Embed Size (px)
Citation preview

Journal of Gastroenterology and Hepatology (1999) 14, 179–193
been, and still are, areas of interest and research forcurrent and ex-members of the Department. Invitedfaculty included Professor Frank Dudley (Alfred Hos-pital, Melbourne) who discussed the medical manage-ment of portal hypertension, Associate ProfessorStephen Locarnini (antiviral agents and when to usethem for viral hepatitis), Professor Lawrie Powell(haemochromatosis) and Professor Neville Yeomans(non-steroidal anti-inflammatory drugs and gastricinjury). The other speakers included Professors BobBatey, Geoff Farrell, Kerry Goulston, John Kaldor, DrsMichael Grimm and Meng Ngu as well as currentmembers of the AW Morrow Gastroenterology andLiver Centre, RPAH. This article includes some of thepresentations made to the meeting.
As mentioned, the meeting paid tribute to ProfessorNeil Gallagher. Neil Gallagher was Director of the AWMorrow Department of Gastroenterology (since 1973)for 25 of its 50 year history. He led a team that trainedat least eight current professors/associate professors ofmedicine and seven current directors of gastroenterol-ogy departments in Australia. His early days in the gas-troenterology unit at RPAH led to the publication ofseminal papers in 1962 on fluid, electrolyte distribu-tions in ileostomy patients, persistent viral hepatitis,chronic painless pancreatitis and an article (with StanGoulston, Bill Morrow and Norman Wyndham) on ful-minant ulcerative colitis.The latter laid the foundationsfor the indications for colectomy in fulminant ulcerativecolitis and changed clinical practice worldwide. Hismain interests at a clinical level have remainedinflammatory bowel disease, malabsorption and viralhepatitis. In the mid 1980s he received major interna-tional recognition for his basic research work in the fieldof vitamin B12 absorption. The ileal receptor remainsuncloned! He also played a pivotal role in the attain-ment, in 1986, of the National Liver TransplantProgram for RPAH and The University of Sydney.
INTRODUCTION¶
A meeting was held on 27–28 February 1998 to cele-brate 50 years of gastroenterology at the Royal PrinceAlfred Hospital, Sydney.This also included a tribute toProfessor Neil Gallagher who retired in January 1998as AW Morrow Professor of Medicine (Gastroenterol-ogy and Hepatology) at the University of Sydney/RoyalPrince Alfred Hospital.
The formal history of gastroenterology at RoyalPrince Alfred began in 1948 when Sir William Morrowwas asked by the Royal Prince Alfred Hospital (RPAH)to establish a specific gastroenterology unit within thehospital. We believe this was the first specific gastroen-terology specialist service to be established in Australia,although concurrent gastroenterology services at theRoyal Melbourne Hospital were established at approx-imately the same time under Ian Wood, in the ClinicalResearch Unit at the Royal Melbourne Hospital. Since1948, gastroenterology and, subsequently, hepatologyhas flourished at RPAH and throughout Australia. Thehistory of the AW Morrow Gastroenterology and LiverUnit has been characterized by pioneering articles ininflammatory bowel and autoimmune liver disease. Acomplete history has been recently edited by ProfessorNeil Gallagher and is available through the Unit.
The meeting was attended by more than 100 dele-gates, including most of the previous members of theUnit, either at registrar or senior level. Notable amongthese were Dr Stanley Goulston, a foundation memberof the Unit, Dr Brian Billington, the first registrar, DrAlan Skyring, early Research Director and subsequentlyUnit Director, Professor Alan Cooke, who had travelledfrom Kansas, and many other early members of theUnit who had subsequently become directors of this orother departments of gastroenterology. The meetingbrought together experts in a wide area of gastroen-terology and liver disease and covered topics that had
SPECIAL REPORT
Fifty years of gastroenterology in Australia
LAWRIE W POWELL,* WARWICK S SELBY,† GEOFFREY W MCCAUGHAN‡ AND MICHAEL C GRIMM§
*The Queensland Institute of Medical Research and Department of Medicine,The University of Queensland,Queensland, †Royal Prince Alfred Hospital, Sydney, ‡AW Morrow Gastroenterology and Liver Centre,Royal Prince Alfred Hospital, Sydney, §Department of Medicine, St George Clinical School, Kogarah,
NSW, Australia
Correspondence: Please see the appendix for correspondence addresses for the authors of this special report.Accepted for publication 25 September 1998.¶Part of the introduction is adapted (with permission) from a speech given by Professor Kerry Goulston.

On a personal level, Neil is quietly spoken, yet self-confident in his own ability. His conversation is notalways easy to follow. His tangential thinking and hiscircumlocution are perhaps only rivalled by those ofRuthven Blackburn, and after years of friendship, manystill have trouble following his train of thought. Neil isunassuming, has complete lack of arrogance and noburning need to impress. He is a man who went his ownway in research and followed no one else’s path. He isa leader who is both loved and respected. We wish himwell in retirement.
Geoffrey W McCaughanDirector, AW Morrow Gastroenterology &
Liver Centre
DISORDERS OF HEPATIC IRONMETABOLISM*
There are four major disorders of iron overload whichwill be addressed in this section of the article: (i)primary, hereditary or genetic haemochromatosis; (ii)aceruloplasminaemia; (iii) metabolic iron overload(mild to moderate iron overload with normal transfer-rin saturation; and (iv) disorders in which iron acts asa cofactor in causing liver damage.
The liver plays a major role in normal and abnormaliron metabolism. In the normal state, it acts as a storageorgan for iron, both within parenchymal cells andKupffer cells of the monocyte–macrophage system. Instates of iron overload, particularly haemochromatosis(HHC), the excess iron is stored predominantly inhepatocytes and when tissue iron concentrations rise tosome five to 10-fold normal levels, hepatic fibrosis andcirrhosis develops.1
Primary, hereditary or genetichaemochromatosis
This condition was described in Europe just over 100years ago.2,3 In this disease, there is progressive increasein iron stores derived from a normal diet as the regula-tory control mechanism governing iron absorption isaffected by the basic metabolic defect. The excess ironis stored in hepatocytes and eventually leads to hepaticfibrosis and cirrhosis. Thus, HHC is probably bestdefined as primary iron overload resulting in cirrhosisand failure of other organs not secondary to chronicanaemia or end-stage liver disease. Although the diseaseaffects primarily the liver, other organs are affected,resulting in diabetes mellitus, cardiomyopathy, skin pig-mentation and hypogonadism. Interestingly, virtuallyidentical complications can arise from secondary ironoverload due to thalassaemia and other chronicanaemias with increased iron absorption or repeatedtransfusion.
The gene responsible for hereditary HHC hasrecently been cloned4 and it has been shown to encodea non-classical class I molecule (HFE) on the short armof chromosome 6. HFE combines with b2-microglob-ulin in the endoplasmic reticulum, whence it is trans-ported to the cell surface. The physiological ligand has
180 LW Powell et al.
not yet been identified with certainty. However, recentwork suggests it is the transferrin receptor.5
Haemochromatosis is very common in populations ofNorthern European extraction. Recent studies show aprevalence of one in 300 affected (homozygous for themutation) and approximately one in 10 carriers (het-erozygous for the mutation). A single point mutationresulting in a cysteine to tyrosine substitution at posi-tion 282 (C282Y) accounts for between 65 and 90% of cases of HHC and virtually all familial cases in Australia.6
First degree relatives of patients with HHC should bescreened using transferrin saturation and, if elevated,they should be further evaluated. Human leucocyteantigen (HLA) typing has been useful in assigning aputative diagnosis of homozygous HHC to the HLAidentical siblings of an index case. A DNA-based diag-nostic test for the C282Y mutation in the HFE gene isan exciting development, but its place in diagnosis andpopulation screening is still under evaluation. However,it has a role in the evaluation of siblings of known cases.In contrast, the transferrin saturation remains a simplereliable screening test for iron overload and is the pre-ferred screening test in the routine evaluation for sub-jects of iron overload without a definite family historyof HHC.Therapy consists of weekly phlebotomies untilthe serum ferritin and transferrin saturation fall tonormal levels, followed by maintenance phlebotomythree to four times per year. The prognosis is excellentif the diagnosis is made before cirrhosis develops andtherapy is instituted. In cirrhotic subjects, primaryhepatocellular carcinoma is now the major threat to lifeand screening programmes for this tumour are cur-rently under evaluation.
Aceruloplasminaemia
This is a recently described abnormality resulting froma genetic defect in the gene that encodes for the proteinceruloplasmin.7 Aceruloplasmin is a ferroxidase and isnecessary for the mobilization of iron on the cellsurface. Hence, in this condition there is a gradualaccumulation of iron in hepatocytes, with resultant highhepatic iron concentrations, although cirrhosis has notyet been described. Interestingly, other clinical featuresnot seen in HHC have been described, including neu-rological abnormalities. At present, there is no satisfac-tory therapy, although iron can be removed from theliver by desferrioxamine therapy.
Iron overload with normal transferrinsaturation
This recently described syndrome8 is characterized bymild to moderate increase in body iron stores (2–3 g)and normal transferrin saturation but elevated serumferritin and, frequently, coexisting metabolic distur-bances, such as obesity and diabetes.The C282Y muta-tion for HHC does not seem to be involved and thenature of the disorder has yet to be fully elucidated. It

does not seem to result in the complications associatedwith iron overload due to HHC.
Iron as a cofactor for other diseases
Several other liver diseases have been shown to be exac-erbated by iron, even in relatively small concentrations,as seen, for example, in subjects heterozygous for theC282Y mutation in HHC. These conditions includeporphyria cutanea tarda9,10 and non-alcoholic steato-hepatitis.11 There is also much interest in the possibleinteraction of iron in the progression of liver disease dueto hepatitis B and C viruses but the situation here is stillunclear. For example, some studies have shownimprovement in liver function tests in subjects withHCV-induced chronic hepatitis after phlebotomy, butsuch findings have not been widely reproduced. In addi-tion, there is substantial evidence that alcohol and ironact as cofactors12 and recent studies have indicated thatgross iron overload, comparable to that seen in HHC,may develop in end-stage alcoholic liver disease.13
INFLAMMATORY BOWEL DISEASE:ARE MEDICAL THERAPIES REALLYIMPROVING?†
In 1948, when gastroenterology started as a specialityin Australia, the early mortality for severe attacks ofulcerative colitis was approximately 33%.There was noeffective medical treatment and surgery was generallyregarded as a last resort.The early 1960s saw two majoradvances in treatment. The first was the use of intra-venous hydrocortisone and, the second, early surgeryfor fulminant disease.Two important papers describingthese forms of management were published by the Gas-troenterology Unit at RPAH at this time.14,15 Crohn’sdisease had been described in 1932, but diseaseconfined to the colon was not recognized until 1960. Afurther report outlining Crohn’s colitis was publishedby McGovern and Goulston.16 Since that time, manypapers from members of the Unit describing the patho-genesis, course, epidemiology and complications ofinflammatory bowel disease (IBD) have followed. Themortality of IBD is now similar to that of the generalpopulation and long-term quality of life is, in general,well maintained. However, there are still patients whodo not respond to medical therapy and areas whereimprovements are both required and anticipated.
Conventional treatment for IBD consists of the 5-aminosalicylic acid (ASA) compounds, corticosteroids,immunosuppressants and antibiotics, principallymetronidazole.17 Improvements have been sought ineach of these forms of therapy and are outlined below.
5-Aminosalicylic acid derivatives
The development of mesalazine enemas has been asignificant advance for patients with left-sided ulcera-tive colitis, particularly those with resistant disease not
50 years of gastroenterology in Australia 181
responding to corticosteroids and immunosuppres-sants. Improvement can be seen in more than 80% ofpatients, with remission in the majority. However, treat-ment may need to be continued for several months orlonger to achieve this. More importantly, these enemashave also been shown to be an effective form of main-tenance therapy. In one recent study, a 4 g enema usedtwice a week was associated with a relapse rate at 12months of 39% compared with 69% in controls.18 Thus,mesalazine enemas can be continued in patients withleft-sided disease once remission has been achieved.
The development of delayed-release oral preparationsof mesalazine has led to the use of this agent in Crohn’sdisease. High-dose therapy, 4 g daily, may be of benefitin active disease. However, it is in maintenance ofremission where this agent is most useful. This has been demonstrated in a number of early trials, wheremesalazine has prevented relapse after either medical orpostoperative remission, even up to 2 years. The doseused has varied from 1 to 3.2 g daily. A recent meta-analysis of the 15 studies published to date hasconfirmed that the benefit of oral mesalazine for main-tenance in Crohn’s disease is greater in surgical thanmedical remission, in those with ileal disease and wherethere has been a prolonged disease duration.19
Corticosteroids
Turning to corticosteroids, the disadvantages of theconventional agents, prednisone and prednisolone, hasprompted the development of a controlled ileal release(CIR) formulation of budesonide.This potent, topicallyacting corticosteroid has 90% first-pass hepatic metab-olism and has, in its inhaled formulation, had asignificant impact on the management of asthma.Therehave now been three trials examining its activity inactive ileal or ileocaecal Crohn’s disease. In the multi-centre study involving Australia, there was no differencebetween 9 mg budesonide once daily compared with 40 mg prednisolone, 60% of each group achievingremission.20 There was less adrenal suppression withbudesonide and fewer corticosteroid side effects, in par-ticular moon-face and mood swings. In general, thedrug was well tolerated. When studies were done todetermine whether budesonide could maintain remis-sion, it was found that time to relapse was significantlydelayed, from 39 to 178 days in the study by Greenberget al.21 However, by 1 year, there was no difference inremission rates between patients on budesonide andthose on placebo. Budesonide may be of benefit inselected patients who continually relapse on conven-tional corticosteroids.
Immunosuppressive agents
The benefit of azathioprine in ulcerative colitis has beenwell demonstrated, either for resistant disease, as asteroid-sparing agent or for maintenance of remission.A meta-analysis in Crohn’s disease has also confirmedthe efficacy of azathioprine and its active metabolite, 6-

182 LW Powell et al.
response was seen in all five who were subsequentlygiven cyclosporine. Unfortunately, when the need forcolectomy after this acute treatment was examined,approximately two-thirds of patients had undergonesurgery by 6–12 months. High-dose cyclosporine,5–7.5 mg/kg per day, has also been used in patients withactive Crohn’s disease. Fifty-nine per cent of patientsgiven cyclosporine improved, compared with 32%receiving placebo. However, this response was short-lived. After 6 months of treatment, 81% were no dif-ferent from how they were before treatment, regardlessof whether they received cyclosporine or placebo.Threestudies of low-dose cyclosporine, up to 5 mg/kg per day,in active disease have not been able to show any benefit.Anecdotally, a report of five patients who had a total of12 fistulae showed that in 10 the fistulae closed by 8days and there was reduced drainage in the other two.There was a relapse in five by 10 weeks. No benefit oflow-dose cyclosporin could be demonstrated in main-tenance of remission for up to 18 months.27
When considering the use of cyclosporine, it is essen-tial to keep in mind the significant adverse effects asso-ciated with it. These include nephrotoxicity, infection,neurotoxicity and hepatotoxicity, as well as nausea,vomiting, hypertrichosis and drug interactions. Ofthese, it is the infections that are of greatest concern. Atleast three deaths from pneumocystis have beenreported and we have also had a patient who died fromthis, in combination with cytomegalovirus infection.There has also been a case of a fatal aspergillosis and amycotic aneurysm. Infections are especially likely tooccur in those who have been on high-dose intravenouscorticosteroids, which is common in patients withsevere disease. Prophylaxis for pneumocystis can beconsidered if cyclosporine is to be used. In summary,cyclosporine may have a role in severe ulcerative colitisif surgery is contra-indicated or the patient is not pre-pared. However, it has no role in chronic disease andlittle or no role in Crohn’s disease. A high dose isneeded and, therefore, its safety profile makes its usehazardous. One must consider what the aim of the treat-ment is and whether the risk of cyclosporine outweighsthe risk of surgery.
Methotrexate, at a dose of 25 mg i.m.i. weekly for 16 weeks, is another option for patients with steroid-resistant Crohn’s disease. It was shown to be signifi-cantly better than placebo at inducing remission in 141patients with steroid-resistant Crohn’s disease, althoughonly 38.4% of patients responded. The onset of actionwas within 4 weeks, which is quicker than with aza-thioprine. Seventeen per cent of subjects withdrew fromthe study because of adverse events. However, as withcyclosporine, remission is not maintained bymethotrexate, either at 3, 12 or 18 months. Oralmethotrexate, 12.5 mg/week, is ineffective in activeulcerative colitis and, even in those who respond, isunable to maintain remission.28
Antibiotics
The treatment of Crohn’s disease with antibiotics hasalways seemed attractive because of its suspected infec-
mercaptopurine (6-MP), for the same indications aswell as for closure of fistulae (Fig. 1).22 There are severalproblems associated with these agents. The principalone is the delayed onset of action, approximately 3months. In an attempt to circumvent this problem,Sandborn et al. used an intravenous loading dose of 50mg/h for 36 h, a total of 1800 mg, in patients with activeCrohn’s disease. In six with inflammatory disease, fourhad achieved remission within 4 weeks. Seven of 13fistulae had closed by 4 weeks and all but two hadimproved at 16 weeks. There was no correlation withmetabolite levels and there were no adverse events inthe small number of patients.23
One of the issues relating to treatment with azathio-prine or 6-MP, is how long treatment should be con-tinued once remission has been achieved. A recentFrench study showed that the relapse rate in those whoceased therapy, for a variety of reasons, was greater thanin those who continued the medication. This benefitlasted only until 4 years of therapy, although thenumber of patients still in the study beyond this timewas small.24 Finally, in an attempt to identify patientswho may respond better to azathioprine or 6-MP,Colonna and Korelitz examined the relationshipbetween leucopenia and response to therapy.25 Thenumber who achieved remission, the time to remission,the ability to reduce steroid dose and healing of fistulaewere all greater in patients whose white cell count fellbelow 5000 mm–3. If a patient is not responding, it isworth considering increasing the dose until the whitecell count falls below this level. The concern about anincreased risk of malignancy with long-term use has notbeen confirmed. Connell et al. analysed 755 patientswho had been on treatment for at least 1 year and fol-lowed for 9 years. There was no overall increase incancer risk, other than the expected colorectal cancers.Two cervical cancers were described in women and aregular cervical smear is recommended. There were nolymphomas.26
The treatment of severe attacks of ulcerative colitisremains a difficult problem. Anecdotal reports ofresponse to intravenous cyclosporin led to a small con-trolled trial in 1994. Of 11 patients randomized toreceive cyclosporine, nine responded and only one ofthese required colectomy during the trial. None of ninepatients receiving placebo improved, although a
Figure 1 Meta-analysis of azathioprine/6-mercaptopurinein Crohn’s disease (after Pearson et al.22). (j) Azathioprine,(h) placebo. 1, active disease; 2, fistula closure; 3, steroidsparing; 4, remission maintenance.

tious origin. Metronidazole, or the combination of thisplus ciprofloxacin, is of particular value in perianaldisease. The combination has also been shown, in asmall study, to be as effective as prednisolone in activedisease. However, this is likely to be a non-specific anti-bacterial effect. Metronidazole has recently been shownto be of possible value in preventing post-surgical recur-rence of small bowel Crohn’s disease. After 3 monthstreatment at the high dose of 20 mg/kg per day, endo-scopic recurrence was reduced, particularly in severedisease. Clinical recurrence was reduced at 1 year, butnot at 2 years follow up. A significant proportion ofpatients developed side effects at this high dose, whichlimit its use considerably.29
A particularly contentious issue at present in thetreatment of Crohn’s disease is the role of Mycobac-terium paratuberculosis and the use of antibiotic combi-nations directed against this organism. This atypicalMycobacterium produces a disease in cattle, sheep andgoats called Johne’s disease. This has some similaritiesto Crohn’s disease. Mycobacterium paratuberculosis wasfirst isolated in 1984 from three of 11 patients withCrohn’s disease. It was called Mycobacterium linda, afterthe first patient. Transmission of paratuberculosis toinfant goats was demonstrated by these isolates.Mycobacterium paratuberculosis is found widely in waterand dairy products. Whether this organism plays a rolein the causation of Crohn’s disease is still unclear.Therehave been reports of clustering of disease but this hasnot been confirmed by others. Isolation of the organ-ism occurs in up to 15% of patients with Crohn’sdisease, but some workers have either been unable toisolate it or find a similar frequency of isolation in eithercontrols with ulcerative colitis or normal subjects.Demonstration of M. paratuberculosis DNA in tissuefrom patients with Crohn’s disease has not been uni-versal and anti-M. paratuberculosis antibody responsesare variable. Furthermore, the organism has not beendemonstrated on electron microscopy. Two studies ofantibiotic combinations directed against the organismhave been reported. Rutgeerts et al. gave the combina-tion of rifabutin and ethambutol to 16 patients aftersurgery for 12 months.30 Six withdrew because ofadverse events and in the remaining 10 there was noimprovement.The study that is receiving most attentionat present is that of Gui et al. They used the combina-tion of rifabutin plus clarithromycin in 43 patients andrifabutin plus azithromycin in three patients with resis-tant Crohn’s disease. An additional six patients wereunable to tolerate the medications. The mean durationof therapy was 18.7 months and that of follow up, 25.1months. There was a significant reduction in diseaseactivity, as measured by the Harvey–Bradshaw index,up to 24 months after starting antibiotic therapy. Thisimprovement was seen within 6 months. However, by 2years, only two-thirds of patients remained in remission.Moreover, one-third of patients had required surgery.There was a significant proportion of subjects whodeveloped side effects on the antibiotics, in particular,skin discoloration (in almost 90%), arthralgia (50%),reversible acute uveitis with azithromycin, skin erup-tions, neutropenia and elevated liver function tests.31 Itis too early to determine whether this should become a
50 years of gastroenterology in Australia 183
standard form of therapy for Crohn’s disease and con-trolled clinical trials are needed urgently.
Other therapies
Some interesting forms of therapy have been tried onthe basis of studies into pathogenesis and epidemiology.Perhaps the best example of this has been transdermalnicotine for active ulcerative colitis. This was usedbecause of the well-documented finding that ulcerativecolitis is significantly more common in ex-smokers thancurrent smokers. Forty-nine per cent of patients withmild to moderate disease improved with nicotinepatches compared with 24% of controls. However,three-quarters of the patients on active treatment devel-oped side effects.32 This benefit does not extend tomaintenance of remission. Side effects limit its wide-spread use.
A controlled release formulation of omega-3 fattyacids has been reported to prolong remission in Crohn’sdisease. Topical lidocaine, short-chain fatty acids orbismuth may be effective in active distal ulcerativecolitis. Recent reports of the use of heparin are also ofinterest and further studies are awaited. Interferon hasnot proven to be of benefit. A preliminary study of pan-tothenic acid, a precursor of coenzyme A, is of interest.These forms of therapy may be of value in a limitednumber of patients but do not represent a quantum leapin management.
Cytokine-directed therapy
As our understanding of pathogenesis has expanded,the identification of a number of important inflamma-tory mediators has led to trials of selective immuno-suppression. These include anti-tumour necrosis factora (TNFa), interleukin (IL)-1 receptor antagonist, IL-10, anti-IL-2 receptor and anti-CD4. Most promisingis anti-TNFa for active Crohn’s disease. In the firstcontrolled trial, a 60 min infusion resulted in asignificant improvement by 2 weeks, compared withplacebo.33 In the second, a 2 h infusion of three differ-ent doses was also more effective than placebo asassessed at 4 weeks. More than 50% of patientsachieved remission by this time (Fig. 2). However, thiswas not maintained after the single dose.34 An openstudy of daily bolus injections of IL-10 for 1 week in 46patients with resistant Crohn’s disease induced remis-sion in 50%.35
In conclusion, medical therapies are improving, butthere are undoubtedly significant advances required.The new forms of therapy using anti-inflammatorycytokines or antibodies to pro-inflammatory mediators,while preliminary, offer great promise, particularly ininducing a response in patients with resistant disease.The challenge will remain to then maintain remission.It is worth bearing in mind the significant associationbetween smoking and Crohn’s disease. Smokers aremore likely to relapse, require surgery and spend moretime in hospital. It has been suggested that stopping

184 LW Powell et al.
Figure 3 Indication for liver transplantation in Australians (n = 758 patients37).
smoking in these patients may be as effective as anyform of medical therapy we can give. We should alsoremember that surgery does not have to be the lastresort and that significant improvement in quality of lifeoccurs after surgery both in ulcerative colitis and inCrohn’s disease.
LIVER TRANSPLANTATION:INDICATIONS AND OUTCOMES‡
In many countries, liver transplantation is now part ofroutine assessment and therapy for patients with severe,acute and chronic liver disease. There are more than300 liver transplant units throughout the world whichhave performed liver transplantation in more than
50 000 patients.36 In the Australian context, there arefive units with more than 1000 patients receiving livertransplants over the last decade.37
General indications for transplant
Although criteria vary from disease to disease, it is gen-erally accepted that patients with Child’s B cirrhosis oracute liver failure, unresponsive to medical therapies,are candidates for liver transplantation. These patientsshould not have significant extrahepatic disease, unlesspotentially reversible by liver transplantation itself, andthere should be no persistent extrahepatic infection.Furthermore, continued or recent alcohol and drugabuse usually excludes patients from most transplantprogrammes.
Disease-specific indications and outcomes
The disease-specific indications for transplantation inthe Australian community are seen in Fig. 3. Such datareflect disease causation accumulated over the lastdecade and are similar in spectrum to transplant pro-grammes in the USA and Europe.36 However, in the last5 year period, there has been an increasing number ofpatients transplanted for hepatitis C, alcoholic andhepatitis B virus (HBV)-related cirrhosis, which is notevident from figures dating back to 1986.
Autoimmune hepatitis
Severe autoimmune hepatitis (AIH) is usually initiallycontrolled by immunosuppressive therapy, but progres-sion to cirrhosis is common.Transplantation in patients
Figure 2 Effect of a 2 h intravenous infusion of cA2 anti-body to tumour necrosis factor in active Crohn’s disease(adapted from Targan et al.34). Percentage clinical response at4 weeks (Crohn’s disease activity index fall > 70). Fifty-four of83 treated patients were in remission while four or 24 placebo-treated patients were also in remission.
50 years of gastroenterology in Australia 185
with this disease, which usually persists for decades,is indicated once hepatic decompensation (ascites,encephalopathy, muscle wasting, malnutrition, increas-ing jaundice) starts to occur. Occasionally, AIH canpresent for the first time as an acute or subacute hepaticfailure syndrome which may respond to immunosup-pressive therapy. Outcomes post-transplant are gener-ally very good for this disease. The issue of recurrentautoimmune hepatitis post-transplant is controversial.38
It has been suggested that withdrawal of prednisonefrom the immunosuppressive regimen may predisposepatients to recurrence and is not recommended inpatients undergoing transplantation for AIH.38
Primary biliary cirrhosis
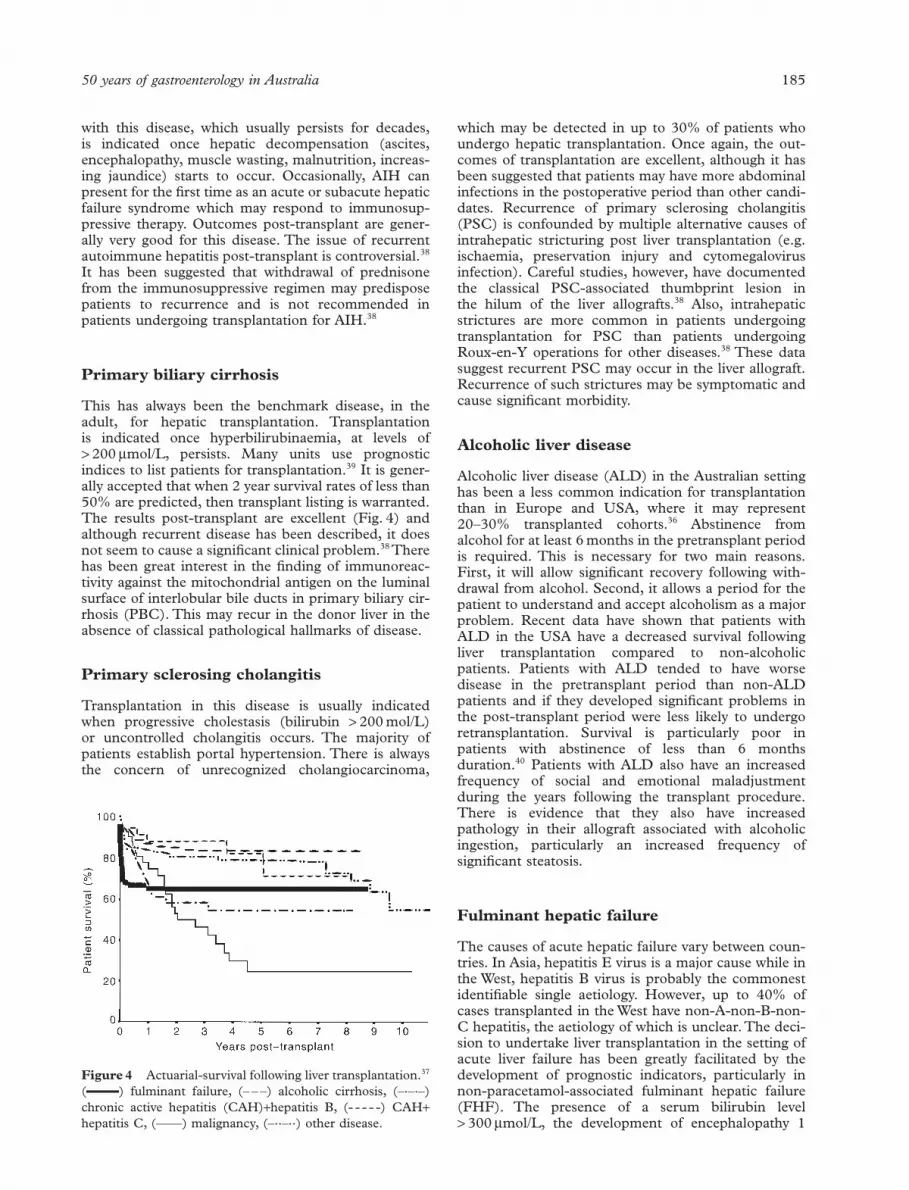
This has always been the benchmark disease, in theadult, for hepatic transplantation. Transplantation is indicated once hyperbilirubinaemia, at levels of > 200 mmol/L, persists. Many units use prognosticindices to list patients for transplantation.39 It is gener-ally accepted that when 2 year survival rates of less than50% are predicted, then transplant listing is warranted.The results post-transplant are excellent (Fig. 4) andalthough recurrent disease has been described, it doesnot seem to cause a significant clinical problem.38 Therehas been great interest in the finding of immunoreac-tivity against the mitochondrial antigen on the luminalsurface of interlobular bile ducts in primary biliary cir-rhosis (PBC). This may recur in the donor liver in theabsence of classical pathological hallmarks of disease.
Primary sclerosing cholangitis
Transplantation in this disease is usually indicated when progressive cholestasis (bilirubin > 200 mol/L) or uncontrolled cholangitis occurs. The majority ofpatients establish portal hypertension. There is alwaysthe concern of unrecognized cholangiocarcinoma,
which may be detected in up to 30% of patients whoundergo hepatic transplantation. Once again, the out-comes of transplantation are excellent, although it hasbeen suggested that patients may have more abdominalinfections in the postoperative period than other candi-dates. Recurrence of primary sclerosing cholangitis(PSC) is confounded by multiple alternative causes ofintrahepatic stricturing post liver transplantation (e.g.ischaemia, preservation injury and cytomegalovirusinfection). Careful studies, however, have documentedthe classical PSC-associated thumbprint lesion in the hilum of the liver allografts.38 Also, intrahepaticstrictures are more common in patients undergoingtransplantation for PSC than patients undergoingRoux-en-Y operations for other diseases.38 These datasuggest recurrent PSC may occur in the liver allograft.Recurrence of such strictures may be symptomatic andcause significant morbidity.
Alcoholic liver disease
Alcoholic liver disease (ALD) in the Australian settinghas been a less common indication for transplantationthan in Europe and USA, where it may represent20–30% transplanted cohorts.36 Abstinence fromalcohol for at least 6 months in the pretransplant periodis required. This is necessary for two main reasons.First, it will allow significant recovery following with-drawal from alcohol. Second, it allows a period for thepatient to understand and accept alcoholism as a majorproblem. Recent data have shown that patients withALD in the USA have a decreased survival followingliver transplantation compared to non-alcoholicpatients. Patients with ALD tended to have worsedisease in the pretransplant period than non-ALDpatients and if they developed significant problems inthe post-transplant period were less likely to undergoretransplantation. Survival is particularly poor inpatients with abstinence of less than 6 months duration.40 Patients with ALD also have an increasedfrequency of social and emotional maladjustmentduring the years following the transplant procedure.There is evidence that they also have increased pathology in their allograft associated with alcoholicingestion, particularly an increased frequency ofsignificant steatosis.
Fulminant hepatic failure
The causes of acute hepatic failure vary between coun-tries. In Asia, hepatitis E virus is a major cause while inthe West, hepatitis B virus is probably the commonestidentifiable single aetiology. However, up to 40% ofcases transplanted in the West have non-A-non-B-non-C hepatitis, the aetiology of which is unclear.The deci-sion to undertake liver transplantation in the setting ofacute liver failure has been greatly facilitated by thedevelopment of prognostic indicators, particularly innon-paracetamol-associated fulminant hepatic failure(FHF). The presence of a serum bilirubin level > 300 mmol/L, the development of encephalopathy 1
Figure 4 Actuarial-survival following liver transplantation.37
(–––––) fulminant failure, (– – –) alcoholic cirrhosis, (–·–·–)chronic active hepatitis (CAH)+hepatitis B, (- - - - -) CAH+hepatitis C, (——) malignancy, (–··–··) other disease.

week after the onset of jaundice, non-A-non-B-non-Cor drug aetiology and age < 10 years or > 40 years aremajor predictors of death.41 Indeed, patients with threeor more of the above five criteria are generally listed fortransplantation. Outcomes for transplantation for FHFare generally worse than for other diseases with manycentres reporting only 60% 1 year survival. The vastmajority of the deaths occur in the first month posttransplantation. Fungal and bacterial sepsis and cere-bral catastrophes are the major causes of death.Bioartificial liver assist devices are now being exploredas a bridge to hepatic transplantation. Survival inpatients who make it through the first postoperativemonth are excellent. Recurrent disease is very uncom-mon.
Hepatitis B virus infection
It has been recognized that outcomes for hepatic trans-plantation over the last decade in patients with HBVinfection have been significantly worse than non-HBVpatients. However, immunoprophylaxis with large dosesof hepatitis B immunoglobulin and the new antiviralagents (particularly lamivudine) that prevent HBVrecurrence have recently improved outcomes.42,43
Hepatitis B virus recurrence is increased in patients whoare HBV-DNA positive and/or hepatitis B virus earlyantigen positive pretransplant and decreased in patientswith hepatitis D virus coinfection. Severe recurrence of HBV post transplant may be associated with a progressive form of disease known as fibrosing cholesta-tic hepatitis. There is conflicting data in the literaturewhether patients with precore mutant HBV have anincreased incidence of graft loss due to this conditionin the post-transplant period.44,45 Studies performed by our group have found an association in the Australian setting, but this has not been confirmed by a recent study from Germany. Once recurrent HBV disease does occur, the use of antiviral agents,particularly lamivudine, to decrease HBV-DNA levelsand slow progression of disease is now routine.However, there are problems with emerging resistanceto lamivudine, which occurs in 20–30% of cases in a pretransplant non-immunosuppressed setting,but may be higher once lamivudine is continued beyondthe 6 month period in immunosuppressed patients(possibly up 60%). Currently, prophylactic approaches,such as the use of lamivudine in conjunction withhepatitis B immunoglobulin (high or low) dose areresulting in a < 20% HBV recurrence and, conse-quently, outcomes for HBV-related disease are nowexcellent.
Hepatitis C virus infection
In many units around the world, including many Aus-tralian units, hepatitis C virus (HCV)-associated cir-rhosis is now the commonest single indication fortransplantation in the adult community.36 Recurrenceof HCV is universal post transplant, but unlike HBV
186 LW Powell et al.
infection, generally does not lead to severe forms ofhepatitis and early graft loss. However, such a picturemay occur in approximately 10% of patients, usuallyassociated with a cholestatic hepatitis and high levels ofHCV virus.46 At present, therapies for recurrent HCVpost transplant are unclear, but preliminary studies withribavirin and interferon, given at an early stage of recur-rence, have suggested that long-term control of thedisease may be obtainable.47 Such studies need to beconfirmed and properly randomized controlled trialsare required. Survival from HCV recurrent diseaseseems excellent, with little evidence of progressive graftloss over a 5 year period. However, some authors haveindicated that genotype 1b HCV reinfection may leadto a more progressive disease and it is feared that pro-gressive graft loss may occur in the 5–10 years periodpost transplant compared with non-HCV-relateddisease.48
Primary hepatocellular cancer
Although there was initial enthusiasm for liver trans-plantation for this disorder, it was increasingly recog-nized that indiscriminate use of transplantation led topoor patient outcomes. However, recent data indicatethat transplantation of hepatic tumours, under strict cri-teria, can lead to favourable outcomes. In one study, thefulfilment of pretransplant predictors (single tumour <5 cm, no more than three tumours all < 3 cm in diam-eter, no extrahepatic spread) resulted in 3 year survivalrates between 70 and 80%.49 We now accept patients fortransplantation who fit these criteria and the outcomesare excellent. Recurrence rates, however, remain highfor cholangiocarcinoma and transplant is not usuallyindicated for this condition. Other unusual tumours,such as haemangioepitheliomas, fibrolamellar hepato-cellular cancer and hepatoblastoma in children, may beindications for transplantation.
Paediatric transplantation
The commonest indication in the paediatric populationremains biliary atresia. Paediatric transplantation hasbeen revolutionized by the use of reduced donor livers.Some centres, particularly in Asia, have introducedliving related transplantation and, increasingly, ‘splitliver transplantation’ is undertaken, where a single adultliver is split in two with the left lateral segments beingused for a paediatric recipient while the remaining liveris transplanted into an adult.50,51 In some centres thishas led to a dramatic decrease in the waiting times forpaediatric recipients which previously have often beengreater than 12 months.
Metabolic or genetic liver disease are also importantindicators for transplantation in both the paediatric andadult populations.The use of transplantation to correctgenetic diseases that result in non-hepatic disease (e.g.oxalosis, hypercholesterolaemia, amyloid polyneur-opathy) remain uncommon, but well defined, reasonsfor transplantation.

Current immunosuppressive therapies
A combination of prednisone, azathioprine andcyclosporine is still used as the cornerstone forimmunosuppression. Cyclosporine is now available in amicro-emulsion form (neoral) which improves overallbio-availability. Increasingly, however, many units havereplaced cyclosporine with tacrolimus hydrate (FK506)as the primary preventive therapy. Acute rejection isusually treated by pulse corticosteroid therapy. Corti-costeroid-resistant rejection is treated with eitherOKT3 or a switch from cyclosporine to FK506. Bothapproaches are successful in > 80% of cases. Chronicliver allograft rejection occurs in < 10% of recipients.
Long-term outcomes
Although the 2 years survival from liver transplantationis generally in the vicinity of 80%, patients requirecareful long-term medical surveillance and care.52 Upto 30% of patients may have stable renal insufficiencywith serum creatinine levels > 150 mol/L. In our expe-rience, at a mean of 7 years post transplant, 30% ofpatients are on anti-hypertensive medication and 30%have skin cancers. Later cardiovascular deaths between5 and 15 years post transplant are also being increas-ingly recognized. Long-term allograft dysfunction sec-ondary to HBV/HCV and biliary strictures may be asource of significant morbidity. Despite these problems,liver transplant results in the return to employment inthe majority of patients and significant improvementsin pretransplant quality of life.
INFLAMMATORY MEDIATORS ININFLAMMATORY BOWEL DISEASE§
Inflammatory bowel disease (IBD) comprises two dis-tinct clinical entities, ulcerative colitis and Crohn’sdisease. Ulcerative colitis affects the colon exclusively;its histopathological features include epithelial ulcera-tion, loss of mucin-containing goblet cells, micro-abscess formation and a dense inflammatory infiltratein the lamina propria, comprising neutrophils, mono-cytes/macrophages, lymphocytes and plasma cells. InCrohn’s disease, inflammation can occur anywhere inthe gastrointestinal tract, although the terminal ileumand proximal colon predominate and the lesions are dis-continuous and transmural. The chronic infiltrate characteristically consists of lymphocytes and mono-cytes/macrophages and the prototypic histologicalfeature is the granuloma, found in at least 50% ofpatients. Development of scar tissue leading to strictureformation is a common and clinically debilitating result.
Inflammatory bowel disease is a complex problemand elucidation of its pathogenesis is necessary forseveral reasons.The peak age of onset is during the ageof 20–30, the diseases are chronic and are characterizedby remissions and exacerbations, the aetiology isunknown and the non-specific anti-inflammatory treat-ment used in the 1990s is fundamentally unchanged
50 years of gastroenterology in Australia 187
from that used in the 1970s. Nevertheless, significantadvances in understanding its pathogenesis have beenmade in the last 10 years and these are now starting toprovide more rational, targeted therapies.
This review will present some of the informationlearnt about the contribution of individual cell types tothe inflammatory milieu in IBD and about the role ofintercellular mediators, such as cytokines, in perpetuat-ing the tissue destruction seen in these diseases.
Cell types in inflammatory bowel disease
NeutrophilsThere is a profound and striking increase in neutrophilturnover in patients suffering from active intestinalinflammation. Neutrophils form a major part of the leu-cocyte infiltrate in IBD mucosa and they are associatedwith extensive mucosal injury, suggesting their role inmediating tissue damage in IBD. Neutrophils exert theirtissue destructive potential through two major means:oxidative mechanisms and non-oxidative, principallyprotease-mediated, mechanisms. Oxidative damage oc-curs through NADPH oxidase-generated superoxide(O2
–) and hydrogen peroxide (H2O2), which interactwith the haemoprotein myeloperoxidase to generate the highly potent oxidizing agent hypochlorous acid(HOCl). Recent evidence has shown that these agentsare capable of inducing metabolic derangements inintestinal epithelial cells.53
Neutrophils release a cascade of more than 40 dif-ferent proteolytic enzymes, although the major poten-tial for degradation appears to arise from the release ofelastase, collagenase and gelatinase. Natural inhibitorsof these proteases, such as a1-proteinase inhibitor, arethemselves inactivated by oxidative damage, creating acycle of tissue destruction.
Monocytes/macrophagesThere is evidence of increased recruitment of mono-cytes to the inflamed intestine in active IBD54 and thesenewly recruited cells are susceptible to the phlogisticinfluence of the Gram-negative bacterial cell wallproduct, lipopolysaccharide (LPS) through theirexpression of the LPS receptor, CD14, not usuallypresent on intestinal macrophages.55 Macrophage func-tions are protean and range from regulation of immuneand inflammatory responses and phagocytosis ofingested organisms and foreign antigens, to productionof a vast array of oxygen free radicals, lipid mediators,lysosomal enzymes, proteases and cytokines.
LymphocytesWhile total lymphocyte numbers are increased in IBD-affected mucosa, the relative proportions of B cells,CD4+ and CD8+ T cells, are unchanged.56 Markers ofactivation, such as transferrin receptor and IL-2 recep-tor, are more prominent on lamina propria and periph-eral blood T and B cells in IBD patients.The functionalcorrelates of these phenotypic observations remain

188 LW Powell et al.
unclear; a number of studies show disparate results inlymphocyte activities as diverse as antibody generation,cytotoxicity, adhesion to endothelial cells and cytokineproduction.
Epithelial cellsThe literature on epithelial cells in IBD has concen-trated on two major areas: epithelial cell antigen pre-sentation and production of cytokines by epithelialcells. While small intestinal epithelium normallyexpresses major histocompatibility complex (MHC)class II molecules (to present luminal food antigens tounderlying lymphocytes?), uninflamed colonic epithe-lium does not. In IBD, however, there is heightenedexpression of MHC class II on epithelial cells, probablyinduced by interferon (IFN) g. In vitro experimentssuggest that class II-expressing epithelial cells processand present soluble antigen to T cells resulting in theproliferation of antigen-non-specific CD8+ suppressorcells.57 Whether or not this plays a role in vivo in IBDis unclear.
There has been a plethora of recent publicationsproposing that epithelial cells are potent producers ofpro-inflammatory cytokines in IBD. These mediatorsrange from IL-1b to IL-6, TNFa and chemotactic
cytokines or chemokines. Many of these studies rely ontransformed epithelial cell lines or isolated colonicepithelial cells potentially contaminated with laminapropria leucocytes. Even where such contamination iscontrolled, the potential for generation of artefacts inthe isolation procedure persists. In circumstances whereepithelium is examined as part of intact mucosa, suchas by in situ hybridization,58–60 the evidence for epithe-lial cell production of most cytokines is lacking.
Cytokines in inflammatory bowel disease
In the absence of defined aetiologies for either of theIBD, many mediators have been explored and their con-tribution to the pathogenesis of IBD postulated. Thelargest group of such mediators is the cytokines, whichfor the purpose of this review are divided into pro-inflammatory, regulatory and chemokine groupings(Table 1). Significant insights into IBD pathogenesishave been contributed by the description of gene-targeted knockout mice, including those with absentregulatory cytokines including IL-2 and IL-10, thathave been shown to develop florid intestinal in-flammation; these models and their relevance to thehuman diseases are an area of intense interest.
Table 1 Cytokines in Inflammatory Bowel disease (IBD)
Pattern of expression or activityCytokine Crohn’s disease Ulcerative colitis Inactive IBD Cells responsible for production
Pro-inflammatoryIL-1b ++ ++ + (?) Monos/MfIL-1ra + + + Monos/MfTNFa +++ ++ – Monos/MfIL-6 ++ ++ – Monos/Mf, ?endothelial cells
RegulatoryTh1 IL-2 ± – + T lymphocytes
IFNg ± – – T lymphocytesIL-12 + – – Mf
Th2 IL-4 Reduced activity Reduced activity Normal CD4+ T lymphocytesIL-10 Normal activity Normal activity Normal CD4+ T lymphocytesIL-13 Reduced activity Reduced activity Normal CD4+ T lymphocytes
Th3 TGFb + ++ – ?
Chemokinesa IL-8 +++ +++ – Monos/Mf, neutrophils
ENA-78 ++ ++ – Epithelial cellsIP-10 ++ + – Monos/Mf, lymphocytes, endothelial cells
b MCP-1 ++ ++ – Monos/Mf, smooth muscle cells, endothelial cellsMIP-1a ++ ++ – Monos/Mf, lymphocytes, endothelial cellsMIP-1b + + – Monos/Mf, lymphocytesRANTES ++ ++ + Monos/Mf, lymphocytes, endothelial cells
IL, interleukin; IL-1ra, interleukin-1 receptor antagonist; TNFa, tumour necrosis factor a; IFNg, interferon g; Th1, T helper1 cell;Th2,T helper 2 cell; ENA-78, epithelial neutrophil attractant-78; IP-10, g-interferon-inducible protein-10; MCP-1, mono-cyte chemoattractant protein-1; MIP-1a, macrophage inflammatory protein-1; RANTES, regulated on activation, normal Texpressed and secreted; monos, monocytes; Mf, macrophages.

50 years of gastroenterology in Australia 189
subtype, and B cells, and it has pleiotropic effects onmany cell types. One of its major effects is to stimulatehepatocytes to produce acute phase proteins; thus, ithas been looked for in the serum in most chronicinflammatory conditions. A number of studies havedemonstrated heightened serum and mucosal tissuelevels of IL-6 in IBD and these levels have been corre-lated with the acute phase response. The controversywith IL-6, however, lies not in its presence or absencein IBD, but in the meaning of its expression. While ithas long been considered a pro-inflammatory cytokine,at least partly in the mould of IL-1 and TNF, recentevidence suggests that it is responsible for significantanti-inflammatory activity, for example, by inducingproduction of IL-1ra and soluble TNF receptors, bothof which act to mop up their pro-inflammatory coun-terparts.The presence of IL-6 in this anti-inflammatoryguise is yet to be re-interpreted in IBD.
Regulatory cytokines
The encounter of a host with antigen has been knownfor many years to result in polarized immune responses:either in cell-mediated immunity or in humoral immun-ity. During the 1980s, this was shown in the murinesystem to be due to heterogeneity of CD4+ T cells,which could be divided into two subsets depending ontheir predominant cytokine secretion profile. T helper 1 cells produce IL-2, interferon (IFN) g and TNFb(lymphotoxin) and are responsible for promotingdelayed-type hypersensitivity responses associated withcell-mediated immunity, while Th2 cells produce IL-4,IL-5 and IL-10, thus directing humoral immuneresponses and activation of mast cells and eosinophils.In their most characteristic forms, Crohn’s disease andulcerative colitis fit the opposing ends of this paradigm,Th1 and Th2, respectively, and to some degree this hasbeen borne out experimentally.
T helper 1 cell cytokinesInterleukin-2 is one of the first cytokines to have beenstudied in IBD, yet its role is one of the least clear.Several groups have shown reduced IL-2 production byisolated lamina propria mononuclear cells from IBD-affected tissues, while others have suggested that this isaccompanied by increased expression of IL-2 receptorsand heightened sensitivity to IL-2 stimulation. Morerecently, several groups have demonstrated results inCrohn’s disease consistent with the cell-mediatedimmunity model, showing that IL-2 mRNA and proteinare present at higher levels in active Crohn’s diseasethan in normal tissue, inactive Crohn’s disease or ulcer-ative colitis. The paradigm is further supported byreports of symptomatic exacerbation of quiescentCrohn’s disease by high-dose IL-2 used for coexistingmalignant disease, as well as by the presence of aninflammatory colitis mimicking ulcerative colitis in micegenetically deficient in IL-2.
Interferon g has a similarly vexed history, with differ-ent groups coming to different conclusions about its
Pro-inflammatory cytokines
Interleukin-1bInterleukin-1 is a cytokine that is produced in and actson virtually all tissues in the body, producing a vastarray of effects such as T and B cell activation, induc-tion of other pro-inflammatory cytokine and proteasegenes, release of eicosanoid products from inflamma-tory cells and systemic effects, such as induction offever, suppression of cardiac function and productionof peripheral blood neutrophilia. Many investigatorshave found evidence of heightened production of IL-1b, in both serum and in inflamed intestinal tissuesfrom IBD patients and at least one group has found thatelevated tissue levels of IL-1b are present during com-plete remission from ulcerative colitis,61 suggesting afundamental defect in IL-1 regulation in these patients.Interleukin-1 in IBD-affected mucosa seems to be gen-erated overwhelmingly by macrophages.
Interleukin-1 receptor antagonistInterleukin-1 receptor antagonist (IL-1ra) is a naturallyoccurring inhibitor of the actions of IL-1. It is usuallyproduced soon after IL-1 and acts as a brake on theintense pro-inflammatory actions of IL-1. In IBD,however, it has been shown that the balance of IL-1 to its antagonist is tilted markedly in favour of IL-1, thereby promoting continuing inflammation.Cominelli’s group has suggested that this is specific forIBD, as similar imbalance is not observed in non-IBDintestinal inflammation.62 This led to analysis of geneticpolymorphisms in IL-1ra, with geographical variabilityin linkage between certain polymorphisms and theoccurrence of IBD. In the absence of reproducibleobservations, it is difficult to determine how importantthe variations in the IL-1ra gene are in the pathogene-sis of IBD.
Tumour necrosis factor aUntil the successful use of anti-TNFa antibodies inCrohn’s disease, evidence for a role for TNFa in IBDhad not been as clear-cut as it was for IL-1. Althoughit shares many of the immune-activating and systemicproperties of IL-1, it has proven more elusive to detectin IBD, particularly in serum during active disease.Tissue levels, though, are elevated, as detected byenzyme-linked immunosorbent assay of tissue homo-genates, analysis of mRNA from tissue, in situ hybridiza-tion and immunohistochemistry.
The clear evidence for a pathogenic role of TNFa inIBD comes from the successful use of humanized anti-TNFa antibodies to ameliorate moderately severeinflammation in patients with Crohn’s disease.63 Thisand similar studies are exciting because they show that,despite the vast array of inflammatory mediators thatcan be implicated in IBD pathogenesis, there are cen-trally important cytokines among them.
Interleukin-6Interleukin-6 is a product of activated monocytes/macrophages,T cells, particularly of the T helper (Th)2

presence in IBD tissues. It seems likely that whenpresent, it is responsible for the abnormal expression of MHC class II molecules on colonic epithelial cellsseen in active disease (vide supra). Both IFNg and oneof its inducers, IL-12, have recently been shown to be present in Crohn’s disease tissues,64 once againconfirming the Th1 nature of the inflammation in thisdisease.
T helper 2 cell cytokines The Th2 cytokines (IL-4, IL-5, IL-10, IL-13) have beendifficult to demonstrate in intestinal tissues, presumablybecause they are present in extremely low concentra-tions or their mRNA is rapidly modulated. Althoughthere are preliminary reports of elevated IL-10 mRNAlevels in ulcerative colitis but not in Crohn’s disease,supporting the notion of ulcerative colitis as a Th2-mediated disease, others have not been able to confirmthese findings. Of major importance is the finding thatmice genetically deficient in IL-10 develop a chronicenterocolitis somewhat similar to human Crohn’sdisease, although development of disease requires thepresence of the intestinal microflora. Schrieber et al.have shown that responsiveness of lamina propriamacrophages to IL-4 and IL-10 are diminished andconserved, respectively, in IBD.65,66 In the absence ofreadily detectable differences in tissue levels of themediators, it seems prudent to look at this next link inthe chain: receptor levels and responsiveness. Indeed,this approach has been used by one group to suggest areduced anti-inflammatory capacity for IL-13 in IBDtissues.67
Chemokines in inflammatory bowel disease
Chemokines are a burgeoning family of chemoattrac-tant cytokines that induce migration and activation in arange of leucocyte and other, less well-characterized,cell types.They are divided into two major subfamilies,depending on the presence (a or CXC family), orabsence (b or CC family) of an intervening amino acidbetween the first two of a conserved motif of four cys-teines. These structural differences are accompanied by differences in cell-type specificity: a chemokines predominantly attract and activate neutrophils,while b chemokines act on monocytes, lymphocytes,eosinophils, basophils, natural killer and dendritic cells. Two additional subfamilies, each with a solit-ary member (so far) have been described: g or Cchemokines (lymphotactin) and CX3C chemokines(fractalkine or neurotactin).68 The wide range of expres-sion of chemokines, the variety of cellular targets, over-lapping receptor specificities and rapidly enlargingnumber (> 45 at last count) suggest extreme redun-dancy of function, but there are surprising indicationsin some diseases of specific activity, which argues forthe potential utility of targeting individual chemokinestherapeutically. Moreover, several chemokine-like mol-ecules and chemokine receptors are encoded in thegenomes or are targeted by a number of pathogens,
190 LW Powell et al.
including cytomegalovirus and other herpes viruses,Plasmodium vivax and human immunodeficiencyviruses (HIV), suggesting that a natural selective advan-tage can be obtained by blocking or mimicking singlechemokines.
As chemokines are responsible for the attraction andactivation of leucocytes, it is hardly surprising that manyof them have been found in large quantities in chronicinflammatory diseases.The best studied of these in IBDis the a chemokine, IL-8, which is abundant in regionsof acute inflammation, particularly associated with neu-trophils. It is generated by recently recruited CD14+
monocytes and by neutrophils themselves,58 implicatingit in a cycle of neutrophil attraction and activation. Asecond a chemokine, interferon-inducible protein-10,which lacks activity for neutrophils but attracts mono-cytes and lymphocytes, has been demonstrated in chronic inflammation in both Crohn’s disease and ulcerative colitis, including Crohn’s granulomas60
(Fig. 5). Unequivocal demonstration of production of achemokine by epithelial cells in IBD has only beenforthcoming for the a chemokine, epithelial neutrophilattractant-78.69
Of the b chemokines, there is evidence for produc-tion of a number of these mononuclear cell chemoat-tractants, including monocyte chemoattractant protein-1, macrophage inflammatory protein (MIP)-1a (Fig. 6)and MIP-1b, and Regulated on Activation, Normal TExpressed and Secreted (RANTES). Once again, theyseem to be produced predominantly by recentlyrecruited monocytes, but also by lymphocytes andendothelial cells.59,60
While it is important to determine the expression pat-terns of chemokines in IBD, a more complete under-standing of their contribution to the inflammatoryprocess will only be achieved with knowledge of expres-sion of their receptors, the signalling pathways activatedby chemokine receptors and the factors that regulatethe responsiveness of those receptors. These variablesare complex and ill-understood but are important areasof current research, especially since the discovery ofchemokine receptors as coreceptors along with CD4 for
Figure 5 In situ hybridization using [35S]-labelled antisenseriboprobe for interferon-inducible protein (IP)-10, showingexpression of IP-10 mRNA in macrophages and T cells of aloosely formed granuloma in Crohn’s disease.

50 years of gastroenterology in Australia 191
hereditary haemochromatosis. Nat. Genet. 1996; 13:399–408.
5 Feder JN, Penny DM, Irrinki A et al. The hemochro-matosis gene product complexes with the transferrinreceptor and lowers its affinity for ligand binding. Proc.Natl Acad. Sci. USA 1998; 95: 1472–7.
6 Jawinska EC, Cullen LM, Busfield F et al. Haemochro-matosis and HLA-H. Nat. Genet. 1996; 14: 249–51.
7 Mukhopadhyay CK, Attieh ZK, Fox PL. Role of ceruloplasmin in cellular iron uptake. Science 1998; 279:714–17.
8 Moirand R, Mortaji AM, Loreal O, Paillard F, Brissot P.A new syndrome of liver iron overload with normal trans-ferrin saturation. Lancet 1997; 349: 95–7.
9 Stuart KA, Busfield F, Jazwinska EC et al. The C282Ymutation in haemochromatosis (HFE) gene and hepatitisC virus infection are independent cofactors for porphyriacutanea tarda in Australian patients. J. Hepatol. 1998; 28:404–9.
10 Roberts G, Whatley SD, Morgan RR, Worwood M, ElderGH. Increased frequency of the haemochromatosisCys282Tyr mutation in sporadic porphyria cutanea tarda.Lancet 1997; 349: 321–3.
11 George DK, Goldwurm S, Macdonald GA et al. Increasedhepatic iron stores in non alcoholic steatohepatitis areassociated with the hemochromatosis mutation andincreased liver damage. Gastroenterology 1998; 114:311–18.
12 Powell LW, Jazwinska EC, Halliday JW. Primary iron over-load. In: Brock JH, Halliday JW, Pippard MJ, Powell LW,eds. Iron Metabolism in Health and Disease. London: WBSaunders, 1994; 227–70.
13 Ludwig J, Hashimoto E, Porayko MK et al. Hemosidero-sis in cirrhosis. A study of 447 native livers. Gastroenterol-ogy 1997; 112: 882–8.
14 Gallagher ND, Goulston SJM, Wyndham N, Morrow W.The management of fulminant ulcerative colitis. Gut1962; 3: 306–11.
15 Rankin JG, Goulston SJM, Boden RW, Morrow W. Ful-minant ulcerative colitis. Q. J. Med. 1960; 29: 375–89.
16 McGovern VJ, Goulston SJM. Crohn’s disease of thecolon. Gut 1968; 9: 164–76.
17 Selby WS. Current medical management of InflammatoryBowel disease. J. Gastroenterol. Hepatol. 1993; 8: 70–83.
18 d’Albasio G, Pacini F, Camarri E et al. Combined therapywith 5-aminosalicylic acid tablets and enemas for main-taining remission in ulcerative colitis: A randomizeddouble-blind study. Am.J.Gastroenterol. 1997; 92: 1143–7.
19 Camma C, Giunta M, Rosselli M, Cottone M.Mesalamine in the maintenance treatment of Crohn’sdisease: A meta-analysis adjusted for confounding vari-ables. Gastroenterology 1997; 113: 1465–73.
20 Campieri M, Ferguson A, Doe W et al. Oral budesonideis as effective as oral prednisolone in active Crohn’sdisease. Gut 1997; 41: 209–14.
21 Greenberg GR, Feagen BG, Martin CN et al. Oral budes-onide as maintenance treatment for Crohn’s disease:A placebo-controlled, dose ranging study. CanadianInflammatory Bowel Disease Study Group. Gastroenterol-ogy 1996; 110: 45–51.
22 Pearson DC, May GR, Fick GH, Sutherland LR. Aza-thioprine and 6-mercaptopurine in Crohn’s disease. Ameta-analysis. Ann. Intern. Med. 1995; 122: 132–42.
HIV cell entry and the enormous impetus that thatfinding has generated for the development ofchemokine receptor antagonists.
Inflammatory mediators in IBD:Where to now?
Inflammatory mediators in chronic IBD are two-edgedswords. Clearly, they are required for protection of thehost from its environment, but it is equally obvious thatthey cause major morbidity when present in an abun-dant, dysregulated fashion. The presence of intestinalinflammation in IL-2 and IL-10 knockout mice and thesuccess of anti-TNF therapy in Crohn’s disease high-light this dichotomy. Greater awareness will come withthe demonstration of the full hierarchy of cytokines andbetter understanding still will come with the analysis oftheir receptors and activities in IBD tissues. Ultimately,the use of specific anti-cytokine therapies in animalmodels of IBD and in other chronic inflammatory dis-eases, will direct us towards likely candidates for tar-geted, biologically sound therapies in human IBD.Finding the inflammatory mediators in disease, then, isonly the beginning.
REFERENCES
1 Bassett ML, Halliday JW, Powell LW. Value of hepatic iron measurements in early hemochromatosis and deter-mination of the critical iron level associated with fibrosis.Hepatology 1986; 6: 24–9.
2 von Recklinghausen FD. Uber Hamochromatose. Tagebl.Versamml. Natur Arzte Heidelberg 1889; 62: 324.
3 Troisier M. Diabete sucre. Bull. La Societe D¢ Anat. Paris1871; 44: 231–5.
4 Feder JN, Gnirke A, Thomas W, Tsuchibashi Z et al. Anovel MHC class-I like gene is mutated in patients with
Figure 6 (a) In situ hybridization using [35S]-labelled anti-sense riboprobe for macrophage inflammatory protein (MIP)-1a, showing abundant expression of MIP-1a mRNA inmacrophages, lymphocytes and endothelial cells in inflamedmucosa in ulcerative colitis. (b) Immunohistochemistry usinga polyclonal rabbit antibody directed against MIP-1a, demon-strating MIP-1a associated with macrophages and lympho-cytes in ulcerative colitis mucosa.

23 Sandborn WJ, Van Os EC, Zins BJ, Tremaine WJ, MaysDC, Lipsky JJ. An intravenous loading dose of azathio-prine decreases the time to response in patients withCrohn’s disease. Gastroenterology 1995; 109: 1808–17.
24 Bouhnik Y, Lemann M, Mary J-Y et al. Long-term follow-up of patients with Crohn’s disease treated withazathioprine or 6-mercaptopurine. Lancet 1996; 347:215–19.
25 Colonna T, Korelitz BI. The role of leukopenia in the 6-mercaptopurine-induced remission of refractory Crohn’sdisease. Am. J. Gastroenterol. 1994; 89: 362–6.
26 Connell WR, Kamm MA, Dickson M, Balkwill AM,Ritchie JK, Lennard-Jones JE. Long-term neoplasia riskafter azathioprine treatment in inflammatory boweldisease. Lancet 1994; 343: 1249–52.
27 Sandborn WJ. Cyclosporine therapy for inflammatorybowel disease: Definitive answers and remaining ques-tions. Gastroenterology 1995; 109: 1001–3.
28 Egan LJ, Sandborn WJ. Methotrexate for inflammatorybowel disease: Pharmacology and preliminary results.Mayo Clin. Proc. 1996; 71: 69–80.
29 Rutgeerts PJ, Heile M, Geboes K et al. Controlled trial ofmetronidazole treatment for prevention of Crohn’s recur-rence after ileal resection. Gastroenterology 1995; 108:1617–21.
30 Rutgeerts PJ, Geboes K,Vantrappen G et al. Rifabutin andethambutol do not help recurrent Crohn’s disease in theneoterminal ileum. J. Clin. Gastroenterol. 1992; 15: 24–8.
31 Gui GPH, Thomas PRS, Tizard MLV, Lake J, SandersonJD, Hermon-Taylor J. Two-year-outcomes analysis ofCrohn’s disease treated with rifabutin and macrolideantibiotics. J. Antimicrob. Chemother. 1997; 39: 393–400.
32 Pullan RD, Rhodes J, Ganesh S et al. Transdermal nico-tine for active ulcerative colitis. N. Engl. J. Med. 1994; 330:811–15.
33 Stack WA, Mann SD, Roy AJ et al. Randomised controlledtrial of CDP571 antibody to tumour necrosis factor-a inCrohn’s disease. Lancet 1997; 349: 521–4.
34 Targan SR, Hanauer SB,Van Deventer SJH et al. A short-term study of chimeric monoclonal antibody cA2 totumor necrosis factor a for Crohn’s disease. N. Engl. J.Med. 1997; 337: 1029–35.
35 Van Deventer SJH, Elson CO, Fedorak RN. Multipledoses of intravenous interleukin 10 in steroid-refractoryCrohn’s disease. Gastroenterology 1997; 113: 383–9.
36 Worldwide transplant center directory liver transplant.Cecka JM, Terasaki PI, eds. Clinical Transplant. LosAngeles: UCLA Tissue Type Laboratory 1996; 625–43.
37 Strong R. Australian Liver Transplant Registry,8th Report. Brisbane: Queensland Liver TransplantService Publications; 1997.
38 Neuberger JM. Recurrence of primary biliary cirrhosis,primary sclerosing cholangitis and autoimmune hepatitis.J. Liver Transplant Surg. 1995; 1: 109–15.
39 Kim WR, Dickson ER. The role of prognostic models inthe timing of liver transplantation. Application in cholesta-tic liver disease. Clinic Liver Dis. 1997; 1: 263–79.
40 Lucey MR, Carr K, Beresford TP et al. Alcohol use afterliver transplantation in alcoholics: A clinical cohort follow-up study. Hepatology 1997; 25: 1223–7.
41 O’Grady JG, Alexander GJM, Hayllar KM, Williams R.Early indicators of prognosis in fulminant hepatic failure.Gastroenterology 1989; 97: 439–45.
192 LW Powell et al.
42 Samuel D, Muller R, Alexander G et al. Liver transplan-tation in European patients with the hepatitis B surfaceantigen. N. Engl. J. Med. 1993; 329: 1824–7.
43 Greillier L, Mutimer D, Ahmed M et al. Lamivudine pro-phylaxis against reinfection in liver transplantation forhepatitis B cirrhosis. Lancet 1996; 348: 1212–15.
44 Angus P, Locarnini S, McCaughan GW, James R, BowdenS. Hepatitis B virus precore mutant infection is associatedwith severe current disease following liver transplantation.Hepatology 1995; 21: 114–18.
45 Naumann U, Protzer-Knolle U, Berg T et al. A pretrans-plant infection with precore mutants of hepatitis B virusdoes not influence the outcome or orthotopic liver trans-plantation in patients on high dose anti-hepatitis B virussurface antigen immunoprophylaxis. Hepatology 1997; 26:478–84.
46 Doughty AL, Spencer JD, Cossart YE, McCaughan GW.Cholestatic hepatitis after liver transplantation is associ-ated with persistently high serum hepatitis C virus RNAlevels. Liver Transplant. Surg. 1998; 4: 15–21.
47 Bizollon T, Palazzo U, Ducerf C et al. Pilot study of thecombination of interferon alfa and ribavirin as therapy ofrecurrent hepatitis C after liver transplantation. Hepatol-ogy 1997; 26: 500.
48 Gane EJ, Bernard CB, Portmann C et al. Long-termoutcome of hepatitis C infection after liver transplanta-tion. N. Engl. J. Med. 1996; 334: 815–20.
49 Mazzaferro V, Regalia E, Doci R et al. Liver transplanta-tion for the treatment of small hepatocellular carcinomasin patients with cirrhosis. N. Engl. J. Med. 1996; 343:693–9.
50 de Ville de Godet J. Split liver transplantation in Europe—1988–93. Transplantation 1995; 59: 1371–6.
51 Heffron TG. Living related liver transplantation. Semin.Liver Dis. 1995; 15: 165–72.
52 McCaughan GW, O’Brien E, Sheil AGR. A follow up of53 adult patients alive beyond 2 years following liver transplantation. J. Gastroenterol. Hepatol. 1993; 8: 569–73.
53 McKenzie SJ, Baker MS, Buffinton GD, Doe WF. Evi-dence of oxidant-induced injury to epithelial cells duringinflammatory bowel disease. J. Clin. Invest. 1996; 98:136–41.
54 Grimm MC, Pullman WE, Bennett GM, Sullivan PJ, PavliP, Doe WF. Direct evidence of monocyte recruitment toinflammatory bowel disease mucosa. J. Gastroenterol.Hepatol. 1995; 10: 387–95.
55 Grimm MC, Pavli P, van de Pol E, Doe WF. Evidence fora CD14+ population of monocytes in inflammatory boweldisease mucosa: Implications for pathogenesis. Clin. Exp.Immunol. 1995; 100: 291–7.
56 Selby WS, Janossy G, Bofill M, Jewell DP. Intestinal lym-phocyte subpopulations in inflammatory bowel disease:An analysis by immunohistochemical and cell isolationtechniques. Gut 1984; 25: 32–40.
57 Mayer L, Schlien R. Evidence for function of Ia moleculeson gut epithelial cells in man. J. Exp. Med. 1987; 166:1471–83.
58 Grimm MC, Elsbury SKO, Pavli P, Doe WF. Interleukin-8: Cells of origin in inflammatory bowel disease. Gut1996; 38: 90–8.
59 Grimm MC, Elsbury SKO, Pavli P, Doe WF. Enhancedexpression and production of monocyte chemoattractant

50 years of gastroenterology in Australia 193
W, Stoll R. Immunoregulatory properties of IL-13 inpatients with inflammatory bowel disease; comparisonwith IL-4 and IL-10. Clin. Exp. Immunol. 1996; 104:483–90.
68 Grimm MC, Oppenheim JJ. Chemokines and their recep-tors provide promising therapeutic targets. MucosalImmunol. Update 1999; (in press).
69 Z’Graggen K, Walz A, Mazzucchelli L, Strieter RM,Mueller C. The C-X-C chemokine ENA-78 is preferen-tially expressed in intestinal epithelium in inflammatorybowel disease. Gastroenterology 1997; 113: 808–16.
APPENDIX
This paper included several contributions from the AWMorrow meeting. The author of each section is indi-cated by*,†,‡,§, respectively at the main heading for eachsection. The authors’ correspondence addresses arelisted below.
*Lawrie Powell, Director, The Queensland Institute ofMedical Research and Professor of Medicine, The Universityof Queensland.
†Warwick Selby, Suite 311, Royal Prince Alfred HospitalMedical Centre, 100 Carillon Avenue, Newtown, NSW 2042,Australia. Email: <[email protected]>
‡Geoffrey McCaughan, AW Morrow Gastroenterol-ogy and Liver Centre, Royal Prince Alfred Hospital,The University of Sydney, NSW, Australia.Email: <[email protected]>
§Michael C Grimm, Department of Medicine, St GeorgeClinical School, Gray Street, Kogarah, NSW 2217, Australia.Email: <[email protected]>
protein-1 in inflammatory bowel disease mucosa. J.Leuko-cyte Biol. 1996; 59: 804–12.
60 Grimm MC, Doe WF. Chemokines in inflammatory boweldisease mucosa: Expression of RANTES, macrophageinflammatory protein (MIP)-1a, MIP-1b and g interferoninducible protein-10 by macrophages, endothelial cells,lymphocytes and granulomas. Infl. Bowel Dis. 1996; 2:88–96.
61 Gionchetti P, Campieri M, Belluzi A et al. Interleukin 1beta (IL-1b) release from fresh and cultured colonicmucosa in patients with ulcerative colitis (UC). AgentsActions 1992; (Suppl.): C50–2.
62 Casini-Raggi V, Kam L, Chong YJT, Fiocchi C, PizarroTT, Cominelli F. Mucosal imbalance of IL-1 and IL-1receptor antagonist in inflammatory bowel disease: Anovel mechanism of chronic intestinal inflammation. J.Immunol. 1995; 154: 2434–40.
63 Stack WA, Mann SD, Roy AJ et al. Randomised controlledtrial of CDP571 antibody to tumour necrosis factor-a inCrohn’s disease. Lancet 1997; 349: 521–4.
64 Parronchi P, Romagnani P, Annunziato F et al. Type 1 T-helper cell predominance and interleukin-12 expression inthe gut of patients with Crohn’s disease. Am. J. Pathol.1997; 150: 823–32.
65 Schrieber S, Heinig T, Panzer U et al. Impaired responseof activated mononuclear phagocytes to interleukin 4 ininflammatory bowel disease. Gastroenterology 1995; 108:21–33.
66 Schrieber S, Heinig T,Thiele HG, Raedler A. Immunoreg-ulatory role of interleukin 10 in patients with inflamma-tory bowel disease. Gastroenterology 1995; 108: 1434–44.
67 Kucharzik T, Lugering N,Weigelt H, Adolf M, Domschke





























