-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
1/42
Introduction to endocrinology
Mariusz Mydlarczyk
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
2/42
Communication between cells
Endocrine system (information is carried bychemical
mediators)
Nervous system (information is carried by
neural impulses)
Immune system
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
3/42
Cooperation between endocrineand nervous system
Some neurotransmitters circulate in theblood as hormones
Neural impulses control the release of
chemical mediators
Hypothalamus this cooperation is most
apparent
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
4/42
Hormones
Substances, that are secreted into thecirculation and act as
chemical
effectors in other tissues
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
5/42
Places of hormone formation
Endocrine glands Diffused endocrine cells
Immune cells Nerve cells
Bloodstream
Extraglandular tissues
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
6/42
Places of hormone action
Target cells through the circulation(endocrine action) most
hormones
The same tissue without entering the
circulation (paracrine and juxtacrine action) sex steroids in
the ovary, angiotensin II inthe kidney
The same cell (autocrine action)- cancer cells
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
7/42
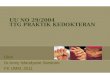
Endocrine
Cell
Neurotransmitter
and hormone
target cell
Hormone
target cell
Neurotransmitter
cell
Actions of hormones and neurotransmitters
Blood vessel
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
8/42
Chemistry of hormones
Peptides Small peptides
Polypeptides
Glycopeptides
Steroids
Amino acids derivatives Fatty acid derivatives
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
9/42
The synthesis of peptide hormones Translation mRNA into protein
precursor
Posttranslational:
cleavage (pre-pro-hormone, prohormone, hormone)
processing (thyroglobulin, thyroid hormones)
Submits:
derived from single precursor
derived from separate precursors
The same peptide cam be formed from different
prohormone encoded by distinct genes (TSH) Individual prohormone
can be metabolized into
different hormones (POMC)
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
10/42
The synthesis of steroid hormones
Precursor
Series of enzymatic transformations
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
11/42
Release mechanisms
Conversion of insoluble to solublederivatives (proteolysis of
thyroglobulin)
Exocytosis of storage granules (insulin,
glucagon, prolactin, GH)
Passive diffusion of newly synthesized
molecules (steroids)
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
12/42
The rate of hormone release
Periodic Rhythmic
Kind of cycles
ultradian: varying in frequently from minutes tohour
circadian: to daily
infradian: to months or year
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
13/42
Pulsatile administration of LHRH
stimulates the release of LH by thepituitary, whereas the
constant infusion
of the same amount of hormone per unittime has the opposite
effects
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
14/42
Transport of Hormones
Blood Lymph
Extracellular fluid
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
15/42
Total hormone
Protein bond
fractionFree fraction
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
16/42
Hormone transport in blood plasma
Most peptide and amine hormones circulate at lowconcentrations
unbound to other proteins (short T1/2)
Insoluble in water hormones are transported in protein-bound
form
Protein-bound form cannot enter most cellularcompartments and
serves as reservoir from with freehormone is liberated into free
(dialyzable) fraction
Only the free hormone interacts with receptors in targetcells
(represents the active hormone), dictates the
magnitude of feedback inhibition that controls hormonerelease,
is the fraction that is cleared from the circulationand correlates
best with clinical states of hormone
excess and deficiency
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
17/42
Degradation of hormones
Small fraction is excreted intact in urine orbile (free
hormones)
Degradation takes place in:
target tissues (peptide hormones)
nontarget tissues (liver, kidneys)
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
18/42
Mechanism of hormone action
Binding to receptor
Activation of postreceptor messengers Cellular answer
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
19/42
Hormone receptors
Cell surface receptors Intracellular receptors
Cytoplasmatic
Nuclear
Mitochondrial
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
20/42
Kinds of membrane receptors Class I: receptors with big
transmembrane part
consisting of 7 segments. These receptors activateG proteins.
Receptors for ACTH, LH, FSH, hCG,
TSH, glucagon, katecholamines, muscarine,serotonine, dopamine,
histamine
Class II: mobile, with own enzymatic properties.
Receptors for insulin, growth factors (tyrosinekinase), ANP
(guanylyl cyclase), TGFbeta (serine-threonine kinase)
Class III: do not possess enzymatic activity ontheir own but
interact with soluable transducermolecules which do possess
tyrosine kinaseactivity. GH, cytokines, interferons
Class IV: ion channels that binds ligands. Ach.
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
21/42
Hormone
G proteinClass I protein receptor
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
22/42
Binding domain
Binding domain
Tyrosine kinasedomain
Accessory protein
with tyrosine kinase
domain
Class II of
protein
receptor
Class III of
protein
receptor
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
23/42
Nuclear receptors
Nuclear receptors are ligand-regulated transcriptionfactor that
control gene expression by binding to targetgenes usually in the
region near their promoters.
Class I: steroid hormone. Unliganted receptors areassociated
with heat shock proteins and are present ineither the cytosol or
the nucleus. Ligand binding
promotes dissociation of the heat shock proteins andformation of
receptor homodimers that bind to specificDNA elements (HREs hormone
response elements)
Class II: thyroid hormone, retinoid, vitamin D,peroxisimal
proliferator-activated receptors (PPR).Receptors already present in
the nucleus in the uligantedstate. They are commonly active in the
absence ofhormone
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
24/42
Regulation of responsiveness tohormone
Down regulation: most hormones
Up regulation: progesterone
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
25/42
Classification of ligands
Inactive compounds Agonists
Antagonists
Partial agonist, partial antagonists
Mixed agonists-antagonists
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
26/42
GTP
ATP
Biological effects
Protein phosphorylation
Protein kinases A(PKA)
Phosphoproteinphosphatases (PP)
cAMP
Adenylyl cyclase
Gs protein GDP
Receptor
(Beta adrenergic, D1, V2, H2, GHRH, glucagon, TSH, ACTH, FSH,
LH)
Hormone
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
27/42
GTP
ATP
Biological effects
Protein phosphorylation
Protein kinases A
(PKA)
Phosphoprotein
phosphatases (PP)
cAMP
Adenylyl cyclase
Gi protein GDP
Receptor
(Alpha2 adrenergic, D2)
Hormone
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
28/42
GTP
Biological effects
Protein phosphorylation
Protein kinases G
(PKG)
Phosphoprotein
phosphatases (PP)
cGMP
Guanylyl cyclase
Receptor
(ANP)
Hormone
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
29/42
GTP
Protein kinases Ca-dependent
Guanyl cyclase
Phosphodiesterases
Phospholipase A2
Calmoduline
Ca++
Inositoltriphosphate
(IP3)
Arachidonic acid
cascade
Phospholipase A2
(PLA2)
Phosphoprotein
phosphatases (PP)
Protein phosphorylation
Protein dephosphorylation
Protein kinases C
(PKC)
Diacylglycerol
(DAG)
Phosphatidylinositol
Phospholipase C(PLC)
Gq protein GDP
Receptor
(alpha1 adrenergic, H1, GnRH, TRH, V1, AT1)
Hormone
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
30/42
Arachidonic acid cascade
PGs
TxA2
PGI2
PGH2
PGG2
Cyclooxygenase
LTX
5HPETE
Lipooxygenase
Arachidonic acid
(AA)
Phospholipase A2
Cell membrane phospholypides
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
31/42
Regulation of hormone secretion - negative feedback
mechanisms
Trophic hormone
Target endocrine organ
Target hormone
Anterior pituitary lobe
Portal pituitary circulation
Hypothalamus
(-)
(-)
(+)
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
32/42
Endocrine hypofunction
Destruction of gland: autoimmune disease,neoplasm, infection,
hemorrhage, injury
The absence of stimulation by trophic hormone
Defects in hormone synthesis Defects in sensitivity to
hormones
Damage to tissues that produce active forms of
hormones
Increased hormone metabolism
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
33/42
Endocrine hyperfunction
Tumors Ectopic production of peptide hormones
Hyperplasia
Autoimmune stimulation
Stimulation by trophic hormone
Diminished hormone metabolism
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
34/42
Defects in sensitivity to hormones
Genetic or acquired Prereceptor
Receptor
Postreceptor
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
35/42
Hypofunction Hyperfunction
Destruction Gland Tumor
Block Hyperplasia
Prohormone
Ectopic production
Iatrogenic
Hormone
Degraded Degraded
Receptor
Effector
Response
BlockStimulation
Block
StimulationDefect
AntibodiesAntibodies
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
36/42
Primary failure of target endocrine organ
Trophic hormone
Target endocrine organ
Target hormone
Anterior pituitary lobe
Portal pituitary circulation
Hypothalamus
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
37/42
Secondary failure fo target endocrine organ
Trophic hormone
Target endocrine organ
Target hormone
Anterior pituitary lobe
Portal pituitary circulation
Hypothalamus
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
38/42
Primary (autonomous) hypersecretion of target endocrine
organ
Trophic hormone
Target endocrine organ
Target hormone
Anterior pituitary lobe
Portal pituitary circulation
Hypothalamus
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
39/42
Secondary hypersecretion of target endocrine organ
Trophic hormone
Target endocrine organ
Target hormone
Anterior pituitary lobe
Portal pituitary circulation
Hypothalamus
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
40/42
Ectopic hormone production
Ectopic hormone
production
Trophic hormone
Target endocrine organ
Target hormone
Anterior pituitary lobe
Portal pituitary circulation
Hypothalamus
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
41/42
Hormonal resistance
Trophic hormone
Target endocrine organ
Target hormone
Anterior pituitary lobe
Portal pituitary circulation
Hypothalamus
-
7/31/2019 Dr.erfan - Endocrinology, Kuliah Fk 2011
42/42
Main hormonal disturbances
Target hormone level
HighNormalLow
Autonomous
(primary) secretion
of target endocrine
organ
Secondary targetendocrine organ
failureLow
Normal rangeNormal
Autonomous
(secondary)
secretion of
pituitary hormone
or hormonal
resistance
Primary failure of
target endocrine
organHigh
Pituitary
hormone
level