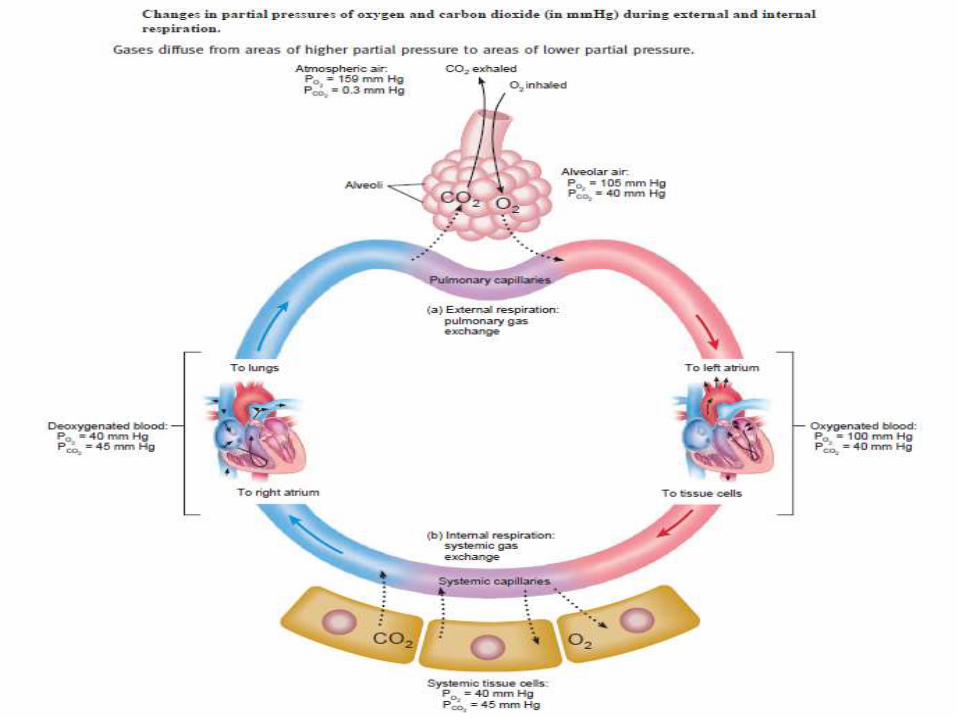
EXTERNAL AND INTERNAL RESPIRATION
• EXTERNAL RESPIRATION
• Process of respirationhappens in pulmonarycapillaries where oxygenfrom inhaled air crossesthe pulmonary capillariesacross the respiratorymembrane into the RBCand CO2 diffuses out intothe expired gas
• INTERNAL RESPIRATION
• Process of respirationhappens in systemiccapillaries where oxygenfrom RBC diffuses intotissue cell and carbondioxide from tissue cellescapes into RBC

Control of respiration• Each minute 200 ml O2 is used, exercise 15 - 20 fold,
trained athletes 30 times• Controlled by
– Respiratory center, medullary rhythmicity area at medulla.– Pneumotaxic area – upper pons.– Apneustic area – lower pons.
• Regulated by– Cortex of brain– Chemoreceptors - central in medulla, aortic and carotid
bodies– Proprioceptors– Inflation reflux (HERING BREUR reflex) stretch and
compression sensory receptors.

Control of respiration
• Respiratory Centre - The nerve impulse from widelydispersed clusters of neurons alter the size of thorax
1.Medullary rhythmicity area – medulla oblongata –control basic rhythm of respiration– 2 areas – inspiratory area & expiratory area.
Quiet breathing –• 2 seconds – inspiration area nerve impulse for 2
seconds – external intercostal, diaphragm contracts,inactive after 2 seconds.
• 3 seconds – expiration area inactive – no impulse –relaxation of muscles.
Forceful breathing – from inspiratory area, and activeexpiratory area, internal intercostal and abdominalmuscle constrict
Control of respiration
• 2. pneumotaxic area – in upper pons –coordinate transition b/w inhalation andexhalation, transmit inhibitory impulse toinspiratory area i.e. turn off inspiratory area,duration of inhalation shorter, breathing ratebecomes rapid
• 3. apnuestic area – in lower pons – sendsstimulatory impulse to inspiratory area - activateand prolong inhalation, long deep inhalation
• active pneumotaxic area overrides apneusticarea

Regulation of respirationbasic rhythm of inspiratory area modified by various influences
• Influence of cortex –
• Voluntary – inhibit the reflux to breath, shorttime, protection from water, irritating gasesentering lungs, limited because increased CO2
& H+, activate inspiratory area.
• Also from hypothalamus & limbic system,emotional laughing & crying

Chemoreceptor regulations • Central chemoreceptors in medulla in CNS – changes
H+, PCO2 in CSF.• Peripheral nervous system
– aortic bodies – cluster of chemoreceptors in wall of arch ofaorta part of vagus nerve
– Carotid bodies – oval nodules in wall of left & right commoncarotid arteries, part of glossopharyngeal nerve.
• Sensitive to changes in PO2, H+, PCO2 in blood• Normal PCO2 - 40 mm in arteries, short change – PCO2 -
Hypercapnia, hypercarbia• Respond to deficiency of O2. If PCO2 falls below 50 mm
of hg and increase in PCO2 & H+, participate in -vefeedback system cause hyperventilation till PCO2 & PO2becomes normal.
• Hypoxia – lower O2 at tissues

• Proprioceptor stimulation– exercise – stimulate respiration (PCO2 increase, PO2
decrease, H+ increase)
– From proprioceptors - in joints and muscles
– Stretch sensitive – baroreceptors in walls of alveoli
• Inflation reflex – Hering breur reflex – during overinflation stretch receptors are stimulated andinspiratory area is stimulated, as exhalation beginslungs deplete and stretch receptors no longerstimulated and inspiratory, apneustic area are nolonger inhibited a new inflation begins, thisprotective mechanism for preventing excessiveinflation of lung called inflation reflex.
Other respiratory influences
• Limbic system stimulation – emotional changesactivates excitatory signal to inspiratory area.
• Temperature – increased temperature increasesrespiration.
• Pain – sudden pain – apnea, prolonged somatic painincreased respiration.
• Stretching of anal sphincter – increases respiration,used in new born.
• Irritation of airways – physical, chemical irritation.
• Blood pressure – sudden rise in BP decreasesrespiration, drop in BP increases respiration.

![Respiratory System [โหมดความเข้ากันได้] · PATHOLOGY OF RESPIRATORY SYSTEM นพ. อรรณพ นาคะป ท Respiratory system U it](https://img.pdfslide.net/doc/110x75/5fa578efd4e80f055f6b3401/respiratory-system-aaaaaaaaaaaaaaaaaa-pathology.jpg)













![Anatomy and Physiology Respiratory System [Tab 2] Respiratory System](https://img.pdfslide.net/doc/110x75/56649ebd5503460f94bc631f/anatomy-and-physiology-respiratory-system-tab-2-respiratory-system.jpg)