Embed Size (px)
Citation preview
Dr Kirtan Bhatt
KIMS
Bangalore
Protocol
• Physiologic anatomy of cardiac muscle
• Electrophysiology of normal cardiac rhythm Cardiac action potential Impulse formation and conduction Control of rhythmicity and conduction by nervesHeterogeneity of action potential in heartRefractoriness and conduction failure
• Mechanism of cardiac arrhythmias Abnormality in impulse formation Abnormality in impulse conduction
• Basic pharmacology of anti-arrhythmic drugs Mechanism of action Classification
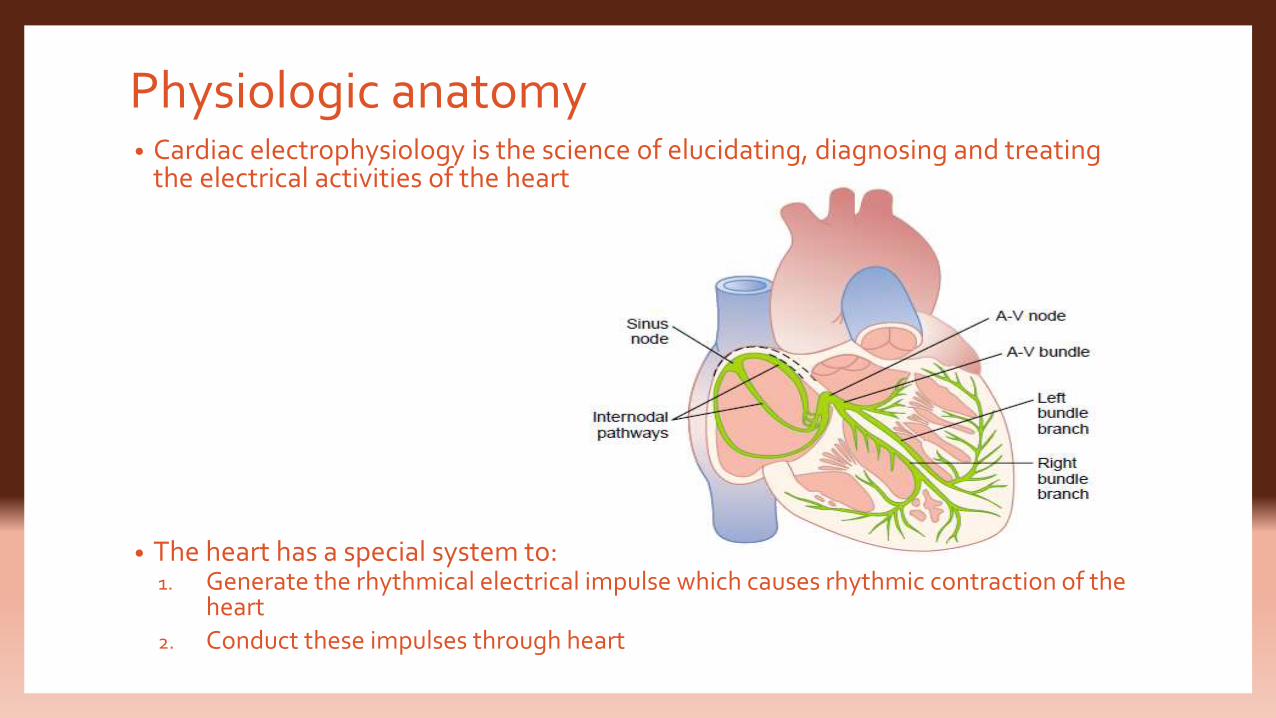
Physiologic anatomy• Cardiac electrophysiology is the science of elucidating, diagnosing and treating
the electrical activities of the heart.
• The heart has a special system to:1. Generate the rhythmical electrical impulse which causes rhythmic contraction of the
heart
2. Conduct these impulses through heart
• The heart is composed of 3 major types of cardiac muscle:1. Atrial muscle
2. Ventricular muscle
3. Specialized excitatory or conductive muscle fibers
• The atrial and the ventricular muscles contract in much the same way as skeletal muscle
• The specialized conductive muscle fibers are mainly responsible for automatic rhythmic discharge in form of action potential or conduction of the action potentials through heart
• Cardiac muscle as a syncytium
Electrophysiology of normal cardiac rhythm
• Each heart beat results from the highly integrated electro-physiologic behaviour
of multiple proteins on multiple cardiac cells.
• The shape and duration of each action potential are determined by activity of ion
channel protein complexes in the membranes of individual cells.
• Cardiac muscle has 3 types of channels that play a role in the action potential:
1. Fast sodium channels
2. Slow sodium-calcium channels
3. Potassium channels
• These channels undergo conformational changes allowing the flow of ions
according to the electrochemical gradient.
• The flow occurs through the specific ion channels and transporters and not
through lipid bilayer
• Channels are macromolecular complexes consisting of a pore-forming α subunit,
as well as β subunits and accessory proteins.
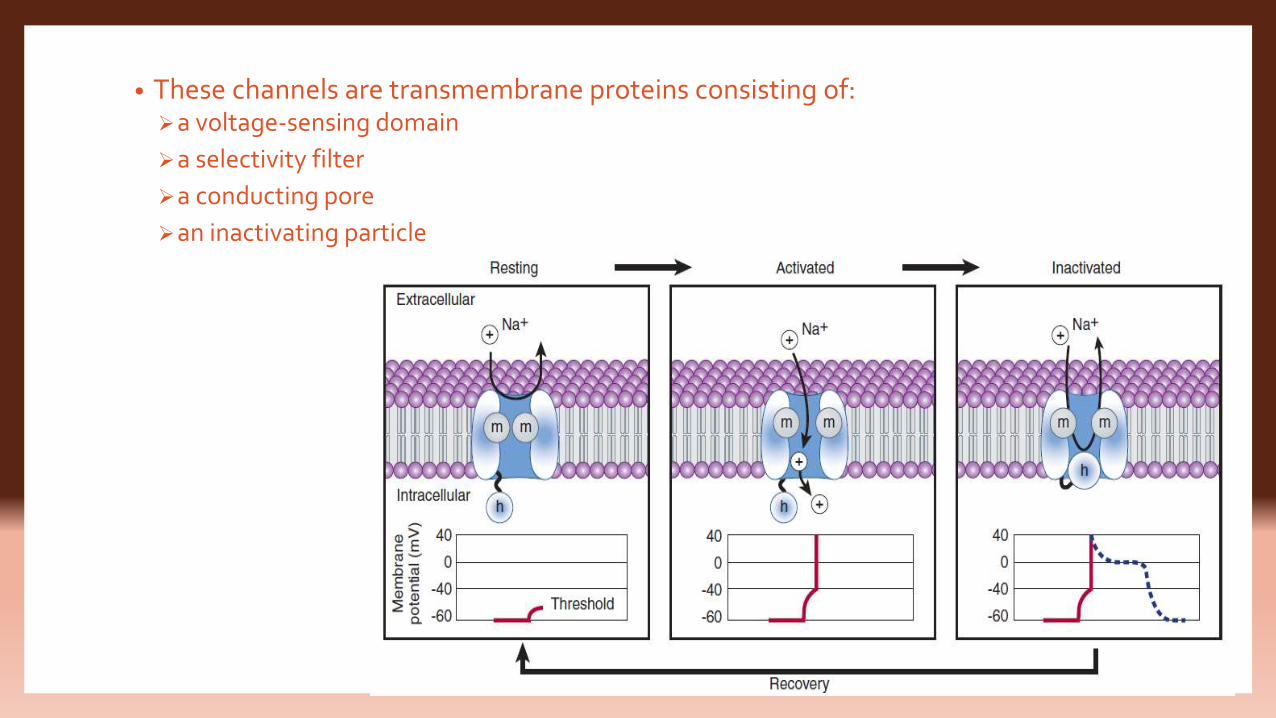
• These channels are transmembrane proteins consisting of:a voltage-sensing domain
a selectivity filter
a conducting pore
an inactivating particle
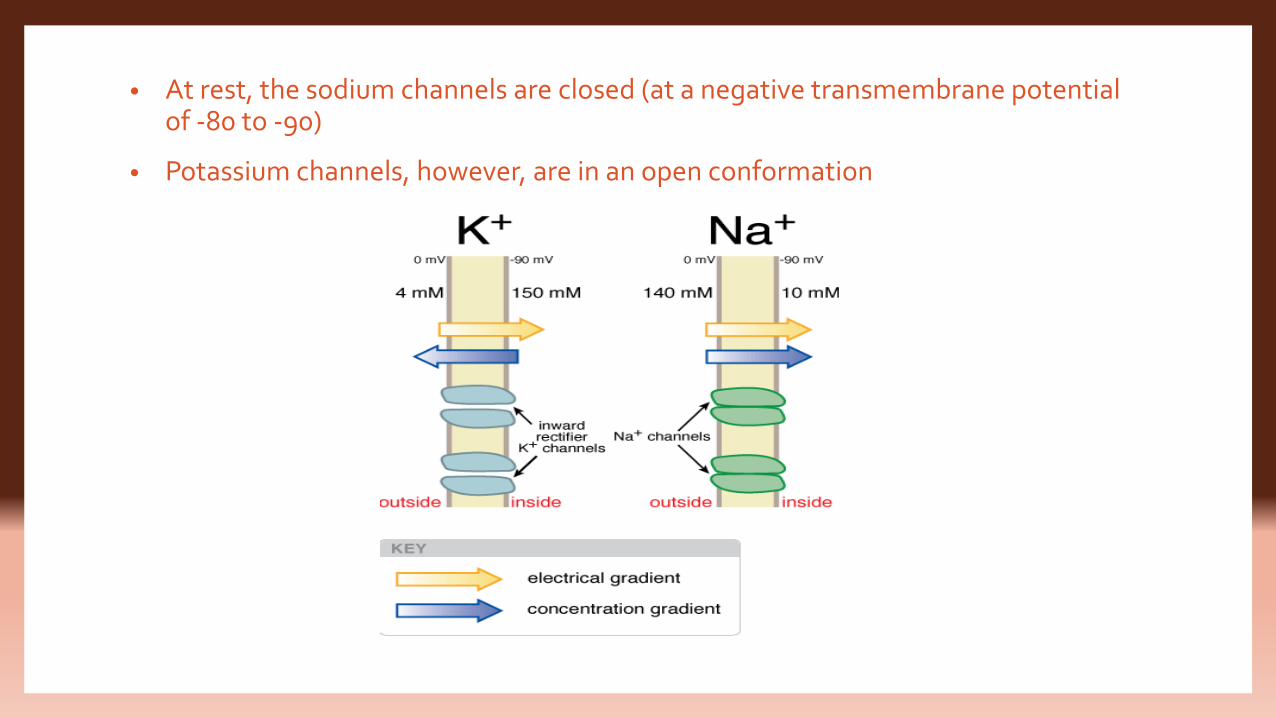
• At rest, the sodium channels are closed (at a negative transmembrane potential of -80 to -90)
• Potassium channels, however, are in an open conformation
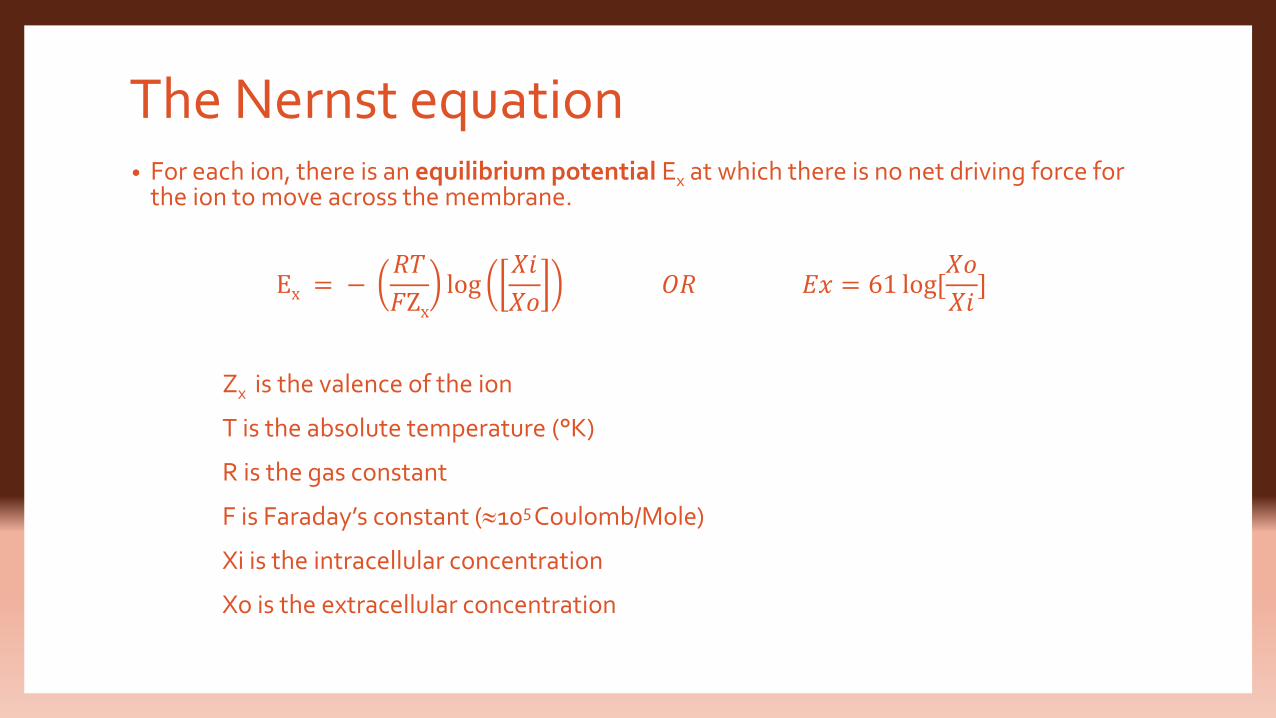
The Nernst equation• For each ion, there is an equilibrium potential Ex at which there is no net driving force for
the ion to move across the membrane.
Ex = −𝑅𝑇
𝐹Zxlog
𝑋𝑖
𝑋𝑜𝑂𝑅 𝐸𝑥 = 61 log[
𝑋𝑜
𝑋𝑖]
Zx is the valence of the ion
T is the absolute temperature (°K)
R is the gas constant
F is Faraday’s constant (105 Coulomb/Mole)
Xi is the intracellular concentration
Xo is the extracellular concentration
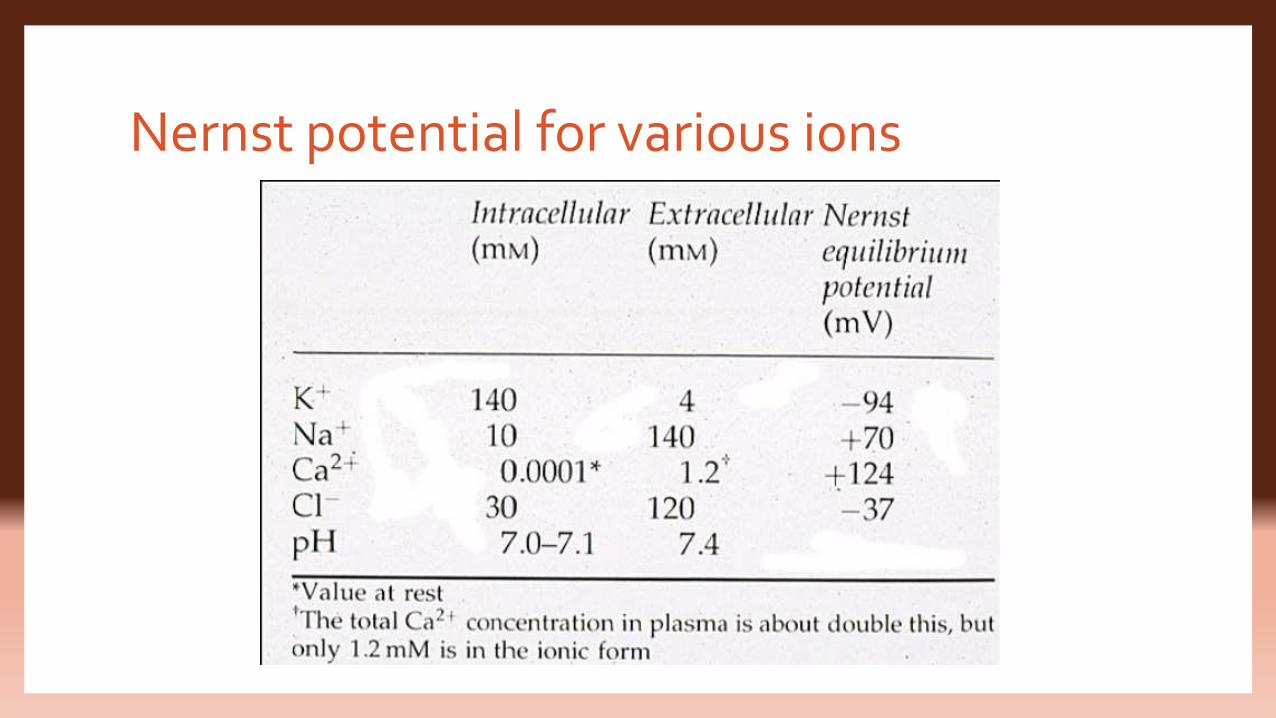
Nernst potential for various ions
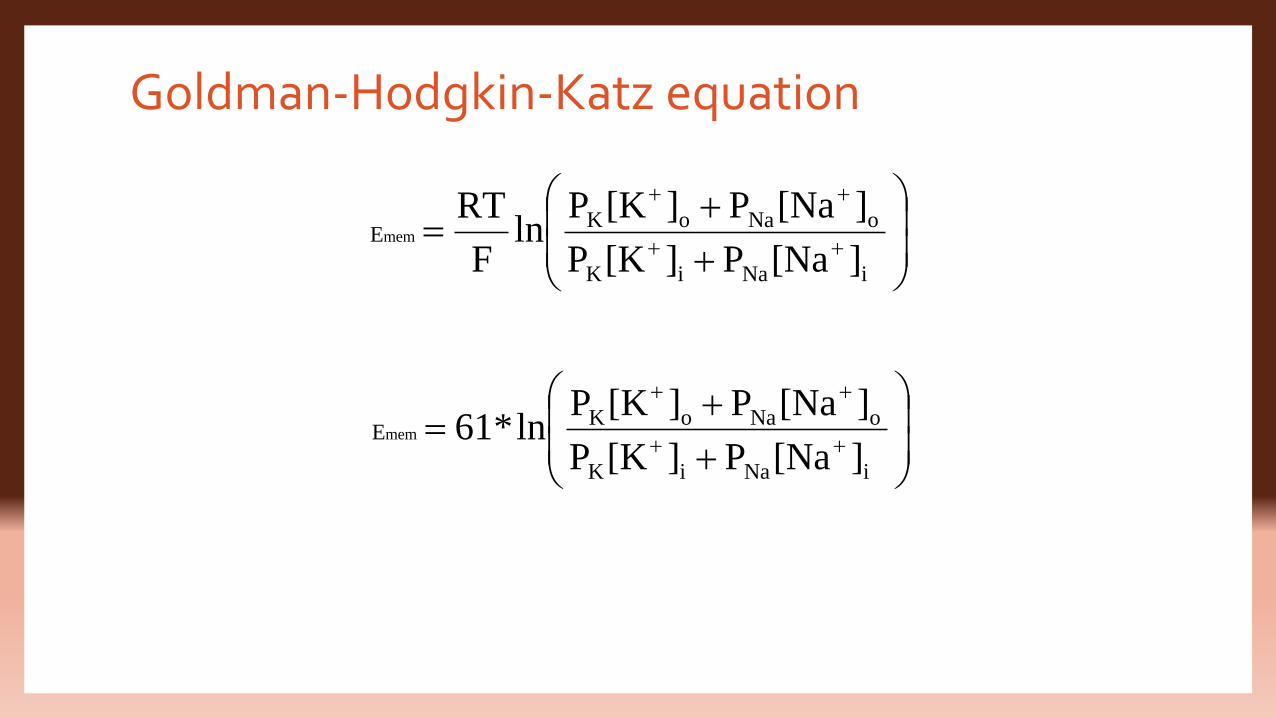
Goldman-Hodgkin-Katz equation
iNaiK
oNaoKE
][NaP][KP
][NaP][KPln
F
RT mem
iNaiK
oNaoKE
][NaP][KP
][NaP][KPln*61 mem
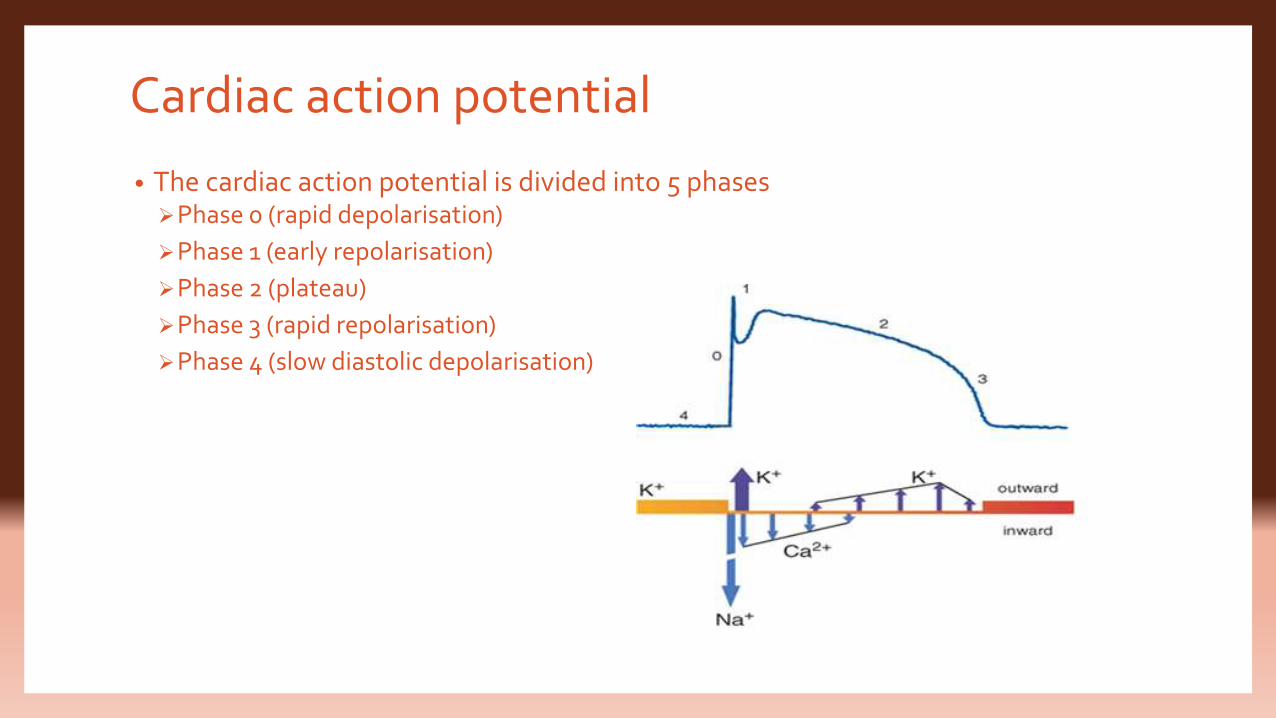
Cardiac action potential
• The cardiac action potential is divided into 5 phasesPhase 0 (rapid depolarisation)
Phase 1 (early repolarisation)
Phase 2 (plateau)
Phase 3 (rapid repolarisation)
Phase 4 (slow diastolic depolarisation)
Phase 0 (rapid depolarisation)
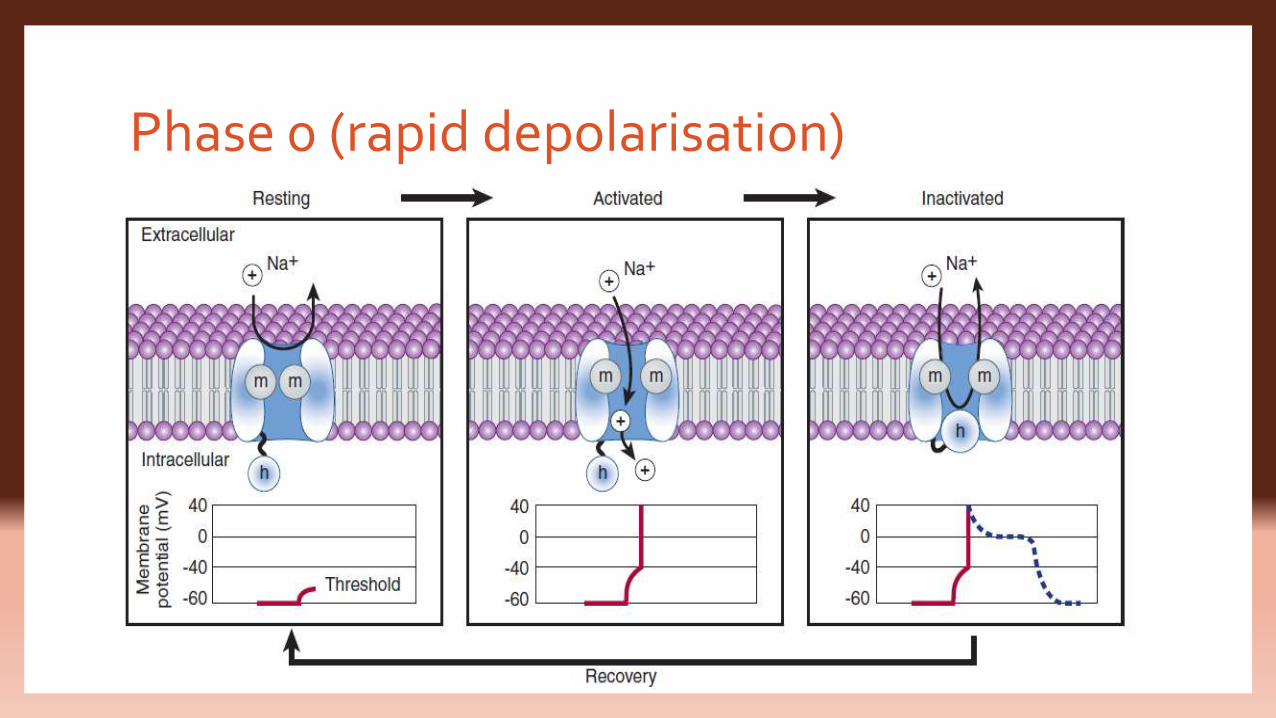
Phase 0 (rapid depolarisation) • Entry of Na+ through the fast inward Na+ channels allowing upto 107 Na+ ions/sec
to enter each cell and moving the transmembrane potential towards ENa (+65mV).
• This surge of sodium ions lasts only about a millisecond, after which the sodium channels changes its conformation from the “open” state to “inactivated” state
• The upstroke of depolarisation ceases as the Na+ inflow stops and at this stage, the inactivated Na+ channels cannot be recruited for further generation of action potential. This interval during which myocyte cannot be stimulated is called the absolute refractory period.
Phase 1 (early repolarisation)
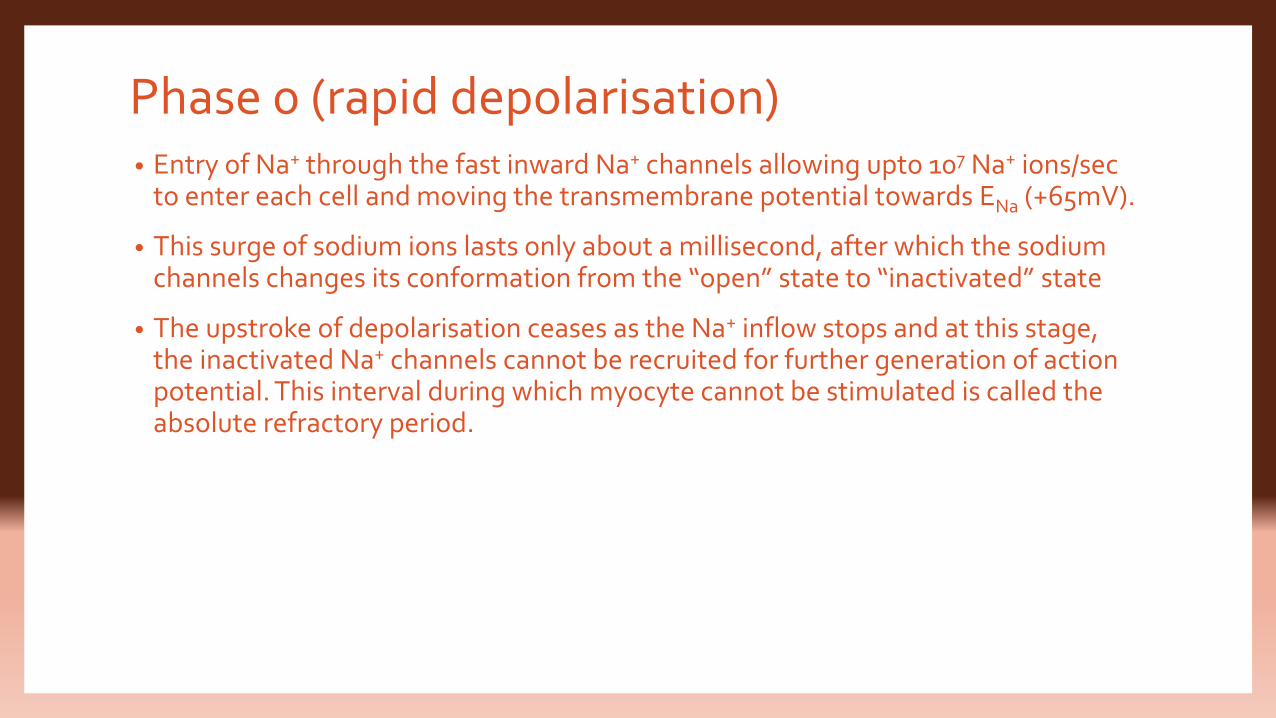
• The voltage-gated Na+ channels close and potassium channels rapidly open which are the “transient outward” potassium channels.
• Because the transmembrane potential at the end of phase 0 is positive to Ek, the opening of these channels and results in outward potassium flux which is responsible for the notch seen in this phase. The repolarising K+ current is known as ITO.
• The cell rapidly repolarises and the membrane potential returns to 0 mV producing a spike and doom pattern of the AP.
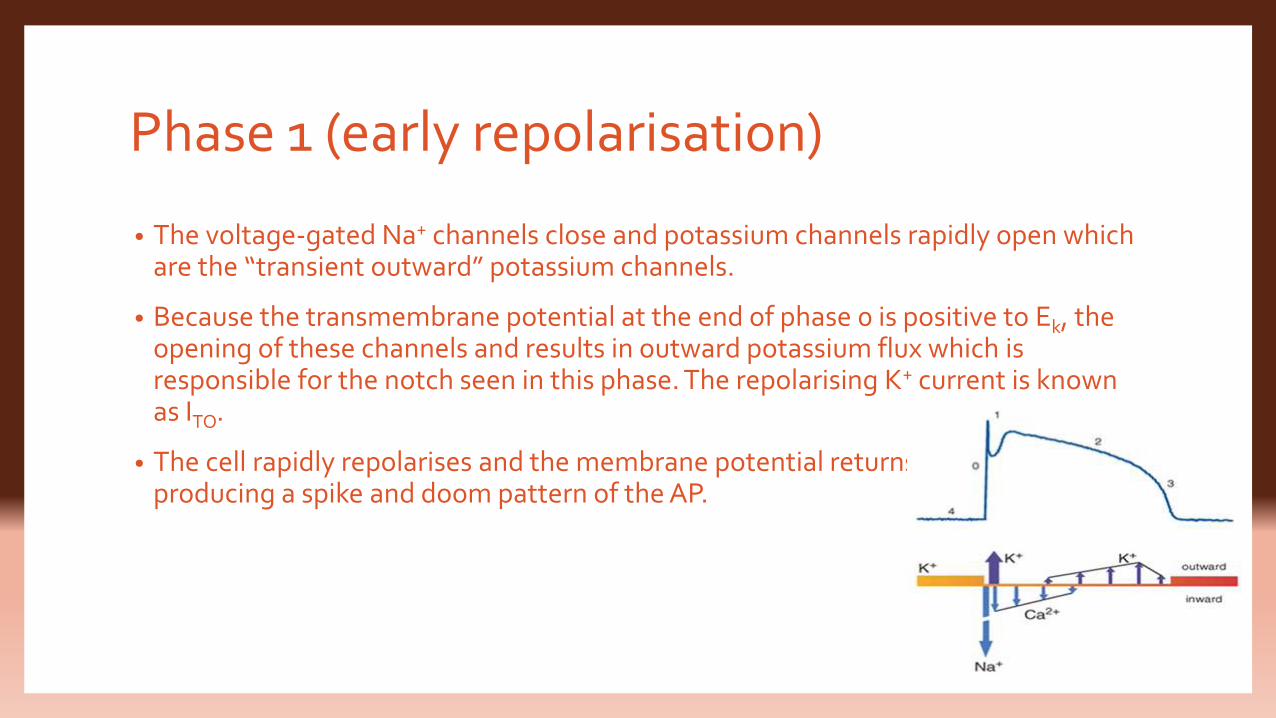
Phase 2 (plateau)• Voltage-sensitive L-type Ca+ channels open causing slow inward current which is
balanced by slow outward K+ (delayed rectifier channels) current. (depolarisation = repolarisation or Ca+= K+)
• The membrane electrical activity stabilizes temporarily and the AP reaches a plateau. This is preceded by a notch at the beginning of the plateau.
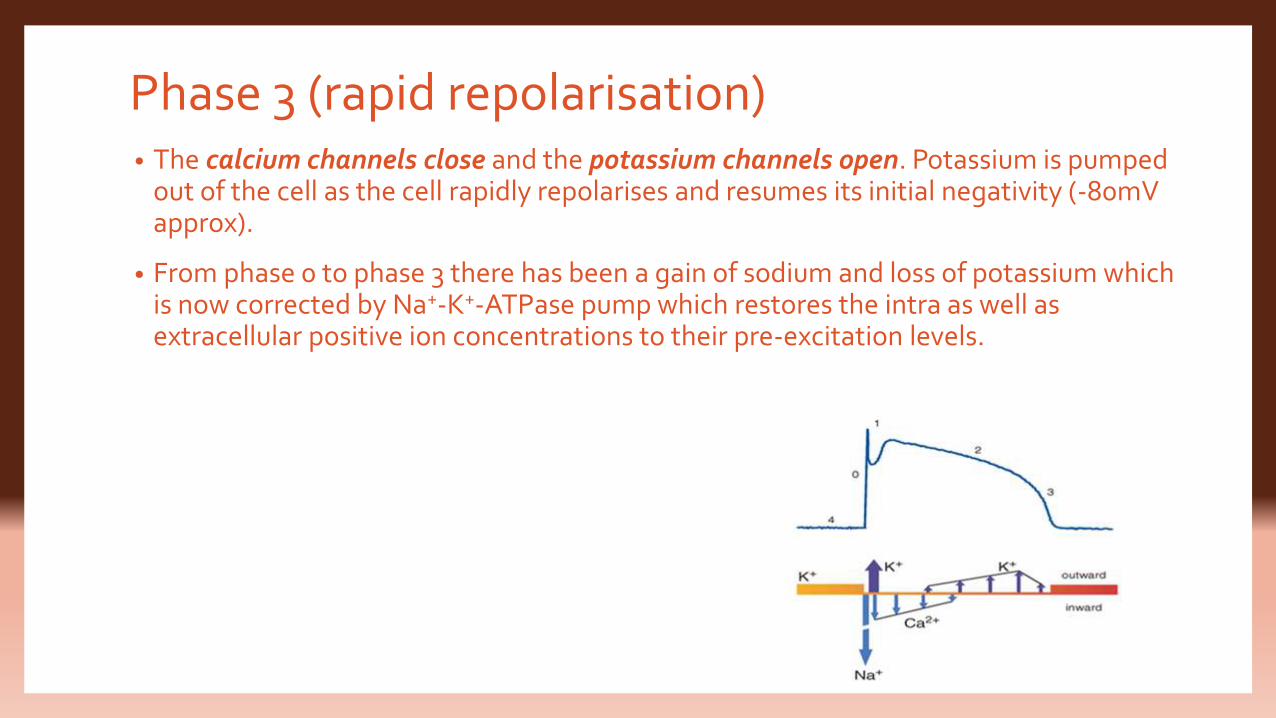
Phase 3 (rapid repolarisation)• The calcium channels close and the potassium channels open. Potassium is pumped
out of the cell as the cell rapidly repolarises and resumes its initial negativity (-80mV approx).
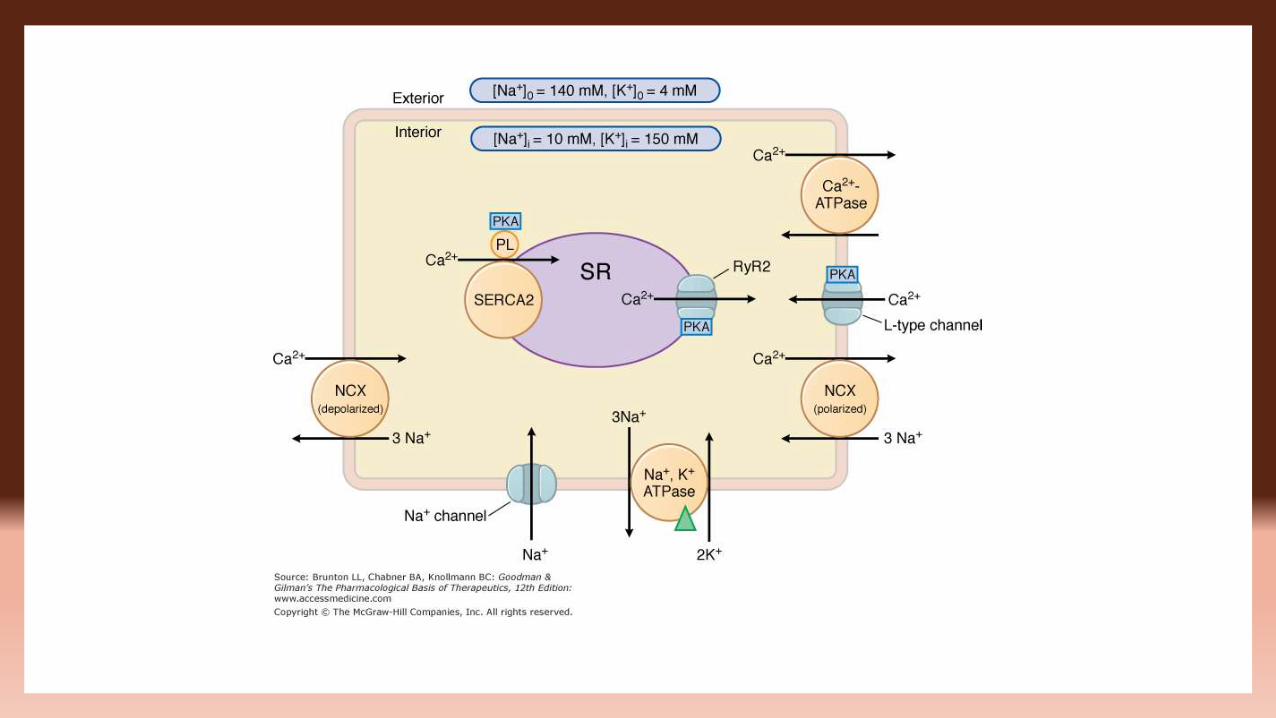
• From phase 0 to phase 3 there has been a gain of sodium and loss of potassium which is now corrected by Na+-K+-ATPase pump which restores the intra as well as extracellular positive ion concentrations to their pre-excitation levels.
Phase 4 (slow diastolic depolarisation)
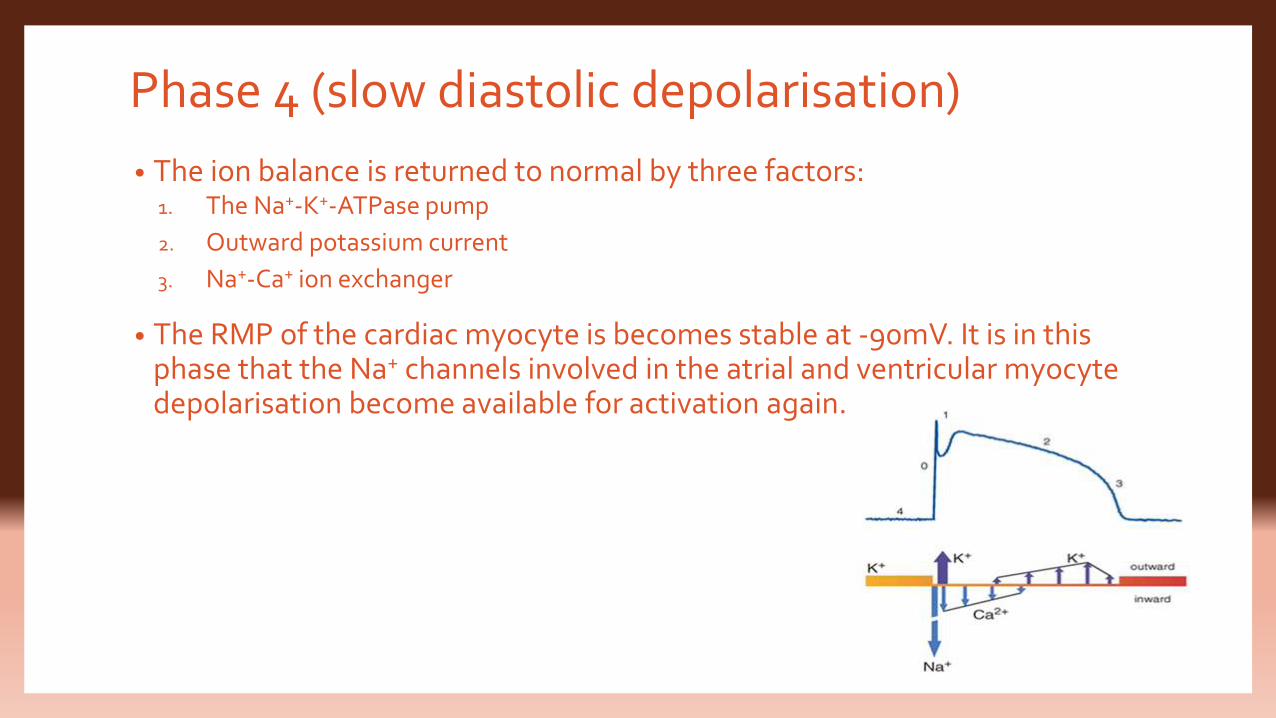
• The ion balance is returned to normal by three factors:1. The Na+-K+-ATPase pump
2. Outward potassium current
3. Na+-Ca+ ion exchanger
• The RMP of the cardiac myocyte is becomes stable at -90mV. It is in this phase that the Na+ channels involved in the atrial and ventricular myocytedepolarisation become available for activation again.
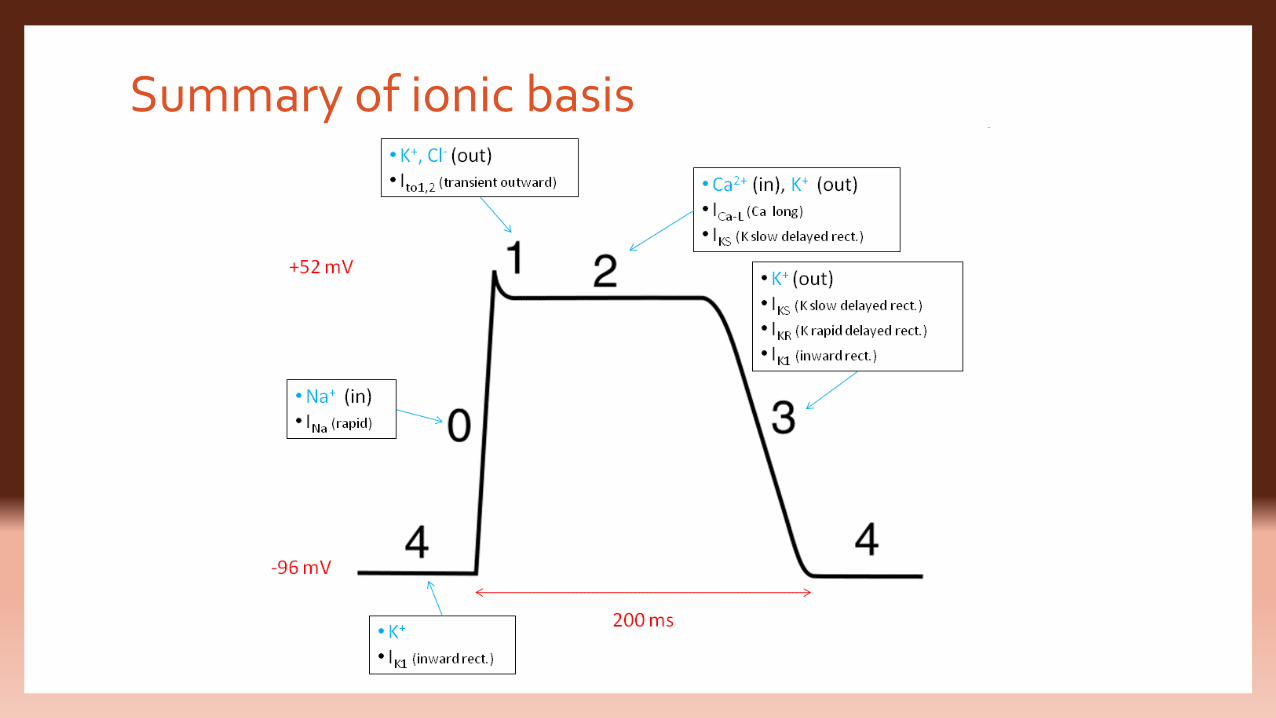
Summary of ionic basis
What causes long action potential and plateau?Two major differences between membrane properties of cardiac and skeletal muscle:
The action potential in skeletal muscle is caused almost entirely by sudden opening of large
numbers of so-called fast sodium channels.
These channels close within a thousandth of a second (a millisecond) and the action
potential is over soon
In cardiac muscles, the action potential is caused by the same fast sodium channels and
also another entirely different population of slow calcium channels (also known as
calcium-sodium channels)
• The other major difference is that immediately after the onset of the action
potential, the permeability of the cardiac muscle membrane for potassium ions
decreases about five-fold
• Due to this, recovery of action potential to its resting level is delayed producing
longer duration of action potential
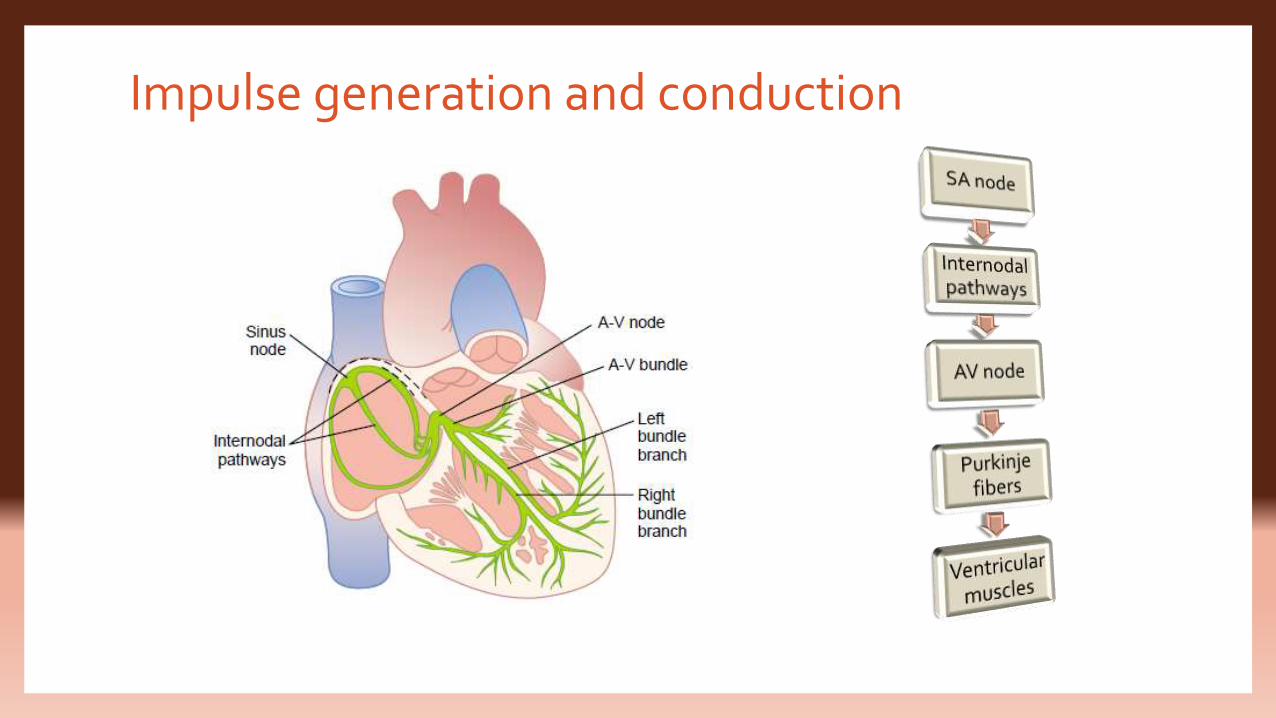
Impulse generation and conduction
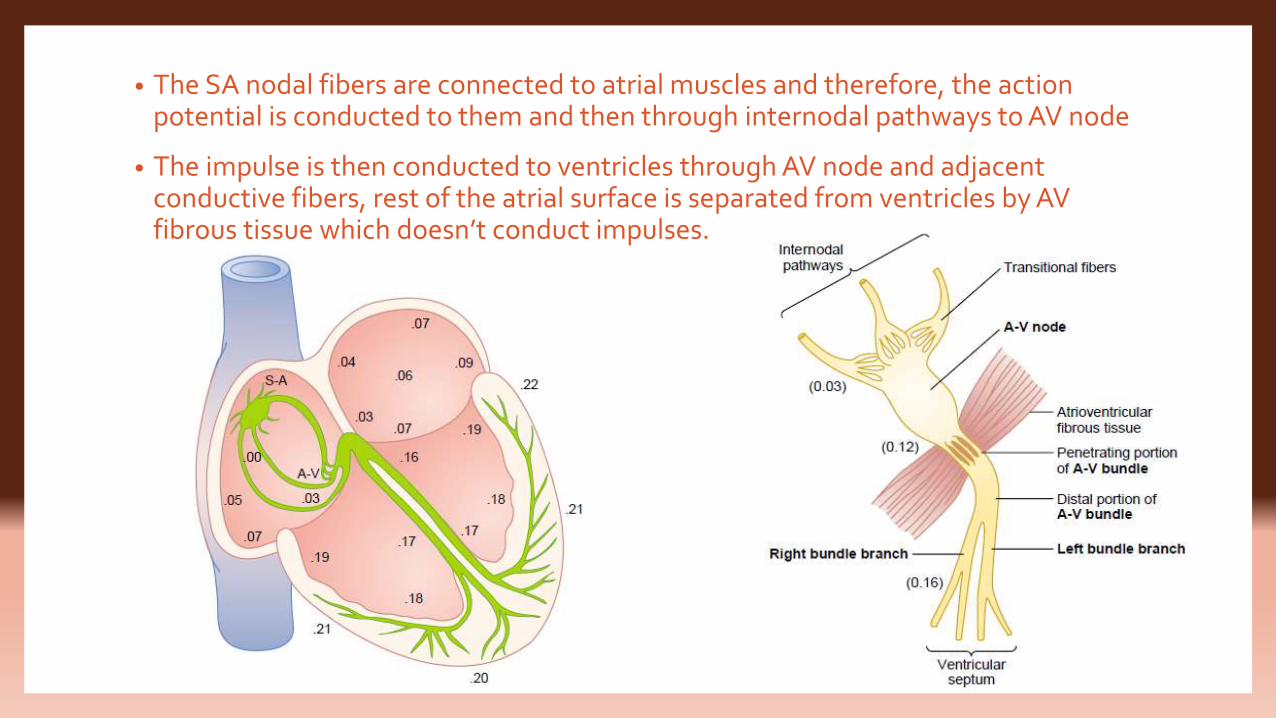
• The SA nodal fibers are connected to atrial muscles and therefore, the action potential is conducted to them and then through internodal pathways to AV node
• The impulse is then conducted to ventricles through AV node and adjacent conductive fibers, rest of the atrial surface is separated from ventricles by AV fibrous tissue which doesn’t conduct impulses.
• The Purkinje system conduct the impulse at a rate of 1.5-4 m/s, 6 times faster than
conduction in ventricular muscles and 150 times faster than some AV nodal fibers
• The Purkinje fibers become continuous with ventricular muscle fibers at their
termination
• The conduction in the ventricular muscles is at 0.3-0.5 m/s and the muscles wrap
the heart in a double spiral, therefore, the impulse doesn’t travel directly towards
the surface of the heart but angulates towards the surface along the direction of
fibers
Conduction velocity in different tissues• Depends on which currents are activated and how much
1.Fastest: Purkinje fibers - largest number of Na+ channels. Many Ca2+
channels.
2.Fast: V and A muscle - large number of Na+ channels. Many Ca2+ channels.
3.Slowest: SA and AV node. No Na+ channels. Ca2+ channels underlie
conducted AP. More than enough Ca2+ channels.
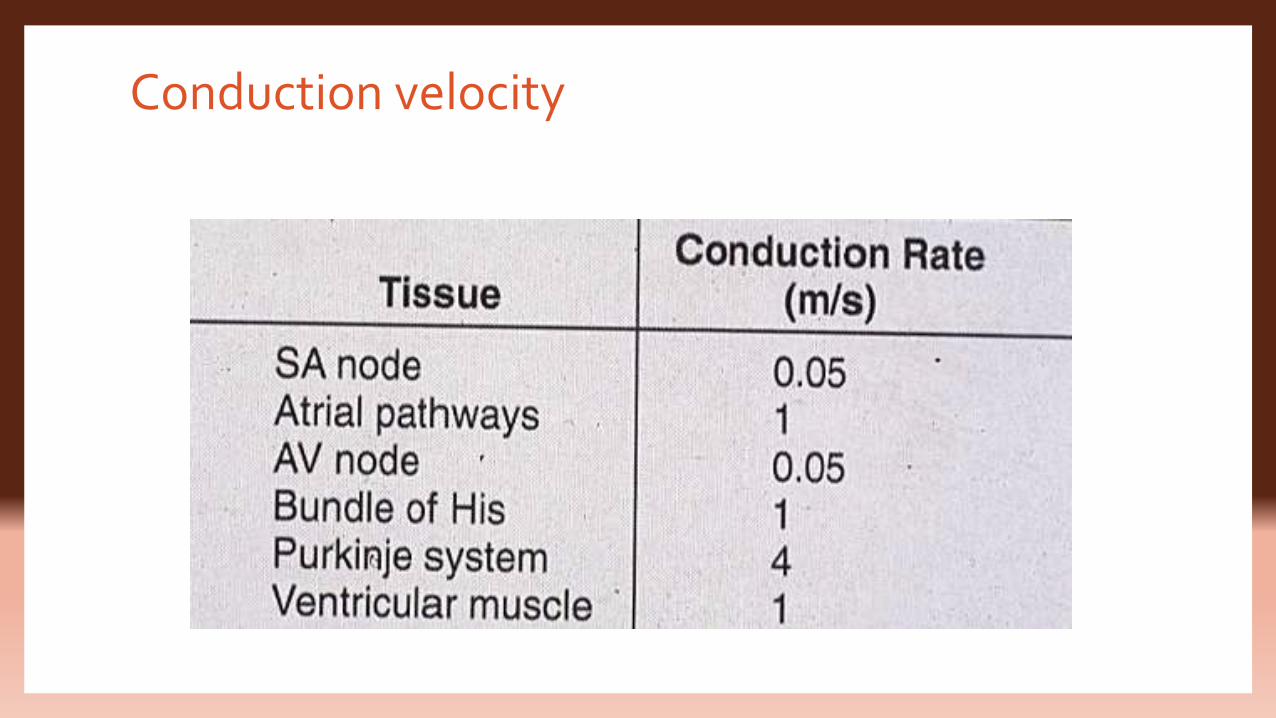
Conduction velocity
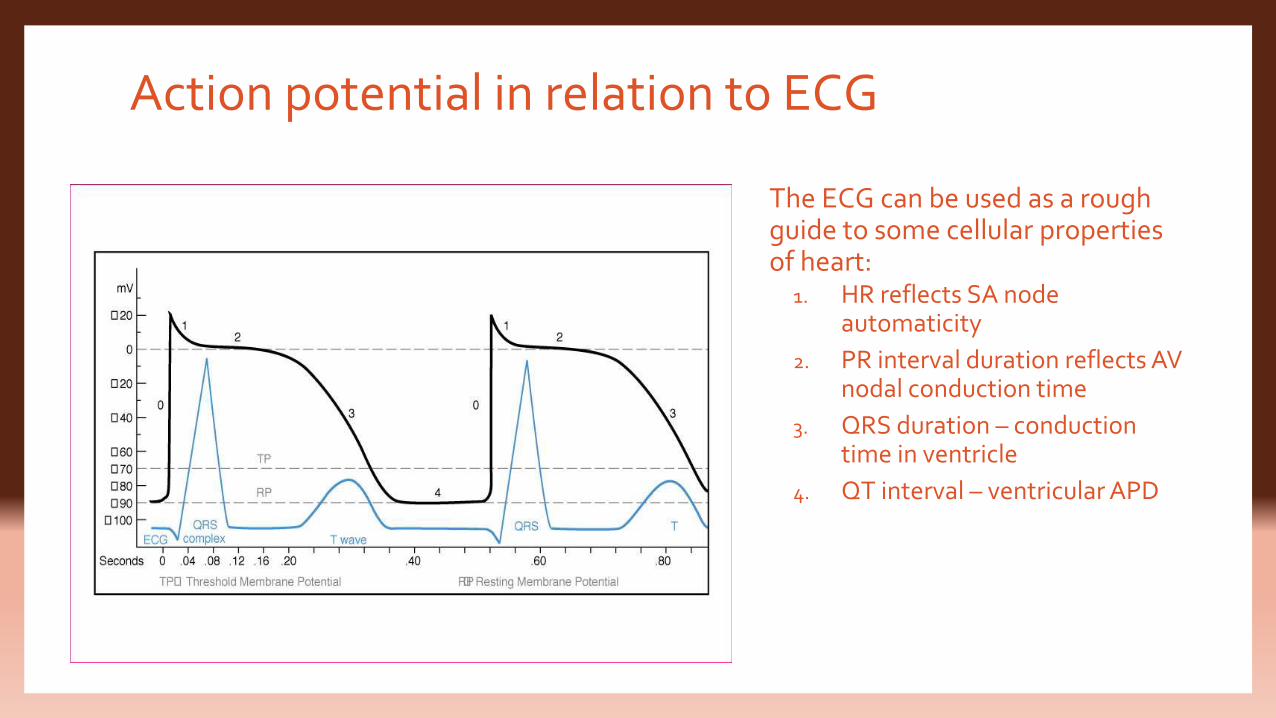
Action potential in relation to ECG
The ECG can be used as a rough guide to some cellular properties of heart:
1. HR reflects SA node automaticity
2. PR interval duration reflects AV nodal conduction time
3. QRS duration – conduction time in ventricle
4. QT interval – ventricular APD
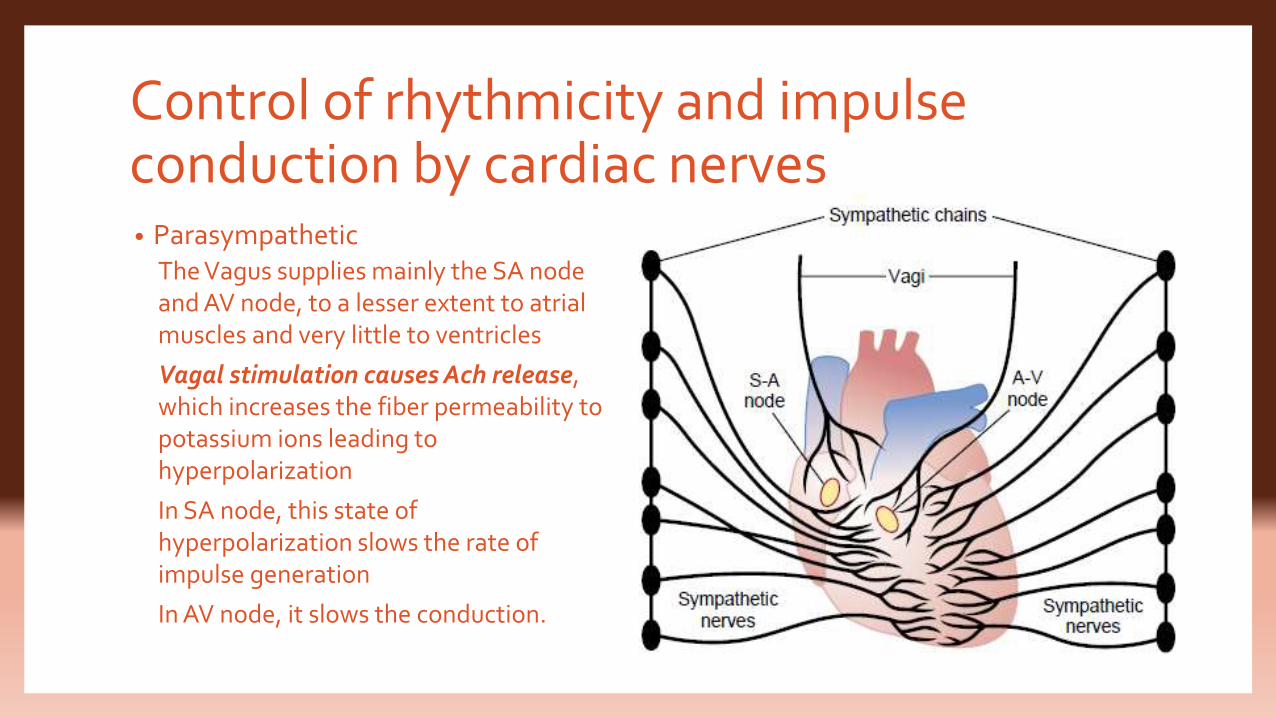
Control of rhythmicity and impulse conduction by cardiac nerves• Parasympathetic
The Vagus supplies mainly the SA node and AV node, to a lesser extent to atrial muscles and very little to ventricles
Vagal stimulation causes Ach release, which increases the fiber permeability to potassium ions leading to hyperpolarization
In SA node, this state of hyperpolarization slows the rate of impulse generation
In AV node, it slows the conduction.
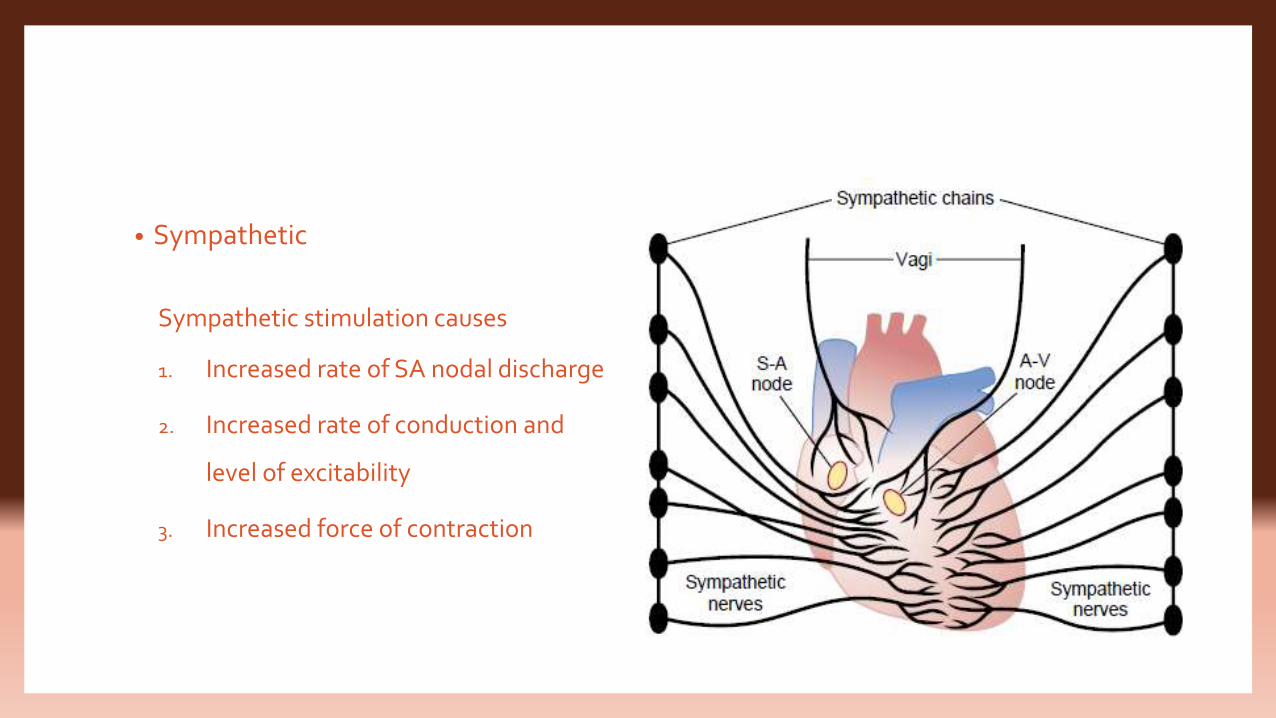
• Sympathetic
Sympathetic stimulation causes
1. Increased rate of SA nodal discharge
2. Increased rate of conduction and
level of excitability
3. Increased force of contraction
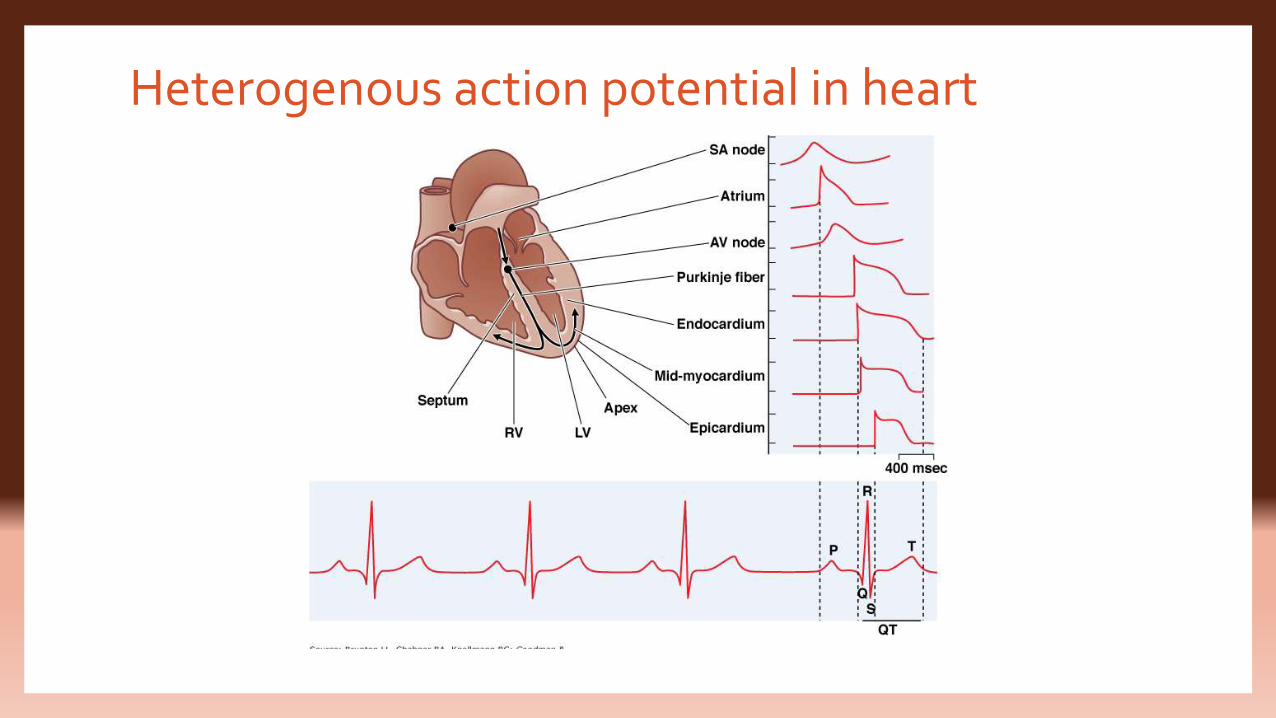
Heterogenous action potential in heart
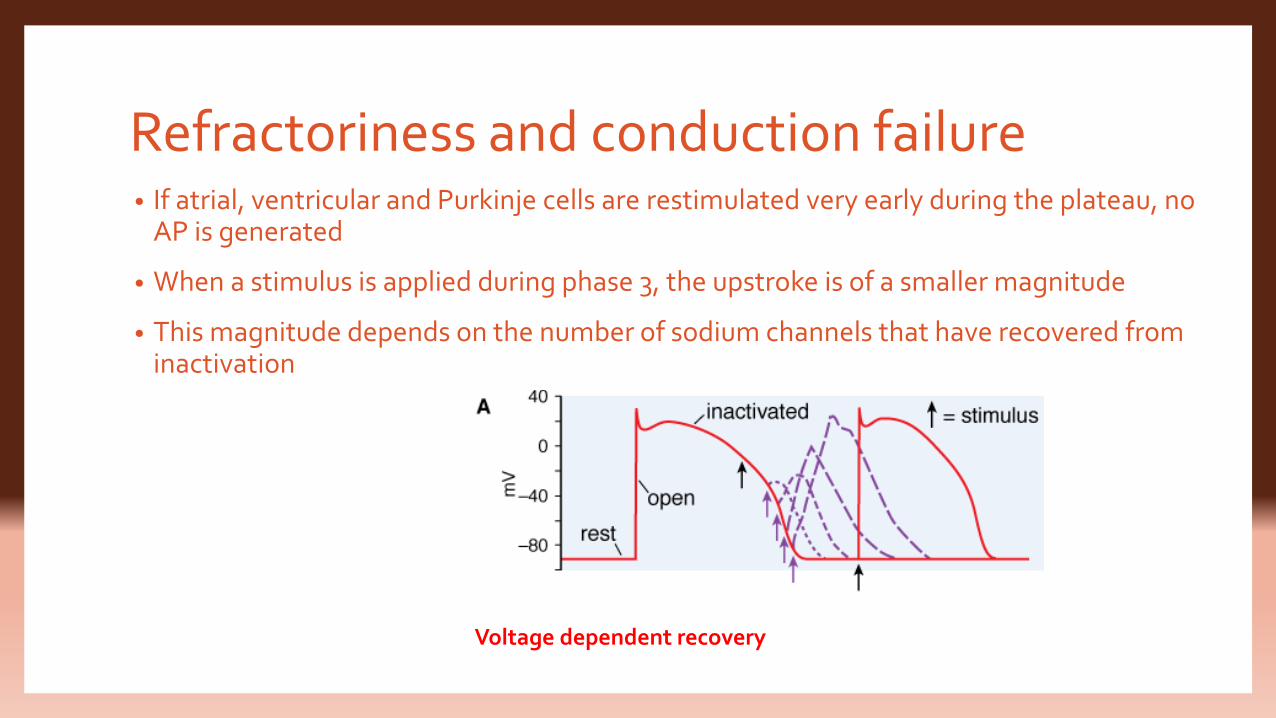
Refractoriness and conduction failure• If atrial, ventricular and Purkinje cells are restimulated very early during the plateau, no
AP is generated
• When a stimulus is applied during phase 3, the upstroke is of a smaller magnitude
• This magnitude depends on the number of sodium channels that have recovered from inactivation
Voltage dependent recovery
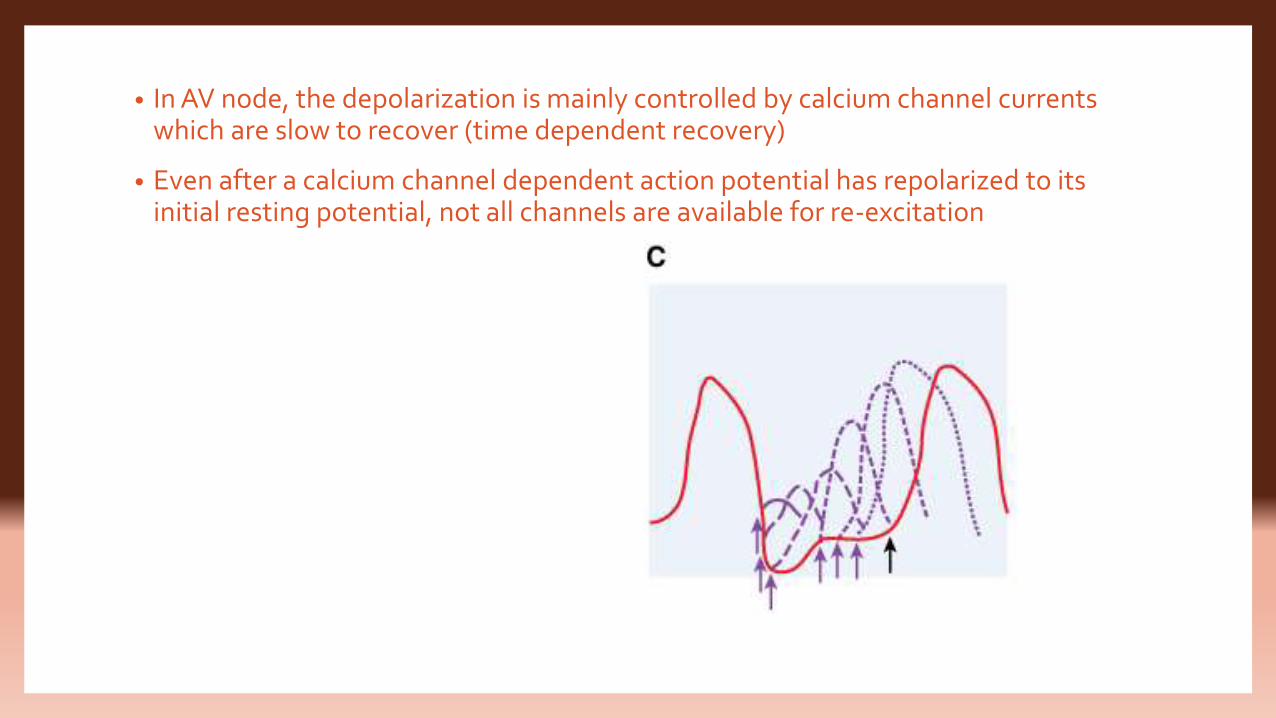
• In AV node, the depolarization is mainly controlled by calcium channel currents which are slow to recover (time dependent recovery)
• Even after a calcium channel dependent action potential has repolarized to its initial resting potential, not all channels are available for re-excitation
Mechanism of cardiac arrhythmias• Cardiac arrhythmias result from abnormalities of electrical impulse generation,
conduction, or both.
• Based on the rate of impulse generation, arrhythmias are;1. Bradyarrhythmia
2. Tachyarrhythmia
Factors precipitating arrhythmias• Ischemia
• Hypoxia
• Acidosis or alkalosis
• Electrolyte disturbances
• Excessive catecholamine exposure
• Autonomic influences
• Drug toxicityGA , Digitalis, sympathomimetic agents , TCA,Terfinadine, Antipsychotics, cisapride, erythromycin
• Overstretching of cardiac fibers
• Presence of scarred or otherwise diseased tissue
Abnormalities in impulse formation• Abnormalities in impulse formation can occur by 2 mechanisms:
1. Enhanced automaticity
2. After depolarisations and triggered automaticity
Enhanced automaticity
• This is seen in cells that normally display spontaneous diastolic depolarisations –
the SA node, AV node and His-Purkinje system
• Hypokalemia, mechanical stretch of cardiac fibers, β adrenergic stimulation,
acidosis and positive inotropic drugs increase the phase 4 slope and so increase
the pacemaker rate
• Vagal stimulation, β blockers and Ach decrease the phase 4 slope and decrease
the pacemaker rate
After depolarisations and triggered automaticity
• Early afterdepolarisations are seen when there is increased duration of action
potential which is seen due to hypokalemia, drugs prolonging action potential
duration
• These EADs occur more readily in Purkinje cells than in epicardial or endocardial
cells and can give rise to polymorphic ventricular tachycardia with long QT interval
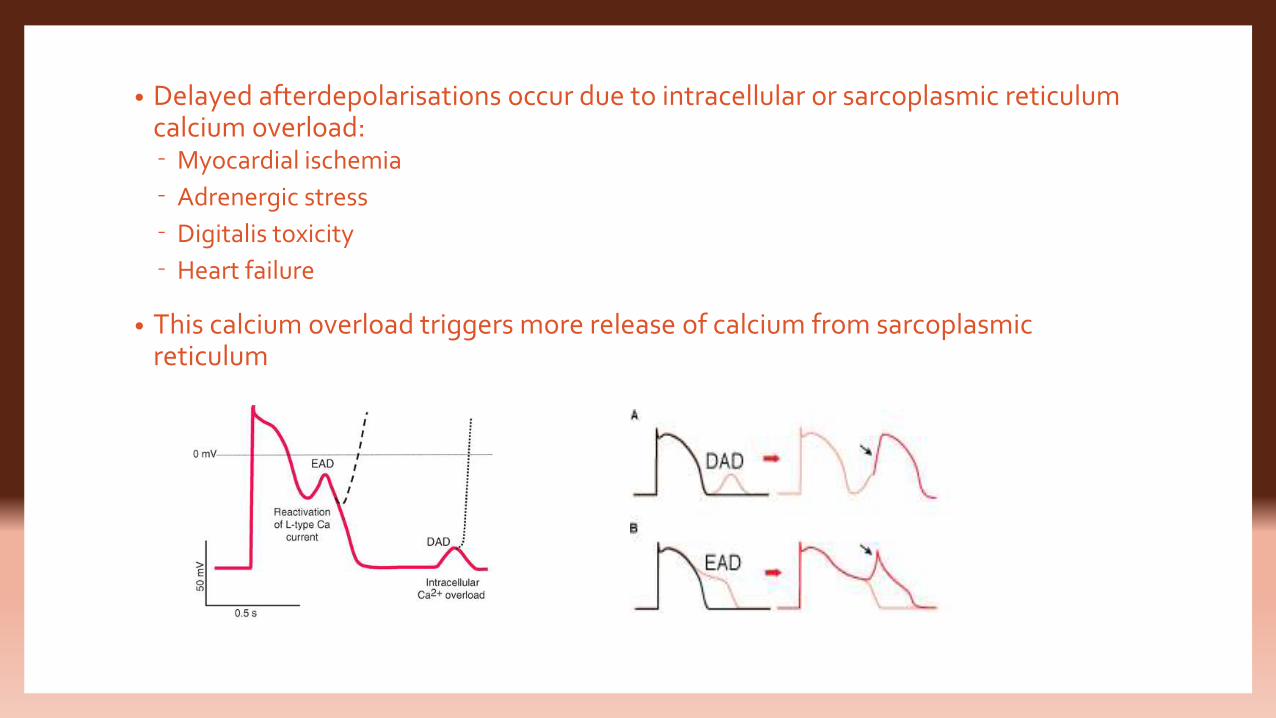
• Delayed afterdepolarisations occur due to intracellular or sarcoplasmic reticulum calcium overload:⁻ Myocardial ischemia
⁻ Adrenergic stress
⁻ Digitalis toxicity
⁻ Heart failure
• This calcium overload triggers more release of calcium from sarcoplasmic reticulum
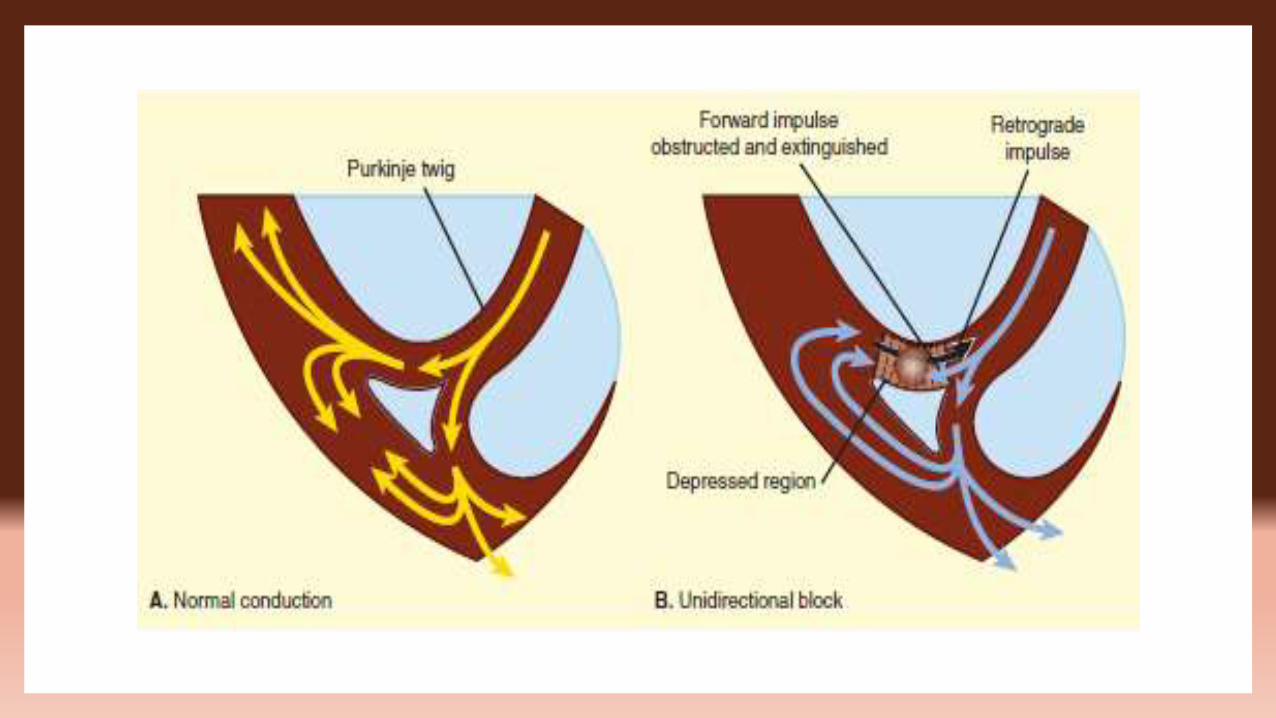
Abnormalities in impulse conduction
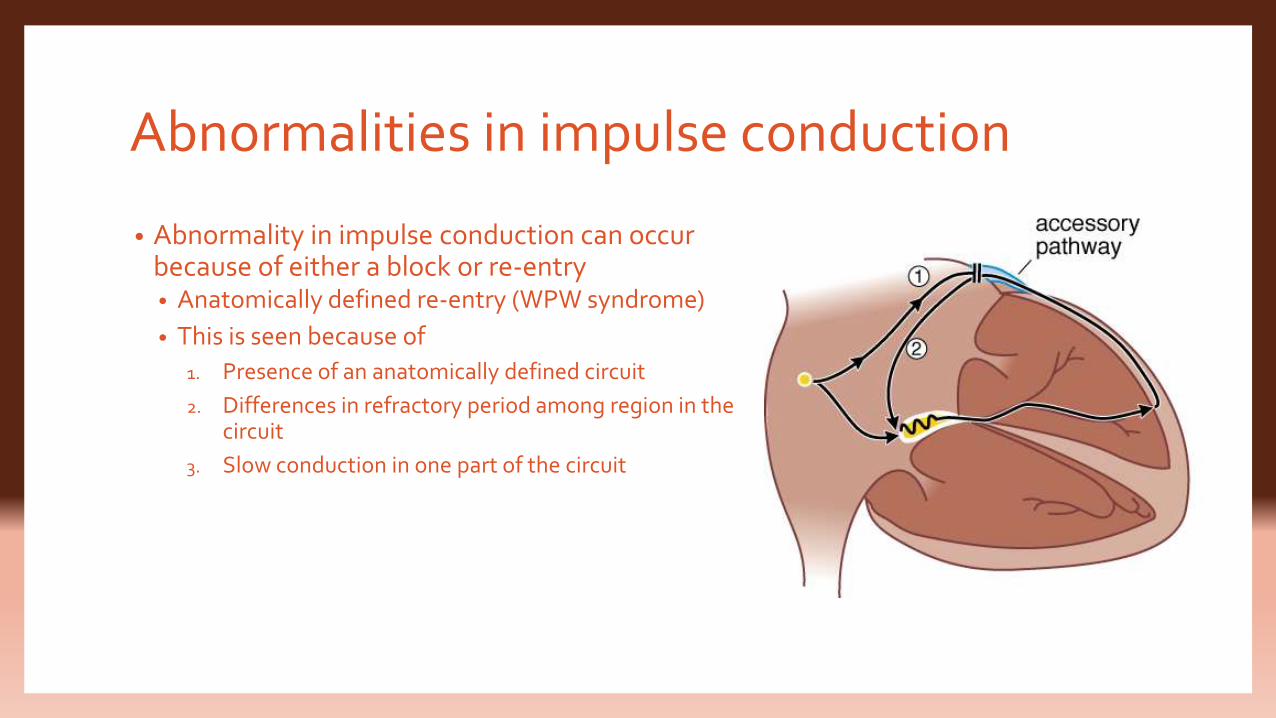
• Abnormality in impulse conduction can occur because of either a block or re-entry• Anatomically defined re-entry (WPW syndrome)
• This is seen because of
1. Presence of an anatomically defined circuit
2. Differences in refractory period among region in the circuit
3. Slow conduction in one part of the circuit
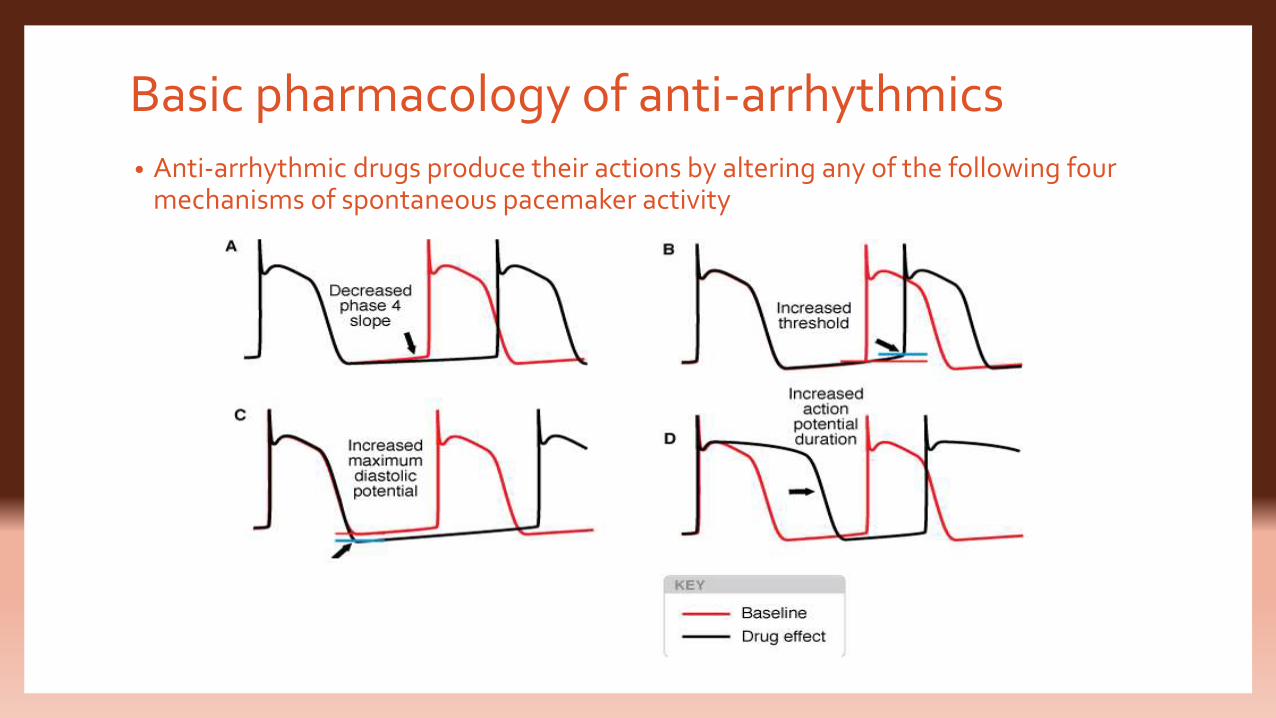
Basic pharmacology of anti-arrhythmics• Anti-arrhythmic drugs produce their actions by altering any of the following four
mechanisms of spontaneous pacemaker activity
• The major mechanisms by which anti-arrhythmic actions of the drugs is achieved are:1. Sodium channel blockade (class 1)
2. Blockade of autonomic effects in heart (class 2)
3. Prolongation of effective refractory period (class 3)
4. Calcium channel blockade (class 4)
1. Class 1 (sodium channel blockers)I. 1a (prolong the APD and dissociate from sodium channels in 1-10s)
procainamide, Quinidine, disopyramide
II. 1b (shorten the APD and dissociate from sodium channel in <1s)
Lidocaine, mexiletine
III. 1c (minimal effects on APD and dissociate slowly >10s)
Flecainide, propafenone, moricizine
2. Class 2 (β blockers) propranolol
3. Class 3 (Drugs prolonging ERP by prolonging APD)Amiodarone, ibutilide, dofetilide, sotalol
4. Class 4 (calcium channel blockers) Verapamil, diltiazem