Embed Size (px)
Citation preview

Clinical Neurophysiology 124 (2013) 581–588
Contents lists available at SciVerse ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
Thermal application modulates orofacial somatosensory perception in healthymen and women
Yuka Oono a, Kelun Wang a,b,⇑, Elif Sibel Atis� a, Lars Arendt-Nielsen a
a Center for Sensory-Motor Interaction (SMI), Department of Health Science and Technology, Faculty of Medicine, Aalborg University, Fredrik Bajers Vej 7, Bld. D3,9220 Aalborg, Denmarkb Department of Oral & Maxillofacial Surgery, Aalborg Hospital, Aalborg, Denmark
a r t i c l e i n f o h i g h l i g h t s
Article history:Accepted 30 August 2012Available online 1 October 2012
Keywords:Modality specific modulationCooling and warming applicationSomatosensory perceptionQuantitative sensory testing (QST)Healthy humanTrigeminal system
1388-2457/$36.00 � 2012 International Federation ohttp://dx.doi.org/10.1016/j.clinph.2012.08.025
⇑ Corresponding author at: Center for Sensory-Motment of Health Science and Technology, Faculty of MFredrik Bajers Vej 7, Bld. D3, 9220 Aalborg E, Denmark98154008.
E-mail address: [email protected] (K. Wang).
� Quantitative sensory testing showed an ipsilateral decrease of cutaneous sensation or pain sensitivity(hypoesthesia or hypoalgesia) during cooling without gender differences.� Hypoalgesia on the contralateral side suggests a central mode of action.� The results support clinical experiences that cooling may alleviates pain (cryotherapy) both locally andgenerally.
a b s t r a c t
Objective: To test if orofacial somatosensory perception can be modulated by experimental thermalapplication in healthy human.Methods: Twelve men and twelve age-matched women participated. In each session thermal applicationwith 10, 42 or 32 �C (cooling, warming, control) was applied to the skin over the right masseter using athermode. Quantitative sensory testing was performed at the skin over the right (testing side) and left(contralateral side) masseter before, during, after the thermal application.Results: During the cooling, mechanical detection threshold (MDT), mechanical pain threshold (MPT) andpressure pain threshold (PPT) were increased, and mechanical pain sensitivity was decreased at testingside compared with baseline (P < 0.005). The MPT and PPT at the contralateral side were also increased(P < 0.004). During the warming and control, the MDT was increased at the testing side compared withbaseline (P = 0.002). The somatosensory sensitivity was decreased during cooling compared to warmingand control (P < 0.05). No gender differences were found.Conclusions: This study shows an ipsilateral decrease of cutaneous sensation or pain sensitivity duringcooling without gender differences. In addition, hypoalgesia on the contralateral side suggests a centralmode of action.Significance: The results support clinical experiences that cooling may alleviates pain both locally andgenerally.� 2012 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved.
1. Introduction
Cryotherapy (e.g., cold compresses) or thermotherapy (e.g.,warm compresses) is clinically used to reduce pain or discomfort(Meeusen and Lievens, 1986; Lavergne, 1997; Leaper, 2006;Melling and Leaper, 2006; Rand et al., 2007). Physiological studiesindicate that cryotherapy resulted in vasoconstriction, reduction of
f Clinical Neurophysiology. Publish
or Interaction (SMI), Depart-edicine, Aalborg University,
. Tel.: +45 99408830; fax: +45
edema, and diminished pain perception (Muldoon, 2006). Coolingof an operation side prior to infiltration of local anesthesia signifi-cantly reduces pain perception associated with infiltration (Leffet al., 2007). Cryotherapy is also applied after intraoral surgicalprocedures (Greenstein, 2007). Thermotherapy with warming iseffective for wound healing and reduction in postoperative pain(Melling and Leaper, 2006). However, little is known about theeffects of thermal application on the somatosensory function andhow thermal application modulates sensory perception in healthyhumans. Thus, it would be interesting to investigate the modula-tion of somatosensory perception by local thermal application inhealthy subjects.
ed by Elsevier Ireland Ltd. All rights reserved.

582 Y. Oono et al. / Clinical Neurophysiology 124 (2013) 581–588
Quantitative sensory testing (QST) is a noninvasive method forthe assessment of sensory nerve function (Dyck, 1993). QST hasbeen developed significantly in recent years (Rolke et al., 2006)and is widely applied in human experimental (Hagander et al.,2000) and clinical studies for the assessment of sensory nervedamage in patients (Yarnitsky, 1997; Forssell et al., 2002;Jääskeläinen et al., 2005; Maruo et al., 2011). QST provides psycho-physical methods that systematically document alterations andreorganization in nervous system functions and, in particular, inthe nociceptive system. QST is defined as the determination ofthresholds or stimulus response curves for sensory processingunder normal and pathophysiological conditions. The modernconcept of advanced QST for experimental pain/sensitizationassessment is a multimodality, multi-tissue approach where differ-ent pain/sensitization modalities (thermal, mechanical, electrical,and chemical) are applied to different tissues (skin, muscles, andviscera) (Arendt-Nielsen and Yarnitsky, 2009), and the responsesare assessed by psychophysical methods (thresholds and stimu-lus–response functions).
To date, gender differences in pain perception have been exam-ined. In most studies women report more intense pain, more fre-quent pain and longer duration of pain than men (Unruh, 1996).Greater pain sensitivity in women compared to men occur in theperipheral actions of glutamate (Cairns et al., 2001) and morphine(Sessle, 2000), suggesting that peripherally based physiologicalmechanisms may contribute to the gender differences in the painconditions (Cairns et al., 2001; Sessle, 2005). The recent reviewon gender differences in pain modulation shows that significantlymore efficient pain inhibition in men than women (Popescu et al.,2010). However, the gender effect on sensory perceptions of thethermal modulation is still controversial.
The specific aims of the present study were to investigate (1)whether somatosensory perception was modulated by experimen-tal thermal application to the skin of the orofacial region (ipsilater-ally and contralaterally) in healthy humans and (2) the possibleinfluence of gender on such modulations.
2. Methods
2.1. Subjects
Twelve healthy men (mean ± SEM age: 25.6 ± 0.9 years, agerange: 21–33 years) and twelve healthy age-matched women(mean ± SEM age: 25.2 ± 1.0 years, age range: 21–31 years) partic-ipated in the study. None of the subjects had any pain complaintsor previous injuries that interfered with normal somatosensoryfunctioning. Informed consent was obtained from all subjects be-fore inclusion. The study followed the Helsinki Declaration andwas approved by the local ethics committee (VN20080057).
2.2. Quantitative sensory testing (QST)
The following QST (4 test measurings and 4 parameters) wasperformed according to the standardized QST protocol recom-mended by German Research Network on Neuropathic Pain (DFNS)(Rolke et al., 2006). In addition, pressure pain tolerance (PPTol) wasrecorded. All measurements were performed at the skin over boththe right (testing side) and left (contralateral side) massetermuscle.
2.2.1. Mechanical detection threshold (MDT)The mechanical detection threshold (MDT) was measured with
calibrated Semmes–Weinstein monofilaments (Touch-Test, NorthCoast Medical, Canada) that exert forces between 0.008 and300 g (0.0784–2941.9 mN). Using the ‘‘method of limits’’, five
threshold determinations were made, each with a series of ascend-ing and descending stimulus intensities. The final threshold wasthe geometric mean of these five series (Baumgärtner et al.,2002; Rolke et al., 2006).
2.2.2. Mechanical pain threshold (MPT) for pinprick stimuliThe mechanical pain threshold (MPT) was measured using a set
of five custom-made spring pinprick stimulators (with a flat con-tact area of 0.03 mm2). The stimulators are able to apply 5 gradesof force with 5 different strengths of the spring. The applied forcesare calibrated as 32, 64, 128, 256, and 512 mN. Again using the‘‘method of limits’’, the final threshold was the geometric meanof five series of ascending and descending stimulus intensities.
2.2.3. Stimulus/response functions; mechanical pain sensitivity (MPS)for pinprick stimuli
Mechanical pain sensitivity (MPS) to sharp stimuli was testedusing the same spring pinprick stimuli as for MPT. To obtain astimulus–response function, these five pinprick stimuli were ap-plied in a randomized order, three times each. The subjects wereasked to give a perception rating for each stimulus on a 0–100numerical rating scale (‘‘0’’ indicating ‘‘no sensation’’, ‘‘50’’ indicat-ing ‘‘slight pain’’ and ‘‘100’’ indicating ‘‘worst pain imaginable’’).The sum of the values multiplied by the exert forces (one valuefor one subject in one session) was used for further analysis.
2.2.4. Pressure pain thresholds (PPT) and pressure pain tolerance(PPTol)
Pressure pain thresholds (PPT) and pressure pain tolerance(PPTol) were measured to test deep pain sensitivity. PPT and PPTolwere recorded by a pressure algometer (Somedic, Sweden) with aprobe area of 1 cm2. Pressure was applied as a slowly increasingramp of 30 kPa/s both in PPT and PPTol (Arendt-Nielsen et al.,2008). The PPT was defined as the amount of pressure (kPa) whichthe subjects first perceived to be painful and was determined withthree series of ascending stimulus intensities. The absolute meanvalue of the three recordings was used for further analysis. ThePPT measurement was followed by PPTol measurement. PPTolwas defined as the most painful pressure (kPa) which the subjectcould tolerate. PPTol was recorded only once at each time pointand side to avoid excessive stimulation and sensitization phenom-ena. The absolute PPTol value was also used for analysis.
2.3. Thermal application
In each session thermal stimulation with a target of 10, 42 or32 �C was applied to the skin surface of the right masseter muscleusing a thermode (ATS, PATHWAY, Medoc, Israel). The computer-driven PATHWAY system contains a metal contact plate (contactarea: 30 � 30 mm) which is cooled and heated by an external Pel-tier element to the target levels and is used for applying the ther-mal stimulation. The baseline temperature was 32 �C and thetarget temperature was obtained by a ramped time of 1 �C/s.
2.4. Temperature monitoring
The temperature on the skin surface of the right masseter mus-cle (testing side) was monitored by an infrared camera (SAT-S280,GSAT, China). The camera was positioned 1 m from the skin surfaceof the subject. The emissivity was set at 0.98 for skin, and the roomtemperature and humidity were calibrated before starting themonitoring in each session. The skin temperature was recorded be-fore and after the thermal stimulation, and in addition before andafter each recording of QST parameters at both testing and contra-lateral sides.

0
Cooling or Warming or
Controlof testing side
for 10 min
Cooling or Warming or
Control of testing side
for 4 min every 2 min
Recording of skin temperature
Baseline 15 min afterDuring thermal application
Time (min)
PPTolPPTM
PS
MPT
MD
T
PPTol
PPT
MPS
MPT
MD
T
PPTolPPTM
PS
MPT
MD
T
15 min break
Fig. 1. Overview of the study design. Quantitative sensory testing (mechanical detection threshold: MDT, mechanical pain threshold: MPT, mechanical pain sensitivity forpinprick stimuli: MPS, pressure pain thresholds: PPT and pressure pain tolerance: PPTol) was performed at the skin over the right (testing side) and left (contralateral side)masseter muscle before (baseline), during and 15 min after the application of thermal stimulation (three sessions, one session per 1 day). The double arrow shows the periodof thermal application. The arrow shows the recording of skin temperature by infrared camera.
Y. Oono et al. / Clinical Neurophysiology 124 (2013) 581–588 583
2.5. Pain ratings
The subjects were asked to rate the pain intensity for thermalstimulation on a 0–10 cm visual analogue scale (VAS, 0 = no pain,10 = worst pain imaginable). The VAS ratings were sampled afterevery thermal application and were used for further analysis.
2.6. Experimental protocol (Fig. 1)
The experiment was carried out in a quiet room with a temper-ature between 21 and 25 �C and a humidity between 32% and 55%.Subjects were seated in a comfortable chair. QST (MDT, MPT, MPS,PPT and PPTol) was performed at the right (testing side) and left(contralateral side) masseter muscle before, during and 15 minafter the end of the thermal stimulation. After QST recording atbaseline, thermal application of 10, 42 or 32 �C (cooling, warming,or control session, respectively) was performed with the thermodeslightly touching the skin surface of the right masseter for 10 min.The skin temperature of the right masseter muscle (testing side)was monitored by an infrared camera throughout experiment,and the thermal application was repeated for 4 min every 2 minduring the QST testing. The subjects rated the pain intensity on a0–10 cm VAS after the application of the thermal stimulation.The three sessions were randomized and separated by at least1 week.
2.7. Statistical analysis
The Kolmogorov–Smirnov test was applied to verify the normaldistribution of data. As the Kolmogorov–Smirnov test showed thatthe absolute values of the QST parameters were not normally dis-tributed (P < 0.05), these data were analyzed by Wilcoxon signed-rank test for the comparison of baseline with during, and 15 minafter the thermal application. Then the absolute values of theQST parameters were normalized to the baseline values to testthe possible differences between genders and among sessions(cooling, warming, and control). Since the Kolmogorov–Smirnovtest showed that the normalized values of the QST parameterswere normally distributed (P > 0.05), 2-way ANOVAs were per-formed at each time point to test the possible differences betweengenders and among sessions (cooling, warming, and control).ANOVAs were followed by the post hoc Bonferroni’s correctiontests for the session comparisons. All tests had also performed afterremoving the data from subjects reporting pain for the thermalstimulation.
All data are presented as mean values and standard errors ofmean (SEM). The level of significance was set at P < 0.05.
3. Results
3.1. Temperature controlling
The typical pictures taken by infrared camera are shown inFig. 2. The mean skin temperatures from all the subjects (n = 24)(mean ± SEM) in the three sessions are shown in Fig. 3. Base skintemperature was 35.1 ± 0.4, 35.1 ± 0.4 and 34.5 ± 0.4 �C (mean ±SEM) in cooling, warming and control sessions, respectively. Themean temperature values of a train of ‘‘after thermal application’’,‘‘after QST test at testing side (right masseter)’’ and ‘‘after QST testat contralateral side (left masseter)’’ are: 19.2 ± 0.1, 25.5 ± 0.6,27.4 ± 1.3 �C in cooling session; 41.8 ± 0.1, 39.0 ± 0.1, 38.8 ± 0.2 �Cin warming session; and 34.9 ± 0.1, 35.5 ± 0.1, 35.8 ± 0.1 �C in con-trol session, respectively.
3.2. VAS ratings for pain
Application of thermal stimulation elicited pain in 9 of 24 sub-jects in the cooling session with a pain intensity of 0.9 ± 0.2 cm(mean values from all 24 subjects) and in 1 of 24 subjects in thewarming session with a pain intensity of 0.2 ± 0.1 cm (mean valuesfrom all 24 subjects). No subject reported thermal pain in the con-trol session.
3.3. QST data from all subjects
The absolute values from both men and women were added upas there was no gender difference in the results. Table 1 shows theQST data at the testing side (right masseter) and contralateral side(left masseter) before, during, and 15 min after thermal applicationin three sessions (combined data from men and women) (mean ±SEM). ⁄Indicates significant change after thermal application com-pared with baseline (Wilcoxon signed-rank test; P < 0.05).
3.3.1. MDTWilcoxon signed-rank test showed that the MDT at the testing
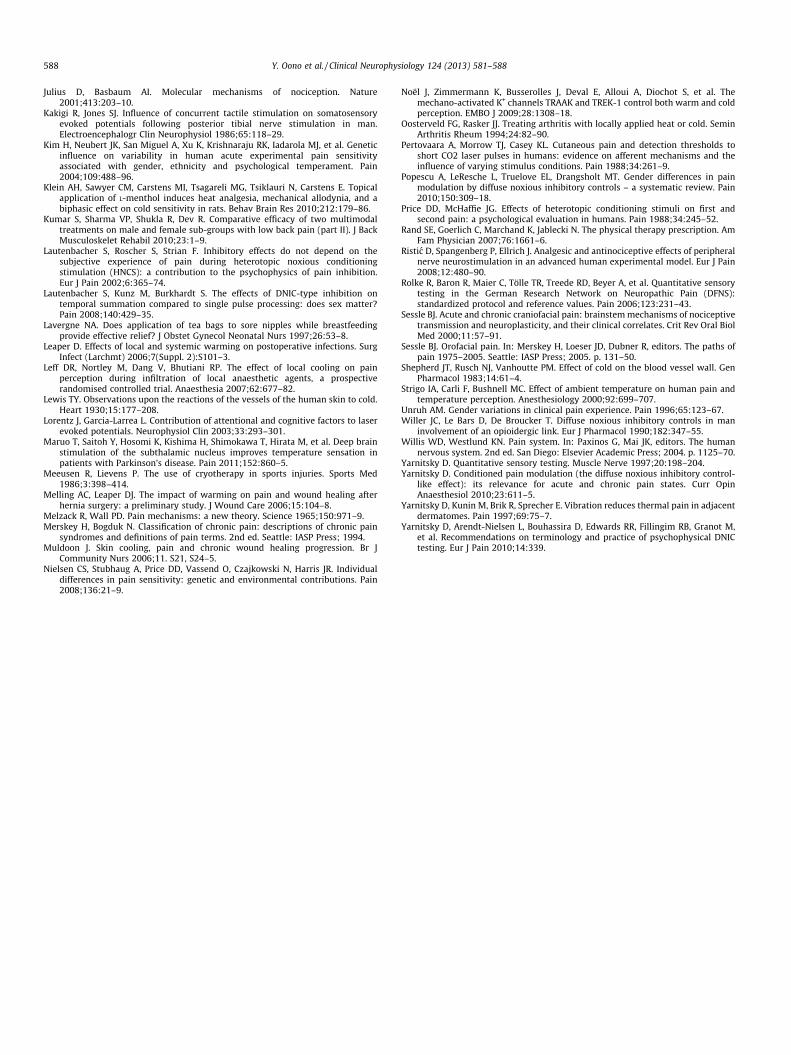
side was significantly increased during the thermal application inthe cooling (P < 0.001), warming (P = 0.002), as well as control ses-sion (P = 0.002) compared with baseline. ANOVAs with normalizedvalues during thermal application showed no gender differences(P = 0.790) but showed significant session differences (P < 0.001).The post hoc tests showed significantly larger increases of MDTduring cooling (630.1 ± 112.9%) compared to warming(198.6 ± 30.8%, P < 0.001) and control (167.1 ± 15.9%, P < 0.001).The significant changes were observed only during the thermalapplication and not 15 min after the thermal application (Fig. 4a).There were no significant changes at the contralateral side.
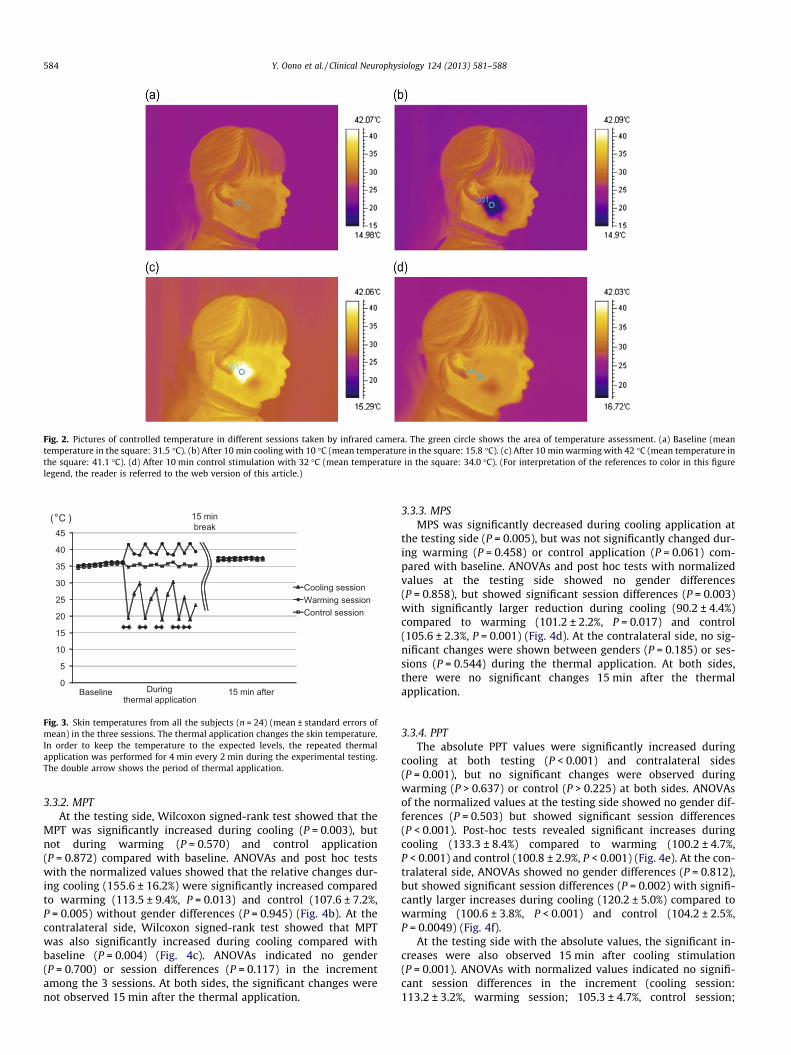
Fig. 2. Pictures of controlled temperature in different sessions taken by infrared camera. The green circle shows the area of temperature assessment. (a) Baseline (meantemperature in the square: 31.5 �C). (b) After 10 min cooling with 10 �C (mean temperature in the square: 15.8 �C). (c) After 10 min warming with 42 �C (mean temperature inthe square: 41.1 �C). (d) After 10 min control stimulation with 32 �C (mean temperature in the square: 34.0 �C). (For interpretation of the references to color in this figurelegend, the reader is referred to the web version of this article.)
0
5
10
15
20
25
30
35
40
45
Cooling sessionWarming sessionControl session
(°C )
Baseline 15 min afterDuringthermal application
15 min break
Fig. 3. Skin temperatures from all the subjects (n = 24) (mean ± standard errors ofmean) in the three sessions. The thermal application changes the skin temperature.In order to keep the temperature to the expected levels, the repeated thermalapplication was performed for 4 min every 2 min during the experimental testing.The double arrow shows the period of thermal application.
584 Y. Oono et al. / Clinical Neurophysiology 124 (2013) 581–588
3.3.2. MPTAt the testing side, Wilcoxon signed-rank test showed that the
MPT was significantly increased during cooling (P = 0.003), butnot during warming (P = 0.570) and control application(P = 0.872) compared with baseline. ANOVAs and post hoc testswith the normalized values showed that the relative changes dur-ing cooling (155.6 ± 16.2%) were significantly increased comparedto warming (113.5 ± 9.4%, P = 0.013) and control (107.6 ± 7.2%,P = 0.005) without gender differences (P = 0.945) (Fig. 4b). At thecontralateral side, Wilcoxon signed-rank test showed that MPTwas also significantly increased during cooling compared withbaseline (P = 0.004) (Fig. 4c). ANOVAs indicated no gender(P = 0.700) or session differences (P = 0.117) in the incrementamong the 3 sessions. At both sides, the significant changes werenot observed 15 min after the thermal application.
3.3.3. MPSMPS was significantly decreased during cooling application at
the testing side (P = 0.005), but was not significantly changed dur-ing warming (P = 0.458) or control application (P = 0.061) com-pared with baseline. ANOVAs and post hoc tests with normalizedvalues at the testing side showed no gender differences(P = 0.858), but showed significant session differences (P = 0.003)with significantly larger reduction during cooling (90.2 ± 4.4%)compared to warming (101.2 ± 2.2%, P = 0.017) and control(105.6 ± 2.3%, P = 0.001) (Fig. 4d). At the contralateral side, no sig-nificant changes were shown between genders (P = 0.185) or ses-sions (P = 0.544) during the thermal application. At both sides,there were no significant changes 15 min after the thermalapplication.
3.3.4. PPTThe absolute PPT values were significantly increased during
cooling at both testing (P < 0.001) and contralateral sides(P = 0.001), but no significant changes were observed duringwarming (P > 0.637) or control (P > 0.225) at both sides. ANOVAsof the normalized values at the testing side showed no gender dif-ferences (P = 0.503) but showed significant session differences(P < 0.001). Post-hoc tests revealed significant increases duringcooling (133.3 ± 8.4%) compared to warming (100.2 ± 4.7%,P < 0.001) and control (100.8 ± 2.9%, P < 0.001) (Fig. 4e). At the con-tralateral side, ANOVAs showed no gender differences (P = 0.812),but showed significant session differences (P = 0.002) with signifi-cantly larger increases during cooling (120.2 ± 5.0%) compared towarming (100.6 ± 3.8%, P < 0.001) and control (104.2 ± 2.5%,P = 0.0049) (Fig. 4f).
At the testing side with the absolute values, the significant in-creases were also observed 15 min after cooling stimulation(P = 0.001). ANOVAs with normalized values indicated no signifi-cant session differences in the increment (cooling session:113.2 ± 3.2%, warming session; 105.3 ± 4.7%, control session;
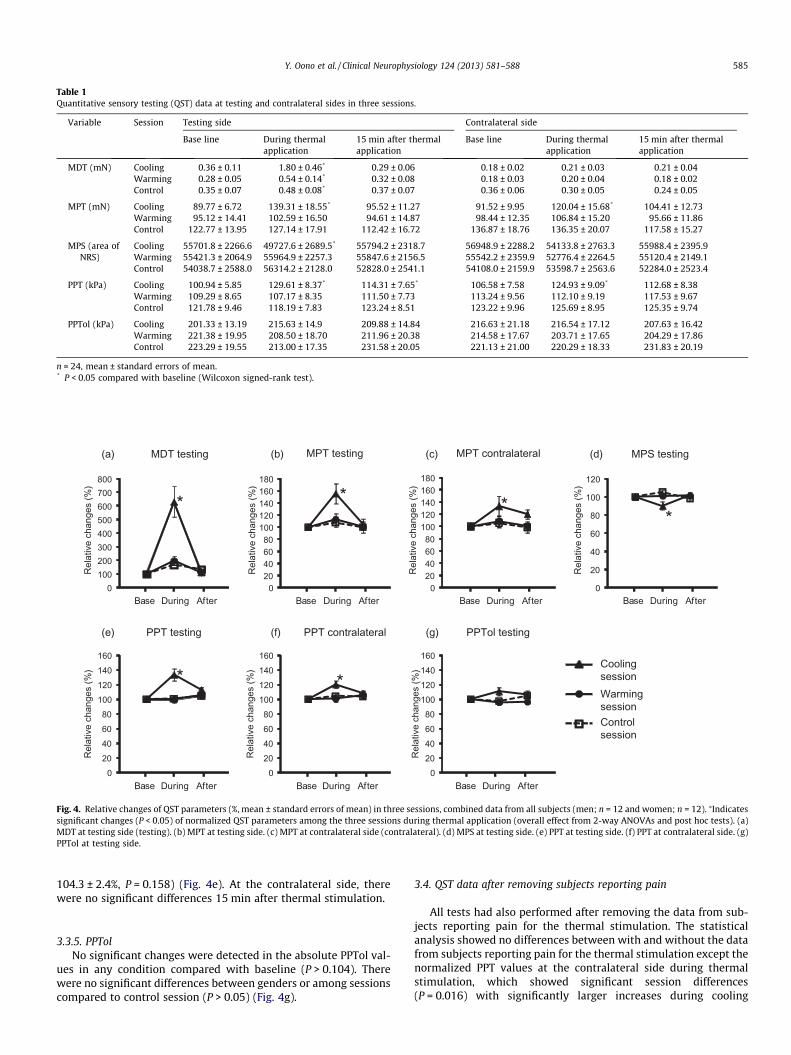
Table 1Quantitative sensory testing (QST) data at testing and contralateral sides in three sessions.
Variable Session Testing side Contralateral side
Base line During thermalapplication
15 min after thermalapplication
Base line During thermalapplication
15 min after thermalapplication
MDT (mN) Cooling 0.36 ± 0.11 1.80 ± 0.46* 0.29 ± 0.06 0.18 ± 0.02 0.21 ± 0.03 0.21 ± 0.04Warming 0.28 ± 0.05 0.54 ± 0.14* 0.32 ± 0.08 0.18 ± 0.03 0.20 ± 0.04 0.18 ± 0.02Control 0.35 ± 0.07 0.48 ± 0.08* 0.37 ± 0.07 0.36 ± 0.06 0.30 ± 0.05 0.24 ± 0.05
MPT (mN) Cooling 89.77 ± 6.72 139.31 ± 18.55* 95.52 ± 11.27 91.52 ± 9.95 120.04 ± 15.68* 104.41 ± 12.73Warming 95.12 ± 14.41 102.59 ± 16.50 94.61 ± 14.87 98.44 ± 12.35 106.84 ± 15.20 95.66 ± 11.86Control 122.77 ± 13.95 127.14 ± 17.91 112.42 ± 16.72 136.87 ± 18.76 136.35 ± 20.07 117.58 ± 15.27
MPS (area ofNRS)
Cooling 55701.8 ± 2266.6 49727.6 ± 2689.5* 55794.2 ± 2318.7 56948.9 ± 2288.2 54133.8 ± 2763.3 55988.4 ± 2395.9Warming 55421.3 ± 2064.9 55964.9 ± 2257.3 55847.6 ± 2156.5 55542.2 ± 2359.9 52776.4 ± 2264.5 55120.4 ± 2149.1Control 54038.7 ± 2588.0 56314.2 ± 2128.0 52828.0 ± 2541.1 54108.0 ± 2159.9 53598.7 ± 2563.6 52284.0 ± 2523.4
PPT (kPa) Cooling 100.94 ± 5.85 129.61 ± 8.37* 114.31 ± 7.65* 106.58 ± 7.58 124.93 ± 9.09* 112.68 ± 8.38Warming 109.29 ± 8.65 107.17 ± 8.35 111.50 ± 7.73 113.24 ± 9.56 112.10 ± 9.19 117.53 ± 9.67Control 121.78 ± 9.46 118.19 ± 7.83 123.24 ± 8.51 123.22 ± 9.96 125.69 ± 8.95 125.35 ± 9.74
PPTol (kPa) Cooling 201.33 ± 13.19 215.63 ± 14.9 209.88 ± 14.84 216.63 ± 21.18 216.54 ± 17.12 207.63 ± 16.42Warming 221.38 ± 19.95 208.50 ± 18.70 211.96 ± 20.38 214.58 ± 17.67 203.71 ± 17.65 204.29 ± 17.86Control 223.29 ± 19.55 213.00 ± 17.35 231.58 ± 20.05 221.13 ± 21.00 220.29 ± 18.33 231.83 ± 20.19
n = 24, mean ± standard errors of mean.* P < 0.05 compared with baseline (Wilcoxon signed-rank test).
020406080
100120140160
020406080
100120140160
020406080
100120140160180
0
20
40
60
80
100
120
020406080
100120140160180
0100200300400500600700800
MDT testing MPT testing
* *
(a)
Rel
ativ
e ch
ange
s (%
)
MPS testing
*
(b) (d)
(e) (g)
Base During After
PPT testing PPTol testing(f) PPT contralateral
* *
020406080
100120140160
Control session
Warming session
Cooling session
Base During AfterBase During After
Base During AfterBase During AfterBase During After
MPT contralateral(c)
*
Base During After
Rel
ativ
e ch
ange
s (%
)
Rel
ativ
e ch
ange
s (%
)
Rel
ativ
e ch
ange
s (%
)
Rel
ativ
e ch
ange
s (%
)
Rel
ativ
e ch
ange
s (%
)
Rel
ativ
e ch
ange
s (%
)
Fig. 4. Relative changes of QST parameters (%, mean ± standard errors of mean) in three sessions, combined data from all subjects (men; n = 12 and women; n = 12). ⁄Indicatessignificant changes (P < 0.05) of normalized QST parameters among the three sessions during thermal application (overall effect from 2-way ANOVAs and post hoc tests). (a)MDT at testing side (testing). (b) MPT at testing side. (c) MPT at contralateral side (contralateral). (d) MPS at testing side. (e) PPT at testing side. (f) PPT at contralateral side. (g)PPTol at testing side.
Y. Oono et al. / Clinical Neurophysiology 124 (2013) 581–588 585
104.3 ± 2.4%, P = 0.158) (Fig. 4e). At the contralateral side, therewere no significant differences 15 min after thermal stimulation.
3.3.5. PPTolNo significant changes were detected in the absolute PPTol val-
ues in any condition compared with baseline (P > 0.104). Therewere no significant differences between genders or among sessionscompared to control session (P > 0.05) (Fig. 4g).
3.4. QST data after removing subjects reporting pain
All tests had also performed after removing the data from sub-jects reporting pain for the thermal stimulation. The statisticalanalysis showed no differences between with and without the datafrom subjects reporting pain for the thermal stimulation except thenormalized PPT values at the contralateral side during thermalstimulation, which showed significant session differences(P = 0.016) with significantly larger increases during cooling

586 Y. Oono et al. / Clinical Neurophysiology 124 (2013) 581–588
(116.2 ± 4.6%) compared to warming (100.9 ± 4.0%, P = 0.006) butnot compared to control (104.2 ± 2.5%, P = 0.028).
4. Discussion and conclusions
This present study showed that sensory perceptions of healthyhumans are modulated by local thermal application without gen-der differences. The most consistent finding is that cooling modu-lates ipsilateral cutaneous sensation and pain, mechanical painsensitivity as well as deep pain sensitivity, which result in localhypoesthesia or hypoalgesia. In addition, the increment of cutane-ous pain threshold and deep pain sensitivity (hypoalgesia) at thecontralateral side implies central modulation during coolingapplication.
4.1. Methodological concerns
In this study, a Peltier thermode was used to perform the ther-mal application, and the temperature of the testing side (skin sur-face of the muscle) was monitored by an infrared camera. Thetarget temperatures were 10 �C in the cooling, 42 �C in the warm-ing, and 32 �C in the control session, whereas the real temperaturecould not reach the target level after 10 min of the thermal appli-cation especially in the cooling session. A possible consideration onthis phenomenon is that the skin surface of the muscle waswarmed-up quickly after finishing the thermal application becauseof capillary perfusion (Lewis, 1930). Therefore, we repeated thethermal application every 2 min during the experiment to keepthe temperature of the skin to the expected levels. Even thoughthe temperatures still fluctuated during the QST recordings, theall recordings were made during the expected temperatures.Hence, it is supposed that the temperature shifts during the ther-mal application have not influenced on the final results.
The temperature shown in the paper was rated from the infra-red camera. The pre-setting parameter could influence the indi-cated temperature. There could be 1–2 �C difference between theindicated and the real temperature according to the technical as-pect of the camera even though the presetting was made beforeeach experiment.
Central modulation comes with delayed onset (Ristic et al.,2008). In this study, the testing side was first tested immediatelyafter the thermal application. The temperature during testingwas in the range from 19.2 to 25.5 �C in cooling, from 41.8 to39.0 �C in warming and from 34.9 to 35.5 �C in control session,respectively. Therefore, we could keep the cooling of the skin tem-perature with 10 �C difference from baseline as expected. Also inthe warming and control sessions, the skin temperature was main-tained within the expected range.
Finally, the small sample size might relate to the partial positiveresults among all tests. The further study with bigger sample size isexpected.
4.2. Local effects of thermal applications on somatosensory perception
The present study showed that the thermal application modu-lates both cutaneous and deep somatosensory perceptions, whichresult in hypoesthesia and hypoalgesia (Merskey and Bogduk,1994).
It is worth noting that the robust hypoesthesic and hypoalgesiceffects in this study were observed with cold application. Innocuousskin cooling leads to increased absolute detection threshold(Pertovaara et al., 1988) and pain thresholds (Hardy et al., 1951;Pertovaara et al., 1988; Strigo et al., 2000). The demonstratedhypoalgesic phenomenon is in line with a previous study which
demonstrates that cold stimulation modulates cutaneous sensationand reduces deep pain sensitivity (Oosterveld and Rasker, 1994).
A peripheral effect may be involved, and a number of theorieshave introduced an explanation of the mechanism of cold inducedanesthesia and analgesia. The classical theory of hypoesthesia andhypoalgesia induced by cold is a peripheral modulation triggeredby the nerve block by cold application (Shepherd et al., 1983). Be-sides, afferent input from cutaneous cold receptors elicits a spatio-temporally patterned vasoconstrictor response in the outside oftheir receptive field (Isii et al., 2007). In addition, low temperaturesretard neuromuscular transmission (Halar et al., 1980). Taken to-gether, topical cold application stimulates myelinated Ad-fibers,activating inhibitory pain pathways, which in turn raises the tactileand pain threshold.
At the peripheral level, transient receptor potential (TRP) chan-nels may be involved as they contribute to sensory transduction,responding to a wide variety of stimuli including temperature,nociceptive stimuli, touch and other stimuli (Clapham, 2003). Thecold-sensitive thermo-TRP channel, TRPM8, is one of the potentialperipheral targets of pain modulation (Klein et al., 2010) which isactivated by temperatures below 25 �C (Behrendt et al., 2004). Coldsensation most likely involves multiple channels (Noël et al., 2009)in transducing and modulating the temperature information (Bel-monte et al., 2009). Moreover, there are excitatory or inhibitoryinteractions in various functional types of peripheral sensory neu-rons for touch, cold or pain which are excited via TRP channelswithin the range of 15–35 �C (Belmonte et al., 2009; Klein et al.,2010). These excitatory or inhibitory interactions mediate allo-dynia or pain attenuation (Belmonte et al., 2009). It is likely thatthese inhibitory interactions were demonstrated in this study.Hence, the peripheral modality-specific modulation of the somato-sensory perception is to be considered.
Regarding the warm application, local warming application re-duces postoperative pain (Melling and Leaper, 2006). Some exper-imental evidences showed that warming inhibited pain sensation,which could be caused by central interaction between warmth andpain (Casey et al., 1993) or peripheral mechanism induced by TRPV(vanilloid) channels for heat sensation (Clapham, 2003). Howeverthe warming application seems to lack significant analgesic effectin the present study. The possible explanation for the inconsistentresults with previous studies might be the different experimentalparadigm to various subjects.
4.3. Central mechanism of modality-specific modulation
In the present study, the hypoalgesia at the contralateral sidewas observed. The finding suggests that the central mechanismcould be involved in addition to the peripheral mechanism. Evi-dence of the central interaction is supported by the observationsthat innocuous cooling stimuli reduce pain perception by inhibit-ing pain processing (Bini et al., 1984; Craig, 1998). The cool ambi-ent temperature decreases the skin temperature and activatescool-sensitive neural pathways mediated by Ad-fiber activity. Con-sequently, this activation leads to centrally mediated inhibition ofnociceptive activity and a subsequent reduction in perceived painintensity (Strigo et al., 2000). Moreover, detection and pain thresh-olds are not determined solely by the liminal primary afferent dis-charge, rather central summation of primary afferent impulses isimportant for liminal non-painful and painful sensations(Pertovaara et al., 1988).
One of the well-known mechanisms relating to central paininhibition is the Gate Control Theory (Melzack and Wall, 1965).The Gate Control Theory posits that large diameter afferents inhibitthe small diameter fiber activation locally. The present study alsoshowed hypoesthesia in the control session at testing side. Thefinding implies that the mechanical tactile stimulation by putting

Y. Oono et al. / Clinical Neurophysiology 124 (2013) 581–588 587
the thermode may have a centrally mediated gating modulatory ef-fect on the somatosensory perceptions (Kakigi and Jones, 1986),possibly via the Gate Control Theory. Another possible mechanismis Conditioned Pain Modulation (CPM). CPM is the phenomenonthrough which the conditioning stimulus affects the test stimulus(Yarnitsky, 2010; Yarnitsky et al., 2010). Previous literature reportsthat the CPM effect can only be seen during conditioning stimulus(Price and McHaffie, 1988), on the contrary, the later study sug-gests that the CPM effect can also be seen after the end of the con-ditioning stimulus (Willer et al., 1990). In addition to the painfulconditioning stimulus, non-painful conditioning stimulation, suchas vibration or warmth, can also trigger CPM (Yarnitsky et al.,1997; Lautenbacher et al., 2002). In fact, there were no remarkabledifferences in this study in spite of removing the data from subjectsreporting pain for the thermal stimulation. Though the modulatoryeffect depends on the modality of the conditioning stimulus, thehypoalgesia at the contralateral side and 15 min after cooling atthe testing side is possibly to be a central effect such as CPM. Fur-thermore, it is noteworthy that the central modulatory system canbe activated not only by stimuli, but also psychological factors,such as attention (Lorentz and Garcia-Larrea, 2003). As suggestedby the higher rate of pain detection during cooling than warming,subjects’ attention could have been diverged from the test stimulusduring cooling more than during warming.
As for the somatosensory perception and pathway from periph-eral to central, the first step is the activation of the free nerve end-ings. All primary sensory nociceptors make synaptic connectionswith neurons in the dorsal horn (Julius and Basbaum, 2001). Sub-sets of dorsal horn neurons, in turn, project axons and transmitpain messages to higher brain centers, including the reticular for-mation, thalamus and ultimately the cerebral cortex (Basbaumand Jessell, 2000; Craig, 2003). Thalamus and a number of cerebralcortical areas are activated by pain, temperature and tactile per-ception and play a role as important structures in the higher pro-cessing (Davis et al., 1998; Willis and Westlund, 2004). Takentogether, the modulation at peripheral or central level might leadto the modality-specific modulation which was demonstrated inthis study.
4.4. Gender effects in thermal modulation
Gender differences were not detected in the present study inthe somatosensory modulation by thermal application. The resultsare consistent with previous literature which showed no genderdifference in pain inhibition with cold stimulation (Baad-Hansenet al., 2005) and heat stimulation (Lautenbacher et al., 2008). Onthe contrary, thermotherapy for chronic low back pain with ultra-sound is more effective in men than women (Kumar et al., 2010).Some of the endogenous pain modulatory systems are less robustin women than in men (Popescu et al., 2010). Further research isrequired to address gender differences in the modulation ofsomatosensory perception.
4.5. Clinical implications
Various cooling modalities are used clinically for application ofcold treatment such as for burned pain (Gallagher et al., 2000).Though the effect of cooling might differ depending on the applica-tion method and targeted tissue, the use of cryotherapy has a po-sitive effect on pain reduction and the recovery from injuries(Meeusen and Lievens, 1986). Even though thermotherapy is effec-tive for relieving pain, the existence of large individual differencesin pain sensitivity is reported (Nielsen et al., 2008). Furthermore,genetic influence on the variability in human thermal pain sensi-tivity associates with gender, ethnicity and psychological temper-ament (Kim et al., 2004). Therefore, the individual difference
should be considered in clinical thermal treatment. The applicationof thermal stimulation might be efficient tailor-made analgesictreatments. Further investigation would be required for moredetails.
In conclusion, this is the first study to systematically show thesomatosensory modulation of the local thermal application byusing QST. Thermal application results in hypoesthesia and hypoal-gesia in the orofacial region of healthy humans ipsilaterally to thethermal application. In addition, contralateral effects were foundsuggesting central modality-specific modulations. Thermotherapy,especially cryotherapy, is likely to be an effective option for mod-ulating the somatosensory perceptions and for pain relief in clini-cal cases.
Acknowledgement
Supported by The Villum Kann Rasmussen Foundation (GrantNo. VKR09B-009). The authors declare no conflicts of interest.
References
Arendt-Nielsen L, Yarnitsky D. Experimental and clinical applications ofquantitative sensory testing applied to skin, muscles and viscera. J Pain2009;10:556–72.
Arendt-Nielsen L, Sluka KA, Nie HL. Experimental muscle pain impairs descendinginhibition. Pain 2008;140:465–71.
Baad-Hansen L, Poulsen HF, Jensen HM, Svensson P. Lack of sex differences inmodulation of experimental intraoral pain by diffuse noxious inhibitorycontrols (DNIC). Pain 2005;116:359–65.
Basbaum AI, Jessell TM. The perception of pain. In: Kandel ER, Schwartz JH, JessellTM, editors. Principles of neural science. 4th ed. New York: McGraw-HillMedical; 2000. p. 472–91.
Baumgärtner U, Magerl W, Klein T, Hopf HC, Treede RD. Neurogenic hyperalgesiaversus painful hypoalgesia: two distinct mechanisms of neuropathic pain. Pain2002;96:141–51.
Behrendt HJ, Germann T, Gillen C, Hatt H, Jostock R. Characterization of the mousecold-menthol receptor TRPM8 and vanilloid receptor type-1 VR1 using afluorometric imaging plate reader (FLIPR) assay. Br J Pharmacol2004;141:737–45.
Belmonte C, Brock J, Viana F. Converting cold into pain. Exp Brain Res2009;196:13–30.
Bini G, Cruccu G, Hagbarth KE, Schady W, Torebjörk E. Analgesic effect of vibrationand cooling on pain induced by intraneural electrical stimulation. Pain1984;18:239–48.
Cairns BE, Hu JW, Arendt-Nielsen L, Sessle BJ, Svensson P. Sex-related differences inhuman pain perception and rat afferent discharge evoked by injection ofglutamate into the masseter muscle. J Neurophysiol 2001;86:782–91.
Casey KL, Zumberg M, Heslep H, Morrow TJ. Afferent modulation of warmthsensation and heat pain in the human hand. Somatosens Mot Res1993;10:327–37.
Clapham DE. TRP channels as cellular sensors. Nature 2003;426:517–24.Craig AD. A new version of the thalamic disinhibition hypothesis of central pain.
Pain Forum 1998;7:1–14.Craig AD. Pain mechanisms: labeled lines versus convergence in central processing.
Annu Rev Neurosci 2003;26:1–30.Davis KD, Kwan CL, Crawley AP, Mikulis DJ. Functional MRI study of thalamic and
cortical activations evoked by cutaneous heat, cold, and tactile stimuli. JNeurophysiol 1998;80:1533–46.
Dyck PJ. Quantitative sensory testing: a consensus report from the PeripheralNeuropathy Association. Neurology 1993;43:1050–2.
Forssell H, Jääskeläinen S, Tenovuo O, Hinkka S. Sensory dysfunction in burningmouth syndrome. Pain 2002;99:41–7.
Gallagher G, Rae CP, Kinsella J. Treatment of pain in severe burns. Am J ClinDermatol 2000;1:329–35.
Greenstein G. Therapeutic efficacy of cold therapy after intraoral surgicalprocedures: a literature review. J Periodontol 2007;78:790–800.
Hagander LG, Midani HA, Kuskowski MA, Parry GJ. Quantitative sensory testing:effect of site and skin temperature on thermal thresholds. Clin Neurophysiol2000;111:17–22.
Halar EM, DeLisa JA, Brozovich FV. Nerve conduction velocity: relationship of skin,subcutaneous and intramuscular temperatures. Arch Phys Med Rehabil1980;61:199–203.
Hardy JD, Goodell H, Wolff HG. The influence of skin temperature upon the painthreshold as evoked by thermal radiation. Science 1951;114:149–50.
Isii Y, Matsukawa K, Tsuchimochi H, Nakamoto T. Ice-water hand immersion causesa reflex decrease in skin temperature in the contralateral hand. J Physiol Sci2007;57:241–8.
Jääskeläinen SK, Teerijoki-Oksa T, Forssell H. Neurophysiologic and quantitativesensory testing in the diagnosis of trigeminal neuropathy and neuropathic pain.Pain 2005;117:349–57.
588 Y. Oono et al. / Clinical Neurophysiology 124 (2013) 581–588
Julius D, Basbaum AI. Molecular mechanisms of nociception. Nature2001;413:203–10.
Kakigi R, Jones SJ. Influence of concurrent tactile stimulation on somatosensoryevoked potentials following posterior tibial nerve stimulation in man.Electroencephalogr Clin Neurophysiol 1986;65:118–29.
Kim H, Neubert JK, San Miguel A, Xu K, Krishnaraju RK, Iadarola MJ, et al. Geneticinfluence on variability in human acute experimental pain sensitivityassociated with gender, ethnicity and psychological temperament. Pain2004;109:488–96.
Klein AH, Sawyer CM, Carstens MI, Tsagareli MG, Tsiklauri N, Carstens E. Topicalapplication of L-menthol induces heat analgesia, mechanical allodynia, and abiphasic effect on cold sensitivity in rats. Behav Brain Res 2010;212:179–86.
Kumar S, Sharma VP, Shukla R, Dev R. Comparative efficacy of two multimodaltreatments on male and female sub-groups with low back pain (part II). J BackMusculoskelet Rehabil 2010;23:1–9.
Lautenbacher S, Roscher S, Strian F. Inhibitory effects do not depend on thesubjective experience of pain during heterotopic noxious conditioningstimulation (HNCS): a contribution to the psychophysics of pain inhibition.Eur J Pain 2002;6:365–74.
Lautenbacher S, Kunz M, Burkhardt S. The effects of DNIC-type inhibition ontemporal summation compared to single pulse processing: does sex matter?Pain 2008;140:429–35.
Lavergne NA. Does application of tea bags to sore nipples while breastfeedingprovide effective relief? J Obstet Gynecol Neonatal Nurs 1997;26:53–8.
Leaper D. Effects of local and systemic warming on postoperative infections. SurgInfect (Larchmt) 2006;7(Suppl. 2):S101–3.
Leff DR, Nortley M, Dang V, Bhutiani RP. The effect of local cooling on painperception during infiltration of local anaesthetic agents, a prospectiverandomised controlled trial. Anaesthesia 2007;62:677–82.
Lewis TY. Observations upon the reactions of the vessels of the human skin to cold.Heart 1930;15:177–208.
Lorentz J, Garcia-Larrea L. Contribution of attentional and cognitive factors to laserevoked potentials. Neurophysiol Clin 2003;33:293–301.
Maruo T, Saitoh Y, Hosomi K, Kishima H, Shimokawa T, Hirata M, et al. Deep brainstimulation of the subthalamic nucleus improves temperature sensation inpatients with Parkinson’s disease. Pain 2011;152:860–5.
Meeusen R, Lievens P. The use of cryotherapy in sports injuries. Sports Med1986;3:398–414.
Melling AC, Leaper DJ. The impact of warming on pain and wound healing afterhernia surgery: a preliminary study. J Wound Care 2006;15:104–8.
Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965;150:971–9.Merskey H, Bogduk N. Classification of chronic pain: descriptions of chronic pain
syndromes and definitions of pain terms. 2nd ed. Seattle: IASP Press; 1994.Muldoon J. Skin cooling, pain and chronic wound healing progression. Br J
Community Nurs 2006;11. S21, S24–5.Nielsen CS, Stubhaug A, Price DD, Vassend O, Czajkowski N, Harris JR. Individual
differences in pain sensitivity: genetic and environmental contributions. Pain2008;136:21–9.
Noël J, Zimmermann K, Busserolles J, Deval E, Alloui A, Diochot S, et al. Themechano-activated K+ channels TRAAK and TREK-1 control both warm and coldperception. EMBO J 2009;28:1308–18.
Oosterveld FG, Rasker JJ. Treating arthritis with locally applied heat or cold. SeminArthritis Rheum 1994;24:82–90.
Pertovaara A, Morrow TJ, Casey KL. Cutaneous pain and detection thresholds toshort CO2 laser pulses in humans: evidence on afferent mechanisms and theinfluence of varying stimulus conditions. Pain 1988;34:261–9.
Popescu A, LeResche L, Truelove EL, Drangsholt MT. Gender differences in painmodulation by diffuse noxious inhibitory controls – a systematic review. Pain2010;150:309–18.
Price DD, McHaffie JG. Effects of heterotopic conditioning stimuli on first andsecond pain: a psychological evaluation in humans. Pain 1988;34:245–52.
Rand SE, Goerlich C, Marchand K, Jablecki N. The physical therapy prescription. AmFam Physician 2007;76:1661–6.
Ristic D, Spangenberg P, Ellrich J. Analgesic and antinociceptive effects of peripheralnerve neurostimulation in an advanced human experimental model. Eur J Pain2008;12:480–90.
Rolke R, Baron R, Maier C, Tölle TR, Treede RD, Beyer A, et al. Quantitative sensorytesting in the German Research Network on Neuropathic Pain (DFNS):standardized protocol and reference values. Pain 2006;123:231–43.
Sessle BJ. Acute and chronic craniofacial pain: brainstem mechanisms of nociceptivetransmission and neuroplasticity, and their clinical correlates. Crit Rev Oral BiolMed 2000;11:57–91.
Sessle BJ. Orofacial pain. In: Merskey H, Loeser JD, Dubner R, editors. The paths ofpain 1975–2005. Seattle: IASP Press; 2005. p. 131–50.
Shepherd JT, Rusch NJ, Vanhoutte PM. Effect of cold on the blood vessel wall. GenPharmacol 1983;14:61–4.
Strigo IA, Carli F, Bushnell MC. Effect of ambient temperature on human pain andtemperature perception. Anesthesiology 2000;92:699–707.
Unruh AM. Gender variations in clinical pain experience. Pain 1996;65:123–67.Willer JC, Le Bars D, De Broucker T. Diffuse noxious inhibitory controls in man
involvement of an opioidergic link. Eur J Pharmacol 1990;182:347–55.Willis WD, Westlund KN. Pain system. In: Paxinos G, Mai JK, editors. The human
nervous system. 2nd ed. San Diego: Elsevier Academic Press; 2004. p. 1125–70.Yarnitsky D. Quantitative sensory testing. Muscle Nerve 1997;20:198–204.Yarnitsky D. Conditioned pain modulation (the diffuse noxious inhibitory control-
like effect): its relevance for acute and chronic pain states. Curr OpinAnaesthesiol 2010;23:611–5.
Yarnitsky D, Kunin M, Brik R, Sprecher E. Vibration reduces thermal pain in adjacentdermatomes. Pain 1997;69:75–7.
Yarnitsky D, Arendt-Nielsen L, Bouhassira D, Edwards RR, Fillingim RB, Granot M,et al. Recommendations on terminology and practice of psychophysical DNICtesting. Eur J Pain 2010;14:339.





























