Embed Size (px)
Citation preview

ANNALS OF SURGERYVol. 221, No. 2, 149-155© 1995 J. B. Lippincott Company
A'e ' A.gR: ,s ._
Laparoscopic AntegradeSphincterotomyA New Technique for the Management ofComplex Choledocholithiasis
Myriam J. Curet, M.D., F.A.C.S., David E. Pitcher, M.D., Daniel T. Martin, M.D., F.A.C.S.,and Karl A. Zucker, M.D., F.A.C.S.
From the Division of Surgical Endoscopy, Department of Surgery, University of New MexicoSchool of Medicine. Albuquerque, New Mexico
ObjectiveLaparoscopic antegrade sphincterotomy represents a new technique that expands the ability ofthe surgeon to manage complex choledocholithiasis at the time of laparoscopic cholecystectomy.The authors describe their experience with six patients with cholelithiasis and complex commonbile duct stone disease who underwent successful laparoscopic cholecystectomy and antegradesphincterotomies.
Summary Background DataPatients with complex choledocholithiasis have represented a technical challenge to the minimallyinvasive surgeon. Recently, a laparoscopic technique of antegrade biliary sphincterotomy hasbeen reported by DePaulo in Brazil. This technique has been successful at clearing the commonbile duct at the time of laparoscopic cholecystectomy.
MethodsLaparoscopic antegrade sphincterotomy was performed in six patients with multiple common bileduct stones. A standard endoscopic sphincterotome was introduced antegrade via the cysticduct or common bile duct and guided through the ampulla. A side-viewing duodenoscope was
used to confirm proper positioning of the sphincterotome. Then a blended current was applieduntil the sphincterotomy was complete.
ResultsThere was no mortality or morbidity associated with laparoscopic antegrade sphincterotomy. Themean additional operative time to complete laparoscopic antegrade sphincterotomy was 19minutes. Three of the six patients were noted to have transient, asymptomatic elevation in serumamylase levels immediately after surgery (average 252 international units/L; normal < 1 15), whichnormalized within 72 hours. The mean postoperative hospital stay was 2.9 days. At a mean follow-up of 5 months (range 1 to 10 months), five patients remain asymptomatic. One individual with
acquired immune deficiency syndrome had persistent symptoms, and a diagnosis ofcytomegalovirus pancreatitis was eventually made.
ConclusionsLaparoscopic antegrade sphincterotomy appears to be a safe and effective technique for the
management of complex biliary tract disease.
149

150 Curet and Others
Laparoscopic cholecystectomy currently is the proce-dure of choice for the majority of patients with symp-tomatic gallbladder disease.13 Decreases in hospital stay,postoperative pain, and recovery time have led to an en-thusiastic acceptance of this technique by the surgicaland patient communities alike. Individuals with com-mon bile duct stones, however, continue to remain achallenge for the minimally invasive surgeon. Choledo-cholithiasis is estimated to be present in 10% to 15% ofallpatients undergoing cholecystectomies.2'46 Currently, ifcommon bile duct stones are suspected preoperatively,most patients are advised to undergo endoscopic retro-grade cholangiography. If stones are identified, an endo-scopic sphincterotomy and stone extraction usually areperformed to clear the common bile duct before laparo-scopic intervention. 1,7-11A continuing dilemma has been the treatment ofcom-
mon bile duct stones detected for the first time at laparo-scopic surgery. This situation is estimated to occur inmore than 50% of patients with choledocholithiasis andin approximately 3% to 5% of all patients undergoingcholecystectomy.2 5 810 12 Ifcommon bile duct stones arediscovered at the time oflaparoscopy, a number of treat-ment modalities are available. In many cases, the proce-dure is converted to open laparotomy and formal com-mon bile duct exploration. Some authors recently haveadvocated laparoscopic exploration of the common bileduct.2'3'8 Unfortunately, in those patients with multiplebile duct stones, stones within the proximal ducts or cal-culi impacted at the ampulla, the current methods oflap-aroscopic stone retrieval are limited and may signifi-cantly prolong the operative procedure. In selected pa-tients, some surgeons have advocated completing thelaparoscopic cholecystectomy and performing postoper-ative endoscopic retrograde cholangiography.3-8"13 Thisapproach, however, increases both the cost and timeneeded for complete management of choledocholithi-asis. In addition, biliary endoscopy itself is associatedwith a 5% to 10% incidence of major complications anda 1% to 3% mortality rate.4"15"16
Recently, a laparoscopic technique of performingantegrade biliary sphincterotomy has been reported byDePaulo in Brazil.'7 This procedure expands the abilityofthe surgeon to provide definitive management ofbothcholelithiasis and choledocholithiasis at the time of lap-aroscopic surgery. In this report, we describe our experi-ence with six patients with cholelithiasis and complexcommon bile duct disease who underwent successful lap-
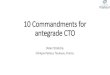
Figure 1. lntraoperative cholangiogram demonstrating multiple small andlarge common bile duct stones.
aroscopic cholecystectomies and antegrade sphinctero-tomies.
METHODS AND MATERIALS
Six patients underwent both laparoscopic cholecystec-tomies and antegrade sphincterotomies. The mean agewas 41 years (range 16 to 74 years), and four of the pa-tients were women. One individual was operated on elec-tively for a history ofbiliary colic and cholelithiasis dem-onstrated on abdominal ultrasonography. Preoperativeexamination and laboratory values were normal, exceptfor mildly elevated liver transaminases (alanine transam-inase = 276 international units/L [normal = 5-35] andgamma-glutamyl transferase = 438 international units/L [normal = 5-85]). Intraoperative cholangiography re-vealed multiple large and small stones in the distal com-mon bile duct (Fig. 1). Transcystic choledochoscopicstone extraction was attempted, but the stones frag-mented easily and could not be retrieved. Two patientswere admitted with clinical diagnoses of acute cholecys-titis and were taken to the operating room within 48hours. Multiple common bile duct stones were seen onthe intraoperative cholangiograms, and in one of thesepatients, there was evidence of one or more stones im-pacted at the ampulla. Two other patients were admittedwith clinical and biochemical manifestations ofgallstonepancreatitis (elevated serum amylase and lipase). Ultra-sonography revealed cholelithiasis and dilated commonbile ducts (>10 mm) in both individuals. After clinicalresolution of their pancreatitis and during the same hos-pitalization, they were taken to the operating room forlaparoscopic cholecystectomy and intraoperative cho-
Address reprint requests to Karl A. Zucker, M.D., F.A.C.S., Depart-ment of Surgery, University of New Mexico, School of Medicine,221 1 Lomas Blvd. NE, Albuquerque, NM 87131.
Accepted for publication May 7, 1994.
Ann. Surg. * February 1995

Laparoscopic Antegrade Sphincterotomy 151
langiography. Intraoperative cholangiography revealedmultiple common bile duct stones in both patients and apresumed stone impaction at the ampulla in one indi-vidual. One patient with acquired immune deficiencysyndrome was admitted with a diagnosis ofrecurrent epi-gastric pain and pancreatitis. An abdominal ultrasoundrevealed cholelithiasis and a 4.0- to 5.0-mm commonbile duct. An endoscopic retrograde cholangiopancrea-tography was performed that demonstrated a normalpancreatic duct and an abrupt cut-off of the left hepaticduct. After an extensive work-up, the diagnosis of gall-stone pancreatitis and possible acquired immune defi-ciency syndrome-related cholangiopathy was made.'8Previous authors have reported improvement of biliarytract symptoms after sphincterotomy'8 in such individu-als, and therefore, the patient was taken to the operatingroom for planned laparoscopic cholecystectomy andantegrade sphincterotomy.
TECHNIQUELaparoscopic cholecystectomy was performed using
the four-puncture technique described by Reddick.'9 Af-ter identifying the juncture of the gallbladder and cysticduct, an intraoperative cholangiogram was performedroutinely. Ifone or more defects suggesting choledochol-ithiasis were observed, an attempt was made at transcys-tic choledochoscopy and stone extraction. A small (outerdiameter 3.1 mm) flexible choledochoscope (URF-P2Choledochoscope; Olympus Corp., Japan) was intro-duced through one of the right lateral 5.0-mm laparo-scopic cannulas. In most cases, the choledochoscopecould be inserted through the opening created previouslyin the cystic duct for cholangiography. The scope thenwas maneuvered into the proximal and distal bile ducts(Fig. 2A). In one patient, a large stone was impacted atthe juncture of the cystic and common bile ducts, whichprevented passage of the choledochoscope. Then theopening in the cystic duct was continued down onto thecommon bile duct until the stone could be removed.This maneuver allowed for direct passage of the choled-ochoscope into the bile ducts (Fig. 2B). If one or morestones were visualized, a four-wire basket was passedthrough the working channel of the choledochoscopeand positioned around the calculus. The small diameter(1.1 mm) of the working channel did not allow for thedirect retrieval of stones; instead, the choledochoscopewas withdrawn completely from the peritoneal cavity aseach stone was secured within the wire basket. Indica-tions for proceeding with antegrade sphincterotomy in-cluded multiple common bile duct stones, calculi im-pacted at the ampulla or inability to remove all of thestones within the bile ducts.A standard endoscopic papillotome (Microvasive Ul-
AJ.::.J
B a. -S_
l.S.:.~~~~~
A~~~~~~~~~~~~~~~2. ... .. . ....@.
....
}: ^s
e j
.:
.9v..,. s_ -iN ___ -t \
a.v At
*:
B
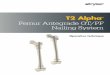
Figure 2. (A) In most patients a small, flexible choledochoscope can beguided through an opening made in the cystic duct and then maneuveredinto the common bile duct. (B) If the transcystic approach is unsuccessful,an incision can be made in the common bile duct to allow direct insertionof the choledochoscope.
tratome with a 30-mm wire; Watertown, MA.) was ma-neuvered antegrade through the cystic duct and into thecommon bile duct. A side-viewing video duodenoscope
Vol. 221 * No. 2

152 Curet and Others
Figure 3. A schematic drawing demonstrating the side-viewing endo-scope positioned within the duodenum, which is used to visualize thesphincterotome.
(Olympus JF 100) was passed orally, and the ampullawas visualized. The sphincterotome then was guidedthrough the ampulla, and the diathermic wire was ma-neuvered into the appropriate 12 o'clock position (Fig.3). In two individuals, the sphincterotome could not bepassed into the duodenum because ofstone impaction atthe ampulla. In these patients, a guide wire was insertedthrough the working channel of the choledochoscopeand advanced into the duodenum under direct vision(Fig. 4). Then the choledochoscope was removed, andthe sphincterotome was passed over the wire. A sphinc-terotomy was performed using a blended electrical cur-rent and extended proximally to the first transverse foldof the ampulla (Fig. 5). In most cases, the stones thenpassed into the duodenum spontaneously or with gentleirrigation. After successful sphincterotomy, repeatcholedochoscopy was performed to ensure that all stoneshad been passed (Fig. 6). If common bile duct explora-tion and passage ofthe sphincterotome were done via thecystic duct, a T tube or similar ductal drainage catheterwas not used, and the cystic duct stump was secured sim-ply with a pre-tied laparoscopic ligature.5 Ifthe commonbile duct was incised and directly instrumented, it wasclosed around a 14- to 16-French T tube, with the end ofthe catheter brought through the right lateral trocar site.Then laparoscopic cholecystectomy was completed.
RESULTSLaparoscopic antegrade sphincterotomy was com-
pleted successfully in all six patients. There was no oper-ative-related morbidity or mortality, and the mean post-
operative stay was 2.9 days (range 2 to 5 days). Threepatients were had transient elevation in serum amylase(average 252 international units/L; normal = <1 15 in-ternational units) immediately after surgery. None ofthese patients manifested clinical signs of pancreatitis orexperienced any delay in discharge from the hospital. Inall cases, the serum amylase levels returned to normalwithin 72 hours of surgery.
Five of the six patients remain asymptomatic fromtheir biliary tract disease after a mean follow-up of 5months (range 1 to 10 months). The individual with sus-pected acquired immune deficiency syndrome-relatedcholangiopathy continues to have recurrent episodes ofepigastric pain and hyperamylasemia. At the time of sur-gery, this patient was found to have both cholelithiasisand multiple small (<2.0 mm in diameter) common bileduct stones. Despite a successful biliary drainage proce-dure, his symptoms have persisted. Continued work-uphas revealed a probable diagnosis of cytomegaloviruspancreatitis, and the patient currently is being treatedwith antiviral medications.
DISCUSSIONAlthough laparoscopic cholecystectomy has been ac-
cepted as the gold standard for the treatment of symp-tomatic cholelithiasis," 2 there continues to be debate asto the most appropriate method to manage those pa-tients with concomitant choledocholithiasis.3 4'7-9"13'20 Atfirst, common bile duct stones were believed to be a con-traindication to attempting laparoscopic cholecystec-tomy. '8 Patients who presented with jaundice or evi-dence of choledocholithiasis on ultrasound often wouldundergo preoperative biliary endoscopy.3'6'7 A numberof recent studies, however, have shown that 50% or moreof these patients will have a normal preoperative endo-scopic retrograde cholangiography, putting a significantproportion of patients through an unnecessary invasiveand expensive procedure.3'8'9Another continuing dilemma concerns the manage-
ment of patients who are found to have choledocholithi-asis at the time of laparoscopic surgery. Five to ten per-cent of patients undergoing laparoscopic cholecystec-tomy are found to have unsuspected common bile ductstones.24-6 12 Until recently, most of these operationswere converted to formal laparotomy so that the surgeoncould perform an open common bile duct exploration.The dramatic benefits of minimally invasive surgeryhave persuaded many surgeons to attempt definitivetherapy of both gallstones and choledocholithiasis at thetime of laparoscopic intervention. Various methods ofaccessing the bile ducts during laparoscopic surgery havebeen explored.2'3'5'81 The opening in the cystic ductthrough which the cholangiogram is obtained may be en-
Ann. Surg. * February 1995

Laparoscopic Antegrade Sphincterotomy 153
Figure 4. Duodenoscopic view of a guide wire that has been maneL-vered through the distal common bile duct and ampulla (,top lehtt
Figure 5. After proper positioning of the diathernmic wire a sptnictero-tomy is performec 'top right)
Figure 6. After antegraoe sprntncterotomy. the croledocnoscoce easilytraverses the ampulla (bottom left).
larged so that various endoscopic devices (wire baskets,biliary balloon catheters, etc.) can be maneuvered intothe main bile ducts under fluoroscopic guidance for re-trieval of stones.2 5'8 Others have preferred to use small,flexible choledochoscopes that can be maneuvered intothe biliary tree and allow for direct visualization of theducts.2'3 5 Although laparoscopic common bile duct ex-ploration is often successful in managing individualswith one or only a few stones floating free in the distalcommon bile duct, there are many patients, such as thosewith multiple stones or stones impacted in the distalduct, who may require extensive instrumentation of theducts or even a biliary drainage procedure. Although pre-operative or postoperative endoscopic retrograde sphinc-terotomy has been shown to be a safe and effectivemethod ofmanaging all ofthese problems, most physici-ans would prefer to avoid performing additional expen-sive and invasive procedures on patients scheduled toundergo a surgical procedure.7' 4l'6,20,21 In an attempt toperform definitive management ofbiliary tract disease atthe time of surgery, some physicians have attempted to
perform intraoperative endoscopic retrograde cholangi-ography. Unfortunately this has not proven to be feasi-ble, because retrograde cannulation of the bile duct canbe very difficult to perform in the operating room be-cause the patient is in the supine position, rather than thetypical prone position, and excessive distension of thesmall bowel must be avoided. As a result, the likelihoodof successful bile duct cannulation and sphincterotomyis lower, and the operative procedure and anesthesiatime are prolonged dramatically.5 7"17 In contrast, laparo-scopic-assisted antegrade sphincterotomy has proven tobe a rapid and effective means of enhancing biliarydrainage and clearing the bile ducts. Although proper po-sitioning of the sphincterotome still is confirmed with aside-viewing duodenoscope, it has proven relatively easyto simply confirm placement of the diathermic cuttingwire. Antegrade passage of the sphincterotome throughthe common bile duct and ampulla is performed rapidlycompared with retrograde cannulation, which often cantake several hours in patients with papillary stenosis, im-pacted calculi, or duodenal diverticula. Many of the
Vol. 221 * No. 2

154 Curet and Others
problems associated with retrograde biliary endoscopy,such as pancreatitis resulting from cannulation of thepancreatic duct, creation of false passages, and duodenalperforation, should be reduced because it is much easierto pass the sphincterotome antegrade through the bileducts. In our series, only three of our six patients werefound to have asymptomatic and transient hyperamy-lasemia postoperatively (mean 252 international units/L; normal = < 1 15). In all cases, serum enzyme levelsreturned to normal within 3 days, and no clinical mani-festations ofpancreatitis were evident. Mild elevations inserum amylase and lipase also have been reported withroutine cholangiography and common bile duct explo-ration.'7The success rate ofantegrade sphincterotomy in clear-
ing the common bile duct of all calculi also should com-pare favorably with that of retrograde biliary endoscopy(90%-95% duct clearance rate).7,14-'6'21 Therefore, ante-grade sphincterotomy should improve the success ratereported for laparoscopic common bile duct explorationalone (70%-90% duct clearance rate).8 In our series, wewere able to clear the common bile duct in all six pa-tients, despite the fact that these cases represented themost difficult to manage under laparoscopic guidance.
Because this is a new procedure, the indications forlaparoscopic antegrade sphincterotomy still are underinvestigation. DePaulo has advocated this procedure forpatients with multiple common bile duct stones, stonesimpacted at the ampulla, and in those individuals withdilated common bile ducts and impaired biliary drainage(i.e., papillary stenosis).'7 In this series, the predominantindications for antegrade sphincterotomy were multiplebile duct stones or stones impacted at the ampulla. Al-though laparoscopic common bile duct exploration maybe attempted in such cases, the procedure often can beprolonged because each stone must be retrieved individ-ually. In many cases, it may prove impossible to com-pletely clear the ducts of all stones and debris, especiallyif calculi are present within the more proximal ducts. Inaddition, a T tube or other biliary drainage catheter oftenis necessary because ofthe extensive instrumentation re-quired. In our experience, antegrade sphincterotomy hasproven to be a safe and rapid method of completelyclearing the bile duct in these individuals. After access tothe common bile duct had been achieved, it took only amean of 19 minutes to perform antegrade sphinctero-tomy. Because the sphincterotomy provides for adequatebiliary drainage, a T tube was not used, except in the onepatient in whom the common bile duct was incised andmanipulated extensively.
Initially, it was difficult to mobilize the additionalequipment to perform intraoperative endoscopy becauseour hospital did not keep a side-viewing duodenoscopein the operating room. Therefore, a portable biliary en-
Ann. Surg. * February 1995
doscopy cart was established that can be transportedfrom the endoscopy suite to the operating room within afew minutes. Biliary endoscopy is preformed routinelyby the surgical service at this institution, so it was rela-tively easy for us to perform the necessary intraoperativeendoscopy (i.e. placement of the side-viewing duodeno-scope). Unfortunately a side-viewing duodenoscope stillis required to visualize the ampulla and position thesphincterotome. This instrument is somewhat moredifficult to maneuver than the standard forward-viewingendoscopes, and specialized training with manipulatingthese devices and in performing sphincterotomy is ad-vised before attempting this procedure. As our confi-dence with this technique has grown, we have reduceddramatically the number of patients with abnormal pre-operative liver function tests or dilated ducts on ultra-sound who are advised to undergo preoperative biliaryendoscopy. Therefore, we have avoided performing aseparate invasive and expensive procedure on many ofour patients. In addition, our patients have indicated apreference to have simultaneous treatment of both cho-lelithiasis and choledocholithiasis at the time of opera-tive intervention rather than undergo two separate pro-cedures.
CONCLUSIONSThe complete management of patients with common
bile duct stones in this new era of laparoscopic biliarytract surgery still is under investigation. More thanlikely, no one method ofmanagement will be successfulfor all individuals with simple or complex choledocholi-thiasis. Options will include biliary endoscopy (preoper-ative and postoperative), formal laparotomy, and opencommon bile duct exploration and laparoscopic man-agement. The evolution of laparoscopic antegradesphincterotomy appears to give surgeons another optionin the management of complex choledocholithiasis.Antegrade sphincterotomy is one of many reasons it isbecoming increasingly important for general surgeons tobecome proficient at flexible endoscopy. The role of the"surgical endoscopist" is a new and emerging conceptthat requires said surgeon to have a full armamentariumof laparoscopic and endoscopic techniques.
References1. Schirmer BD, Edge SB, Dix J, et al. Laparoscopic cholecystectomy
treatment ofchoice for symptomatic cholelithiasis. Ann Surg 1991;213:665-676.
2. Petelin JB. Laparoscopic approach to common duct pathology.Surg Laparosc Endosc 1991; 1:33-41.
3. Pitcher DE, Martin DT, Zucker KA. Laparoscopic and endoscopicmanagement of common bile duct stones. Curr Opin Surg 1994:203-207.

Vol. 221 * No. 2
4. Petelin JB. Laparoscopic approach to common duct pathology.Am J Surg 1993; 165:487-491.
5. Zucker KA, Bailey RW. Laparoscopic cholangiography and man-agement of choledocholithiasis. In Zucker KA, ed. Surgical Lapa-roscopy Update. St. Louis, MO: Quality Medical Publishing, 1993,pp 145-193.
6. NIH Consensus Conference Statement. Am J Surg 1993; 165:390-396.
7. Cotton PB. Endoscopic retrograde cholangiopancreatography andlaparoscopic cholecystectomy. Am J Surg 1993; 165:474-478.
8. Hunter JG. Laparoscopic transcystic common bile duct explora-tion. Am J Surg 1992; 163:53-58.
9. Stiegmann GV, Goff JS, Mansour A, et al. Pre-cholecystectomyendoscopic cholangiography and stone removal is not superior tocholecystectomy, cholangiography and common duct exploration.Am J Surg 1992; 163:227-230.
10. Flowers JL, Zucker KA, Graham SM, et al. Laparoscopic cholan-giography: results and indications. Ann Surg 1992; 215:209-216.
11. Morris JB, Margolis R, Rosato EF. Safe laparoscopic cholecystec-tomy without intraoperative cholangiography. Surg Laparosc En-dosc 1993; 3:17-20.
12. Gerber A, Apt MK. The case against routine operative cholangiog-raphy. Am J Surg 1982; 143:734-736.
Laparoscopic Antegrade Sphincterotomy 155
13. Traverso LW, Kozarek RA, Ball TJ, et al. Endoscopic retrogradecholangiopancreatography after laparoscopic cholecystectomy.Am J Surg 1993; 165:581-586.
14. Reiter JJ, Bayer HP, Menncken C, et al. Results of endoscopicpapillotomy: a collective experience from nine endoscopic centersin West Germany. World J Surg 1978; 2:505-511.
15. Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphinctero-tomy complications and their management: an attempt at consen-sus. Gastrointest Endosc 1991; 37:383-393.
16. Cotton PB. Non-operative removal of bile duct stones by duode-noscopic antegrade sphincterotomy. Br J Surg 1980; 67:1-5.
17. DePaulo AL, Hashiba K, Bafutto M, et al. Laparoscopic antegradesphincterotomy. Surg Laparosc Endosc 1993; 3:157-160.
18. Benhamou, Caumer E, Gerosa Y, et al. AIDS-related cholangiog-raphy. Dig Dis and Science 1993; 38:1113-1118.
19. Reddick EJ, Olsen DO. Laparoscopic laser cholecystectomy: acomparison with mini-laparotomy. Surg Endosc 1989; 3:44-48.
20. Van Stiegmann G, Pearlman NW, GoffJS, et al. Endoscopic cho-langiography and stone removal prior to cholecystectomy. ArchSurg 1989; 124:787-790.
21. Leese T, Neoptolemos JP, Carr-Locke DL. Successes, failures,early complications and their management following endoscopicsphincterotomy: results in 394 consecutive patients from a singlecenter. Br J Surg 1985; 72:215-219.














![Transformation recognises organisations TRANSFORMATION ...docs.awardbase.com.au/aba2020/2020_ABA_Digital_Transformation… · [DTR] 00 ETRY GIDEIES E C M Powered by EMPLOYER OFCHOICE](https://img.pdfslide.net/doc/110x75/5e9fbd9f14c55161eb3905bb/transformation-recognises-organisations-transformation-docs-dtr-00-etry-gideies.jpg)











