Embed Size (px)
Citation preview

• Email : [email protected]
• Fanpage :
• Catatan Nury
• Nury’s keynotes
• Weblogs :
• http://nury-nus.blogspot.com
• http://rehab-med.blogspot.com
• http://rehab-med-
research.blogspot.com
• http://tanpa-pita-suara.blogspot.com
• http://laryngectomees.blogspot.com
Dr. dr. Nury Nusdwinuringtyas, SpKFR-K, M.Epid
Adequate Cardiorespiratory Rehabilitation in Pulmonary Problems
Mucus Clearance
The 7th Jakarta International Chest and Critical Care Internal Medicine
2019

INTRODUCTION
• Mucus secretion and clearance are important for pulmonary defense.
• Mucus secretion volume is between 10 and 100 mL/day in health.
• Pulmonary disorders such as CF, COPD, bronchiectasis alter the production of mucus and mucociliary clearance disorders airway obstruction.
• ACT used to aid in mucus mobilization and expectoration.
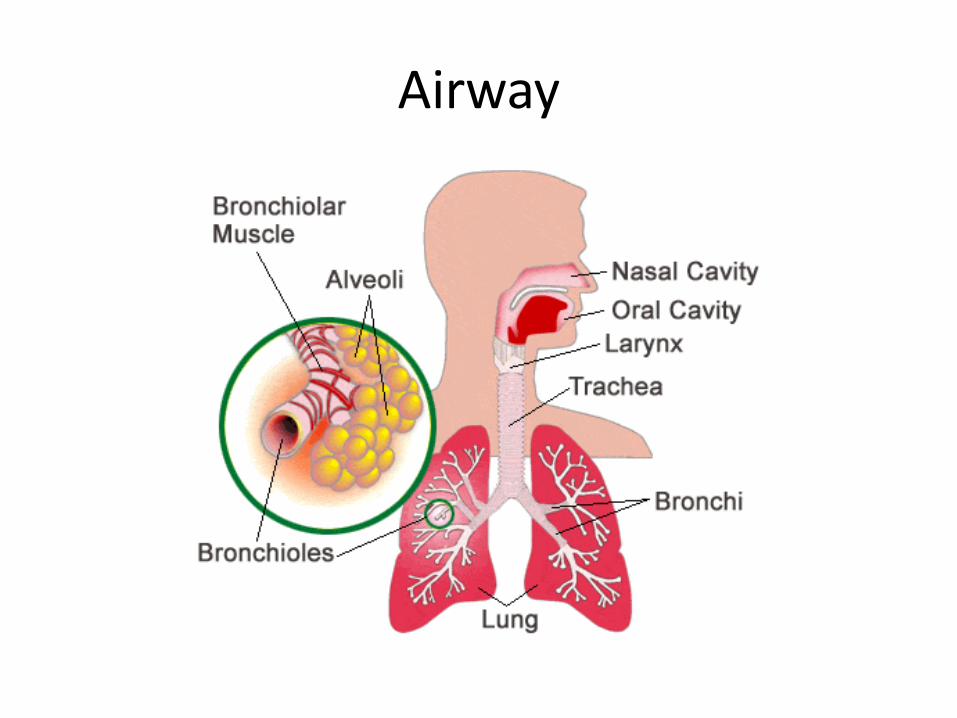
Airway
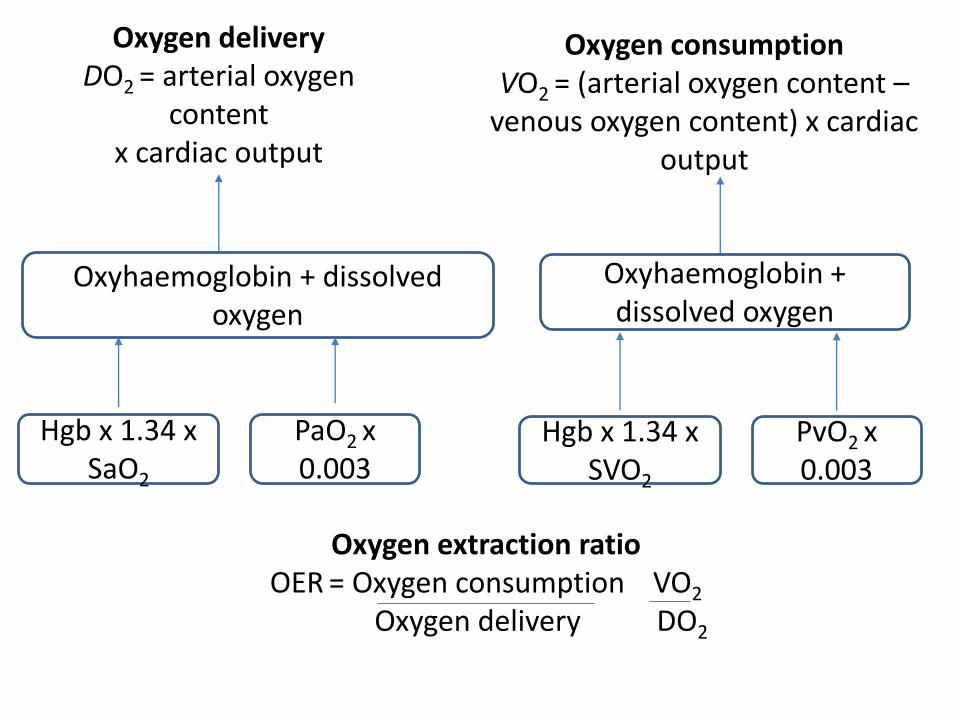
Oxygen consumptionVO2 = (arterial oxygen content –
venous oxygen content) x cardiac output
Oxygen deliveryDO2 = arterial oxygen
contentx cardiac output
Oxyhaemoglobin + dissolved oxygen
Hgb x 1.34 x SaO2
PaO2 x 0.003
Oxyhaemoglobin + dissolved oxygen
Hgb x 1.34 x SVO2
PvO2 x 0.003
Oxygen extraction ratioOER = Oxygen consumption VO2
Oxygen delivery DO2
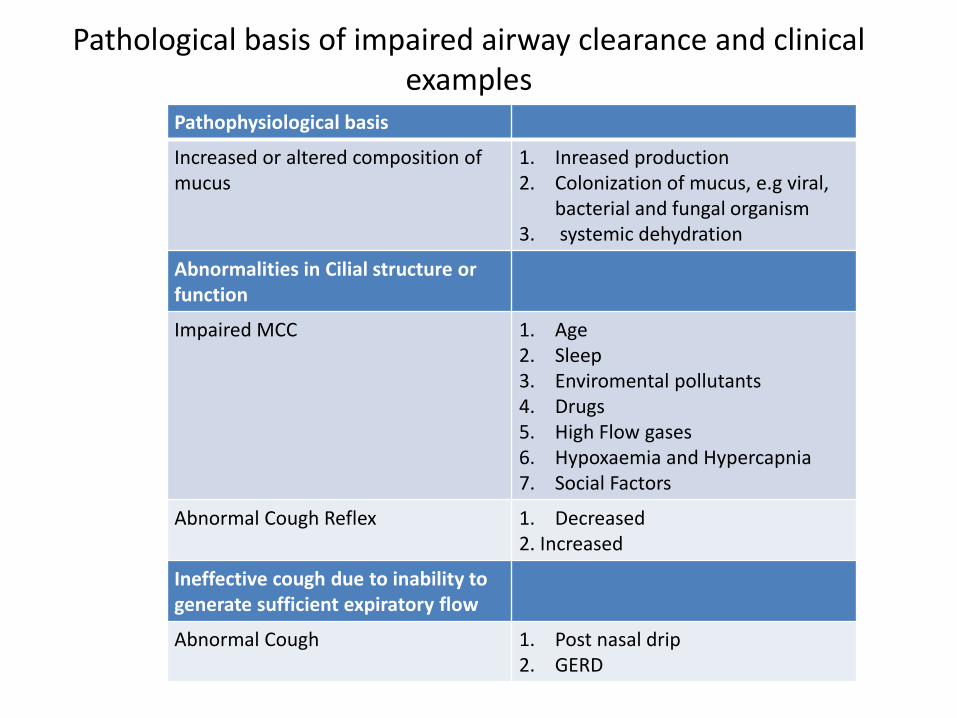
Pathological basis of impaired airway clearance and clinical examples
Pathophysiological basis
Increased or altered composition of mucus
1. Inreased production2. Colonization of mucus, e.g viral,
bacterial and fungal organism3. systemic dehydration
Abnormalities in Cilial structure or function
Impaired MCC 1. Age2. Sleep3. Enviromental pollutants4. Drugs5. High Flow gases6. Hypoxaemia and Hypercapnia7. Social Factors
Abnormal Cough Reflex 1. Decreased2. Increased
Ineffective cough due to inability to generate sufficient expiratory flow
Abnormal Cough 1. Post nasal drip2. GERD
Airway clearance in the normal lung
1. Mucociliary clearance (MCC)
1. Cough

MUCOCILIARY CLEARANCE
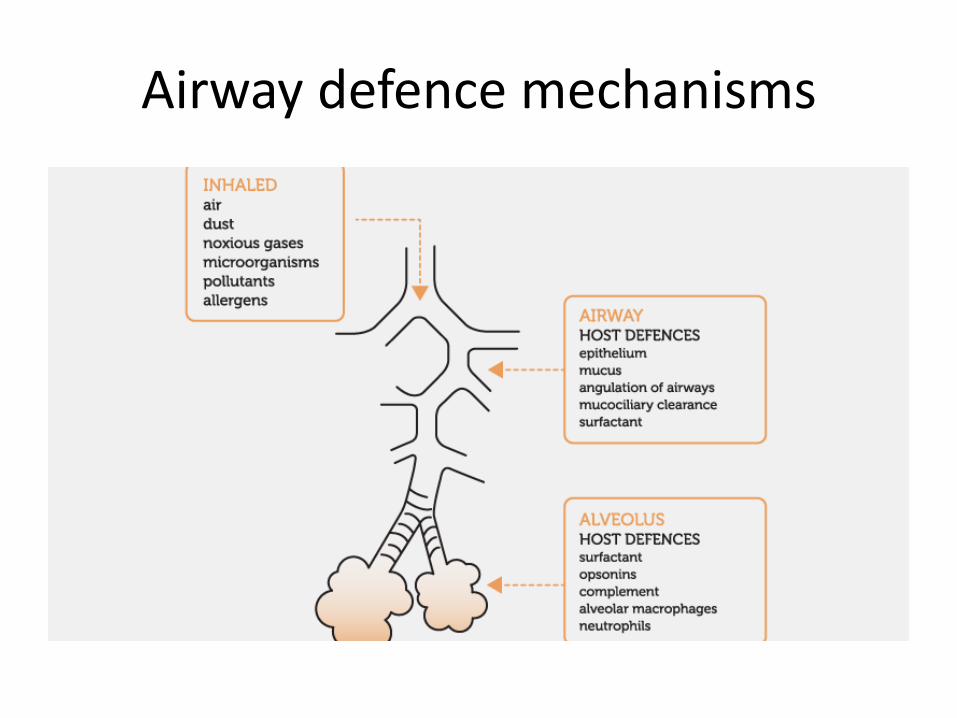
Airway defence mechanisms
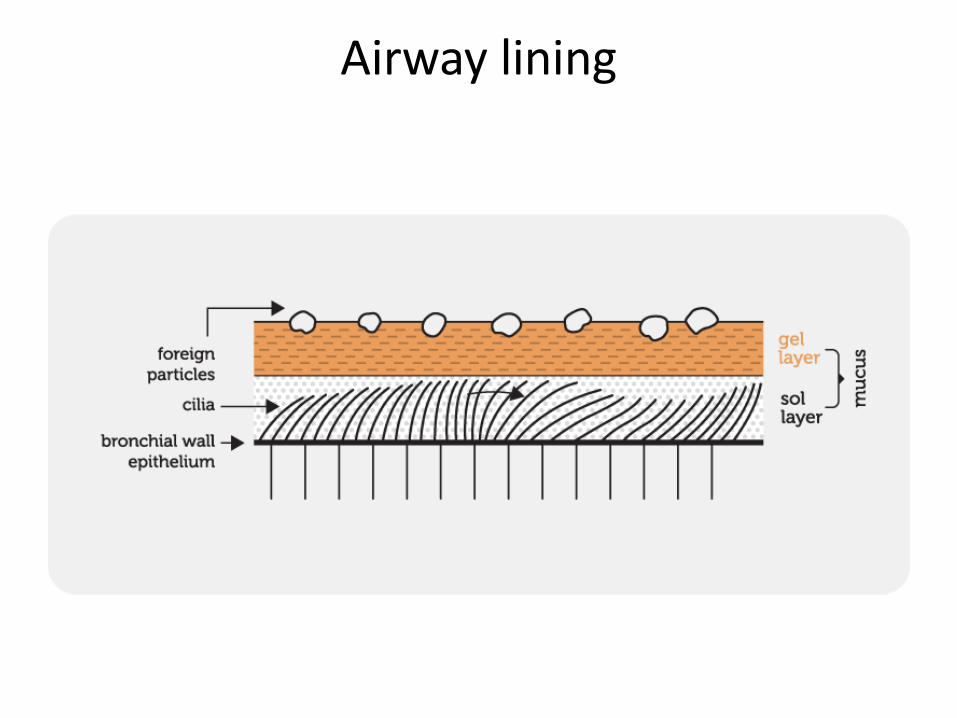
Airway lining
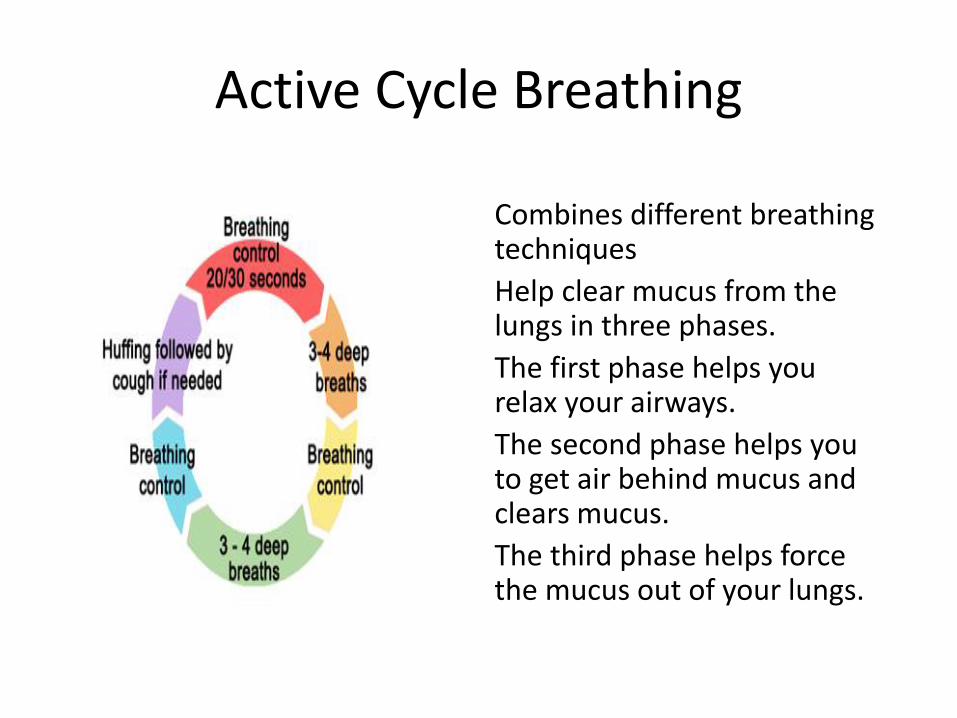
Active Cycle Breathing
Combines different breathing techniques
Help clear mucus from the lungs in three phases.
The first phase helps you relax your airways.
The second phase helps you to get air behind mucus and clears mucus.
The third phase helps force the mucus out of your lungs.
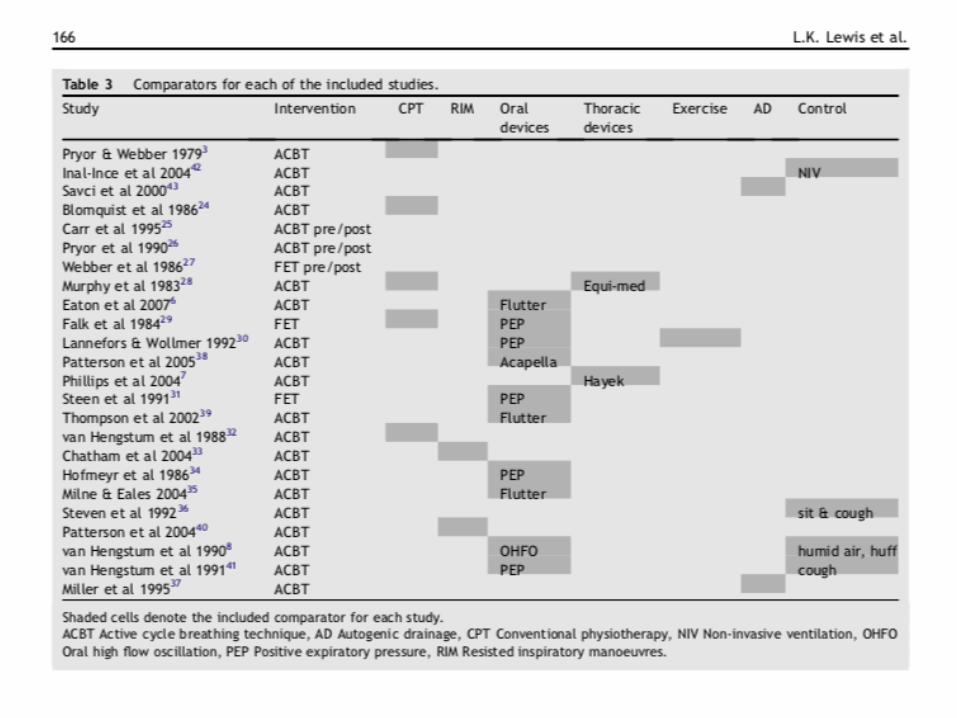
Discussion
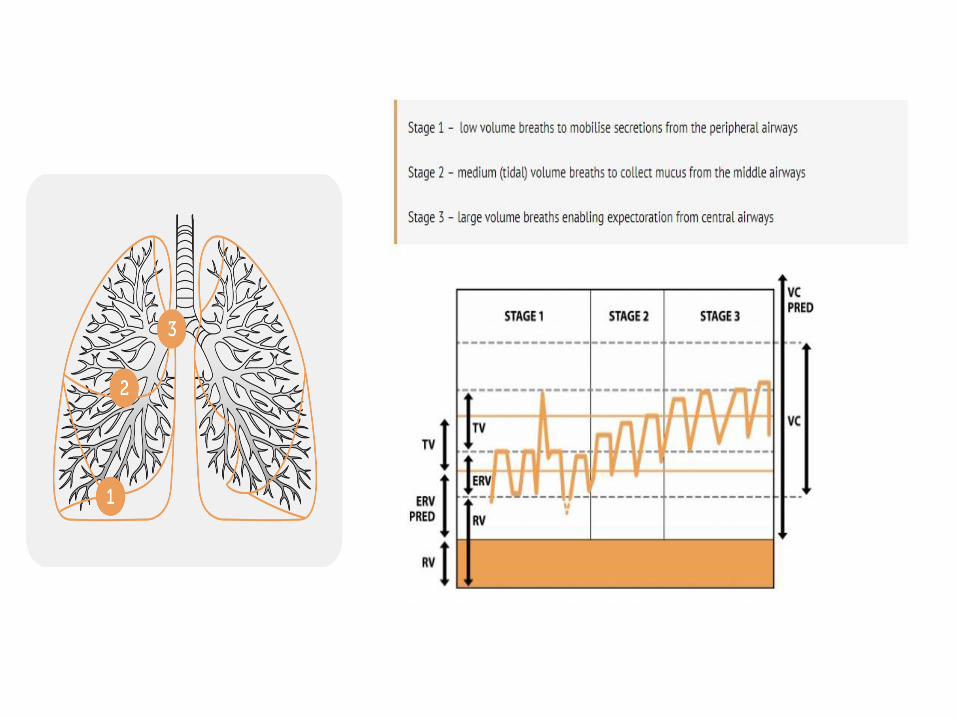
Autogenic Drainage
Is a breathing technique aims to maximize airflow within the airways, to improve ventilation and the clearance of mucus.
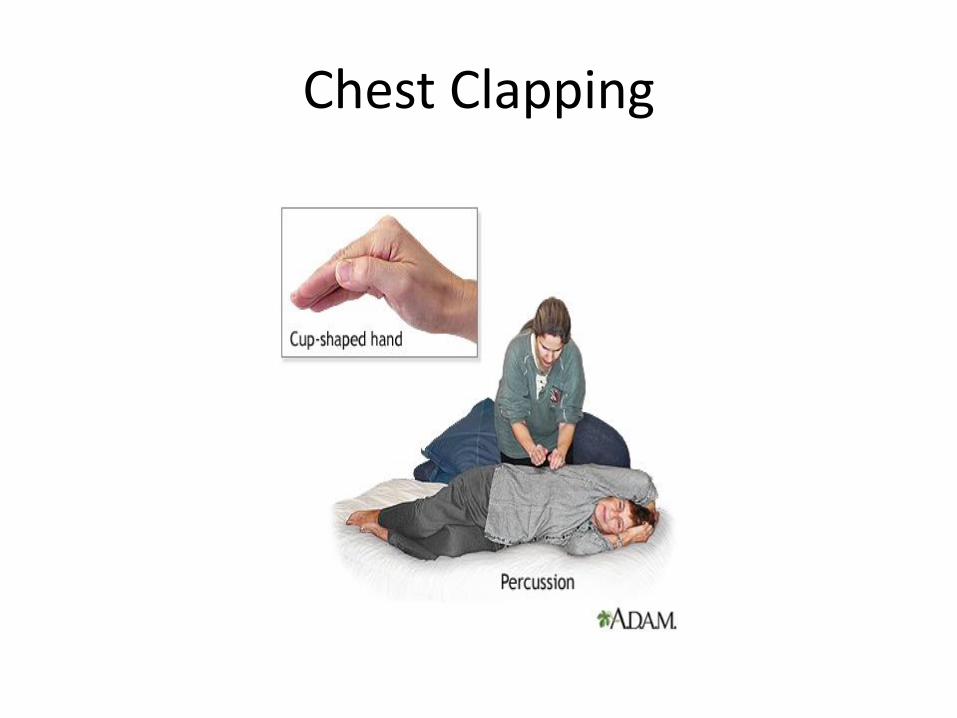
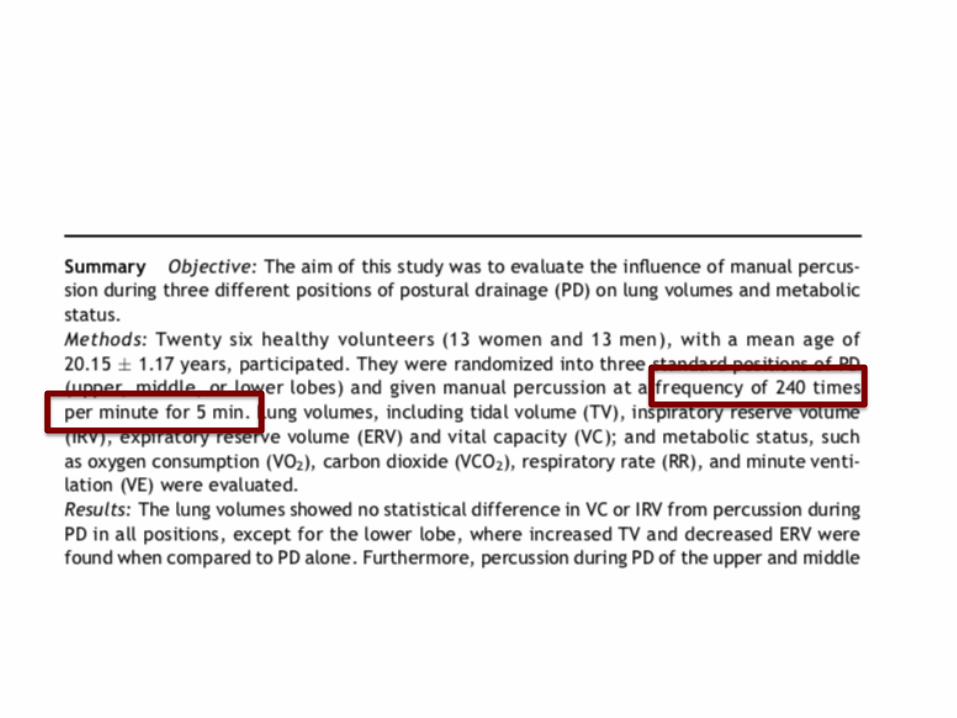
Chest Clapping
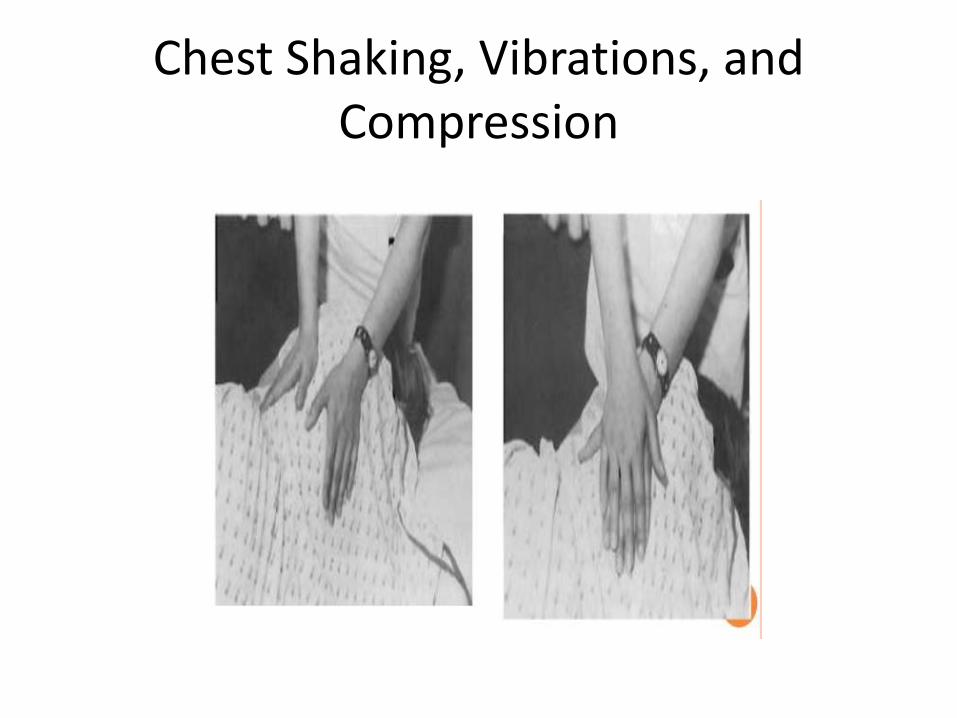
Chest Shaking, Vibrations, and Compression
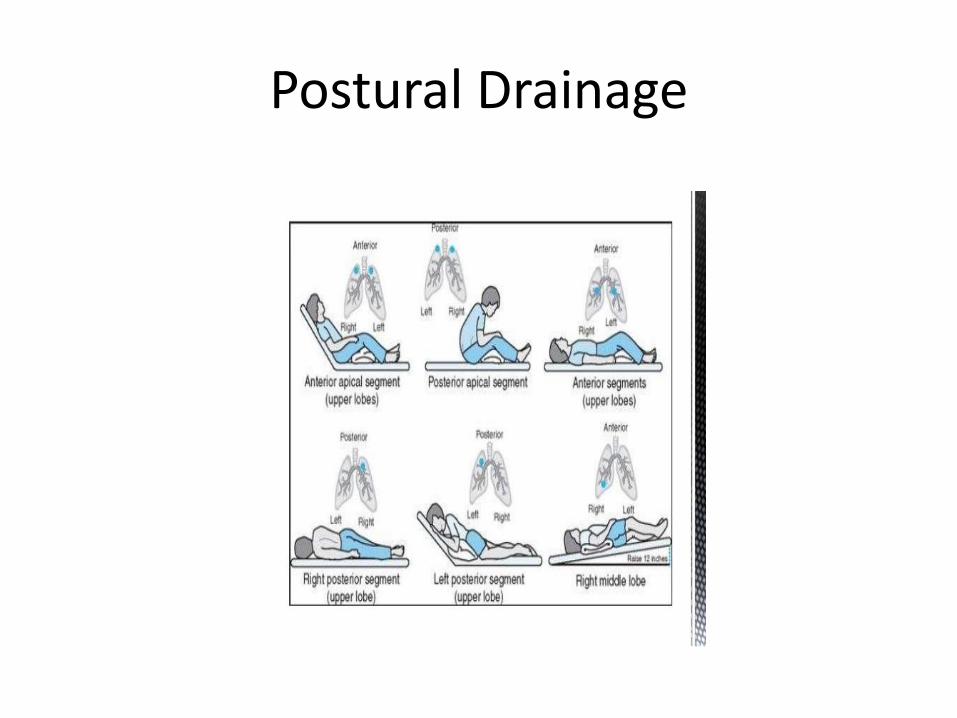
Postural Drainage
Contraindications to Postural Drainage
• Severe hemoptysis
• Severe pulmonary edema
• CHF
• Large pleural effusion
• Aortic aneurysm
• Cardiac arrhythmia
• Severe hypertension
• Unstable angina

DEVICES
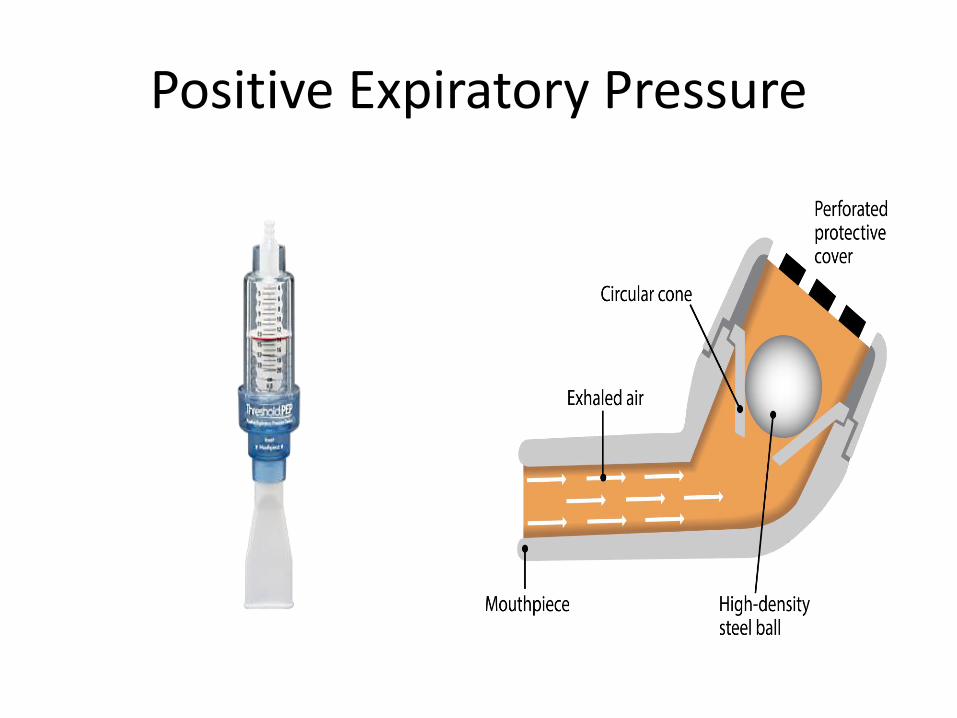
Positive Expiratory Pressure
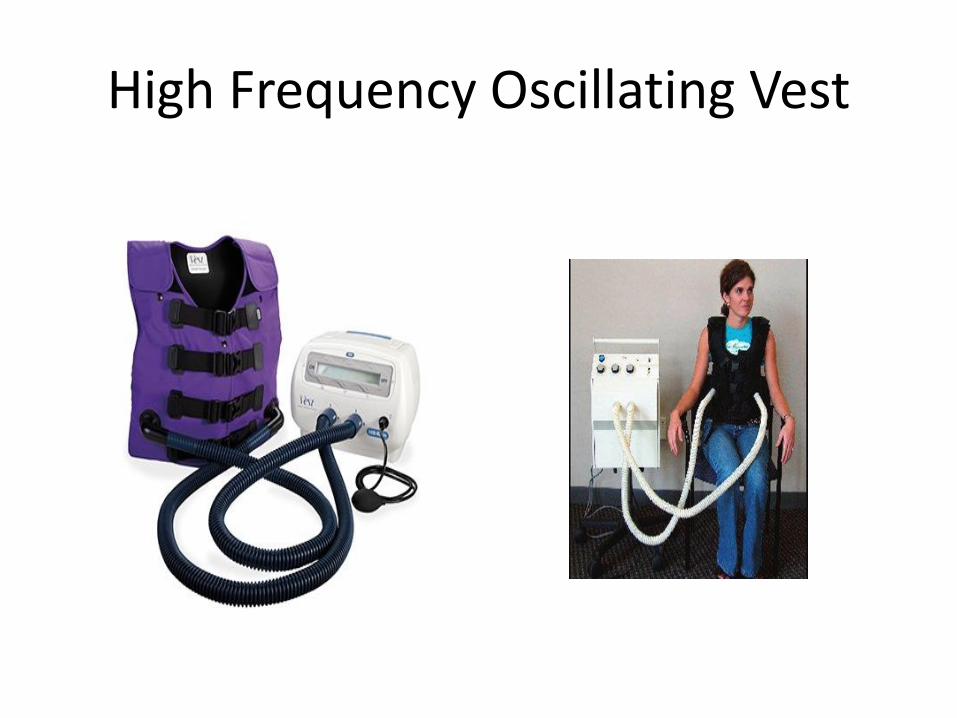
High Frequency Oscillating Vest
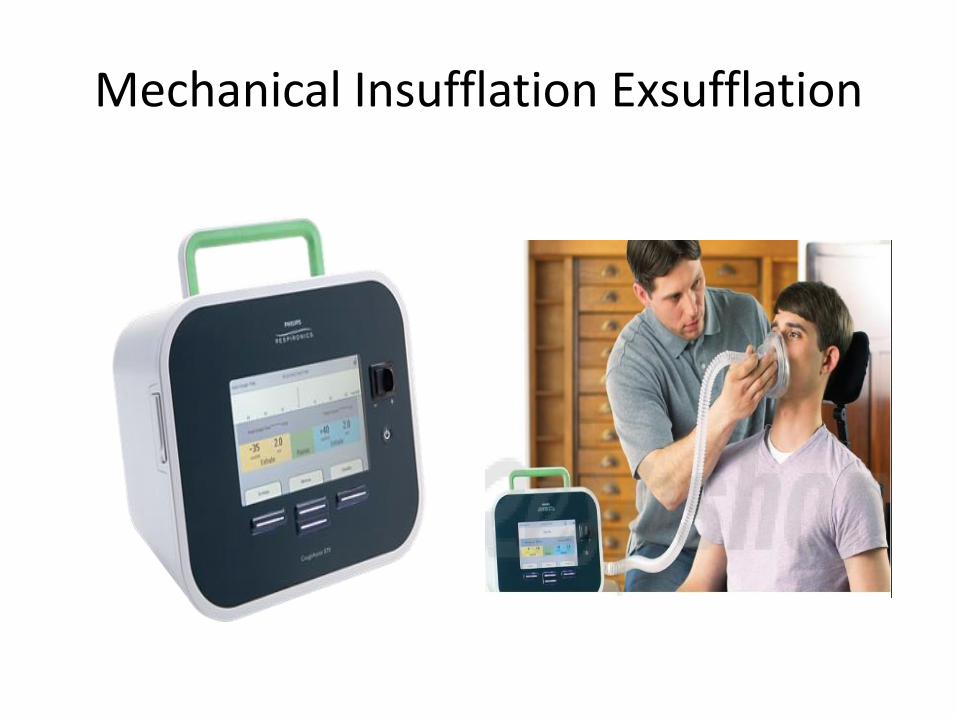
Mechanical Insufflation Exsufflation
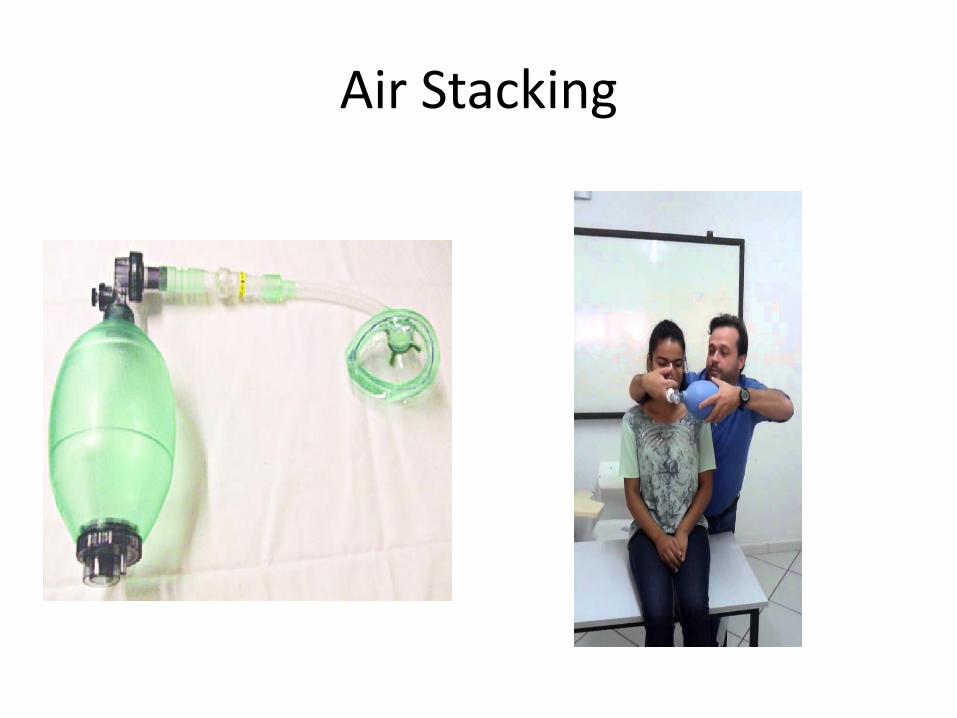
Air Stacking
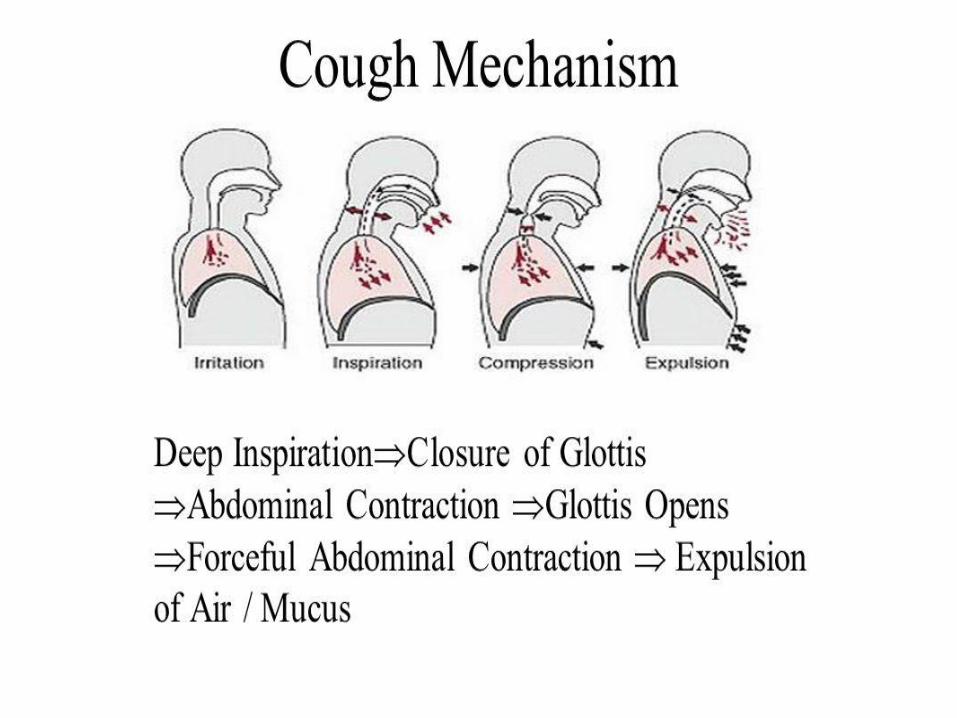
COUGH
Contraindications Cough Assist
• History of bullous emphysema
• Pneumothorax
• Barotrauma
• Pneumomediastinum
• Pulmonary oedema
• Haemoptysis
• Acute respiratory distress syndrome
Huff Coughing:
• Huff coughing, or huffing, is an alternative to deep coughing if you have trouble clearing your mucus.
• Take a breath that is slightly deeper than normal.
• Use your stomach muscles to make a series of three rapid exhalations with the airway open, making a "ha, ha, ha" sound.
Contraindications Forced Breathing
• Inability to control possible transmission of infection from patients suspected or known to have pathogens transmittable by droplet nuclei (eg: M tuberculosis)
• Presence of an elevated intracranial pressure or intracranial aneurysm
• Presence of reduced coronary artery perfusion, such as in acute myocardial infarction
• Acute unstable head, neck, or spine injury

EVALUATION
COUGH EVALUATION
Peak Cough Flow
• Effective peak cough flow in healthy subjects > 360 - 400 L/min
• Peak cough flow (PCF) for mucusexpectoration > 160 - 200 L/min.
• PCF > 250 - 270 L/min has been shown to besufficient to prevent pneumonia in patients with NMDs
Mellies U, Goebel C. Optimum Insufflation Capacity and Peak Cough Flow in Neuromuscular Disorders. Ann Am Thorac Soc. 2014
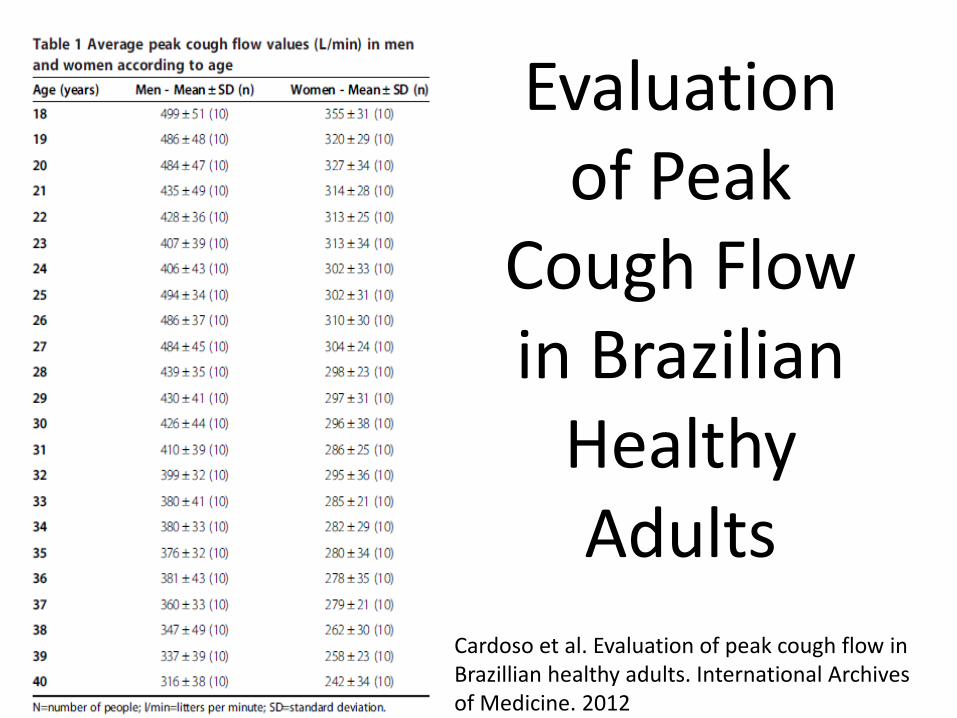
Evaluation of Peak
Cough Flow in Brazilian
Healthy Adults
Cardoso et al. Evaluation of peak cough flow in Brazillian healthy adults. International Archives of Medicine. 2012
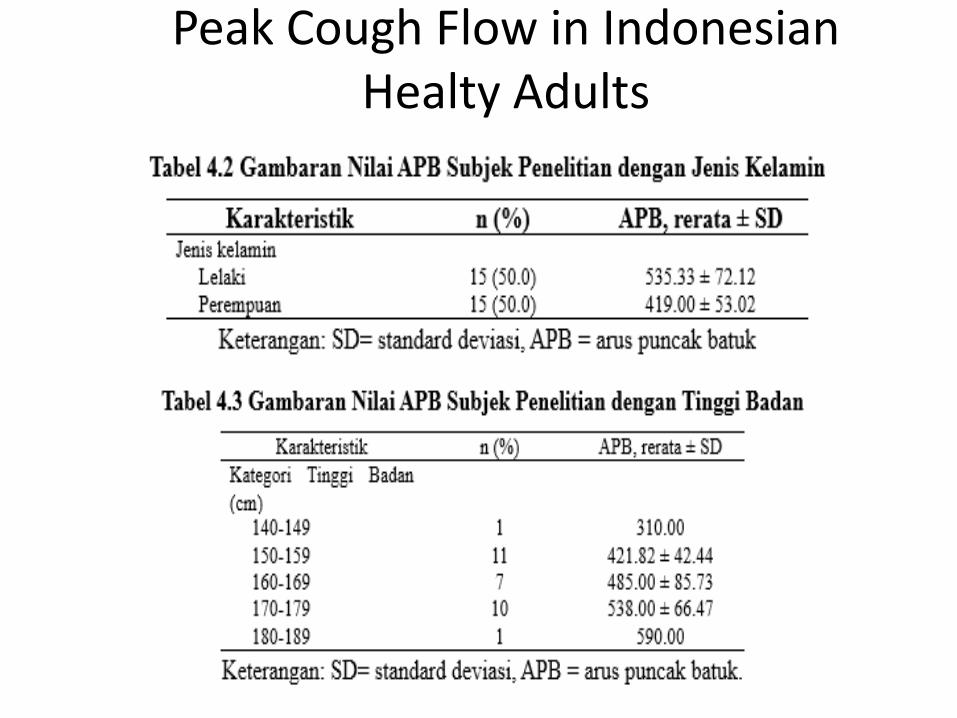
Peak Cough Flow in Indonesian Healty Adults
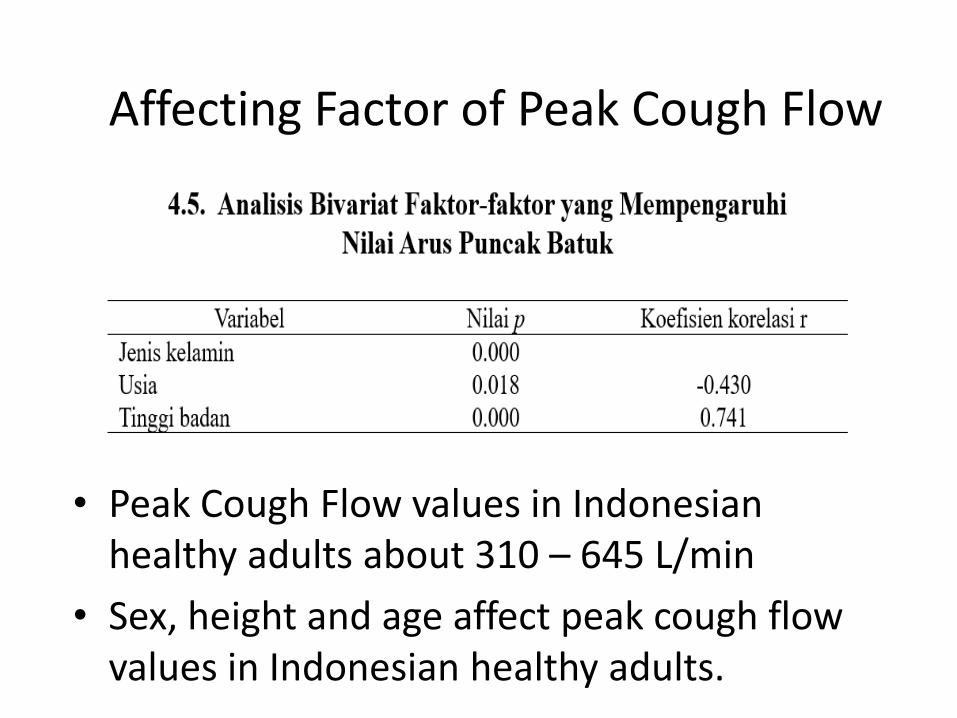
Affecting Factor of Peak Cough Flow
• Peak Cough Flow values in Indonesian healthy adults about 310 – 645 L/min
• Sex, height and age affect peak cough flow values in Indonesian healthy adults.

FUNCTIONAL CAPACITY & QUALITY OF LIFE
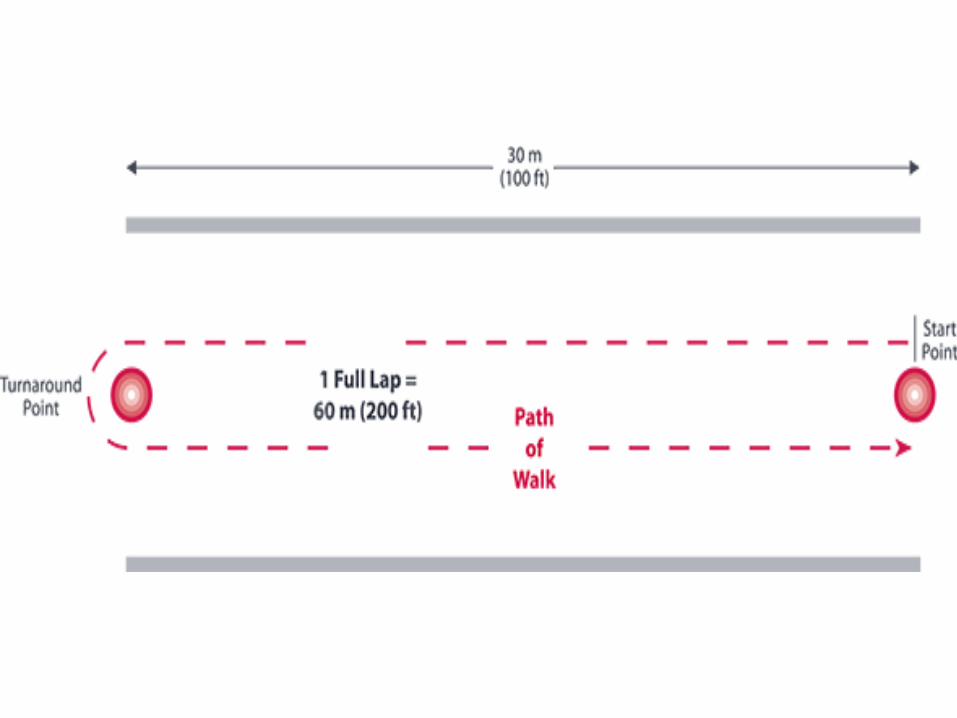
6-Minute Walk Test
1. Walk as FAR (not as FAST) as possible; running is prohibited
2. Walk around the marking cones for 6 minutes
3. Exhaustion or discomfort may cause the patient to stop but stopwatch will keep running
4. Every minute passed will be notified by the examiner
5. Examiner will monitor vital signs and O2 saturation
6. Upon completion, BORG Scale is re-assessed
7. Calculate total walking distance, rounded to the nearest meter
Take home message
• Proper manipulation technique performed by professionals is required for effective mucus evacuation
• Comprehensive evaluation should be done before and after intervention for optimal results

THANK YOU