Embed Size (px)
Citation preview

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 123
486
41 Functional Neuroimaging Functional MagneticResonance Imaging Positron Emission Tomographyand Single-Photon Emission Computed Tomography
Philipp T Meyer Michel Rijntjes Sabine Hellwig Stefan Kloumlppel Cornelius Weiller
CHAPTER OUTLINE
FUNCTIONAL NEUROIMAGING MODALITIESFunctional Magnetic Resonance ImagingPositron Emission TomographySingle-Photon Emission Computed Tomography
CLINICAL APPLICATIONSDementia and Mild Cognitive ImpairmentParkinsonismBrain Tumors
EpilepsyPresurgical Brain MappingRecovery from StrokeConscious and Unconscious Processes
Structural imaging modalities such as computed tomography(CT) and magnetic resonance imaging (MRI) are essentialtechniques for evaluating various central nervous system(CNS) disorders providing superb structural resolution andtissue contrast On the other hand functional imaging modal-ities like functional MRI (fMRI) positron emission tomogra-phy (PET) and single-photon emission computed tomography(SPECT) visualize brain functions that are not necessarilyrelated to brain structure most notably cerebral blood flowmetabolism receptor binding and pathological depositionsFunctional neuroimaging is particularly valuable for mappingbrain functions or depicting disease-related molecular changesthat occur independently of or before structural changes Theprinciples of fMRI PET and SPECT and their applications inclinical neurosciences will be discussed in this chapter Regard-ing applications of PET and SPECT the focus will be on inves-tigations of cerebral blood flow (CBF) and glucose metabolismin dementia parkinsonism brain tumors and epilepsy Theseapplications are particularly well established and important inclinical practice Localization of brain function may be themain focus of fMRI research at present and is increasinglyutilized in presurgical mapping Furthermore one of the
oldest questions in clinical neurology is how brain functionis lost and can be regained Numerous fMRI studies in strokepatients have demonstrated relevant plasticity in the humanbrain and that cerebral reorganization is related to improve-ment of function which can be reinforced by training
FUNCTIONAL NEUROIMAGING MODALITIES
Functional Magnetic Resonance Imaging
Today fMRI is a standard technique in neuroscience brainimaging It relates to the blood oxygen level-dependent(BOLD) effect which is due to a transient and local access of
oxygenated blood resulting from changes in regional CBFand neuronal activity Experimental stimuli (eg words thatmust be read) are presented either in a block design (series of words for 20ndash30 seconds alternating by rest blocks of similarlength over several minutes) or event related (asymp30ndash40 stimuliof each type are presented in a counterbalanced order eachfollowed by some baseline period) Experiments are oftenconducted with multiple subjects which requires stereotacticnormalization into a standard space Time series are analyzedin a general linear model (GLM) allowing inferences on effectsizes Resulting visualizations illustrate regions with a task-specific statistically significant difference in brain activation
Time series of fMRI studies are used to detect functionaldependencies between brain regions (ldquofunctionalrdquo or ldquoeffec-tiverdquo connectivity) with mathematical approaches such asdynamic causal modeling directed partial correlations usingGranger causality Bayesian learning networks graph theoryand others
Positron Emission Tomography
The concept of modern PET was developed during the 1970s(Phelps et al 1975) The underlying principle of PET andalso of SPECT is to image and quantify a physiological func-tion or molecular target of interest in vivo by noninvasivelyassessing the spatial and temporal distribution of the radia-tion emitted by an intravenously injected target-specific probe
(radiotracer) Importantly PET and SPECT tracers are admin-istered in a nonpharmacological dose (micrograms or less)so they neither disturb the underlying system nor cause phar-macological or behavioral effects Because of their ability to visualize molecular targets and functions on a macroscopiclevel with unsurpassed sensitivity down to picomolar concen-tration PET and SPECT are also called molecular imaging tech-niques (See Cherry et al 2003 for an excellent textbook onPET and SPECT physics) (See Table 411 for a glossary on PETand SPECT tracers)
In the case of PET a positron-emitting radiotracer isinjected The emitted positron travels a short distance in tissue(effective range lt 1 mm for common PET nuclides) before itencounters an electron yielding a pair of two 511-keV annihi-lation photons emitted in opposite directions This photon
pair leaving the body is detected quasi-simultaneously (withina few nanoseconds) by scintillation detectors of the PET detec-tor rings that surround the patientrsquos head Assuming that theannihilation site is located on the line connecting both detec-tors (known as the line of response [LOR]) three-dimensional(3D) PET image data sets of the distribution of the PET tracerand its target are generated by standard image reconstructionalgorithms To actually gain quantitative PET images (ieradioactivitytracer concentration per unit tissue) the acquireddata are corrected for scatter and random coincidences andphoton attenuation by tissue absorption (eg using calculatedmethods CT or segmented MRI scans) The spatial resolutionof modern PET systems is about 3 to 5 mm Thus PET is
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 223
Functional Neuroimaging 487
tion of cerebral glucose metabolism and thus neuronal func-tion By use of appropriate pharmacokinetic models and aplasma input function (ie [18F]FDG concentration in arterialor arterialized venous plasma) the absolute cerebral meta-bolic rate of glucose (CMRglc in 983221molmin100 g tissue) canbe estimated In the case of [18F]FDG absolute quantification
is usually not necessary for routine clinical studies since thediagnostic information can often be obtained from the cere-bral pattern of [18F]FDG uptake or relative estimates of regionalglucose metabolism gained by normalizing regional [18F]FDGuptake to the uptake of a suitable reference region unaffectedby disease
Radiolabeled amino acids like [11C]methionine ([11C]MET)and O-(2-[18F]fluoroethyl)-L -tyrosine ([18F]FET) are increas-ingly used for neurooncological applications (Herholz et al 2012) Cerebral uptake of these amino acids reflects transportby sodium-independent L -transporters which are driven byconcentration gradients and thus by intracellular amino acidmetabolism and protein synthesis Although only [11C]METis actually incorporated into proteins cerebral uptake of[11C]MET and [18F]FET is commonly used as a surrogate marker
of protein synthesis and proliferation Opposed to [18
F]FDGcerebral uptake of amino acids is very low under normal con-ditions but greatly increased in neoplastic cells allowing foran excellent imaging contrast of most brain tumors (Glaude-mans et al 2013 Herholz et al 2012)
Single-Photon Emission Computed Tomography
The first SPECT measurements were performed in the 1960s(Kuhl and Edwards 1964) SPECT employs gamma-emittingradionuclides that decay by emitting a single gamma ray Typical radionuclides employed for neurological SPECT aretechnetium-99m (99m Tc half-life = 602 hours) and iodine-123(123I half-life = 132 hours) Gamma cameras are used forSPECT acquisition whereby usually two or three detector
heads rotate around the patientrsquos head to acquire two-dimensional planar images (projections) of the head frommultiple angles (eg in 3-degree steps) Whereas radiationcollimation is achieved by coincidence detection in PET hard- ware collimators with lead septa are placed in front of thedetector heads in the case of SPECT scanners Finally 3Dimage data reconstruction is done by conventional reconstruc-tion algorithms With combined SPECTCT systems a CTtransmission scan can replace less accurate calculated attenu-ation correction
The different acquisition principles imply that SPECT pos-sesses a considerably lower sensitivity than PET Thus rapidtemporal sampling (image frames of seconds to minutes) as
susceptible to partial volume effects if the object or lesion sizeis below two times the scanner resolution (as a rule of thumb) Todayrsquos PET systems are either constructed as hybrid PETCTor more recently PETMRI systems Although the clinicalutility of the latter still needs to be defined integrated PETMRI allows for a comprehensive synchronous imaging of
several morphological functional and molecular parametersin a single scanning session Possible applications are mani-fold reaching from cross-validation of imaging techniquesand multi-modal neurobiological activation studies overmethodological synergies (eg integrated motion and partial volume corrections of PET by MRI) to optimized patientcomfort throughput and diagnostics by one-stop shop multi-parametric imaging (eg in neurodegeneration epilepsy neu-rooncology and stroke) (Catana et al 2012) Time will tell whether integrated PETMRI can replicate the tremendoussuccess of integrated PETCT in clinical oncology
Commonly used radionuclides in neurological PET studiesare carbon-11 (11C half-life = 204 minutes) nitrogen-13 (13Nhalf-life = 100 minutes) oxygen-15 (15O physical half-life = 203 minutes) and fluorine-18 (18F half-life = 1097 minutes)
which are all cyclotron products Whereas the relatively longhalf-life of 18F allows shipping 18F-labeled tracers from a cyclo-tron site to a distant PET site this is not possible in the caseof 15O and 11C This clearly limits the clinical use of 15O-labeled water molecular oxygen and carbon dioxide for quantifica-tion of CBF cerebral metabolic rate of oxygen and oxygenextraction fraction This also applies to clinically very interest-ing 11C-labeled tracers like [11C]raclopride (dopamine D2 D3 receptor) [11C]flumazenil (GABA A receptor) [11C]methionine(amino acid transport) and [11C]PIB (amyloid-beta) Thus18F-labeled substitutes have been proposed and are currentlyunder investigation including several amyloid-beta ligandsrecently approved by the FDA
In this chapter on perfusion and metabolism we will pri-marily focus on PET studies using the glucose analog 2-deoxy-
2-(
18
F)fluoro-d-glucose ([
18
F]FDG) to assess cerebral glucosemetabolism With the rate of glucose metabolism beingclosely related to maintenance of ion gradients and transmit-ter turnover (in particular glutamate) [18F]FDG represents anideal tracer for assessment of neuronal function and itschanges (Sokoloff 1977) After uptake in cerebral tissue byspecific glucose transporters [18F]FDG is phosphorylated byhexokinase Since [18F]FDG-6-P is neither a substrate for trans-port back out of the cell nor can it be metabolized further itis virtually irreversible trapped in cells Therefore the distribu-tion of [18F]FDG in tissue imaged by PET (started 30ndash60minutes after injection to allow for sufficient uptake 5- to20-minute scan duration) closely reflects the regional distribu-
TABLE 411 Glossary PET and SPECT Tracers
Abbreviation Tracer Target processstructure
[99m Tc]ECD [99m Tc]ethylcysteinatedimer Cerebral blood flow
[18F]FDG [18F]2-fluoro-2-deoxy-D-glucose Cerebral glucose metabolism
[18F]FET [18F]O-(2-fluoroethyl)-L-tyrosine Amino acid transport
[18F]FLT [18F]3rsquo-deoxy-3rsquo-fluorothymidine Proliferation
[123I]FP-CIT [123I]N-ω -fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane Dopamine transporter
[99m Tc]HMPAO [99m Tc]hexamethylpropyleneamine oxime Cerebral blood flow
[123I]IBZM [123I]iodobenzamide Dopamine D2D3 receptor
[123I]MIBG [123I]metaiodobenzylguanidine Cardiac sympathetic innervation
[11C]MET [11C]methionine Amino acid transport (protein synthesis)
[11C]PIB [11C]Pittsburgh compound B Amyloid-beta plaques
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 323
488 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 411 [
18
F]FDG PET in early Alzheimer disease Early diseasestage is characterized by mild to moderate hypometabolism of tem-
poral and parietal cortices and posterior cingulate gyrus and pre-
cuneus Distinct asymmetry is often noticed as in this case As disease
progresses frontal cortices also become involved Top Transaxial PET
images of [18F]FDG uptake (color coded see color scale on right
orientation in radiological convention as indicated) Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Three-
dimensional stereotactic surface projections of [18F]FDG uptake (upper
row) and statistical deviation of the individualrsquos examination (as z score)
from age-matched healthy controls (lower row) Data are color coded
in rainbow scale (see lower right for z scale) Given are right and left
lateral and mesial views
a prerequisite for pharmacokinetic analyses is the strength ofPET whereas a single SPECT acquisition usually takes 20 to30 minutes Furthermore the spatial resolution of modernSPECT is only about 7 to 10 mm deteriorating with increasingdistance between object and collimator (ie higher resolutionfor cortical than subcortical structures distance betweenpatient and collimator should be minimized for optimal reso-lution) Thus SPECT is more susceptible to partial volumeeffects than PET which can be a particular drawback when itcomes to imaging small structures or lesions (eg braintumors) Nevertheless brain-dedicated SPECT instrumentsthat allow for optimized spatial and temporal sampling andpharmacokinetic data quantification have been proposed(Meyer et al 2008) and further technical developmentsare underway (Jansen and Vanderheyden 2007) The impor-tant advantages of SPECT over PET are the lower costsand broad availability of SPECT systems and radionuclides While 123I-labeled tracers (eg [123I]FP-CIT ([123I]ioflupaneDaTSCAN) for dopamine transporter (DAT) imaging) caneasily be shipped over long distances technetium-99m can beeluted onsite from molybdenum-99 (99Mo)99m Tc generatorsand used for labeling commercially available radiopharma-ceutical kits
We will focus on the two most widely used CBF tracershexamethylpropyleneamine oxime ([99m Tc]HMPAO) and
ethylcysteinate dimer ([99m Tc]ECD) Owing to their lipophilicnature and thus high first-pass extraction both radiotracers arerapidly taken up by the brain They are quasi-irreversiblyretained after conversion into hydrophilic compounds (enzy-matic de-esterification of [99m Tc]ECD instability and possiblyinteraction with glutathione in the case of [99m Tc]HMPAO)Differences in uptake mechanisms may explain slightdifferences in biological behavior (eg in stroke) with[99m Tc]HMPAO being more closely correlated to perfusion while [99m Tc]ECD uptake is also influenced by metabolic activ-ity Despite the fact that cerebral radiotracer uptake is virtuallycomplete within just 1 to 2 minutes after injection SPECTacquisition is usually started after 30 to 60 minutes to allowfor sufficient background clearance
Given the fact that the CBF is closely coupled to cerebral
glucose metabolism and thus to neuronal function (with afew rare exceptions) [99m Tc]HMPAO and [99m Tc]ECD are usedto assess neuronal activity However since cerebral autoregula-tion is also affected by many other factors (eg carbon dioxidelevel) and possibly diseases cerebral glucose metabolism rep-resents a more direct and probably less variable marker ofneuronal activity Given the technical limitations mentionedearlier [18F]FDG PET is generally preferred to CBF SPECT Oneimportant exception however is the use of ictal CBF SPECTin the assessment of patients with epilepsy [123I]FP-CIT SPECTscans for assessment of nigrostriatal integrity in suspected par-kinsonism or dementia with Lewy bodies are typically acquired3 hours after tracer injection and evaluated by visual inspec-tion and semi-quantitative region-of-interest analyses as out-lined by the respective practice guidelines (Djang et al 2012)
(see also Chapter 42)
CLINICAL APPLICATIONS
Dementia and Mild Cognitive Impairment
Early and accurate diagnosis of dementia is of crucial impor-tance for appropriate treatment (including possible enroll-ment into treatment trials and avoidance of possible sideeffects of treatments) for prognosis and for adequate coun-seling of patients and caregivers The diagnostic power of[18F]FDG PET in this situation is well established (Bohnen et al 2012 Herholz 2003) In clinical practice [18F]FDG PET
studies are interpreted by qualitative visual readings Toachieve optimal diagnostic accuracy these readings should besupported by voxel-based statistical analyses in comparison toaged-matched normal controls (eg Frisoni et al 2013Herholz et al 2002a Minoshima et al 1995) PET studiesshould always be interpreted with parallel inspection of arecent CT or MRI scan to detect structural defects (egischemia atrophy subdural hematoma) that cause regionalhypometabolism
Alzheimer Disease The typical finding in Alzheimer disease (AD) the most fre-quent neurodegenerative dementia is bilateral hypometabo-lism of the temporal and parietal association cortices with thetemporoparietal junction being the center of impairment Asthe disease progresses frontal association cortices also getinvolved (Figs 411 and 412) The magnitude and extent ofthe hypometabolism increases with progressing disease withrelative sparing of the primary motor and visual cortices thebasal ganglia and the cerebellum (often used as referenceregions) The degree of hypometabolism is usually well cor-related with the dementia severity (Herholz et al 2002aMinoshima et al 1997 Salmon et al 2005) Furthermorecortical hypometabolism is often asymmetrical correspond-
ing to predominant clinical symptoms (language impairmentif dominant or visuospatial impairment if nondominant hem-isphere is affected) Voxel-based statistical analyses consist-ently show that the posterior cingulate gyrus and precuneusare also affected which is an important diagnostic clue evenin the earliest AD stages (Minoshima et al 1997) The hip-pocampus is particularly affected by AD pathology and
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 423
Functional Neuroimaging 489
Fig 413 [18F]FDG PET in the different variants of primary progressive aphasia (PPA) [18F]FDG PET scans in logopenic variant PPA (lvPPA)
are characterized by a leftward asymmetric temporoparietal hypometabolism whereas the semantic variant PPA (svPPA) involves the most rostral
part of the temporal lobes Patients with the nonfluent variant PPA (nfvPPA) typically show leftward asymmetric frontal hypometabolism with
inferior frontal or posterior fronto-insular emphasis Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left
lateral views (see Fig 411 for additional details)
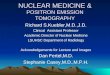
Fig 412 [18F]FDG PET in advanced Alzheimer disease Advanced
disease stage is characterized by severe hypometabolism of temporal
and parietal cortices and posterior cingulate gyrus and precuneus
Frontal cortex is also involved while sensorimotor and occipital corti-
ces basal ganglia thalamus and cerebellum are spared Mesiotem-
poral hypometabolism is also apparent Top Transaxial PET images
of [18F]FDG uptake Bottom Results of voxel-based statistical analysis
using Neurostat3D-SSP Given are right and left lateral superior and
posterior views (see Fig 411 for additional details)
consequently neurodegeneration This likely also contributesto posterior cingulateprecuneus hypometabolism by dias-chisis However studies on hippocampal metabolism in AD yielded conflicting results often showing no significanthypometabolism This may be due to the relatively low[18F]FDG uptake small size and AD-related atrophy of thisstructure which render visual and voxel-based statistical anal- yses insensitive Region-based analyses (eg using automatedhippocampal masking) can help overcome these limitations
and provide valuable incremental diagnostic information(Mosconi et al 2005)
The logopenic variant primary progressive aphasia (lvPPA) which is characterized by most prominent deficits in wordretrieval and sentence repetition is commonly assumed toalso be caused by AD LvPPA patients typically show a stronglyleftward asymmetric hypometabolism of the temporoparietalcortex (Gorno-Tempini et al 2011 Lehmann et al 2013Madhavan et al 2013) (Fig 413) Conversely patients withposterior cortical atrophy (PCA) another nonamnestic pres-entation of AD with predominant visuospatial and visuoper-ceptual deficits typically exhibit a rightward asymmetrictemporoparietal hypometabolism with strong involvement ofthe lateral occipital cortex (Lehmann et al 2013 Spehl et al 2014) (Fig 414)
A meta-analysis of recent [18F]FDG-PET cross-sectionalcase-control studies (n = 562 in total) revealed a very highsensitivity (96) and specificity (90) of [18F]FDG PET forthe diagnosis of AD (Bohnen et al 2012) In [18F]FDG PETstudies with autopsy confirmation in patients with memorycomplaints the pattern of temporoparietal hypometabolismas assessed by visual readings alone showed a high sensitivityof 84 to 94 for detecting pathologically confirmed AD with a specificity of 73 to 74 (Jagust et al 2007 Silverman et al 2001) Visual inspection of [18F]FDG PET was found to
be of similar accuracy to a clinical follow-up examinationperformed 4 years after PET Moreover when [18F]FDG PETdisagreed with the initial clinical diagnosis the PET diagnosis was considerably more likely to be congruent with the patho-logical diagnosis than the clinical diagnosis (Jagust et al 2007) In a large multicenter trial voxel-based statistical analy-ses of cortical [18F]FDG uptake differentiated AD from demen-tia with Lewy bodies (DLB see later section Dementia with Lewy Bodies) with 99 sensitivity and 71 specificity (97accuracy) and from frontotemporal dementia (FTD) with 99sensitivity and 65 specificity (97 accuracy) (Mosconi et al 2008) However the use of an additional hippocampal analy-sis (being relatively preserved in DLB and FTD) greatlyimproved specificity (100 and 94 for AD vs DLB and FTDrespectively) yielding an overall classification accuracy of
96 for the aforementioned patient groups and controls
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 523
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 623
Functional Neuroimaging 491
both groups there were only minor differences if any ( Yong et al 2007) However according to a recent meta-analysisabout two-thirds of DLB patients but only one-third of PDDpatients show a positive amyloid-beta PET scan (Donaghy
et al 2015) suggesting a differential contribution of amyloid-beta to the manifestation of cognitive impairment and itstiming in PD and DLB (reviewed in Meyer et al 2014) Recent[18F]FDG PET studies also support the notion that PD with MCI(PD-MCI) represents a prodromal stage of PDD (Litvan et al 2012) Similar to the pattern observed in PDD PD-MCIpatients typically exhibit a decreased temporoparietal occipi-tal precuneus and frontal metabolism when compared tohealthy controls and to a lesser extent to PD patients withoutMCI (Garcia-Garcia et al 2012 Hosokai et al 2009 Pappatagrave et al 2011) These changes are more pronounced in multi-domain compared to single-domain MCI (Huang et al 2008Lyoo et al 2010) and correlate with overall cognitive perform-ance across patients with PD PD-MCI and PDD (Garcia-Garcia et al 2012 Meyer et al 2014) Finally conversion from
PD to PDD was predicted by hypometabolism in posteriorcingulate occipital cortex (BA1819) and caudate nucleus while hypometabolism of the primary visual cortex (BA17) wasalso observed in cognitively stable PD patients Convertersshowed a widespread metabolic decline in several cortical andsubcortical areas on follow-up imaging (Bohnen et al 2011)
Frontotemporal Dementia
FTD probably represents the third most common overall causeof neurodegenerative dementia FTD refers to a heterogeneousgroup of syndromes characterized by predominant deficits inbehavior language and executive functions that are caused
et al 2009) is relatively preserved in DLB compared to ADoffering a high specificity for DLB However differencesbetween AD and DLB may be hard to appreciate in routineclinical examination of individual patients In this situation
PET or SPECT examinations of nigrostriatal integrity (mostnotably [123I]FP-CIT SPECT) can be very helpful in differentiat-ing between AD and DLB (McKeith et al 2007) A recentmeta-analysis indicated a pooled sensitivity and specificity of[123I]FP-CIT SPECT for DLB of 87 and 94 respectively(Papathanasiou et al 2012) Furthermore in a direct compari-son of [18F]FDG PET and dopamine transporter (DAT) SPECTthe latter was found to be superior for the differential diagnosisof DLB versus AD (Lim et al 2009) In line with this striatalDAT loss is defined as a suggestive feature in the current diag-nostic criteria for DLB while occipital hypometabolism is a supportive feature (McKeith et al 2005) Of note nigrostriatalprojections may also be damaged in FTD (Rinne et al 2002)and atypical parkinsonian syndromes with dementia (eg PSPand CBD see later section Parkinsonism) Concerning a pos-
sible prodromal stage of DLB it has been shown that primary visual cortex hypometabolism is associated with clinical corefeatures of DLB in as yet nondemented memory clinic patients(Fujishiro et al 2012) Those who converted to DLB duringfollow-up showed a more pronounced lateral occipital andparietal hypometabolism (Fujishiro et al 2013)
DLB is clinically distinguished from Parkinson disease (PD) with dementia (PDD) by the so-called 1-year rule In line withthe notion that both diseases most likely represent manifesta-tions of the same disease spectrum (Lewy body disease spec-trum) (Lippa et al 2007) [18F]FDG PET studies in PDD(Peppard et al 1992 Vander Borght et al 1997) found results very similar to those in DLB In fact in a direct comparison of
Fig 415 [18F]FDG PET in dementia with Lewy bodies (DLB) This disorder affects similar areas as those affected by Alzheimer disease (AD)
Occipital cortex is also involved which may distinguish DLB from AD in turn the mesiotemporal lobe is relatively spared in DLB A very similar
if not identical pattern is observed in Parkinson disease with dementia (PDD) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for addi-
tional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 723
492 PART II Neurological Investigations and Related Clinical Neurosciences
in an autopsy-confirmed study which was clearly superior toclinical diagnosis alone (Foster et al 2007) Consequentlyfrontal or anterior temporal hypoperfusion or hypometabo-lism was incorporated as a criterion for probable bvFTD intothe revised diagnostic criteria (Rascovsky et al 2011) Anormal [18F]FDG PET may be particularly helpful to assure ahigh specificity of the clinical diagnosis of bvFTD by identify-ing ldquophenocopiesrdquo (Kipps et al 2009) Patients with svPPAtypically show a predominant hypometabolism of the rostraltemporal lobes which is usually leftward asymmetrical (seeFig 413) (Diehl et al 2004 Rabinovici et al 2008) Thispattern distinguishes patients with svPPA from those withlvPPA that present a more posterior temporoparietal hypome-tabolism (as a nonamnestic AD manifestation see earlier)Finally opposed to the postrolandic hypometabolism foundin lvPPA and svPPA patients with nfvPPA exhibit a left frontalhypometabolism with inferior frontal or posterior fronto-insular emphasis (see Fig 413) (Josephs et al 2010 Nestor et al 2003 Rabinovici et al 2008) The aforementionedPPA-related patterns of hypometabolism on [18F]FDG PET (orhypoperfusion on SPECT) are also necessary findings to makethe diagnosis of imaging-supported lvPPA svPPA or nfvPPAaccording to the recently proposed classification (Gorno- Tempini et al 2011)
Vascular Dementia
Finally pure vascular dementia (VD) seems to be rather rarein North America and Europe and more prevalent in Japan atleast when several large cortical infarcts are seen as the causeof the dementia (so called multi-infarct dementia) But Bin-swanger disease or subcortical arteriosclerotic encephalopathymay be underdiagnosed or mistaken as ldquovascular changesrdquo in
by a progressive degeneration of frontal andor temporallobes FTD can be clinically subdivided into three major syn-dromes behavioral variant frontotemporal dementia (bvFTDprominent behavioralcognitive symptoms like disinhibitionapathy or executive deficits) semantic variant primary pro-gressive aphasia (svPPA prominent confrontation namingand single-word comprehension deficits) and nonfluent variant primary progressive aphasia (nfvPPA prominentagrammatism and motor speech difficulties) Although asso-ciations between clinical syndromes and underlying patholo-gies have been described (eg tauopathies like Pick disease orcorticobasal degeneration in nfvPPA tau-negative TDP-43- orFUS-positive aggregates in svPPA and bvFTD) clinical syn-dromes as well as pathologies may considerably overlap which hinders predicting the underlying pathology by theclinical phenotype (Kertesz et al 2005 Kertesz and McMona-gle 2011 Pressman and Miller 2014) In fact since patientsoften develop several syndromes during disease course leadingto a convergence of clinical presentations over time the clini-cal fractionation of this ldquoPick complexrdquo has been challenged(Kertesz et al 2005 Kertesz and McMonagle 2011) BvFTD isusually associated with a bilateral often asymmetrical frontalhypometabolism which is most pronounced in the mesial(polar) frontal cortex (Fig 416) (Garraux et al 1999 Salmon et al 2003) The striatum thalamus and temporal and pari-
etal cortices are also affected although to a lesser extent(Garraux et al 1999 Ishii et al 1998b) Despite the fact thatbvFTD and AD affect overlapping cortical areas the predomi-nance of frontal and temporoparietal deficits respectively isusually very apparent and allows a clear distinction betweenFTD and AD In line with this a voxel-based statistical analysisprovided a diagnostic accuracy of 90 (sensitivity 98 spe-cificity 86) for separating FTD (bvFTD and svPPA) and AD
Fig 416 [18F]FDG PET in behavioral variant of frontotemporal dementia (bvFTD) Bifrontal hypometabolism is usually found in FTD often
in a somewhat asymmetrical distribution as in this case At early stages frontomesial and frontopolar involvement is most pronounced while
parietal cortices can be affected later in disease course Top Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-based statistical
analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for additional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 823
Functional Neuroimaging 493
MSA-P) pons and cerebellum (especially in MSA-C) (Fig 418) In the case of PSP regional hypometabolism is consist-ently noted in medial dorso- and ventrolateral frontal areas(pronounced in anterior cingulate gyrus supplementarymotor and premotor areas) caudate nucleus (medial) thala-mus and upper brainstem (Fig 419) Finally CBD is charac-terized by a usually highly asymmetric hypometabolism offrontoparietal areas (pronounced parietal) motor cortex
middle cingulate gyrus striatum and thalamus contralateralto the most affected body side (Fig 4110) The aforemen-tioned results gained from categorical comparisons fit theresults gained from spatial covariance analyses These wereemployed to detect abnormal disease-related metabolic pat-terns in PD MSA and PSP (ie PDRP MSARP and PSPRPrespectively) which were demonstrated to be highly reproduc-ible to correlate with disease severity and duration and toallow for prospective discrimination between cohorts (Eckert et al 2008 Ma et al 2007 Poston et al 2012) The expres-sion of two distinctive spatial covariance patterns characterizesPD one related to motor manifestations (PDRP) and onerelated to cognitive manifestations (PDCP) The PDRP isalready significantly increased in the ipsilateral (ldquopresympto-maticrdquo) hemisphere of patients with hemi-parkinsonism
( Tang et al 2010b) Finally a very recent study (using [
18
F]FDG PET and CBF SPECT) demonstrated that PDRP is alsoincreased in REM sleep behavior disorder (RBD) being a sig-nificant predictor of phenoconversion to PD or DLB (Holt -bernd et al 2014) Thus covariance patterns of cerebralglucose metabolism represent very interesting biomarkers for(early) diagnosis and therapy monitoring in parkinsonism(Hirano et al 2009)
PSP and CBD may be considered to represent differentmanifestations of a disease spectrum with several commonclinical pathological genetic and biochemical features (Kouri et al 2011) This issue gets even more complex if one consid-ers that FTD is often caused by PSP and CBD pathology (see
AD [18F]FDG PET adds little to the diagnosis of VD In agree-ment with CT and MRI PET may show defects of [18F]FDGuptake corresponding to ischemic infarcts in all cerebralregions including primary cortices striatumthalamus andcerebellum Since the latter are usually well preserved in ADdefects in these regions can be an important diagnostic clueDeficits due to vascular lesions can be considerably larger orcause remote deficits of [18F]FDG uptake due to diaschisisFurthermore cerebral glucose metabolism was reported to beglobally reduced (Mielke et al 1992) but without absolutequantification this finding cannot be reliably assessed
Parkinsonism
An early and correct differential diagnosis of parkinsonism isof paramount therapeutic and prognostic importance giventhe possible excellent treatment options and prognosis inpatients without nigrostriatal degeneration (eg drug-inducedparkinsonism essential tremor) and the limited responsive-ness to levodopa and faster progression to disability and deathin patients with atypical parkinsonism syndromes (APS) com-pared to PD (Kempster et al 2007 OrsquoSullivan et al 2008)However postmortem studies suggest that the clinical diagno-sis of PD as the most frequent cause of parkinsonism isincorrect in about 25 of patients ( Tolosa et al 2006) Fre-
quent misdiagnoses include secondary parkinsonism and APSlike multiple system atrophy (MSA) PSP and CBD In turncumulative clinicopathological data suggest that about 30of MSA and PSP and up to 74 of CBD patients are not cor-rectly diagnosed even at late stage (Ling et al 2010)
Against this background SPECT and PET are used with twoaims first to identify patients with progressive nigrostriataldegeneration which is the common pathological feature inPD MSA PSP and CBD Second to differentiate between thelatter patient groups Accurate diagnosis of neurodegenerativeparkinsonism can be achieved by imaging nigrostriatal func-tion (most notably [123I]FP-CIT SPECT) (Benamer et al 2000Benitez-Rivero et al 2013 Marshall et al 2009) (For a moredetailed overview on nigrostriatal imaging in parkinsonismplease refer to Chapter 42) However dopamine transporter
imaging does not allow for a reliable differential diagnosis ofPD MSA PSP and CBD (Meyer and Hellwig 2014) Instead[18F]FDG PET has gained acceptance as the method of choicehere It surpasses the diagnostic accuracies of other commontechniques like imaging cardiac sympathetic innervation (egusing [123I]metaiodobenzylguanidine ([123I]MIBG) scintigra-phy) or imaging of striatal dopamine D2D3 receptors (egusing [123I]iodobenzamide([ 123I]IBZM)) (Meyer and Hellwig 2014) Assessment of regional CBF changes with SPECT mayalso be used for this purpose (eg Eckert et al 2007)However since [18F]FDG PET is technically superior and also widely available we will focus on [18F]FDG PET
[18F]FDG PET shows disease-specific alterations of cerebralglucose metabolism (eg Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Teune et al 2010) scans in PD patients
often show no major abnormality on first glance On closerinspection and especially on voxel-based statistical analysesPD is characterized by a posterior temporoparietal occipitaland sometimes frontal hypometabolism (especially in PD withmild cognitive impairment and PDD) and a relative hyperme-tabolism of putamen globus pallidus sensorimotor cortexpons and cerebellum (Fig 417) Interestingly temporoparieto-occipital hypometabolism may also seen in nondementedPD patients (Hellwig et al 2012 Hu et al 2000) possiblyindicating an increased risk of subsequent development ofPDD (see earlier section on Dementia and Mild Cognitive Impairment ) Conversely MSA patients show a markedhypometabolism of striatum (posterior putamen especially in
Fig 417 [18F]FDG PET in Parkinson disease (PD) PD is typically
characterized by (relative) striatal hypermetabolism Temporoparietal
occipital and sometime frontal hypometabolism can be observed in a
significant fraction of PD patients without apparent cognitive impair-
ment Cortical hypometabolism can be fairly pronounced possiblyrepresenting a risk factor for subsequent development of PDD Top
Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-
based statistical analysis using Neurostat3D-SSP Given are right and
left lateral superior and posterior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 223
Functional Neuroimaging 487
tion of cerebral glucose metabolism and thus neuronal func-tion By use of appropriate pharmacokinetic models and aplasma input function (ie [18F]FDG concentration in arterialor arterialized venous plasma) the absolute cerebral meta-bolic rate of glucose (CMRglc in 983221molmin100 g tissue) canbe estimated In the case of [18F]FDG absolute quantification
is usually not necessary for routine clinical studies since thediagnostic information can often be obtained from the cere-bral pattern of [18F]FDG uptake or relative estimates of regionalglucose metabolism gained by normalizing regional [18F]FDGuptake to the uptake of a suitable reference region unaffectedby disease
Radiolabeled amino acids like [11C]methionine ([11C]MET)and O-(2-[18F]fluoroethyl)-L -tyrosine ([18F]FET) are increas-ingly used for neurooncological applications (Herholz et al 2012) Cerebral uptake of these amino acids reflects transportby sodium-independent L -transporters which are driven byconcentration gradients and thus by intracellular amino acidmetabolism and protein synthesis Although only [11C]METis actually incorporated into proteins cerebral uptake of[11C]MET and [18F]FET is commonly used as a surrogate marker
of protein synthesis and proliferation Opposed to [18
F]FDGcerebral uptake of amino acids is very low under normal con-ditions but greatly increased in neoplastic cells allowing foran excellent imaging contrast of most brain tumors (Glaude-mans et al 2013 Herholz et al 2012)
Single-Photon Emission Computed Tomography
The first SPECT measurements were performed in the 1960s(Kuhl and Edwards 1964) SPECT employs gamma-emittingradionuclides that decay by emitting a single gamma ray Typical radionuclides employed for neurological SPECT aretechnetium-99m (99m Tc half-life = 602 hours) and iodine-123(123I half-life = 132 hours) Gamma cameras are used forSPECT acquisition whereby usually two or three detector
heads rotate around the patientrsquos head to acquire two-dimensional planar images (projections) of the head frommultiple angles (eg in 3-degree steps) Whereas radiationcollimation is achieved by coincidence detection in PET hard- ware collimators with lead septa are placed in front of thedetector heads in the case of SPECT scanners Finally 3Dimage data reconstruction is done by conventional reconstruc-tion algorithms With combined SPECTCT systems a CTtransmission scan can replace less accurate calculated attenu-ation correction
The different acquisition principles imply that SPECT pos-sesses a considerably lower sensitivity than PET Thus rapidtemporal sampling (image frames of seconds to minutes) as
susceptible to partial volume effects if the object or lesion sizeis below two times the scanner resolution (as a rule of thumb) Todayrsquos PET systems are either constructed as hybrid PETCTor more recently PETMRI systems Although the clinicalutility of the latter still needs to be defined integrated PETMRI allows for a comprehensive synchronous imaging of
several morphological functional and molecular parametersin a single scanning session Possible applications are mani-fold reaching from cross-validation of imaging techniquesand multi-modal neurobiological activation studies overmethodological synergies (eg integrated motion and partial volume corrections of PET by MRI) to optimized patientcomfort throughput and diagnostics by one-stop shop multi-parametric imaging (eg in neurodegeneration epilepsy neu-rooncology and stroke) (Catana et al 2012) Time will tell whether integrated PETMRI can replicate the tremendoussuccess of integrated PETCT in clinical oncology
Commonly used radionuclides in neurological PET studiesare carbon-11 (11C half-life = 204 minutes) nitrogen-13 (13Nhalf-life = 100 minutes) oxygen-15 (15O physical half-life = 203 minutes) and fluorine-18 (18F half-life = 1097 minutes)
which are all cyclotron products Whereas the relatively longhalf-life of 18F allows shipping 18F-labeled tracers from a cyclo-tron site to a distant PET site this is not possible in the caseof 15O and 11C This clearly limits the clinical use of 15O-labeled water molecular oxygen and carbon dioxide for quantifica-tion of CBF cerebral metabolic rate of oxygen and oxygenextraction fraction This also applies to clinically very interest-ing 11C-labeled tracers like [11C]raclopride (dopamine D2 D3 receptor) [11C]flumazenil (GABA A receptor) [11C]methionine(amino acid transport) and [11C]PIB (amyloid-beta) Thus18F-labeled substitutes have been proposed and are currentlyunder investigation including several amyloid-beta ligandsrecently approved by the FDA
In this chapter on perfusion and metabolism we will pri-marily focus on PET studies using the glucose analog 2-deoxy-
2-(
18
F)fluoro-d-glucose ([
18
F]FDG) to assess cerebral glucosemetabolism With the rate of glucose metabolism beingclosely related to maintenance of ion gradients and transmit-ter turnover (in particular glutamate) [18F]FDG represents anideal tracer for assessment of neuronal function and itschanges (Sokoloff 1977) After uptake in cerebral tissue byspecific glucose transporters [18F]FDG is phosphorylated byhexokinase Since [18F]FDG-6-P is neither a substrate for trans-port back out of the cell nor can it be metabolized further itis virtually irreversible trapped in cells Therefore the distribu-tion of [18F]FDG in tissue imaged by PET (started 30ndash60minutes after injection to allow for sufficient uptake 5- to20-minute scan duration) closely reflects the regional distribu-
TABLE 411 Glossary PET and SPECT Tracers
Abbreviation Tracer Target processstructure
[99m Tc]ECD [99m Tc]ethylcysteinatedimer Cerebral blood flow
[18F]FDG [18F]2-fluoro-2-deoxy-D-glucose Cerebral glucose metabolism
[18F]FET [18F]O-(2-fluoroethyl)-L-tyrosine Amino acid transport
[18F]FLT [18F]3rsquo-deoxy-3rsquo-fluorothymidine Proliferation
[123I]FP-CIT [123I]N-ω -fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane Dopamine transporter
[99m Tc]HMPAO [99m Tc]hexamethylpropyleneamine oxime Cerebral blood flow
[123I]IBZM [123I]iodobenzamide Dopamine D2D3 receptor
[123I]MIBG [123I]metaiodobenzylguanidine Cardiac sympathetic innervation
[11C]MET [11C]methionine Amino acid transport (protein synthesis)
[11C]PIB [11C]Pittsburgh compound B Amyloid-beta plaques
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 323
488 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 411 [
18
F]FDG PET in early Alzheimer disease Early diseasestage is characterized by mild to moderate hypometabolism of tem-
poral and parietal cortices and posterior cingulate gyrus and pre-
cuneus Distinct asymmetry is often noticed as in this case As disease
progresses frontal cortices also become involved Top Transaxial PET
images of [18F]FDG uptake (color coded see color scale on right
orientation in radiological convention as indicated) Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Three-
dimensional stereotactic surface projections of [18F]FDG uptake (upper
row) and statistical deviation of the individualrsquos examination (as z score)
from age-matched healthy controls (lower row) Data are color coded
in rainbow scale (see lower right for z scale) Given are right and left
lateral and mesial views
a prerequisite for pharmacokinetic analyses is the strength ofPET whereas a single SPECT acquisition usually takes 20 to30 minutes Furthermore the spatial resolution of modernSPECT is only about 7 to 10 mm deteriorating with increasingdistance between object and collimator (ie higher resolutionfor cortical than subcortical structures distance betweenpatient and collimator should be minimized for optimal reso-lution) Thus SPECT is more susceptible to partial volumeeffects than PET which can be a particular drawback when itcomes to imaging small structures or lesions (eg braintumors) Nevertheless brain-dedicated SPECT instrumentsthat allow for optimized spatial and temporal sampling andpharmacokinetic data quantification have been proposed(Meyer et al 2008) and further technical developmentsare underway (Jansen and Vanderheyden 2007) The impor-tant advantages of SPECT over PET are the lower costsand broad availability of SPECT systems and radionuclides While 123I-labeled tracers (eg [123I]FP-CIT ([123I]ioflupaneDaTSCAN) for dopamine transporter (DAT) imaging) caneasily be shipped over long distances technetium-99m can beeluted onsite from molybdenum-99 (99Mo)99m Tc generatorsand used for labeling commercially available radiopharma-ceutical kits
We will focus on the two most widely used CBF tracershexamethylpropyleneamine oxime ([99m Tc]HMPAO) and
ethylcysteinate dimer ([99m Tc]ECD) Owing to their lipophilicnature and thus high first-pass extraction both radiotracers arerapidly taken up by the brain They are quasi-irreversiblyretained after conversion into hydrophilic compounds (enzy-matic de-esterification of [99m Tc]ECD instability and possiblyinteraction with glutathione in the case of [99m Tc]HMPAO)Differences in uptake mechanisms may explain slightdifferences in biological behavior (eg in stroke) with[99m Tc]HMPAO being more closely correlated to perfusion while [99m Tc]ECD uptake is also influenced by metabolic activ-ity Despite the fact that cerebral radiotracer uptake is virtuallycomplete within just 1 to 2 minutes after injection SPECTacquisition is usually started after 30 to 60 minutes to allowfor sufficient background clearance
Given the fact that the CBF is closely coupled to cerebral
glucose metabolism and thus to neuronal function (with afew rare exceptions) [99m Tc]HMPAO and [99m Tc]ECD are usedto assess neuronal activity However since cerebral autoregula-tion is also affected by many other factors (eg carbon dioxidelevel) and possibly diseases cerebral glucose metabolism rep-resents a more direct and probably less variable marker ofneuronal activity Given the technical limitations mentionedearlier [18F]FDG PET is generally preferred to CBF SPECT Oneimportant exception however is the use of ictal CBF SPECTin the assessment of patients with epilepsy [123I]FP-CIT SPECTscans for assessment of nigrostriatal integrity in suspected par-kinsonism or dementia with Lewy bodies are typically acquired3 hours after tracer injection and evaluated by visual inspec-tion and semi-quantitative region-of-interest analyses as out-lined by the respective practice guidelines (Djang et al 2012)
(see also Chapter 42)
CLINICAL APPLICATIONS
Dementia and Mild Cognitive Impairment
Early and accurate diagnosis of dementia is of crucial impor-tance for appropriate treatment (including possible enroll-ment into treatment trials and avoidance of possible sideeffects of treatments) for prognosis and for adequate coun-seling of patients and caregivers The diagnostic power of[18F]FDG PET in this situation is well established (Bohnen et al 2012 Herholz 2003) In clinical practice [18F]FDG PET
studies are interpreted by qualitative visual readings Toachieve optimal diagnostic accuracy these readings should besupported by voxel-based statistical analyses in comparison toaged-matched normal controls (eg Frisoni et al 2013Herholz et al 2002a Minoshima et al 1995) PET studiesshould always be interpreted with parallel inspection of arecent CT or MRI scan to detect structural defects (egischemia atrophy subdural hematoma) that cause regionalhypometabolism
Alzheimer Disease The typical finding in Alzheimer disease (AD) the most fre-quent neurodegenerative dementia is bilateral hypometabo-lism of the temporal and parietal association cortices with thetemporoparietal junction being the center of impairment Asthe disease progresses frontal association cortices also getinvolved (Figs 411 and 412) The magnitude and extent ofthe hypometabolism increases with progressing disease withrelative sparing of the primary motor and visual cortices thebasal ganglia and the cerebellum (often used as referenceregions) The degree of hypometabolism is usually well cor-related with the dementia severity (Herholz et al 2002aMinoshima et al 1997 Salmon et al 2005) Furthermorecortical hypometabolism is often asymmetrical correspond-
ing to predominant clinical symptoms (language impairmentif dominant or visuospatial impairment if nondominant hem-isphere is affected) Voxel-based statistical analyses consist-ently show that the posterior cingulate gyrus and precuneusare also affected which is an important diagnostic clue evenin the earliest AD stages (Minoshima et al 1997) The hip-pocampus is particularly affected by AD pathology and
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 423
Functional Neuroimaging 489
Fig 413 [18F]FDG PET in the different variants of primary progressive aphasia (PPA) [18F]FDG PET scans in logopenic variant PPA (lvPPA)
are characterized by a leftward asymmetric temporoparietal hypometabolism whereas the semantic variant PPA (svPPA) involves the most rostral
part of the temporal lobes Patients with the nonfluent variant PPA (nfvPPA) typically show leftward asymmetric frontal hypometabolism with
inferior frontal or posterior fronto-insular emphasis Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left
lateral views (see Fig 411 for additional details)
Fig 412 [18F]FDG PET in advanced Alzheimer disease Advanced
disease stage is characterized by severe hypometabolism of temporal
and parietal cortices and posterior cingulate gyrus and precuneus
Frontal cortex is also involved while sensorimotor and occipital corti-
ces basal ganglia thalamus and cerebellum are spared Mesiotem-
poral hypometabolism is also apparent Top Transaxial PET images
of [18F]FDG uptake Bottom Results of voxel-based statistical analysis
using Neurostat3D-SSP Given are right and left lateral superior and
posterior views (see Fig 411 for additional details)
consequently neurodegeneration This likely also contributesto posterior cingulateprecuneus hypometabolism by dias-chisis However studies on hippocampal metabolism in AD yielded conflicting results often showing no significanthypometabolism This may be due to the relatively low[18F]FDG uptake small size and AD-related atrophy of thisstructure which render visual and voxel-based statistical anal- yses insensitive Region-based analyses (eg using automatedhippocampal masking) can help overcome these limitations
and provide valuable incremental diagnostic information(Mosconi et al 2005)
The logopenic variant primary progressive aphasia (lvPPA) which is characterized by most prominent deficits in wordretrieval and sentence repetition is commonly assumed toalso be caused by AD LvPPA patients typically show a stronglyleftward asymmetric hypometabolism of the temporoparietalcortex (Gorno-Tempini et al 2011 Lehmann et al 2013Madhavan et al 2013) (Fig 413) Conversely patients withposterior cortical atrophy (PCA) another nonamnestic pres-entation of AD with predominant visuospatial and visuoper-ceptual deficits typically exhibit a rightward asymmetrictemporoparietal hypometabolism with strong involvement ofthe lateral occipital cortex (Lehmann et al 2013 Spehl et al 2014) (Fig 414)
A meta-analysis of recent [18F]FDG-PET cross-sectionalcase-control studies (n = 562 in total) revealed a very highsensitivity (96) and specificity (90) of [18F]FDG PET forthe diagnosis of AD (Bohnen et al 2012) In [18F]FDG PETstudies with autopsy confirmation in patients with memorycomplaints the pattern of temporoparietal hypometabolismas assessed by visual readings alone showed a high sensitivityof 84 to 94 for detecting pathologically confirmed AD with a specificity of 73 to 74 (Jagust et al 2007 Silverman et al 2001) Visual inspection of [18F]FDG PET was found to
be of similar accuracy to a clinical follow-up examinationperformed 4 years after PET Moreover when [18F]FDG PETdisagreed with the initial clinical diagnosis the PET diagnosis was considerably more likely to be congruent with the patho-logical diagnosis than the clinical diagnosis (Jagust et al 2007) In a large multicenter trial voxel-based statistical analy-ses of cortical [18F]FDG uptake differentiated AD from demen-tia with Lewy bodies (DLB see later section Dementia with Lewy Bodies) with 99 sensitivity and 71 specificity (97accuracy) and from frontotemporal dementia (FTD) with 99sensitivity and 65 specificity (97 accuracy) (Mosconi et al 2008) However the use of an additional hippocampal analy-sis (being relatively preserved in DLB and FTD) greatlyimproved specificity (100 and 94 for AD vs DLB and FTDrespectively) yielding an overall classification accuracy of
96 for the aforementioned patient groups and controls
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 523
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 623
Functional Neuroimaging 491
both groups there were only minor differences if any ( Yong et al 2007) However according to a recent meta-analysisabout two-thirds of DLB patients but only one-third of PDDpatients show a positive amyloid-beta PET scan (Donaghy
et al 2015) suggesting a differential contribution of amyloid-beta to the manifestation of cognitive impairment and itstiming in PD and DLB (reviewed in Meyer et al 2014) Recent[18F]FDG PET studies also support the notion that PD with MCI(PD-MCI) represents a prodromal stage of PDD (Litvan et al 2012) Similar to the pattern observed in PDD PD-MCIpatients typically exhibit a decreased temporoparietal occipi-tal precuneus and frontal metabolism when compared tohealthy controls and to a lesser extent to PD patients withoutMCI (Garcia-Garcia et al 2012 Hosokai et al 2009 Pappatagrave et al 2011) These changes are more pronounced in multi-domain compared to single-domain MCI (Huang et al 2008Lyoo et al 2010) and correlate with overall cognitive perform-ance across patients with PD PD-MCI and PDD (Garcia-Garcia et al 2012 Meyer et al 2014) Finally conversion from
PD to PDD was predicted by hypometabolism in posteriorcingulate occipital cortex (BA1819) and caudate nucleus while hypometabolism of the primary visual cortex (BA17) wasalso observed in cognitively stable PD patients Convertersshowed a widespread metabolic decline in several cortical andsubcortical areas on follow-up imaging (Bohnen et al 2011)
Frontotemporal Dementia
FTD probably represents the third most common overall causeof neurodegenerative dementia FTD refers to a heterogeneousgroup of syndromes characterized by predominant deficits inbehavior language and executive functions that are caused
et al 2009) is relatively preserved in DLB compared to ADoffering a high specificity for DLB However differencesbetween AD and DLB may be hard to appreciate in routineclinical examination of individual patients In this situation
PET or SPECT examinations of nigrostriatal integrity (mostnotably [123I]FP-CIT SPECT) can be very helpful in differentiat-ing between AD and DLB (McKeith et al 2007) A recentmeta-analysis indicated a pooled sensitivity and specificity of[123I]FP-CIT SPECT for DLB of 87 and 94 respectively(Papathanasiou et al 2012) Furthermore in a direct compari-son of [18F]FDG PET and dopamine transporter (DAT) SPECTthe latter was found to be superior for the differential diagnosisof DLB versus AD (Lim et al 2009) In line with this striatalDAT loss is defined as a suggestive feature in the current diag-nostic criteria for DLB while occipital hypometabolism is a supportive feature (McKeith et al 2005) Of note nigrostriatalprojections may also be damaged in FTD (Rinne et al 2002)and atypical parkinsonian syndromes with dementia (eg PSPand CBD see later section Parkinsonism) Concerning a pos-
sible prodromal stage of DLB it has been shown that primary visual cortex hypometabolism is associated with clinical corefeatures of DLB in as yet nondemented memory clinic patients(Fujishiro et al 2012) Those who converted to DLB duringfollow-up showed a more pronounced lateral occipital andparietal hypometabolism (Fujishiro et al 2013)
DLB is clinically distinguished from Parkinson disease (PD) with dementia (PDD) by the so-called 1-year rule In line withthe notion that both diseases most likely represent manifesta-tions of the same disease spectrum (Lewy body disease spec-trum) (Lippa et al 2007) [18F]FDG PET studies in PDD(Peppard et al 1992 Vander Borght et al 1997) found results very similar to those in DLB In fact in a direct comparison of
Fig 415 [18F]FDG PET in dementia with Lewy bodies (DLB) This disorder affects similar areas as those affected by Alzheimer disease (AD)
Occipital cortex is also involved which may distinguish DLB from AD in turn the mesiotemporal lobe is relatively spared in DLB A very similar
if not identical pattern is observed in Parkinson disease with dementia (PDD) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for addi-
tional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 723
492 PART II Neurological Investigations and Related Clinical Neurosciences
in an autopsy-confirmed study which was clearly superior toclinical diagnosis alone (Foster et al 2007) Consequentlyfrontal or anterior temporal hypoperfusion or hypometabo-lism was incorporated as a criterion for probable bvFTD intothe revised diagnostic criteria (Rascovsky et al 2011) Anormal [18F]FDG PET may be particularly helpful to assure ahigh specificity of the clinical diagnosis of bvFTD by identify-ing ldquophenocopiesrdquo (Kipps et al 2009) Patients with svPPAtypically show a predominant hypometabolism of the rostraltemporal lobes which is usually leftward asymmetrical (seeFig 413) (Diehl et al 2004 Rabinovici et al 2008) Thispattern distinguishes patients with svPPA from those withlvPPA that present a more posterior temporoparietal hypome-tabolism (as a nonamnestic AD manifestation see earlier)Finally opposed to the postrolandic hypometabolism foundin lvPPA and svPPA patients with nfvPPA exhibit a left frontalhypometabolism with inferior frontal or posterior fronto-insular emphasis (see Fig 413) (Josephs et al 2010 Nestor et al 2003 Rabinovici et al 2008) The aforementionedPPA-related patterns of hypometabolism on [18F]FDG PET (orhypoperfusion on SPECT) are also necessary findings to makethe diagnosis of imaging-supported lvPPA svPPA or nfvPPAaccording to the recently proposed classification (Gorno- Tempini et al 2011)
Vascular Dementia
Finally pure vascular dementia (VD) seems to be rather rarein North America and Europe and more prevalent in Japan atleast when several large cortical infarcts are seen as the causeof the dementia (so called multi-infarct dementia) But Bin-swanger disease or subcortical arteriosclerotic encephalopathymay be underdiagnosed or mistaken as ldquovascular changesrdquo in
by a progressive degeneration of frontal andor temporallobes FTD can be clinically subdivided into three major syn-dromes behavioral variant frontotemporal dementia (bvFTDprominent behavioralcognitive symptoms like disinhibitionapathy or executive deficits) semantic variant primary pro-gressive aphasia (svPPA prominent confrontation namingand single-word comprehension deficits) and nonfluent variant primary progressive aphasia (nfvPPA prominentagrammatism and motor speech difficulties) Although asso-ciations between clinical syndromes and underlying patholo-gies have been described (eg tauopathies like Pick disease orcorticobasal degeneration in nfvPPA tau-negative TDP-43- orFUS-positive aggregates in svPPA and bvFTD) clinical syn-dromes as well as pathologies may considerably overlap which hinders predicting the underlying pathology by theclinical phenotype (Kertesz et al 2005 Kertesz and McMona-gle 2011 Pressman and Miller 2014) In fact since patientsoften develop several syndromes during disease course leadingto a convergence of clinical presentations over time the clini-cal fractionation of this ldquoPick complexrdquo has been challenged(Kertesz et al 2005 Kertesz and McMonagle 2011) BvFTD isusually associated with a bilateral often asymmetrical frontalhypometabolism which is most pronounced in the mesial(polar) frontal cortex (Fig 416) (Garraux et al 1999 Salmon et al 2003) The striatum thalamus and temporal and pari-
etal cortices are also affected although to a lesser extent(Garraux et al 1999 Ishii et al 1998b) Despite the fact thatbvFTD and AD affect overlapping cortical areas the predomi-nance of frontal and temporoparietal deficits respectively isusually very apparent and allows a clear distinction betweenFTD and AD In line with this a voxel-based statistical analysisprovided a diagnostic accuracy of 90 (sensitivity 98 spe-cificity 86) for separating FTD (bvFTD and svPPA) and AD
Fig 416 [18F]FDG PET in behavioral variant of frontotemporal dementia (bvFTD) Bifrontal hypometabolism is usually found in FTD often
in a somewhat asymmetrical distribution as in this case At early stages frontomesial and frontopolar involvement is most pronounced while
parietal cortices can be affected later in disease course Top Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-based statistical
analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for additional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 823
Functional Neuroimaging 493
MSA-P) pons and cerebellum (especially in MSA-C) (Fig 418) In the case of PSP regional hypometabolism is consist-ently noted in medial dorso- and ventrolateral frontal areas(pronounced in anterior cingulate gyrus supplementarymotor and premotor areas) caudate nucleus (medial) thala-mus and upper brainstem (Fig 419) Finally CBD is charac-terized by a usually highly asymmetric hypometabolism offrontoparietal areas (pronounced parietal) motor cortex
middle cingulate gyrus striatum and thalamus contralateralto the most affected body side (Fig 4110) The aforemen-tioned results gained from categorical comparisons fit theresults gained from spatial covariance analyses These wereemployed to detect abnormal disease-related metabolic pat-terns in PD MSA and PSP (ie PDRP MSARP and PSPRPrespectively) which were demonstrated to be highly reproduc-ible to correlate with disease severity and duration and toallow for prospective discrimination between cohorts (Eckert et al 2008 Ma et al 2007 Poston et al 2012) The expres-sion of two distinctive spatial covariance patterns characterizesPD one related to motor manifestations (PDRP) and onerelated to cognitive manifestations (PDCP) The PDRP isalready significantly increased in the ipsilateral (ldquopresympto-maticrdquo) hemisphere of patients with hemi-parkinsonism
( Tang et al 2010b) Finally a very recent study (using [
18
F]FDG PET and CBF SPECT) demonstrated that PDRP is alsoincreased in REM sleep behavior disorder (RBD) being a sig-nificant predictor of phenoconversion to PD or DLB (Holt -bernd et al 2014) Thus covariance patterns of cerebralglucose metabolism represent very interesting biomarkers for(early) diagnosis and therapy monitoring in parkinsonism(Hirano et al 2009)
PSP and CBD may be considered to represent differentmanifestations of a disease spectrum with several commonclinical pathological genetic and biochemical features (Kouri et al 2011) This issue gets even more complex if one consid-ers that FTD is often caused by PSP and CBD pathology (see
AD [18F]FDG PET adds little to the diagnosis of VD In agree-ment with CT and MRI PET may show defects of [18F]FDGuptake corresponding to ischemic infarcts in all cerebralregions including primary cortices striatumthalamus andcerebellum Since the latter are usually well preserved in ADdefects in these regions can be an important diagnostic clueDeficits due to vascular lesions can be considerably larger orcause remote deficits of [18F]FDG uptake due to diaschisisFurthermore cerebral glucose metabolism was reported to beglobally reduced (Mielke et al 1992) but without absolutequantification this finding cannot be reliably assessed
Parkinsonism
An early and correct differential diagnosis of parkinsonism isof paramount therapeutic and prognostic importance giventhe possible excellent treatment options and prognosis inpatients without nigrostriatal degeneration (eg drug-inducedparkinsonism essential tremor) and the limited responsive-ness to levodopa and faster progression to disability and deathin patients with atypical parkinsonism syndromes (APS) com-pared to PD (Kempster et al 2007 OrsquoSullivan et al 2008)However postmortem studies suggest that the clinical diagno-sis of PD as the most frequent cause of parkinsonism isincorrect in about 25 of patients ( Tolosa et al 2006) Fre-
quent misdiagnoses include secondary parkinsonism and APSlike multiple system atrophy (MSA) PSP and CBD In turncumulative clinicopathological data suggest that about 30of MSA and PSP and up to 74 of CBD patients are not cor-rectly diagnosed even at late stage (Ling et al 2010)
Against this background SPECT and PET are used with twoaims first to identify patients with progressive nigrostriataldegeneration which is the common pathological feature inPD MSA PSP and CBD Second to differentiate between thelatter patient groups Accurate diagnosis of neurodegenerativeparkinsonism can be achieved by imaging nigrostriatal func-tion (most notably [123I]FP-CIT SPECT) (Benamer et al 2000Benitez-Rivero et al 2013 Marshall et al 2009) (For a moredetailed overview on nigrostriatal imaging in parkinsonismplease refer to Chapter 42) However dopamine transporter
imaging does not allow for a reliable differential diagnosis ofPD MSA PSP and CBD (Meyer and Hellwig 2014) Instead[18F]FDG PET has gained acceptance as the method of choicehere It surpasses the diagnostic accuracies of other commontechniques like imaging cardiac sympathetic innervation (egusing [123I]metaiodobenzylguanidine ([123I]MIBG) scintigra-phy) or imaging of striatal dopamine D2D3 receptors (egusing [123I]iodobenzamide([ 123I]IBZM)) (Meyer and Hellwig 2014) Assessment of regional CBF changes with SPECT mayalso be used for this purpose (eg Eckert et al 2007)However since [18F]FDG PET is technically superior and also widely available we will focus on [18F]FDG PET
[18F]FDG PET shows disease-specific alterations of cerebralglucose metabolism (eg Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Teune et al 2010) scans in PD patients
often show no major abnormality on first glance On closerinspection and especially on voxel-based statistical analysesPD is characterized by a posterior temporoparietal occipitaland sometimes frontal hypometabolism (especially in PD withmild cognitive impairment and PDD) and a relative hyperme-tabolism of putamen globus pallidus sensorimotor cortexpons and cerebellum (Fig 417) Interestingly temporoparieto-occipital hypometabolism may also seen in nondementedPD patients (Hellwig et al 2012 Hu et al 2000) possiblyindicating an increased risk of subsequent development ofPDD (see earlier section on Dementia and Mild Cognitive Impairment ) Conversely MSA patients show a markedhypometabolism of striatum (posterior putamen especially in
Fig 417 [18F]FDG PET in Parkinson disease (PD) PD is typically
characterized by (relative) striatal hypermetabolism Temporoparietal
occipital and sometime frontal hypometabolism can be observed in a
significant fraction of PD patients without apparent cognitive impair-
ment Cortical hypometabolism can be fairly pronounced possiblyrepresenting a risk factor for subsequent development of PDD Top
Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-
based statistical analysis using Neurostat3D-SSP Given are right and
left lateral superior and posterior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 323
488 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 411 [
18
F]FDG PET in early Alzheimer disease Early diseasestage is characterized by mild to moderate hypometabolism of tem-
poral and parietal cortices and posterior cingulate gyrus and pre-
cuneus Distinct asymmetry is often noticed as in this case As disease
progresses frontal cortices also become involved Top Transaxial PET
images of [18F]FDG uptake (color coded see color scale on right
orientation in radiological convention as indicated) Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Three-
dimensional stereotactic surface projections of [18F]FDG uptake (upper
row) and statistical deviation of the individualrsquos examination (as z score)
from age-matched healthy controls (lower row) Data are color coded
in rainbow scale (see lower right for z scale) Given are right and left
lateral and mesial views
a prerequisite for pharmacokinetic analyses is the strength ofPET whereas a single SPECT acquisition usually takes 20 to30 minutes Furthermore the spatial resolution of modernSPECT is only about 7 to 10 mm deteriorating with increasingdistance between object and collimator (ie higher resolutionfor cortical than subcortical structures distance betweenpatient and collimator should be minimized for optimal reso-lution) Thus SPECT is more susceptible to partial volumeeffects than PET which can be a particular drawback when itcomes to imaging small structures or lesions (eg braintumors) Nevertheless brain-dedicated SPECT instrumentsthat allow for optimized spatial and temporal sampling andpharmacokinetic data quantification have been proposed(Meyer et al 2008) and further technical developmentsare underway (Jansen and Vanderheyden 2007) The impor-tant advantages of SPECT over PET are the lower costsand broad availability of SPECT systems and radionuclides While 123I-labeled tracers (eg [123I]FP-CIT ([123I]ioflupaneDaTSCAN) for dopamine transporter (DAT) imaging) caneasily be shipped over long distances technetium-99m can beeluted onsite from molybdenum-99 (99Mo)99m Tc generatorsand used for labeling commercially available radiopharma-ceutical kits
We will focus on the two most widely used CBF tracershexamethylpropyleneamine oxime ([99m Tc]HMPAO) and
ethylcysteinate dimer ([99m Tc]ECD) Owing to their lipophilicnature and thus high first-pass extraction both radiotracers arerapidly taken up by the brain They are quasi-irreversiblyretained after conversion into hydrophilic compounds (enzy-matic de-esterification of [99m Tc]ECD instability and possiblyinteraction with glutathione in the case of [99m Tc]HMPAO)Differences in uptake mechanisms may explain slightdifferences in biological behavior (eg in stroke) with[99m Tc]HMPAO being more closely correlated to perfusion while [99m Tc]ECD uptake is also influenced by metabolic activ-ity Despite the fact that cerebral radiotracer uptake is virtuallycomplete within just 1 to 2 minutes after injection SPECTacquisition is usually started after 30 to 60 minutes to allowfor sufficient background clearance
Given the fact that the CBF is closely coupled to cerebral
glucose metabolism and thus to neuronal function (with afew rare exceptions) [99m Tc]HMPAO and [99m Tc]ECD are usedto assess neuronal activity However since cerebral autoregula-tion is also affected by many other factors (eg carbon dioxidelevel) and possibly diseases cerebral glucose metabolism rep-resents a more direct and probably less variable marker ofneuronal activity Given the technical limitations mentionedearlier [18F]FDG PET is generally preferred to CBF SPECT Oneimportant exception however is the use of ictal CBF SPECTin the assessment of patients with epilepsy [123I]FP-CIT SPECTscans for assessment of nigrostriatal integrity in suspected par-kinsonism or dementia with Lewy bodies are typically acquired3 hours after tracer injection and evaluated by visual inspec-tion and semi-quantitative region-of-interest analyses as out-lined by the respective practice guidelines (Djang et al 2012)
(see also Chapter 42)
CLINICAL APPLICATIONS
Dementia and Mild Cognitive Impairment
Early and accurate diagnosis of dementia is of crucial impor-tance for appropriate treatment (including possible enroll-ment into treatment trials and avoidance of possible sideeffects of treatments) for prognosis and for adequate coun-seling of patients and caregivers The diagnostic power of[18F]FDG PET in this situation is well established (Bohnen et al 2012 Herholz 2003) In clinical practice [18F]FDG PET
studies are interpreted by qualitative visual readings Toachieve optimal diagnostic accuracy these readings should besupported by voxel-based statistical analyses in comparison toaged-matched normal controls (eg Frisoni et al 2013Herholz et al 2002a Minoshima et al 1995) PET studiesshould always be interpreted with parallel inspection of arecent CT or MRI scan to detect structural defects (egischemia atrophy subdural hematoma) that cause regionalhypometabolism
Alzheimer Disease The typical finding in Alzheimer disease (AD) the most fre-quent neurodegenerative dementia is bilateral hypometabo-lism of the temporal and parietal association cortices with thetemporoparietal junction being the center of impairment Asthe disease progresses frontal association cortices also getinvolved (Figs 411 and 412) The magnitude and extent ofthe hypometabolism increases with progressing disease withrelative sparing of the primary motor and visual cortices thebasal ganglia and the cerebellum (often used as referenceregions) The degree of hypometabolism is usually well cor-related with the dementia severity (Herholz et al 2002aMinoshima et al 1997 Salmon et al 2005) Furthermorecortical hypometabolism is often asymmetrical correspond-
ing to predominant clinical symptoms (language impairmentif dominant or visuospatial impairment if nondominant hem-isphere is affected) Voxel-based statistical analyses consist-ently show that the posterior cingulate gyrus and precuneusare also affected which is an important diagnostic clue evenin the earliest AD stages (Minoshima et al 1997) The hip-pocampus is particularly affected by AD pathology and
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 423
Functional Neuroimaging 489
Fig 413 [18F]FDG PET in the different variants of primary progressive aphasia (PPA) [18F]FDG PET scans in logopenic variant PPA (lvPPA)
are characterized by a leftward asymmetric temporoparietal hypometabolism whereas the semantic variant PPA (svPPA) involves the most rostral
part of the temporal lobes Patients with the nonfluent variant PPA (nfvPPA) typically show leftward asymmetric frontal hypometabolism with
inferior frontal or posterior fronto-insular emphasis Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left
lateral views (see Fig 411 for additional details)
Fig 412 [18F]FDG PET in advanced Alzheimer disease Advanced
disease stage is characterized by severe hypometabolism of temporal
and parietal cortices and posterior cingulate gyrus and precuneus
Frontal cortex is also involved while sensorimotor and occipital corti-
ces basal ganglia thalamus and cerebellum are spared Mesiotem-
poral hypometabolism is also apparent Top Transaxial PET images
of [18F]FDG uptake Bottom Results of voxel-based statistical analysis
using Neurostat3D-SSP Given are right and left lateral superior and
posterior views (see Fig 411 for additional details)
consequently neurodegeneration This likely also contributesto posterior cingulateprecuneus hypometabolism by dias-chisis However studies on hippocampal metabolism in AD yielded conflicting results often showing no significanthypometabolism This may be due to the relatively low[18F]FDG uptake small size and AD-related atrophy of thisstructure which render visual and voxel-based statistical anal- yses insensitive Region-based analyses (eg using automatedhippocampal masking) can help overcome these limitations
and provide valuable incremental diagnostic information(Mosconi et al 2005)
The logopenic variant primary progressive aphasia (lvPPA) which is characterized by most prominent deficits in wordretrieval and sentence repetition is commonly assumed toalso be caused by AD LvPPA patients typically show a stronglyleftward asymmetric hypometabolism of the temporoparietalcortex (Gorno-Tempini et al 2011 Lehmann et al 2013Madhavan et al 2013) (Fig 413) Conversely patients withposterior cortical atrophy (PCA) another nonamnestic pres-entation of AD with predominant visuospatial and visuoper-ceptual deficits typically exhibit a rightward asymmetrictemporoparietal hypometabolism with strong involvement ofthe lateral occipital cortex (Lehmann et al 2013 Spehl et al 2014) (Fig 414)
A meta-analysis of recent [18F]FDG-PET cross-sectionalcase-control studies (n = 562 in total) revealed a very highsensitivity (96) and specificity (90) of [18F]FDG PET forthe diagnosis of AD (Bohnen et al 2012) In [18F]FDG PETstudies with autopsy confirmation in patients with memorycomplaints the pattern of temporoparietal hypometabolismas assessed by visual readings alone showed a high sensitivityof 84 to 94 for detecting pathologically confirmed AD with a specificity of 73 to 74 (Jagust et al 2007 Silverman et al 2001) Visual inspection of [18F]FDG PET was found to
be of similar accuracy to a clinical follow-up examinationperformed 4 years after PET Moreover when [18F]FDG PETdisagreed with the initial clinical diagnosis the PET diagnosis was considerably more likely to be congruent with the patho-logical diagnosis than the clinical diagnosis (Jagust et al 2007) In a large multicenter trial voxel-based statistical analy-ses of cortical [18F]FDG uptake differentiated AD from demen-tia with Lewy bodies (DLB see later section Dementia with Lewy Bodies) with 99 sensitivity and 71 specificity (97accuracy) and from frontotemporal dementia (FTD) with 99sensitivity and 65 specificity (97 accuracy) (Mosconi et al 2008) However the use of an additional hippocampal analy-sis (being relatively preserved in DLB and FTD) greatlyimproved specificity (100 and 94 for AD vs DLB and FTDrespectively) yielding an overall classification accuracy of
96 for the aforementioned patient groups and controls
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 523
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 623
Functional Neuroimaging 491
both groups there were only minor differences if any ( Yong et al 2007) However according to a recent meta-analysisabout two-thirds of DLB patients but only one-third of PDDpatients show a positive amyloid-beta PET scan (Donaghy
et al 2015) suggesting a differential contribution of amyloid-beta to the manifestation of cognitive impairment and itstiming in PD and DLB (reviewed in Meyer et al 2014) Recent[18F]FDG PET studies also support the notion that PD with MCI(PD-MCI) represents a prodromal stage of PDD (Litvan et al 2012) Similar to the pattern observed in PDD PD-MCIpatients typically exhibit a decreased temporoparietal occipi-tal precuneus and frontal metabolism when compared tohealthy controls and to a lesser extent to PD patients withoutMCI (Garcia-Garcia et al 2012 Hosokai et al 2009 Pappatagrave et al 2011) These changes are more pronounced in multi-domain compared to single-domain MCI (Huang et al 2008Lyoo et al 2010) and correlate with overall cognitive perform-ance across patients with PD PD-MCI and PDD (Garcia-Garcia et al 2012 Meyer et al 2014) Finally conversion from
PD to PDD was predicted by hypometabolism in posteriorcingulate occipital cortex (BA1819) and caudate nucleus while hypometabolism of the primary visual cortex (BA17) wasalso observed in cognitively stable PD patients Convertersshowed a widespread metabolic decline in several cortical andsubcortical areas on follow-up imaging (Bohnen et al 2011)
Frontotemporal Dementia
FTD probably represents the third most common overall causeof neurodegenerative dementia FTD refers to a heterogeneousgroup of syndromes characterized by predominant deficits inbehavior language and executive functions that are caused
et al 2009) is relatively preserved in DLB compared to ADoffering a high specificity for DLB However differencesbetween AD and DLB may be hard to appreciate in routineclinical examination of individual patients In this situation
PET or SPECT examinations of nigrostriatal integrity (mostnotably [123I]FP-CIT SPECT) can be very helpful in differentiat-ing between AD and DLB (McKeith et al 2007) A recentmeta-analysis indicated a pooled sensitivity and specificity of[123I]FP-CIT SPECT for DLB of 87 and 94 respectively(Papathanasiou et al 2012) Furthermore in a direct compari-son of [18F]FDG PET and dopamine transporter (DAT) SPECTthe latter was found to be superior for the differential diagnosisof DLB versus AD (Lim et al 2009) In line with this striatalDAT loss is defined as a suggestive feature in the current diag-nostic criteria for DLB while occipital hypometabolism is a supportive feature (McKeith et al 2005) Of note nigrostriatalprojections may also be damaged in FTD (Rinne et al 2002)and atypical parkinsonian syndromes with dementia (eg PSPand CBD see later section Parkinsonism) Concerning a pos-
sible prodromal stage of DLB it has been shown that primary visual cortex hypometabolism is associated with clinical corefeatures of DLB in as yet nondemented memory clinic patients(Fujishiro et al 2012) Those who converted to DLB duringfollow-up showed a more pronounced lateral occipital andparietal hypometabolism (Fujishiro et al 2013)
DLB is clinically distinguished from Parkinson disease (PD) with dementia (PDD) by the so-called 1-year rule In line withthe notion that both diseases most likely represent manifesta-tions of the same disease spectrum (Lewy body disease spec-trum) (Lippa et al 2007) [18F]FDG PET studies in PDD(Peppard et al 1992 Vander Borght et al 1997) found results very similar to those in DLB In fact in a direct comparison of
Fig 415 [18F]FDG PET in dementia with Lewy bodies (DLB) This disorder affects similar areas as those affected by Alzheimer disease (AD)
Occipital cortex is also involved which may distinguish DLB from AD in turn the mesiotemporal lobe is relatively spared in DLB A very similar
if not identical pattern is observed in Parkinson disease with dementia (PDD) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for addi-
tional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 723
492 PART II Neurological Investigations and Related Clinical Neurosciences
in an autopsy-confirmed study which was clearly superior toclinical diagnosis alone (Foster et al 2007) Consequentlyfrontal or anterior temporal hypoperfusion or hypometabo-lism was incorporated as a criterion for probable bvFTD intothe revised diagnostic criteria (Rascovsky et al 2011) Anormal [18F]FDG PET may be particularly helpful to assure ahigh specificity of the clinical diagnosis of bvFTD by identify-ing ldquophenocopiesrdquo (Kipps et al 2009) Patients with svPPAtypically show a predominant hypometabolism of the rostraltemporal lobes which is usually leftward asymmetrical (seeFig 413) (Diehl et al 2004 Rabinovici et al 2008) Thispattern distinguishes patients with svPPA from those withlvPPA that present a more posterior temporoparietal hypome-tabolism (as a nonamnestic AD manifestation see earlier)Finally opposed to the postrolandic hypometabolism foundin lvPPA and svPPA patients with nfvPPA exhibit a left frontalhypometabolism with inferior frontal or posterior fronto-insular emphasis (see Fig 413) (Josephs et al 2010 Nestor et al 2003 Rabinovici et al 2008) The aforementionedPPA-related patterns of hypometabolism on [18F]FDG PET (orhypoperfusion on SPECT) are also necessary findings to makethe diagnosis of imaging-supported lvPPA svPPA or nfvPPAaccording to the recently proposed classification (Gorno- Tempini et al 2011)
Vascular Dementia
Finally pure vascular dementia (VD) seems to be rather rarein North America and Europe and more prevalent in Japan atleast when several large cortical infarcts are seen as the causeof the dementia (so called multi-infarct dementia) But Bin-swanger disease or subcortical arteriosclerotic encephalopathymay be underdiagnosed or mistaken as ldquovascular changesrdquo in
by a progressive degeneration of frontal andor temporallobes FTD can be clinically subdivided into three major syn-dromes behavioral variant frontotemporal dementia (bvFTDprominent behavioralcognitive symptoms like disinhibitionapathy or executive deficits) semantic variant primary pro-gressive aphasia (svPPA prominent confrontation namingand single-word comprehension deficits) and nonfluent variant primary progressive aphasia (nfvPPA prominentagrammatism and motor speech difficulties) Although asso-ciations between clinical syndromes and underlying patholo-gies have been described (eg tauopathies like Pick disease orcorticobasal degeneration in nfvPPA tau-negative TDP-43- orFUS-positive aggregates in svPPA and bvFTD) clinical syn-dromes as well as pathologies may considerably overlap which hinders predicting the underlying pathology by theclinical phenotype (Kertesz et al 2005 Kertesz and McMona-gle 2011 Pressman and Miller 2014) In fact since patientsoften develop several syndromes during disease course leadingto a convergence of clinical presentations over time the clini-cal fractionation of this ldquoPick complexrdquo has been challenged(Kertesz et al 2005 Kertesz and McMonagle 2011) BvFTD isusually associated with a bilateral often asymmetrical frontalhypometabolism which is most pronounced in the mesial(polar) frontal cortex (Fig 416) (Garraux et al 1999 Salmon et al 2003) The striatum thalamus and temporal and pari-
etal cortices are also affected although to a lesser extent(Garraux et al 1999 Ishii et al 1998b) Despite the fact thatbvFTD and AD affect overlapping cortical areas the predomi-nance of frontal and temporoparietal deficits respectively isusually very apparent and allows a clear distinction betweenFTD and AD In line with this a voxel-based statistical analysisprovided a diagnostic accuracy of 90 (sensitivity 98 spe-cificity 86) for separating FTD (bvFTD and svPPA) and AD
Fig 416 [18F]FDG PET in behavioral variant of frontotemporal dementia (bvFTD) Bifrontal hypometabolism is usually found in FTD often
in a somewhat asymmetrical distribution as in this case At early stages frontomesial and frontopolar involvement is most pronounced while
parietal cortices can be affected later in disease course Top Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-based statistical
analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for additional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 823
Functional Neuroimaging 493
MSA-P) pons and cerebellum (especially in MSA-C) (Fig 418) In the case of PSP regional hypometabolism is consist-ently noted in medial dorso- and ventrolateral frontal areas(pronounced in anterior cingulate gyrus supplementarymotor and premotor areas) caudate nucleus (medial) thala-mus and upper brainstem (Fig 419) Finally CBD is charac-terized by a usually highly asymmetric hypometabolism offrontoparietal areas (pronounced parietal) motor cortex
middle cingulate gyrus striatum and thalamus contralateralto the most affected body side (Fig 4110) The aforemen-tioned results gained from categorical comparisons fit theresults gained from spatial covariance analyses These wereemployed to detect abnormal disease-related metabolic pat-terns in PD MSA and PSP (ie PDRP MSARP and PSPRPrespectively) which were demonstrated to be highly reproduc-ible to correlate with disease severity and duration and toallow for prospective discrimination between cohorts (Eckert et al 2008 Ma et al 2007 Poston et al 2012) The expres-sion of two distinctive spatial covariance patterns characterizesPD one related to motor manifestations (PDRP) and onerelated to cognitive manifestations (PDCP) The PDRP isalready significantly increased in the ipsilateral (ldquopresympto-maticrdquo) hemisphere of patients with hemi-parkinsonism
( Tang et al 2010b) Finally a very recent study (using [
18
F]FDG PET and CBF SPECT) demonstrated that PDRP is alsoincreased in REM sleep behavior disorder (RBD) being a sig-nificant predictor of phenoconversion to PD or DLB (Holt -bernd et al 2014) Thus covariance patterns of cerebralglucose metabolism represent very interesting biomarkers for(early) diagnosis and therapy monitoring in parkinsonism(Hirano et al 2009)
PSP and CBD may be considered to represent differentmanifestations of a disease spectrum with several commonclinical pathological genetic and biochemical features (Kouri et al 2011) This issue gets even more complex if one consid-ers that FTD is often caused by PSP and CBD pathology (see
AD [18F]FDG PET adds little to the diagnosis of VD In agree-ment with CT and MRI PET may show defects of [18F]FDGuptake corresponding to ischemic infarcts in all cerebralregions including primary cortices striatumthalamus andcerebellum Since the latter are usually well preserved in ADdefects in these regions can be an important diagnostic clueDeficits due to vascular lesions can be considerably larger orcause remote deficits of [18F]FDG uptake due to diaschisisFurthermore cerebral glucose metabolism was reported to beglobally reduced (Mielke et al 1992) but without absolutequantification this finding cannot be reliably assessed
Parkinsonism
An early and correct differential diagnosis of parkinsonism isof paramount therapeutic and prognostic importance giventhe possible excellent treatment options and prognosis inpatients without nigrostriatal degeneration (eg drug-inducedparkinsonism essential tremor) and the limited responsive-ness to levodopa and faster progression to disability and deathin patients with atypical parkinsonism syndromes (APS) com-pared to PD (Kempster et al 2007 OrsquoSullivan et al 2008)However postmortem studies suggest that the clinical diagno-sis of PD as the most frequent cause of parkinsonism isincorrect in about 25 of patients ( Tolosa et al 2006) Fre-
quent misdiagnoses include secondary parkinsonism and APSlike multiple system atrophy (MSA) PSP and CBD In turncumulative clinicopathological data suggest that about 30of MSA and PSP and up to 74 of CBD patients are not cor-rectly diagnosed even at late stage (Ling et al 2010)
Against this background SPECT and PET are used with twoaims first to identify patients with progressive nigrostriataldegeneration which is the common pathological feature inPD MSA PSP and CBD Second to differentiate between thelatter patient groups Accurate diagnosis of neurodegenerativeparkinsonism can be achieved by imaging nigrostriatal func-tion (most notably [123I]FP-CIT SPECT) (Benamer et al 2000Benitez-Rivero et al 2013 Marshall et al 2009) (For a moredetailed overview on nigrostriatal imaging in parkinsonismplease refer to Chapter 42) However dopamine transporter
imaging does not allow for a reliable differential diagnosis ofPD MSA PSP and CBD (Meyer and Hellwig 2014) Instead[18F]FDG PET has gained acceptance as the method of choicehere It surpasses the diagnostic accuracies of other commontechniques like imaging cardiac sympathetic innervation (egusing [123I]metaiodobenzylguanidine ([123I]MIBG) scintigra-phy) or imaging of striatal dopamine D2D3 receptors (egusing [123I]iodobenzamide([ 123I]IBZM)) (Meyer and Hellwig 2014) Assessment of regional CBF changes with SPECT mayalso be used for this purpose (eg Eckert et al 2007)However since [18F]FDG PET is technically superior and also widely available we will focus on [18F]FDG PET
[18F]FDG PET shows disease-specific alterations of cerebralglucose metabolism (eg Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Teune et al 2010) scans in PD patients
often show no major abnormality on first glance On closerinspection and especially on voxel-based statistical analysesPD is characterized by a posterior temporoparietal occipitaland sometimes frontal hypometabolism (especially in PD withmild cognitive impairment and PDD) and a relative hyperme-tabolism of putamen globus pallidus sensorimotor cortexpons and cerebellum (Fig 417) Interestingly temporoparieto-occipital hypometabolism may also seen in nondementedPD patients (Hellwig et al 2012 Hu et al 2000) possiblyindicating an increased risk of subsequent development ofPDD (see earlier section on Dementia and Mild Cognitive Impairment ) Conversely MSA patients show a markedhypometabolism of striatum (posterior putamen especially in
Fig 417 [18F]FDG PET in Parkinson disease (PD) PD is typically
characterized by (relative) striatal hypermetabolism Temporoparietal
occipital and sometime frontal hypometabolism can be observed in a
significant fraction of PD patients without apparent cognitive impair-
ment Cortical hypometabolism can be fairly pronounced possiblyrepresenting a risk factor for subsequent development of PDD Top
Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-
based statistical analysis using Neurostat3D-SSP Given are right and
left lateral superior and posterior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
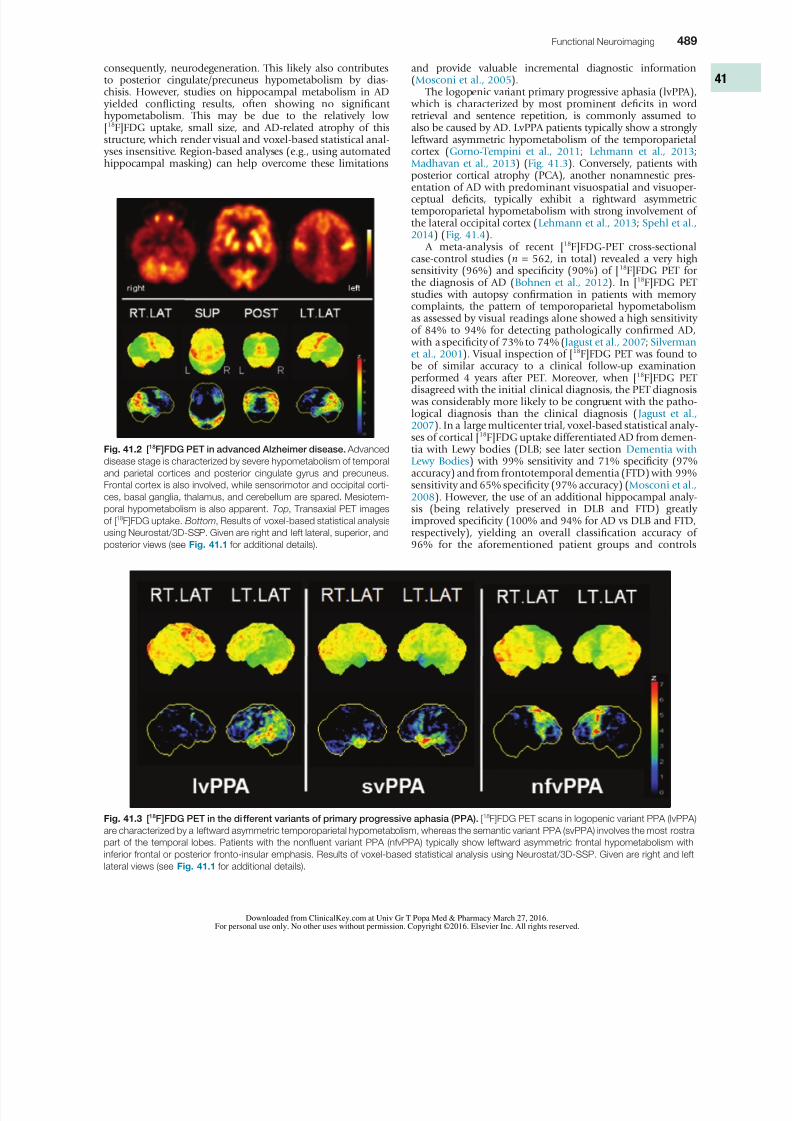
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 423
Functional Neuroimaging 489
Fig 413 [18F]FDG PET in the different variants of primary progressive aphasia (PPA) [18F]FDG PET scans in logopenic variant PPA (lvPPA)
are characterized by a leftward asymmetric temporoparietal hypometabolism whereas the semantic variant PPA (svPPA) involves the most rostral
part of the temporal lobes Patients with the nonfluent variant PPA (nfvPPA) typically show leftward asymmetric frontal hypometabolism with
inferior frontal or posterior fronto-insular emphasis Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left
lateral views (see Fig 411 for additional details)
Fig 412 [18F]FDG PET in advanced Alzheimer disease Advanced
disease stage is characterized by severe hypometabolism of temporal
and parietal cortices and posterior cingulate gyrus and precuneus
Frontal cortex is also involved while sensorimotor and occipital corti-
ces basal ganglia thalamus and cerebellum are spared Mesiotem-
poral hypometabolism is also apparent Top Transaxial PET images
of [18F]FDG uptake Bottom Results of voxel-based statistical analysis
using Neurostat3D-SSP Given are right and left lateral superior and
posterior views (see Fig 411 for additional details)
consequently neurodegeneration This likely also contributesto posterior cingulateprecuneus hypometabolism by dias-chisis However studies on hippocampal metabolism in AD yielded conflicting results often showing no significanthypometabolism This may be due to the relatively low[18F]FDG uptake small size and AD-related atrophy of thisstructure which render visual and voxel-based statistical anal- yses insensitive Region-based analyses (eg using automatedhippocampal masking) can help overcome these limitations
and provide valuable incremental diagnostic information(Mosconi et al 2005)
The logopenic variant primary progressive aphasia (lvPPA) which is characterized by most prominent deficits in wordretrieval and sentence repetition is commonly assumed toalso be caused by AD LvPPA patients typically show a stronglyleftward asymmetric hypometabolism of the temporoparietalcortex (Gorno-Tempini et al 2011 Lehmann et al 2013Madhavan et al 2013) (Fig 413) Conversely patients withposterior cortical atrophy (PCA) another nonamnestic pres-entation of AD with predominant visuospatial and visuoper-ceptual deficits typically exhibit a rightward asymmetrictemporoparietal hypometabolism with strong involvement ofthe lateral occipital cortex (Lehmann et al 2013 Spehl et al 2014) (Fig 414)
A meta-analysis of recent [18F]FDG-PET cross-sectionalcase-control studies (n = 562 in total) revealed a very highsensitivity (96) and specificity (90) of [18F]FDG PET forthe diagnosis of AD (Bohnen et al 2012) In [18F]FDG PETstudies with autopsy confirmation in patients with memorycomplaints the pattern of temporoparietal hypometabolismas assessed by visual readings alone showed a high sensitivityof 84 to 94 for detecting pathologically confirmed AD with a specificity of 73 to 74 (Jagust et al 2007 Silverman et al 2001) Visual inspection of [18F]FDG PET was found to
be of similar accuracy to a clinical follow-up examinationperformed 4 years after PET Moreover when [18F]FDG PETdisagreed with the initial clinical diagnosis the PET diagnosis was considerably more likely to be congruent with the patho-logical diagnosis than the clinical diagnosis (Jagust et al 2007) In a large multicenter trial voxel-based statistical analy-ses of cortical [18F]FDG uptake differentiated AD from demen-tia with Lewy bodies (DLB see later section Dementia with Lewy Bodies) with 99 sensitivity and 71 specificity (97accuracy) and from frontotemporal dementia (FTD) with 99sensitivity and 65 specificity (97 accuracy) (Mosconi et al 2008) However the use of an additional hippocampal analy-sis (being relatively preserved in DLB and FTD) greatlyimproved specificity (100 and 94 for AD vs DLB and FTDrespectively) yielding an overall classification accuracy of
96 for the aforementioned patient groups and controls
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 523
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 623
Functional Neuroimaging 491
both groups there were only minor differences if any ( Yong et al 2007) However according to a recent meta-analysisabout two-thirds of DLB patients but only one-third of PDDpatients show a positive amyloid-beta PET scan (Donaghy
et al 2015) suggesting a differential contribution of amyloid-beta to the manifestation of cognitive impairment and itstiming in PD and DLB (reviewed in Meyer et al 2014) Recent[18F]FDG PET studies also support the notion that PD with MCI(PD-MCI) represents a prodromal stage of PDD (Litvan et al 2012) Similar to the pattern observed in PDD PD-MCIpatients typically exhibit a decreased temporoparietal occipi-tal precuneus and frontal metabolism when compared tohealthy controls and to a lesser extent to PD patients withoutMCI (Garcia-Garcia et al 2012 Hosokai et al 2009 Pappatagrave et al 2011) These changes are more pronounced in multi-domain compared to single-domain MCI (Huang et al 2008Lyoo et al 2010) and correlate with overall cognitive perform-ance across patients with PD PD-MCI and PDD (Garcia-Garcia et al 2012 Meyer et al 2014) Finally conversion from
PD to PDD was predicted by hypometabolism in posteriorcingulate occipital cortex (BA1819) and caudate nucleus while hypometabolism of the primary visual cortex (BA17) wasalso observed in cognitively stable PD patients Convertersshowed a widespread metabolic decline in several cortical andsubcortical areas on follow-up imaging (Bohnen et al 2011)
Frontotemporal Dementia
FTD probably represents the third most common overall causeof neurodegenerative dementia FTD refers to a heterogeneousgroup of syndromes characterized by predominant deficits inbehavior language and executive functions that are caused
et al 2009) is relatively preserved in DLB compared to ADoffering a high specificity for DLB However differencesbetween AD and DLB may be hard to appreciate in routineclinical examination of individual patients In this situation
PET or SPECT examinations of nigrostriatal integrity (mostnotably [123I]FP-CIT SPECT) can be very helpful in differentiat-ing between AD and DLB (McKeith et al 2007) A recentmeta-analysis indicated a pooled sensitivity and specificity of[123I]FP-CIT SPECT for DLB of 87 and 94 respectively(Papathanasiou et al 2012) Furthermore in a direct compari-son of [18F]FDG PET and dopamine transporter (DAT) SPECTthe latter was found to be superior for the differential diagnosisof DLB versus AD (Lim et al 2009) In line with this striatalDAT loss is defined as a suggestive feature in the current diag-nostic criteria for DLB while occipital hypometabolism is a supportive feature (McKeith et al 2005) Of note nigrostriatalprojections may also be damaged in FTD (Rinne et al 2002)and atypical parkinsonian syndromes with dementia (eg PSPand CBD see later section Parkinsonism) Concerning a pos-
sible prodromal stage of DLB it has been shown that primary visual cortex hypometabolism is associated with clinical corefeatures of DLB in as yet nondemented memory clinic patients(Fujishiro et al 2012) Those who converted to DLB duringfollow-up showed a more pronounced lateral occipital andparietal hypometabolism (Fujishiro et al 2013)
DLB is clinically distinguished from Parkinson disease (PD) with dementia (PDD) by the so-called 1-year rule In line withthe notion that both diseases most likely represent manifesta-tions of the same disease spectrum (Lewy body disease spec-trum) (Lippa et al 2007) [18F]FDG PET studies in PDD(Peppard et al 1992 Vander Borght et al 1997) found results very similar to those in DLB In fact in a direct comparison of
Fig 415 [18F]FDG PET in dementia with Lewy bodies (DLB) This disorder affects similar areas as those affected by Alzheimer disease (AD)
Occipital cortex is also involved which may distinguish DLB from AD in turn the mesiotemporal lobe is relatively spared in DLB A very similar
if not identical pattern is observed in Parkinson disease with dementia (PDD) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for addi-
tional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 723
492 PART II Neurological Investigations and Related Clinical Neurosciences
in an autopsy-confirmed study which was clearly superior toclinical diagnosis alone (Foster et al 2007) Consequentlyfrontal or anterior temporal hypoperfusion or hypometabo-lism was incorporated as a criterion for probable bvFTD intothe revised diagnostic criteria (Rascovsky et al 2011) Anormal [18F]FDG PET may be particularly helpful to assure ahigh specificity of the clinical diagnosis of bvFTD by identify-ing ldquophenocopiesrdquo (Kipps et al 2009) Patients with svPPAtypically show a predominant hypometabolism of the rostraltemporal lobes which is usually leftward asymmetrical (seeFig 413) (Diehl et al 2004 Rabinovici et al 2008) Thispattern distinguishes patients with svPPA from those withlvPPA that present a more posterior temporoparietal hypome-tabolism (as a nonamnestic AD manifestation see earlier)Finally opposed to the postrolandic hypometabolism foundin lvPPA and svPPA patients with nfvPPA exhibit a left frontalhypometabolism with inferior frontal or posterior fronto-insular emphasis (see Fig 413) (Josephs et al 2010 Nestor et al 2003 Rabinovici et al 2008) The aforementionedPPA-related patterns of hypometabolism on [18F]FDG PET (orhypoperfusion on SPECT) are also necessary findings to makethe diagnosis of imaging-supported lvPPA svPPA or nfvPPAaccording to the recently proposed classification (Gorno- Tempini et al 2011)
Vascular Dementia
Finally pure vascular dementia (VD) seems to be rather rarein North America and Europe and more prevalent in Japan atleast when several large cortical infarcts are seen as the causeof the dementia (so called multi-infarct dementia) But Bin-swanger disease or subcortical arteriosclerotic encephalopathymay be underdiagnosed or mistaken as ldquovascular changesrdquo in
by a progressive degeneration of frontal andor temporallobes FTD can be clinically subdivided into three major syn-dromes behavioral variant frontotemporal dementia (bvFTDprominent behavioralcognitive symptoms like disinhibitionapathy or executive deficits) semantic variant primary pro-gressive aphasia (svPPA prominent confrontation namingand single-word comprehension deficits) and nonfluent variant primary progressive aphasia (nfvPPA prominentagrammatism and motor speech difficulties) Although asso-ciations between clinical syndromes and underlying patholo-gies have been described (eg tauopathies like Pick disease orcorticobasal degeneration in nfvPPA tau-negative TDP-43- orFUS-positive aggregates in svPPA and bvFTD) clinical syn-dromes as well as pathologies may considerably overlap which hinders predicting the underlying pathology by theclinical phenotype (Kertesz et al 2005 Kertesz and McMona-gle 2011 Pressman and Miller 2014) In fact since patientsoften develop several syndromes during disease course leadingto a convergence of clinical presentations over time the clini-cal fractionation of this ldquoPick complexrdquo has been challenged(Kertesz et al 2005 Kertesz and McMonagle 2011) BvFTD isusually associated with a bilateral often asymmetrical frontalhypometabolism which is most pronounced in the mesial(polar) frontal cortex (Fig 416) (Garraux et al 1999 Salmon et al 2003) The striatum thalamus and temporal and pari-
etal cortices are also affected although to a lesser extent(Garraux et al 1999 Ishii et al 1998b) Despite the fact thatbvFTD and AD affect overlapping cortical areas the predomi-nance of frontal and temporoparietal deficits respectively isusually very apparent and allows a clear distinction betweenFTD and AD In line with this a voxel-based statistical analysisprovided a diagnostic accuracy of 90 (sensitivity 98 spe-cificity 86) for separating FTD (bvFTD and svPPA) and AD
Fig 416 [18F]FDG PET in behavioral variant of frontotemporal dementia (bvFTD) Bifrontal hypometabolism is usually found in FTD often
in a somewhat asymmetrical distribution as in this case At early stages frontomesial and frontopolar involvement is most pronounced while
parietal cortices can be affected later in disease course Top Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-based statistical
analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for additional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 823
Functional Neuroimaging 493
MSA-P) pons and cerebellum (especially in MSA-C) (Fig 418) In the case of PSP regional hypometabolism is consist-ently noted in medial dorso- and ventrolateral frontal areas(pronounced in anterior cingulate gyrus supplementarymotor and premotor areas) caudate nucleus (medial) thala-mus and upper brainstem (Fig 419) Finally CBD is charac-terized by a usually highly asymmetric hypometabolism offrontoparietal areas (pronounced parietal) motor cortex
middle cingulate gyrus striatum and thalamus contralateralto the most affected body side (Fig 4110) The aforemen-tioned results gained from categorical comparisons fit theresults gained from spatial covariance analyses These wereemployed to detect abnormal disease-related metabolic pat-terns in PD MSA and PSP (ie PDRP MSARP and PSPRPrespectively) which were demonstrated to be highly reproduc-ible to correlate with disease severity and duration and toallow for prospective discrimination between cohorts (Eckert et al 2008 Ma et al 2007 Poston et al 2012) The expres-sion of two distinctive spatial covariance patterns characterizesPD one related to motor manifestations (PDRP) and onerelated to cognitive manifestations (PDCP) The PDRP isalready significantly increased in the ipsilateral (ldquopresympto-maticrdquo) hemisphere of patients with hemi-parkinsonism
( Tang et al 2010b) Finally a very recent study (using [
18
F]FDG PET and CBF SPECT) demonstrated that PDRP is alsoincreased in REM sleep behavior disorder (RBD) being a sig-nificant predictor of phenoconversion to PD or DLB (Holt -bernd et al 2014) Thus covariance patterns of cerebralglucose metabolism represent very interesting biomarkers for(early) diagnosis and therapy monitoring in parkinsonism(Hirano et al 2009)
PSP and CBD may be considered to represent differentmanifestations of a disease spectrum with several commonclinical pathological genetic and biochemical features (Kouri et al 2011) This issue gets even more complex if one consid-ers that FTD is often caused by PSP and CBD pathology (see
AD [18F]FDG PET adds little to the diagnosis of VD In agree-ment with CT and MRI PET may show defects of [18F]FDGuptake corresponding to ischemic infarcts in all cerebralregions including primary cortices striatumthalamus andcerebellum Since the latter are usually well preserved in ADdefects in these regions can be an important diagnostic clueDeficits due to vascular lesions can be considerably larger orcause remote deficits of [18F]FDG uptake due to diaschisisFurthermore cerebral glucose metabolism was reported to beglobally reduced (Mielke et al 1992) but without absolutequantification this finding cannot be reliably assessed
Parkinsonism
An early and correct differential diagnosis of parkinsonism isof paramount therapeutic and prognostic importance giventhe possible excellent treatment options and prognosis inpatients without nigrostriatal degeneration (eg drug-inducedparkinsonism essential tremor) and the limited responsive-ness to levodopa and faster progression to disability and deathin patients with atypical parkinsonism syndromes (APS) com-pared to PD (Kempster et al 2007 OrsquoSullivan et al 2008)However postmortem studies suggest that the clinical diagno-sis of PD as the most frequent cause of parkinsonism isincorrect in about 25 of patients ( Tolosa et al 2006) Fre-
quent misdiagnoses include secondary parkinsonism and APSlike multiple system atrophy (MSA) PSP and CBD In turncumulative clinicopathological data suggest that about 30of MSA and PSP and up to 74 of CBD patients are not cor-rectly diagnosed even at late stage (Ling et al 2010)
Against this background SPECT and PET are used with twoaims first to identify patients with progressive nigrostriataldegeneration which is the common pathological feature inPD MSA PSP and CBD Second to differentiate between thelatter patient groups Accurate diagnosis of neurodegenerativeparkinsonism can be achieved by imaging nigrostriatal func-tion (most notably [123I]FP-CIT SPECT) (Benamer et al 2000Benitez-Rivero et al 2013 Marshall et al 2009) (For a moredetailed overview on nigrostriatal imaging in parkinsonismplease refer to Chapter 42) However dopamine transporter
imaging does not allow for a reliable differential diagnosis ofPD MSA PSP and CBD (Meyer and Hellwig 2014) Instead[18F]FDG PET has gained acceptance as the method of choicehere It surpasses the diagnostic accuracies of other commontechniques like imaging cardiac sympathetic innervation (egusing [123I]metaiodobenzylguanidine ([123I]MIBG) scintigra-phy) or imaging of striatal dopamine D2D3 receptors (egusing [123I]iodobenzamide([ 123I]IBZM)) (Meyer and Hellwig 2014) Assessment of regional CBF changes with SPECT mayalso be used for this purpose (eg Eckert et al 2007)However since [18F]FDG PET is technically superior and also widely available we will focus on [18F]FDG PET
[18F]FDG PET shows disease-specific alterations of cerebralglucose metabolism (eg Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Teune et al 2010) scans in PD patients
often show no major abnormality on first glance On closerinspection and especially on voxel-based statistical analysesPD is characterized by a posterior temporoparietal occipitaland sometimes frontal hypometabolism (especially in PD withmild cognitive impairment and PDD) and a relative hyperme-tabolism of putamen globus pallidus sensorimotor cortexpons and cerebellum (Fig 417) Interestingly temporoparieto-occipital hypometabolism may also seen in nondementedPD patients (Hellwig et al 2012 Hu et al 2000) possiblyindicating an increased risk of subsequent development ofPDD (see earlier section on Dementia and Mild Cognitive Impairment ) Conversely MSA patients show a markedhypometabolism of striatum (posterior putamen especially in
Fig 417 [18F]FDG PET in Parkinson disease (PD) PD is typically
characterized by (relative) striatal hypermetabolism Temporoparietal
occipital and sometime frontal hypometabolism can be observed in a
significant fraction of PD patients without apparent cognitive impair-
ment Cortical hypometabolism can be fairly pronounced possiblyrepresenting a risk factor for subsequent development of PDD Top
Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-
based statistical analysis using Neurostat3D-SSP Given are right and
left lateral superior and posterior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 523
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 623
Functional Neuroimaging 491
both groups there were only minor differences if any ( Yong et al 2007) However according to a recent meta-analysisabout two-thirds of DLB patients but only one-third of PDDpatients show a positive amyloid-beta PET scan (Donaghy
et al 2015) suggesting a differential contribution of amyloid-beta to the manifestation of cognitive impairment and itstiming in PD and DLB (reviewed in Meyer et al 2014) Recent[18F]FDG PET studies also support the notion that PD with MCI(PD-MCI) represents a prodromal stage of PDD (Litvan et al 2012) Similar to the pattern observed in PDD PD-MCIpatients typically exhibit a decreased temporoparietal occipi-tal precuneus and frontal metabolism when compared tohealthy controls and to a lesser extent to PD patients withoutMCI (Garcia-Garcia et al 2012 Hosokai et al 2009 Pappatagrave et al 2011) These changes are more pronounced in multi-domain compared to single-domain MCI (Huang et al 2008Lyoo et al 2010) and correlate with overall cognitive perform-ance across patients with PD PD-MCI and PDD (Garcia-Garcia et al 2012 Meyer et al 2014) Finally conversion from
PD to PDD was predicted by hypometabolism in posteriorcingulate occipital cortex (BA1819) and caudate nucleus while hypometabolism of the primary visual cortex (BA17) wasalso observed in cognitively stable PD patients Convertersshowed a widespread metabolic decline in several cortical andsubcortical areas on follow-up imaging (Bohnen et al 2011)
Frontotemporal Dementia
FTD probably represents the third most common overall causeof neurodegenerative dementia FTD refers to a heterogeneousgroup of syndromes characterized by predominant deficits inbehavior language and executive functions that are caused
et al 2009) is relatively preserved in DLB compared to ADoffering a high specificity for DLB However differencesbetween AD and DLB may be hard to appreciate in routineclinical examination of individual patients In this situation
PET or SPECT examinations of nigrostriatal integrity (mostnotably [123I]FP-CIT SPECT) can be very helpful in differentiat-ing between AD and DLB (McKeith et al 2007) A recentmeta-analysis indicated a pooled sensitivity and specificity of[123I]FP-CIT SPECT for DLB of 87 and 94 respectively(Papathanasiou et al 2012) Furthermore in a direct compari-son of [18F]FDG PET and dopamine transporter (DAT) SPECTthe latter was found to be superior for the differential diagnosisof DLB versus AD (Lim et al 2009) In line with this striatalDAT loss is defined as a suggestive feature in the current diag-nostic criteria for DLB while occipital hypometabolism is a supportive feature (McKeith et al 2005) Of note nigrostriatalprojections may also be damaged in FTD (Rinne et al 2002)and atypical parkinsonian syndromes with dementia (eg PSPand CBD see later section Parkinsonism) Concerning a pos-
sible prodromal stage of DLB it has been shown that primary visual cortex hypometabolism is associated with clinical corefeatures of DLB in as yet nondemented memory clinic patients(Fujishiro et al 2012) Those who converted to DLB duringfollow-up showed a more pronounced lateral occipital andparietal hypometabolism (Fujishiro et al 2013)
DLB is clinically distinguished from Parkinson disease (PD) with dementia (PDD) by the so-called 1-year rule In line withthe notion that both diseases most likely represent manifesta-tions of the same disease spectrum (Lewy body disease spec-trum) (Lippa et al 2007) [18F]FDG PET studies in PDD(Peppard et al 1992 Vander Borght et al 1997) found results very similar to those in DLB In fact in a direct comparison of
Fig 415 [18F]FDG PET in dementia with Lewy bodies (DLB) This disorder affects similar areas as those affected by Alzheimer disease (AD)
Occipital cortex is also involved which may distinguish DLB from AD in turn the mesiotemporal lobe is relatively spared in DLB A very similar
if not identical pattern is observed in Parkinson disease with dementia (PDD) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for addi-
tional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 723
492 PART II Neurological Investigations and Related Clinical Neurosciences
in an autopsy-confirmed study which was clearly superior toclinical diagnosis alone (Foster et al 2007) Consequentlyfrontal or anterior temporal hypoperfusion or hypometabo-lism was incorporated as a criterion for probable bvFTD intothe revised diagnostic criteria (Rascovsky et al 2011) Anormal [18F]FDG PET may be particularly helpful to assure ahigh specificity of the clinical diagnosis of bvFTD by identify-ing ldquophenocopiesrdquo (Kipps et al 2009) Patients with svPPAtypically show a predominant hypometabolism of the rostraltemporal lobes which is usually leftward asymmetrical (seeFig 413) (Diehl et al 2004 Rabinovici et al 2008) Thispattern distinguishes patients with svPPA from those withlvPPA that present a more posterior temporoparietal hypome-tabolism (as a nonamnestic AD manifestation see earlier)Finally opposed to the postrolandic hypometabolism foundin lvPPA and svPPA patients with nfvPPA exhibit a left frontalhypometabolism with inferior frontal or posterior fronto-insular emphasis (see Fig 413) (Josephs et al 2010 Nestor et al 2003 Rabinovici et al 2008) The aforementionedPPA-related patterns of hypometabolism on [18F]FDG PET (orhypoperfusion on SPECT) are also necessary findings to makethe diagnosis of imaging-supported lvPPA svPPA or nfvPPAaccording to the recently proposed classification (Gorno- Tempini et al 2011)
Vascular Dementia
Finally pure vascular dementia (VD) seems to be rather rarein North America and Europe and more prevalent in Japan atleast when several large cortical infarcts are seen as the causeof the dementia (so called multi-infarct dementia) But Bin-swanger disease or subcortical arteriosclerotic encephalopathymay be underdiagnosed or mistaken as ldquovascular changesrdquo in
by a progressive degeneration of frontal andor temporallobes FTD can be clinically subdivided into three major syn-dromes behavioral variant frontotemporal dementia (bvFTDprominent behavioralcognitive symptoms like disinhibitionapathy or executive deficits) semantic variant primary pro-gressive aphasia (svPPA prominent confrontation namingand single-word comprehension deficits) and nonfluent variant primary progressive aphasia (nfvPPA prominentagrammatism and motor speech difficulties) Although asso-ciations between clinical syndromes and underlying patholo-gies have been described (eg tauopathies like Pick disease orcorticobasal degeneration in nfvPPA tau-negative TDP-43- orFUS-positive aggregates in svPPA and bvFTD) clinical syn-dromes as well as pathologies may considerably overlap which hinders predicting the underlying pathology by theclinical phenotype (Kertesz et al 2005 Kertesz and McMona-gle 2011 Pressman and Miller 2014) In fact since patientsoften develop several syndromes during disease course leadingto a convergence of clinical presentations over time the clini-cal fractionation of this ldquoPick complexrdquo has been challenged(Kertesz et al 2005 Kertesz and McMonagle 2011) BvFTD isusually associated with a bilateral often asymmetrical frontalhypometabolism which is most pronounced in the mesial(polar) frontal cortex (Fig 416) (Garraux et al 1999 Salmon et al 2003) The striatum thalamus and temporal and pari-
etal cortices are also affected although to a lesser extent(Garraux et al 1999 Ishii et al 1998b) Despite the fact thatbvFTD and AD affect overlapping cortical areas the predomi-nance of frontal and temporoparietal deficits respectively isusually very apparent and allows a clear distinction betweenFTD and AD In line with this a voxel-based statistical analysisprovided a diagnostic accuracy of 90 (sensitivity 98 spe-cificity 86) for separating FTD (bvFTD and svPPA) and AD
Fig 416 [18F]FDG PET in behavioral variant of frontotemporal dementia (bvFTD) Bifrontal hypometabolism is usually found in FTD often
in a somewhat asymmetrical distribution as in this case At early stages frontomesial and frontopolar involvement is most pronounced while
parietal cortices can be affected later in disease course Top Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-based statistical
analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for additional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 823
Functional Neuroimaging 493
MSA-P) pons and cerebellum (especially in MSA-C) (Fig 418) In the case of PSP regional hypometabolism is consist-ently noted in medial dorso- and ventrolateral frontal areas(pronounced in anterior cingulate gyrus supplementarymotor and premotor areas) caudate nucleus (medial) thala-mus and upper brainstem (Fig 419) Finally CBD is charac-terized by a usually highly asymmetric hypometabolism offrontoparietal areas (pronounced parietal) motor cortex
middle cingulate gyrus striatum and thalamus contralateralto the most affected body side (Fig 4110) The aforemen-tioned results gained from categorical comparisons fit theresults gained from spatial covariance analyses These wereemployed to detect abnormal disease-related metabolic pat-terns in PD MSA and PSP (ie PDRP MSARP and PSPRPrespectively) which were demonstrated to be highly reproduc-ible to correlate with disease severity and duration and toallow for prospective discrimination between cohorts (Eckert et al 2008 Ma et al 2007 Poston et al 2012) The expres-sion of two distinctive spatial covariance patterns characterizesPD one related to motor manifestations (PDRP) and onerelated to cognitive manifestations (PDCP) The PDRP isalready significantly increased in the ipsilateral (ldquopresympto-maticrdquo) hemisphere of patients with hemi-parkinsonism
( Tang et al 2010b) Finally a very recent study (using [
18
F]FDG PET and CBF SPECT) demonstrated that PDRP is alsoincreased in REM sleep behavior disorder (RBD) being a sig-nificant predictor of phenoconversion to PD or DLB (Holt -bernd et al 2014) Thus covariance patterns of cerebralglucose metabolism represent very interesting biomarkers for(early) diagnosis and therapy monitoring in parkinsonism(Hirano et al 2009)
PSP and CBD may be considered to represent differentmanifestations of a disease spectrum with several commonclinical pathological genetic and biochemical features (Kouri et al 2011) This issue gets even more complex if one consid-ers that FTD is often caused by PSP and CBD pathology (see
AD [18F]FDG PET adds little to the diagnosis of VD In agree-ment with CT and MRI PET may show defects of [18F]FDGuptake corresponding to ischemic infarcts in all cerebralregions including primary cortices striatumthalamus andcerebellum Since the latter are usually well preserved in ADdefects in these regions can be an important diagnostic clueDeficits due to vascular lesions can be considerably larger orcause remote deficits of [18F]FDG uptake due to diaschisisFurthermore cerebral glucose metabolism was reported to beglobally reduced (Mielke et al 1992) but without absolutequantification this finding cannot be reliably assessed
Parkinsonism
An early and correct differential diagnosis of parkinsonism isof paramount therapeutic and prognostic importance giventhe possible excellent treatment options and prognosis inpatients without nigrostriatal degeneration (eg drug-inducedparkinsonism essential tremor) and the limited responsive-ness to levodopa and faster progression to disability and deathin patients with atypical parkinsonism syndromes (APS) com-pared to PD (Kempster et al 2007 OrsquoSullivan et al 2008)However postmortem studies suggest that the clinical diagno-sis of PD as the most frequent cause of parkinsonism isincorrect in about 25 of patients ( Tolosa et al 2006) Fre-
quent misdiagnoses include secondary parkinsonism and APSlike multiple system atrophy (MSA) PSP and CBD In turncumulative clinicopathological data suggest that about 30of MSA and PSP and up to 74 of CBD patients are not cor-rectly diagnosed even at late stage (Ling et al 2010)
Against this background SPECT and PET are used with twoaims first to identify patients with progressive nigrostriataldegeneration which is the common pathological feature inPD MSA PSP and CBD Second to differentiate between thelatter patient groups Accurate diagnosis of neurodegenerativeparkinsonism can be achieved by imaging nigrostriatal func-tion (most notably [123I]FP-CIT SPECT) (Benamer et al 2000Benitez-Rivero et al 2013 Marshall et al 2009) (For a moredetailed overview on nigrostriatal imaging in parkinsonismplease refer to Chapter 42) However dopamine transporter
imaging does not allow for a reliable differential diagnosis ofPD MSA PSP and CBD (Meyer and Hellwig 2014) Instead[18F]FDG PET has gained acceptance as the method of choicehere It surpasses the diagnostic accuracies of other commontechniques like imaging cardiac sympathetic innervation (egusing [123I]metaiodobenzylguanidine ([123I]MIBG) scintigra-phy) or imaging of striatal dopamine D2D3 receptors (egusing [123I]iodobenzamide([ 123I]IBZM)) (Meyer and Hellwig 2014) Assessment of regional CBF changes with SPECT mayalso be used for this purpose (eg Eckert et al 2007)However since [18F]FDG PET is technically superior and also widely available we will focus on [18F]FDG PET
[18F]FDG PET shows disease-specific alterations of cerebralglucose metabolism (eg Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Teune et al 2010) scans in PD patients
often show no major abnormality on first glance On closerinspection and especially on voxel-based statistical analysesPD is characterized by a posterior temporoparietal occipitaland sometimes frontal hypometabolism (especially in PD withmild cognitive impairment and PDD) and a relative hyperme-tabolism of putamen globus pallidus sensorimotor cortexpons and cerebellum (Fig 417) Interestingly temporoparieto-occipital hypometabolism may also seen in nondementedPD patients (Hellwig et al 2012 Hu et al 2000) possiblyindicating an increased risk of subsequent development ofPDD (see earlier section on Dementia and Mild Cognitive Impairment ) Conversely MSA patients show a markedhypometabolism of striatum (posterior putamen especially in
Fig 417 [18F]FDG PET in Parkinson disease (PD) PD is typically
characterized by (relative) striatal hypermetabolism Temporoparietal
occipital and sometime frontal hypometabolism can be observed in a
significant fraction of PD patients without apparent cognitive impair-
ment Cortical hypometabolism can be fairly pronounced possiblyrepresenting a risk factor for subsequent development of PDD Top
Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-
based statistical analysis using Neurostat3D-SSP Given are right and
left lateral superior and posterior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 623
Functional Neuroimaging 491
both groups there were only minor differences if any ( Yong et al 2007) However according to a recent meta-analysisabout two-thirds of DLB patients but only one-third of PDDpatients show a positive amyloid-beta PET scan (Donaghy
et al 2015) suggesting a differential contribution of amyloid-beta to the manifestation of cognitive impairment and itstiming in PD and DLB (reviewed in Meyer et al 2014) Recent[18F]FDG PET studies also support the notion that PD with MCI(PD-MCI) represents a prodromal stage of PDD (Litvan et al 2012) Similar to the pattern observed in PDD PD-MCIpatients typically exhibit a decreased temporoparietal occipi-tal precuneus and frontal metabolism when compared tohealthy controls and to a lesser extent to PD patients withoutMCI (Garcia-Garcia et al 2012 Hosokai et al 2009 Pappatagrave et al 2011) These changes are more pronounced in multi-domain compared to single-domain MCI (Huang et al 2008Lyoo et al 2010) and correlate with overall cognitive perform-ance across patients with PD PD-MCI and PDD (Garcia-Garcia et al 2012 Meyer et al 2014) Finally conversion from
PD to PDD was predicted by hypometabolism in posteriorcingulate occipital cortex (BA1819) and caudate nucleus while hypometabolism of the primary visual cortex (BA17) wasalso observed in cognitively stable PD patients Convertersshowed a widespread metabolic decline in several cortical andsubcortical areas on follow-up imaging (Bohnen et al 2011)
Frontotemporal Dementia
FTD probably represents the third most common overall causeof neurodegenerative dementia FTD refers to a heterogeneousgroup of syndromes characterized by predominant deficits inbehavior language and executive functions that are caused
et al 2009) is relatively preserved in DLB compared to ADoffering a high specificity for DLB However differencesbetween AD and DLB may be hard to appreciate in routineclinical examination of individual patients In this situation
PET or SPECT examinations of nigrostriatal integrity (mostnotably [123I]FP-CIT SPECT) can be very helpful in differentiat-ing between AD and DLB (McKeith et al 2007) A recentmeta-analysis indicated a pooled sensitivity and specificity of[123I]FP-CIT SPECT for DLB of 87 and 94 respectively(Papathanasiou et al 2012) Furthermore in a direct compari-son of [18F]FDG PET and dopamine transporter (DAT) SPECTthe latter was found to be superior for the differential diagnosisof DLB versus AD (Lim et al 2009) In line with this striatalDAT loss is defined as a suggestive feature in the current diag-nostic criteria for DLB while occipital hypometabolism is a supportive feature (McKeith et al 2005) Of note nigrostriatalprojections may also be damaged in FTD (Rinne et al 2002)and atypical parkinsonian syndromes with dementia (eg PSPand CBD see later section Parkinsonism) Concerning a pos-
sible prodromal stage of DLB it has been shown that primary visual cortex hypometabolism is associated with clinical corefeatures of DLB in as yet nondemented memory clinic patients(Fujishiro et al 2012) Those who converted to DLB duringfollow-up showed a more pronounced lateral occipital andparietal hypometabolism (Fujishiro et al 2013)
DLB is clinically distinguished from Parkinson disease (PD) with dementia (PDD) by the so-called 1-year rule In line withthe notion that both diseases most likely represent manifesta-tions of the same disease spectrum (Lewy body disease spec-trum) (Lippa et al 2007) [18F]FDG PET studies in PDD(Peppard et al 1992 Vander Borght et al 1997) found results very similar to those in DLB In fact in a direct comparison of
Fig 415 [18F]FDG PET in dementia with Lewy bodies (DLB) This disorder affects similar areas as those affected by Alzheimer disease (AD)
Occipital cortex is also involved which may distinguish DLB from AD in turn the mesiotemporal lobe is relatively spared in DLB A very similar
if not identical pattern is observed in Parkinson disease with dementia (PDD) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for addi-
tional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 723
492 PART II Neurological Investigations and Related Clinical Neurosciences
in an autopsy-confirmed study which was clearly superior toclinical diagnosis alone (Foster et al 2007) Consequentlyfrontal or anterior temporal hypoperfusion or hypometabo-lism was incorporated as a criterion for probable bvFTD intothe revised diagnostic criteria (Rascovsky et al 2011) Anormal [18F]FDG PET may be particularly helpful to assure ahigh specificity of the clinical diagnosis of bvFTD by identify-ing ldquophenocopiesrdquo (Kipps et al 2009) Patients with svPPAtypically show a predominant hypometabolism of the rostraltemporal lobes which is usually leftward asymmetrical (seeFig 413) (Diehl et al 2004 Rabinovici et al 2008) Thispattern distinguishes patients with svPPA from those withlvPPA that present a more posterior temporoparietal hypome-tabolism (as a nonamnestic AD manifestation see earlier)Finally opposed to the postrolandic hypometabolism foundin lvPPA and svPPA patients with nfvPPA exhibit a left frontalhypometabolism with inferior frontal or posterior fronto-insular emphasis (see Fig 413) (Josephs et al 2010 Nestor et al 2003 Rabinovici et al 2008) The aforementionedPPA-related patterns of hypometabolism on [18F]FDG PET (orhypoperfusion on SPECT) are also necessary findings to makethe diagnosis of imaging-supported lvPPA svPPA or nfvPPAaccording to the recently proposed classification (Gorno- Tempini et al 2011)
Vascular Dementia
Finally pure vascular dementia (VD) seems to be rather rarein North America and Europe and more prevalent in Japan atleast when several large cortical infarcts are seen as the causeof the dementia (so called multi-infarct dementia) But Bin-swanger disease or subcortical arteriosclerotic encephalopathymay be underdiagnosed or mistaken as ldquovascular changesrdquo in
by a progressive degeneration of frontal andor temporallobes FTD can be clinically subdivided into three major syn-dromes behavioral variant frontotemporal dementia (bvFTDprominent behavioralcognitive symptoms like disinhibitionapathy or executive deficits) semantic variant primary pro-gressive aphasia (svPPA prominent confrontation namingand single-word comprehension deficits) and nonfluent variant primary progressive aphasia (nfvPPA prominentagrammatism and motor speech difficulties) Although asso-ciations between clinical syndromes and underlying patholo-gies have been described (eg tauopathies like Pick disease orcorticobasal degeneration in nfvPPA tau-negative TDP-43- orFUS-positive aggregates in svPPA and bvFTD) clinical syn-dromes as well as pathologies may considerably overlap which hinders predicting the underlying pathology by theclinical phenotype (Kertesz et al 2005 Kertesz and McMona-gle 2011 Pressman and Miller 2014) In fact since patientsoften develop several syndromes during disease course leadingto a convergence of clinical presentations over time the clini-cal fractionation of this ldquoPick complexrdquo has been challenged(Kertesz et al 2005 Kertesz and McMonagle 2011) BvFTD isusually associated with a bilateral often asymmetrical frontalhypometabolism which is most pronounced in the mesial(polar) frontal cortex (Fig 416) (Garraux et al 1999 Salmon et al 2003) The striatum thalamus and temporal and pari-
etal cortices are also affected although to a lesser extent(Garraux et al 1999 Ishii et al 1998b) Despite the fact thatbvFTD and AD affect overlapping cortical areas the predomi-nance of frontal and temporoparietal deficits respectively isusually very apparent and allows a clear distinction betweenFTD and AD In line with this a voxel-based statistical analysisprovided a diagnostic accuracy of 90 (sensitivity 98 spe-cificity 86) for separating FTD (bvFTD and svPPA) and AD
Fig 416 [18F]FDG PET in behavioral variant of frontotemporal dementia (bvFTD) Bifrontal hypometabolism is usually found in FTD often
in a somewhat asymmetrical distribution as in this case At early stages frontomesial and frontopolar involvement is most pronounced while
parietal cortices can be affected later in disease course Top Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-based statistical
analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for additional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 823
Functional Neuroimaging 493
MSA-P) pons and cerebellum (especially in MSA-C) (Fig 418) In the case of PSP regional hypometabolism is consist-ently noted in medial dorso- and ventrolateral frontal areas(pronounced in anterior cingulate gyrus supplementarymotor and premotor areas) caudate nucleus (medial) thala-mus and upper brainstem (Fig 419) Finally CBD is charac-terized by a usually highly asymmetric hypometabolism offrontoparietal areas (pronounced parietal) motor cortex
middle cingulate gyrus striatum and thalamus contralateralto the most affected body side (Fig 4110) The aforemen-tioned results gained from categorical comparisons fit theresults gained from spatial covariance analyses These wereemployed to detect abnormal disease-related metabolic pat-terns in PD MSA and PSP (ie PDRP MSARP and PSPRPrespectively) which were demonstrated to be highly reproduc-ible to correlate with disease severity and duration and toallow for prospective discrimination between cohorts (Eckert et al 2008 Ma et al 2007 Poston et al 2012) The expres-sion of two distinctive spatial covariance patterns characterizesPD one related to motor manifestations (PDRP) and onerelated to cognitive manifestations (PDCP) The PDRP isalready significantly increased in the ipsilateral (ldquopresympto-maticrdquo) hemisphere of patients with hemi-parkinsonism
( Tang et al 2010b) Finally a very recent study (using [
18
F]FDG PET and CBF SPECT) demonstrated that PDRP is alsoincreased in REM sleep behavior disorder (RBD) being a sig-nificant predictor of phenoconversion to PD or DLB (Holt -bernd et al 2014) Thus covariance patterns of cerebralglucose metabolism represent very interesting biomarkers for(early) diagnosis and therapy monitoring in parkinsonism(Hirano et al 2009)
PSP and CBD may be considered to represent differentmanifestations of a disease spectrum with several commonclinical pathological genetic and biochemical features (Kouri et al 2011) This issue gets even more complex if one consid-ers that FTD is often caused by PSP and CBD pathology (see
AD [18F]FDG PET adds little to the diagnosis of VD In agree-ment with CT and MRI PET may show defects of [18F]FDGuptake corresponding to ischemic infarcts in all cerebralregions including primary cortices striatumthalamus andcerebellum Since the latter are usually well preserved in ADdefects in these regions can be an important diagnostic clueDeficits due to vascular lesions can be considerably larger orcause remote deficits of [18F]FDG uptake due to diaschisisFurthermore cerebral glucose metabolism was reported to beglobally reduced (Mielke et al 1992) but without absolutequantification this finding cannot be reliably assessed
Parkinsonism
An early and correct differential diagnosis of parkinsonism isof paramount therapeutic and prognostic importance giventhe possible excellent treatment options and prognosis inpatients without nigrostriatal degeneration (eg drug-inducedparkinsonism essential tremor) and the limited responsive-ness to levodopa and faster progression to disability and deathin patients with atypical parkinsonism syndromes (APS) com-pared to PD (Kempster et al 2007 OrsquoSullivan et al 2008)However postmortem studies suggest that the clinical diagno-sis of PD as the most frequent cause of parkinsonism isincorrect in about 25 of patients ( Tolosa et al 2006) Fre-
quent misdiagnoses include secondary parkinsonism and APSlike multiple system atrophy (MSA) PSP and CBD In turncumulative clinicopathological data suggest that about 30of MSA and PSP and up to 74 of CBD patients are not cor-rectly diagnosed even at late stage (Ling et al 2010)
Against this background SPECT and PET are used with twoaims first to identify patients with progressive nigrostriataldegeneration which is the common pathological feature inPD MSA PSP and CBD Second to differentiate between thelatter patient groups Accurate diagnosis of neurodegenerativeparkinsonism can be achieved by imaging nigrostriatal func-tion (most notably [123I]FP-CIT SPECT) (Benamer et al 2000Benitez-Rivero et al 2013 Marshall et al 2009) (For a moredetailed overview on nigrostriatal imaging in parkinsonismplease refer to Chapter 42) However dopamine transporter
imaging does not allow for a reliable differential diagnosis ofPD MSA PSP and CBD (Meyer and Hellwig 2014) Instead[18F]FDG PET has gained acceptance as the method of choicehere It surpasses the diagnostic accuracies of other commontechniques like imaging cardiac sympathetic innervation (egusing [123I]metaiodobenzylguanidine ([123I]MIBG) scintigra-phy) or imaging of striatal dopamine D2D3 receptors (egusing [123I]iodobenzamide([ 123I]IBZM)) (Meyer and Hellwig 2014) Assessment of regional CBF changes with SPECT mayalso be used for this purpose (eg Eckert et al 2007)However since [18F]FDG PET is technically superior and also widely available we will focus on [18F]FDG PET
[18F]FDG PET shows disease-specific alterations of cerebralglucose metabolism (eg Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Teune et al 2010) scans in PD patients
often show no major abnormality on first glance On closerinspection and especially on voxel-based statistical analysesPD is characterized by a posterior temporoparietal occipitaland sometimes frontal hypometabolism (especially in PD withmild cognitive impairment and PDD) and a relative hyperme-tabolism of putamen globus pallidus sensorimotor cortexpons and cerebellum (Fig 417) Interestingly temporoparieto-occipital hypometabolism may also seen in nondementedPD patients (Hellwig et al 2012 Hu et al 2000) possiblyindicating an increased risk of subsequent development ofPDD (see earlier section on Dementia and Mild Cognitive Impairment ) Conversely MSA patients show a markedhypometabolism of striatum (posterior putamen especially in
Fig 417 [18F]FDG PET in Parkinson disease (PD) PD is typically
characterized by (relative) striatal hypermetabolism Temporoparietal
occipital and sometime frontal hypometabolism can be observed in a
significant fraction of PD patients without apparent cognitive impair-
ment Cortical hypometabolism can be fairly pronounced possiblyrepresenting a risk factor for subsequent development of PDD Top
Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-
based statistical analysis using Neurostat3D-SSP Given are right and
left lateral superior and posterior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
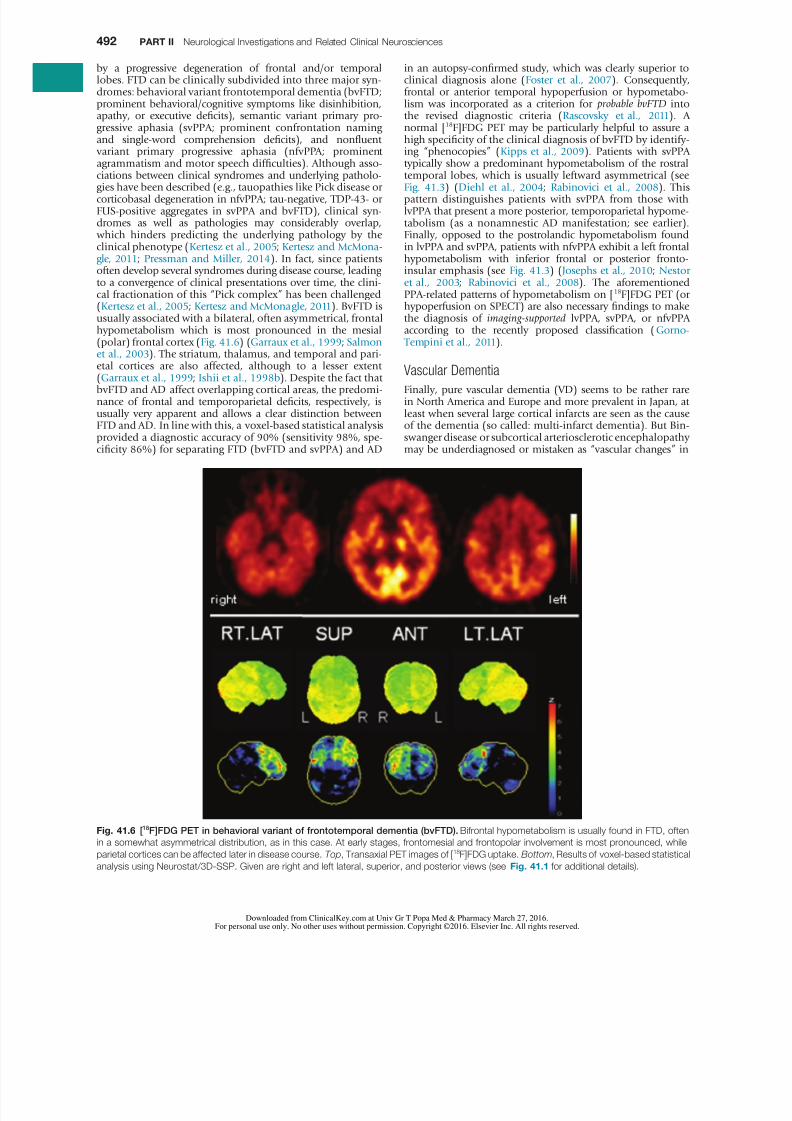
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 723
492 PART II Neurological Investigations and Related Clinical Neurosciences
in an autopsy-confirmed study which was clearly superior toclinical diagnosis alone (Foster et al 2007) Consequentlyfrontal or anterior temporal hypoperfusion or hypometabo-lism was incorporated as a criterion for probable bvFTD intothe revised diagnostic criteria (Rascovsky et al 2011) Anormal [18F]FDG PET may be particularly helpful to assure ahigh specificity of the clinical diagnosis of bvFTD by identify-ing ldquophenocopiesrdquo (Kipps et al 2009) Patients with svPPAtypically show a predominant hypometabolism of the rostraltemporal lobes which is usually leftward asymmetrical (seeFig 413) (Diehl et al 2004 Rabinovici et al 2008) Thispattern distinguishes patients with svPPA from those withlvPPA that present a more posterior temporoparietal hypome-tabolism (as a nonamnestic AD manifestation see earlier)Finally opposed to the postrolandic hypometabolism foundin lvPPA and svPPA patients with nfvPPA exhibit a left frontalhypometabolism with inferior frontal or posterior fronto-insular emphasis (see Fig 413) (Josephs et al 2010 Nestor et al 2003 Rabinovici et al 2008) The aforementionedPPA-related patterns of hypometabolism on [18F]FDG PET (orhypoperfusion on SPECT) are also necessary findings to makethe diagnosis of imaging-supported lvPPA svPPA or nfvPPAaccording to the recently proposed classification (Gorno- Tempini et al 2011)
Vascular Dementia
Finally pure vascular dementia (VD) seems to be rather rarein North America and Europe and more prevalent in Japan atleast when several large cortical infarcts are seen as the causeof the dementia (so called multi-infarct dementia) But Bin-swanger disease or subcortical arteriosclerotic encephalopathymay be underdiagnosed or mistaken as ldquovascular changesrdquo in
by a progressive degeneration of frontal andor temporallobes FTD can be clinically subdivided into three major syn-dromes behavioral variant frontotemporal dementia (bvFTDprominent behavioralcognitive symptoms like disinhibitionapathy or executive deficits) semantic variant primary pro-gressive aphasia (svPPA prominent confrontation namingand single-word comprehension deficits) and nonfluent variant primary progressive aphasia (nfvPPA prominentagrammatism and motor speech difficulties) Although asso-ciations between clinical syndromes and underlying patholo-gies have been described (eg tauopathies like Pick disease orcorticobasal degeneration in nfvPPA tau-negative TDP-43- orFUS-positive aggregates in svPPA and bvFTD) clinical syn-dromes as well as pathologies may considerably overlap which hinders predicting the underlying pathology by theclinical phenotype (Kertesz et al 2005 Kertesz and McMona-gle 2011 Pressman and Miller 2014) In fact since patientsoften develop several syndromes during disease course leadingto a convergence of clinical presentations over time the clini-cal fractionation of this ldquoPick complexrdquo has been challenged(Kertesz et al 2005 Kertesz and McMonagle 2011) BvFTD isusually associated with a bilateral often asymmetrical frontalhypometabolism which is most pronounced in the mesial(polar) frontal cortex (Fig 416) (Garraux et al 1999 Salmon et al 2003) The striatum thalamus and temporal and pari-
etal cortices are also affected although to a lesser extent(Garraux et al 1999 Ishii et al 1998b) Despite the fact thatbvFTD and AD affect overlapping cortical areas the predomi-nance of frontal and temporoparietal deficits respectively isusually very apparent and allows a clear distinction betweenFTD and AD In line with this a voxel-based statistical analysisprovided a diagnostic accuracy of 90 (sensitivity 98 spe-cificity 86) for separating FTD (bvFTD and svPPA) and AD
Fig 416 [18F]FDG PET in behavioral variant of frontotemporal dementia (bvFTD) Bifrontal hypometabolism is usually found in FTD often
in a somewhat asymmetrical distribution as in this case At early stages frontomesial and frontopolar involvement is most pronounced while
parietal cortices can be affected later in disease course Top Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-based statistical
analysis using Neurostat3D-SSP Given are right and left lateral superior and posterior views (see Fig 411 for additional details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 823
Functional Neuroimaging 493
MSA-P) pons and cerebellum (especially in MSA-C) (Fig 418) In the case of PSP regional hypometabolism is consist-ently noted in medial dorso- and ventrolateral frontal areas(pronounced in anterior cingulate gyrus supplementarymotor and premotor areas) caudate nucleus (medial) thala-mus and upper brainstem (Fig 419) Finally CBD is charac-terized by a usually highly asymmetric hypometabolism offrontoparietal areas (pronounced parietal) motor cortex
middle cingulate gyrus striatum and thalamus contralateralto the most affected body side (Fig 4110) The aforemen-tioned results gained from categorical comparisons fit theresults gained from spatial covariance analyses These wereemployed to detect abnormal disease-related metabolic pat-terns in PD MSA and PSP (ie PDRP MSARP and PSPRPrespectively) which were demonstrated to be highly reproduc-ible to correlate with disease severity and duration and toallow for prospective discrimination between cohorts (Eckert et al 2008 Ma et al 2007 Poston et al 2012) The expres-sion of two distinctive spatial covariance patterns characterizesPD one related to motor manifestations (PDRP) and onerelated to cognitive manifestations (PDCP) The PDRP isalready significantly increased in the ipsilateral (ldquopresympto-maticrdquo) hemisphere of patients with hemi-parkinsonism
( Tang et al 2010b) Finally a very recent study (using [
18
F]FDG PET and CBF SPECT) demonstrated that PDRP is alsoincreased in REM sleep behavior disorder (RBD) being a sig-nificant predictor of phenoconversion to PD or DLB (Holt -bernd et al 2014) Thus covariance patterns of cerebralglucose metabolism represent very interesting biomarkers for(early) diagnosis and therapy monitoring in parkinsonism(Hirano et al 2009)
PSP and CBD may be considered to represent differentmanifestations of a disease spectrum with several commonclinical pathological genetic and biochemical features (Kouri et al 2011) This issue gets even more complex if one consid-ers that FTD is often caused by PSP and CBD pathology (see
AD [18F]FDG PET adds little to the diagnosis of VD In agree-ment with CT and MRI PET may show defects of [18F]FDGuptake corresponding to ischemic infarcts in all cerebralregions including primary cortices striatumthalamus andcerebellum Since the latter are usually well preserved in ADdefects in these regions can be an important diagnostic clueDeficits due to vascular lesions can be considerably larger orcause remote deficits of [18F]FDG uptake due to diaschisisFurthermore cerebral glucose metabolism was reported to beglobally reduced (Mielke et al 1992) but without absolutequantification this finding cannot be reliably assessed
Parkinsonism
An early and correct differential diagnosis of parkinsonism isof paramount therapeutic and prognostic importance giventhe possible excellent treatment options and prognosis inpatients without nigrostriatal degeneration (eg drug-inducedparkinsonism essential tremor) and the limited responsive-ness to levodopa and faster progression to disability and deathin patients with atypical parkinsonism syndromes (APS) com-pared to PD (Kempster et al 2007 OrsquoSullivan et al 2008)However postmortem studies suggest that the clinical diagno-sis of PD as the most frequent cause of parkinsonism isincorrect in about 25 of patients ( Tolosa et al 2006) Fre-
quent misdiagnoses include secondary parkinsonism and APSlike multiple system atrophy (MSA) PSP and CBD In turncumulative clinicopathological data suggest that about 30of MSA and PSP and up to 74 of CBD patients are not cor-rectly diagnosed even at late stage (Ling et al 2010)
Against this background SPECT and PET are used with twoaims first to identify patients with progressive nigrostriataldegeneration which is the common pathological feature inPD MSA PSP and CBD Second to differentiate between thelatter patient groups Accurate diagnosis of neurodegenerativeparkinsonism can be achieved by imaging nigrostriatal func-tion (most notably [123I]FP-CIT SPECT) (Benamer et al 2000Benitez-Rivero et al 2013 Marshall et al 2009) (For a moredetailed overview on nigrostriatal imaging in parkinsonismplease refer to Chapter 42) However dopamine transporter
imaging does not allow for a reliable differential diagnosis ofPD MSA PSP and CBD (Meyer and Hellwig 2014) Instead[18F]FDG PET has gained acceptance as the method of choicehere It surpasses the diagnostic accuracies of other commontechniques like imaging cardiac sympathetic innervation (egusing [123I]metaiodobenzylguanidine ([123I]MIBG) scintigra-phy) or imaging of striatal dopamine D2D3 receptors (egusing [123I]iodobenzamide([ 123I]IBZM)) (Meyer and Hellwig 2014) Assessment of regional CBF changes with SPECT mayalso be used for this purpose (eg Eckert et al 2007)However since [18F]FDG PET is technically superior and also widely available we will focus on [18F]FDG PET
[18F]FDG PET shows disease-specific alterations of cerebralglucose metabolism (eg Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Teune et al 2010) scans in PD patients
often show no major abnormality on first glance On closerinspection and especially on voxel-based statistical analysesPD is characterized by a posterior temporoparietal occipitaland sometimes frontal hypometabolism (especially in PD withmild cognitive impairment and PDD) and a relative hyperme-tabolism of putamen globus pallidus sensorimotor cortexpons and cerebellum (Fig 417) Interestingly temporoparieto-occipital hypometabolism may also seen in nondementedPD patients (Hellwig et al 2012 Hu et al 2000) possiblyindicating an increased risk of subsequent development ofPDD (see earlier section on Dementia and Mild Cognitive Impairment ) Conversely MSA patients show a markedhypometabolism of striatum (posterior putamen especially in
Fig 417 [18F]FDG PET in Parkinson disease (PD) PD is typically
characterized by (relative) striatal hypermetabolism Temporoparietal
occipital and sometime frontal hypometabolism can be observed in a
significant fraction of PD patients without apparent cognitive impair-
ment Cortical hypometabolism can be fairly pronounced possiblyrepresenting a risk factor for subsequent development of PDD Top
Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-
based statistical analysis using Neurostat3D-SSP Given are right and
left lateral superior and posterior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 823
Functional Neuroimaging 493
MSA-P) pons and cerebellum (especially in MSA-C) (Fig 418) In the case of PSP regional hypometabolism is consist-ently noted in medial dorso- and ventrolateral frontal areas(pronounced in anterior cingulate gyrus supplementarymotor and premotor areas) caudate nucleus (medial) thala-mus and upper brainstem (Fig 419) Finally CBD is charac-terized by a usually highly asymmetric hypometabolism offrontoparietal areas (pronounced parietal) motor cortex
middle cingulate gyrus striatum and thalamus contralateralto the most affected body side (Fig 4110) The aforemen-tioned results gained from categorical comparisons fit theresults gained from spatial covariance analyses These wereemployed to detect abnormal disease-related metabolic pat-terns in PD MSA and PSP (ie PDRP MSARP and PSPRPrespectively) which were demonstrated to be highly reproduc-ible to correlate with disease severity and duration and toallow for prospective discrimination between cohorts (Eckert et al 2008 Ma et al 2007 Poston et al 2012) The expres-sion of two distinctive spatial covariance patterns characterizesPD one related to motor manifestations (PDRP) and onerelated to cognitive manifestations (PDCP) The PDRP isalready significantly increased in the ipsilateral (ldquopresympto-maticrdquo) hemisphere of patients with hemi-parkinsonism
( Tang et al 2010b) Finally a very recent study (using [
18
F]FDG PET and CBF SPECT) demonstrated that PDRP is alsoincreased in REM sleep behavior disorder (RBD) being a sig-nificant predictor of phenoconversion to PD or DLB (Holt -bernd et al 2014) Thus covariance patterns of cerebralglucose metabolism represent very interesting biomarkers for(early) diagnosis and therapy monitoring in parkinsonism(Hirano et al 2009)
PSP and CBD may be considered to represent differentmanifestations of a disease spectrum with several commonclinical pathological genetic and biochemical features (Kouri et al 2011) This issue gets even more complex if one consid-ers that FTD is often caused by PSP and CBD pathology (see
AD [18F]FDG PET adds little to the diagnosis of VD In agree-ment with CT and MRI PET may show defects of [18F]FDGuptake corresponding to ischemic infarcts in all cerebralregions including primary cortices striatumthalamus andcerebellum Since the latter are usually well preserved in ADdefects in these regions can be an important diagnostic clueDeficits due to vascular lesions can be considerably larger orcause remote deficits of [18F]FDG uptake due to diaschisisFurthermore cerebral glucose metabolism was reported to beglobally reduced (Mielke et al 1992) but without absolutequantification this finding cannot be reliably assessed
Parkinsonism
An early and correct differential diagnosis of parkinsonism isof paramount therapeutic and prognostic importance giventhe possible excellent treatment options and prognosis inpatients without nigrostriatal degeneration (eg drug-inducedparkinsonism essential tremor) and the limited responsive-ness to levodopa and faster progression to disability and deathin patients with atypical parkinsonism syndromes (APS) com-pared to PD (Kempster et al 2007 OrsquoSullivan et al 2008)However postmortem studies suggest that the clinical diagno-sis of PD as the most frequent cause of parkinsonism isincorrect in about 25 of patients ( Tolosa et al 2006) Fre-
quent misdiagnoses include secondary parkinsonism and APSlike multiple system atrophy (MSA) PSP and CBD In turncumulative clinicopathological data suggest that about 30of MSA and PSP and up to 74 of CBD patients are not cor-rectly diagnosed even at late stage (Ling et al 2010)
Against this background SPECT and PET are used with twoaims first to identify patients with progressive nigrostriataldegeneration which is the common pathological feature inPD MSA PSP and CBD Second to differentiate between thelatter patient groups Accurate diagnosis of neurodegenerativeparkinsonism can be achieved by imaging nigrostriatal func-tion (most notably [123I]FP-CIT SPECT) (Benamer et al 2000Benitez-Rivero et al 2013 Marshall et al 2009) (For a moredetailed overview on nigrostriatal imaging in parkinsonismplease refer to Chapter 42) However dopamine transporter
imaging does not allow for a reliable differential diagnosis ofPD MSA PSP and CBD (Meyer and Hellwig 2014) Instead[18F]FDG PET has gained acceptance as the method of choicehere It surpasses the diagnostic accuracies of other commontechniques like imaging cardiac sympathetic innervation (egusing [123I]metaiodobenzylguanidine ([123I]MIBG) scintigra-phy) or imaging of striatal dopamine D2D3 receptors (egusing [123I]iodobenzamide([ 123I]IBZM)) (Meyer and Hellwig 2014) Assessment of regional CBF changes with SPECT mayalso be used for this purpose (eg Eckert et al 2007)However since [18F]FDG PET is technically superior and also widely available we will focus on [18F]FDG PET
[18F]FDG PET shows disease-specific alterations of cerebralglucose metabolism (eg Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Teune et al 2010) scans in PD patients
often show no major abnormality on first glance On closerinspection and especially on voxel-based statistical analysesPD is characterized by a posterior temporoparietal occipitaland sometimes frontal hypometabolism (especially in PD withmild cognitive impairment and PDD) and a relative hyperme-tabolism of putamen globus pallidus sensorimotor cortexpons and cerebellum (Fig 417) Interestingly temporoparieto-occipital hypometabolism may also seen in nondementedPD patients (Hellwig et al 2012 Hu et al 2000) possiblyindicating an increased risk of subsequent development ofPDD (see earlier section on Dementia and Mild Cognitive Impairment ) Conversely MSA patients show a markedhypometabolism of striatum (posterior putamen especially in
Fig 417 [18F]FDG PET in Parkinson disease (PD) PD is typically
characterized by (relative) striatal hypermetabolism Temporoparietal
occipital and sometime frontal hypometabolism can be observed in a
significant fraction of PD patients without apparent cognitive impair-
ment Cortical hypometabolism can be fairly pronounced possiblyrepresenting a risk factor for subsequent development of PDD Top
Transaxial PET images of [18F]FDG uptake Bottom Results of voxel-
based statistical analysis using Neurostat3D-SSP Given are right and
left lateral superior and posterior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
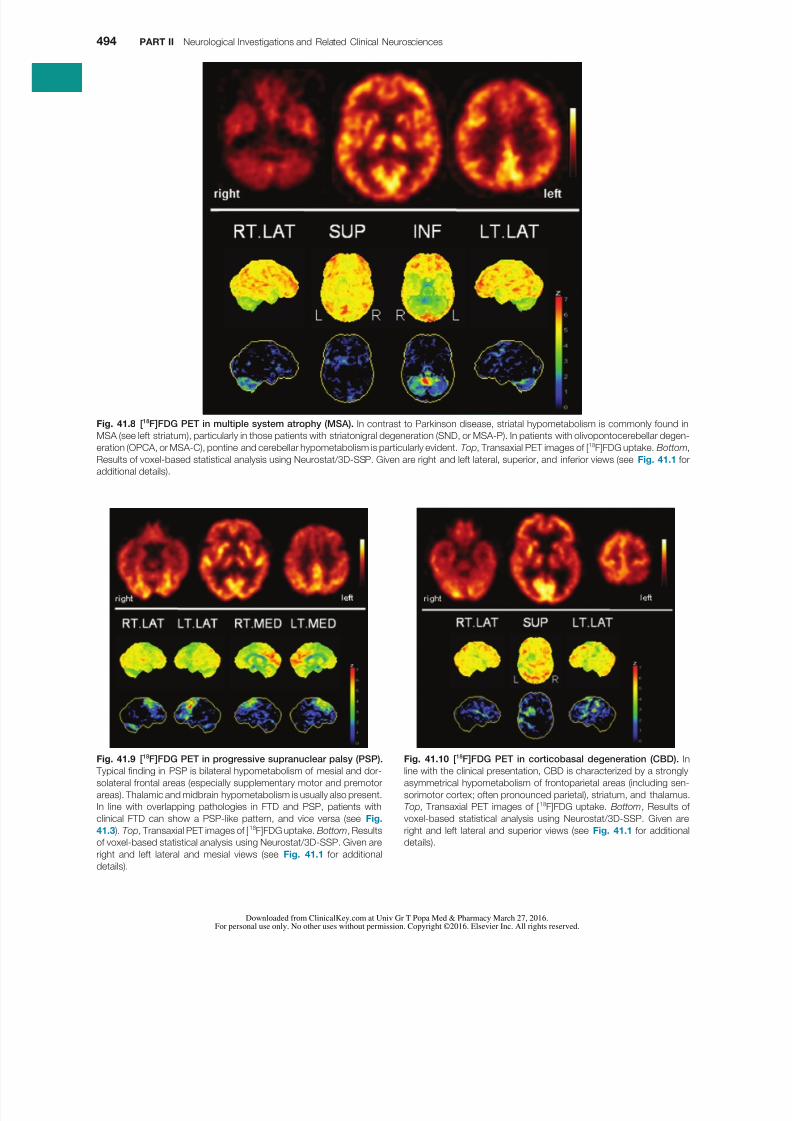
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 923
494 PART II Neurological Investigations and Related Clinical Neurosciences
Fig 418 [18F]FDG PET in multiple system atrophy (MSA) In contrast to Parkinson disease striatal hypometabolism is commonly found in
MSA (see left striatum) particularly in those patients with striatonigral degeneration (SND or MSA-P) In patients with olivopontocerebellar degen-
eration (OPCA or MSA-C) pontine and cerebellar hypometabolism is particularly evident Top Transaxial PET images of [18F]FDG uptake Bottom
Results of voxel-based statistical analysis using Neurostat3D-SSP Given are right and left lateral superior and inferior views (see Fig 411 for
additional details)
Fig 419 [18F]FDG PET in progressive supranuclear palsy (PSP)
Typical finding in PSP is bilateral hypometabolism of mesial and dor-
solateral frontal areas (especially supplementary motor and premotor
areas) Thalamic and midbrain hypometabolism is usually also present
In line with overlapping pathologies in FTD and PSP patients with
clinical FTD can show a PSP-like pattern and vice versa (see Fig
413 ) Top Transaxial PET images of [18F]FDG uptake Bottom Results
of voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and mesial views (see Fig 411 for additional
details)
Fig 4110 [18F]FDG PET in corticobasal degeneration (CBD) In
line with the clinical presentation CBD is characterized by a strongly
asymmetrical hypometabolism of frontoparietal areas (including sen-
sorimotor cortex often pronounced parietal) striatum and thalamus
Top Transaxial PET images of [18F]FDG uptake Bottom Results of
voxel-based statistical analysis using Neurostat3D-SSP Given are
right and left lateral and superior views (see Fig 411 for additional
details)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
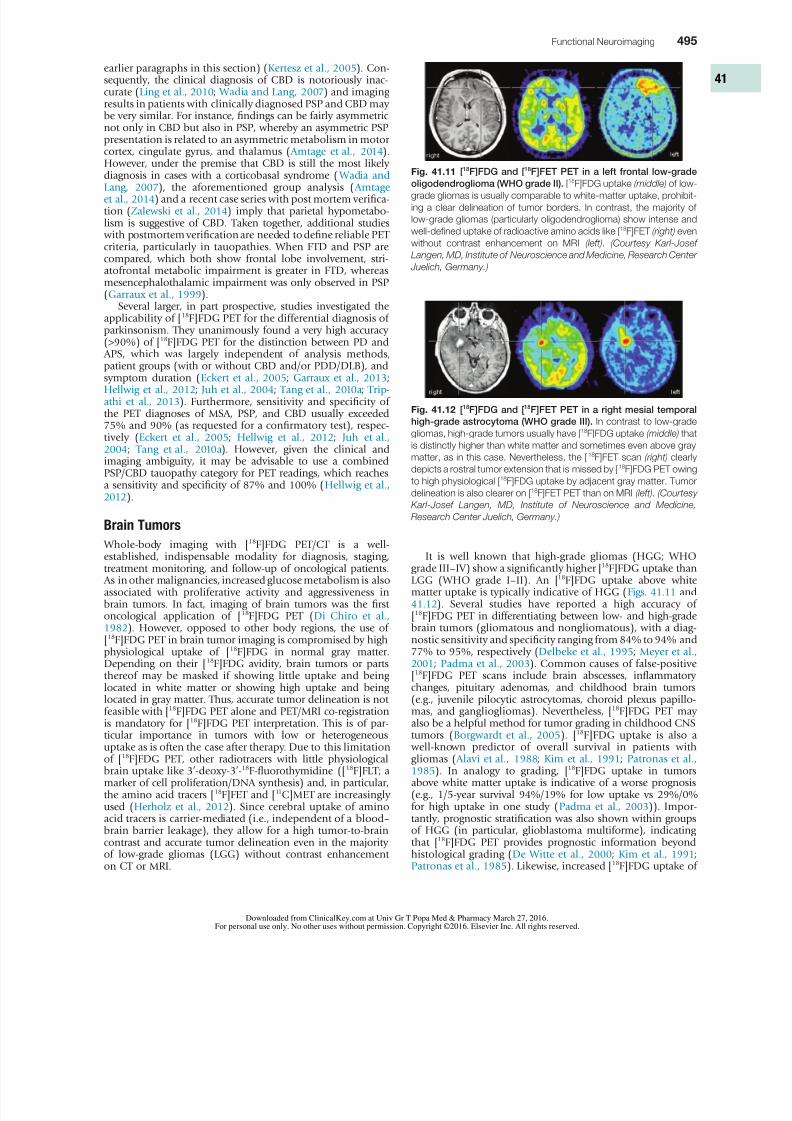
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1023
Functional Neuroimaging 495
It is well known that high-grade gliomas (HGG WHOgrade IIIndashIV) show a significantly higher [18F]FDG uptake thanLGG (WHO grade IndashII) An [18F]FDG uptake above whitematter uptake is typically indicative of HGG (Figs 4111 and4112) Several studies have reported a high accuracy of[18F]FDG PET in differentiating between low- and high-gradebrain tumors (gliomatous and nongliomatous) with a diag-nostic sensitivity and specificity ranging from 84 to 94 and77 to 95 respectively (Delbeke et al 1995 Meyer et al 2001 Padma et al 2003) Common causes of false-positive[18F]FDG PET scans include brain abscesses inflammatorychanges pituitary adenomas and childhood brain tumors(eg juvenile pilocytic astrocytomas choroid plexus papillo-mas and gangliogliomas) Nevertheless [18F]FDG PET may
also be a helpful method for tumor grading in childhood CNStumors (Borgwardt et al 2005) [18F]FDG uptake is also a well-known predictor of overall survival in patients withgliomas ( Alavi et al 1988 Kim et al 1991 Patronas et al 1985) In analogy to grading [18F]FDG uptake in tumorsabove white matter uptake is indicative of a worse prognosis(eg 15-year survival 9419 for low uptake vs 290for high uptake in one study (Padma et al 2003)) Impor-tantly prognostic stratification was also shown within groupsof HGG (in particular glioblastoma multiforme) indicatingthat [18F]FDG PET provides prognostic information beyondhistological grading (De Witte et al 2000 Kim et al 1991Patronas et al 1985) Likewise increased [18F]FDG uptake of
earlier paragraphs in this section) (Kertesz et al 2005) Con-sequently the clinical diagnosis of CBD is notoriously inac-curate (Ling et al 2010 Wadia and Lang 2007) and imagingresults in patients with clinically diagnosed PSP and CBD maybe very similar For instance findings can be fairly asymmetricnot only in CBD but also in PSP whereby an asymmetric PSPpresentation is related to an asymmetric metabolism in motorcortex cingulate gyrus and thalamus ( Amtage et al 2014)However under the premise that CBD is still the most likelydiagnosis in cases with a corticobasal syndrome ( Wadia and Lang 2007) the aforementioned group analysis ( Amtage et al 2014) and a recent case series with post mortem verifica-tion (Zalewski et al 2014) imply that parietal hypometabo-lism is suggestive of CBD Taken together additional studies with postmortem verification are needed to define reliable PETcriteria particularly in tauopathies When FTD and PSP arecompared which both show frontal lobe involvement stri-atofrontal metabolic impairment is greater in FTD whereasmesencephalothalamic impairment was only observed in PSP(Garraux et al 1999)
Several larger in part prospective studies investigated theapplicability of [18F]FDG PET for the differential diagnosis ofparkinsonism They unanimously found a very high accuracy(gt90) of [18F]FDG PET for the distinction between PD and APS which was largely independent of analysis methods
patient groups (with or without CBD andor PDDDLB) andsymptom duration (Eckert et al 2005 Garraux et al 2013Hellwig et al 2012 Juh et al 2004 Tang et al 2010a Trip-athi et al 2013) Furthermore sensitivity and specificity ofthe PET diagnoses of MSA PSP and CBD usually exceeded75 and 90 (as requested for a confirmatory test) respec-tively (Eckert et al 2005 Hellwig et al 2012 Juh et al 2004 Tang et al 2010a) However given the clinical andimaging ambiguity it may be advisable to use a combinedPSPCBD tauopathy category for PET readings which reachesa sensitivity and specificity of 87 and 100 (Hellwig et al 2012)
Brain Tumors
Whole-body imaging with [18
F]FDG PETCT is a well-established indispensable modality for diagnosis stagingtreatment monitoring and follow-up of oncological patients As in other malignancies increased glucose metabolism is alsoassociated with proliferative activity and aggressiveness inbrain tumors In fact imaging of brain tumors was the firstoncological application of [18F]FDG PET (Di Chiro et al 1982) However opposed to other body regions the use of[18F]FDG PET in brain tumor imaging is compromised by highphysiological uptake of [18F]FDG in normal gray matterDepending on their [18F]FDG avidity brain tumors or partsthereof may be masked if showing little uptake and beinglocated in white matter or showing high uptake and beinglocated in gray matter Thus accurate tumor delineation is notfeasible with [18F]FDG PET alone and PETMRI co-registration
is mandatory for [
18
F]FDG PET interpretation This is of par-ticular importance in tumors with low or heterogeneousuptake as is often the case after therapy Due to this limitationof [18F]FDG PET other radiotracers with little physiologicalbrain uptake like 3rsquo-deoxy-3rsquo-18F-fluorothymidine ([18F]FLT amarker of cell proliferationDNA synthesis) and in particularthe amino acid tracers [18F]FET and [11C]MET are increasinglyused (Herholz et al 2012) Since cerebral uptake of aminoacid tracers is carrier-mediated (ie independent of a bloodndashbrain barrier leakage) they allow for a high tumor-to-braincontrast and accurate tumor delineation even in the majorityof low-grade gliomas (LGG) without contrast enhancementon CT or MRI
Fig 4111 [18F]FDG and [18F]FET PET in a left frontal low-grade
oligodendroglioma (WHO grade II) [18F]FDG uptake (middle) of low-grade gliomas is usually comparable to white-matter uptake prohibit-
ing a clear delineation of tumor borders In contrast the majority of
low-grade gliomas (particularly oligodendroglioma) show intense and
well-defined uptake of radioactive amino acids like [18F]FET (right) even
without contrast enhancement on MRI (left) (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Fig 4112 [18F]FDG and [18F]FET PET in a right mesial temporal
high-grade astrocytoma (WHO grade III) In contrast to low-grade
gliomas high-grade tumors usually have [18F]FDG uptake (middle) that
is distinctly higher than white matter and sometimes even above gray
matter as in this case Nevertheless the [18F]FET scan (right) clearly
depicts a rostral tumor extension that is missed by [18F]FDG PET owing
to high physiological [18F]FDG uptake by adjacent gray matter Tumor
delineation is also clearer on [18F]FET PET than on MRI (left) (Courtesy
Karl-Josef Langen MD Institute of Neuroscience and Medicine
Research Center Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1123
496 PART II Neurological Investigations and Related Clinical Neurosciences
changes (Grosu et al 2005) Concerning grading moststudies showed a higher amino acid uptake of HGG than ofLGG However a considerable overlap between groups pro-hibits a reliable distinction This situation is further compli-cated by the observation that tumors with an oligodendroglialcomponent show a higher amino acid uptake than corre-
sponding astrocytomas (Glaudemans et al 2013 Herholz et al 2012) Consequently the prognostic value of aminoacid uptake is inferior to [18F]FDG PET in mixed populations(Pauleit et al 2009) However the time course of [18F]FET(but not [11C]MET) uptake was found to be highly predictiveof tumor grade (accuracy ~90) (Calcagni et al 2011 Poumlpperl et al 2006) HGG usually show an early peak with subse-quent decrease of [18F]FET uptake whereas LGG commonlyshow a delayed and steadily increasing [18F]FET uptake Thesekinetic patterns were also found to predict malignant transfor-mation and prognosis in patients with LGG (Galldiks et al 2013 Jansen et al 2014) Within groups of LGG lower [11C]MET and [18F]FET uptake is also associated with a better prog-nosis (Floeth et al 2007 Smits et al 2008)
Differentiation between benign treatment-associated
changes (radiation necrosis and pseudoprogression in par-ticular) and residual or recurrent tumor is of paramountimportance Since specificity of CT and MRI is compromisedby contrast enhancement due to non-neoplastic post-therapeutic changes PET imaging is frequently used Howeverthe merit of [18F]FDG PET is controversial since earlier studiesprovided highly variable results with sensitivity and specificityranging from 40 to 100 (Herholz et al 2012 Langleben and Segall 2000) False-negative results are relatively frequentand may result from very recent radiation therapy pretreat-ment low FDG uptake (eg in LGG or metastases with lowFDG avidity) masking by physiological uptake and smalltumor volumes Conversely intense inflammatory reactionafter (especially stereotactic) radiation therapy and seizureactivity may result in false-positive findings Accurate PETMRI
co-registration is crucial to carefully evaluate if tumor uptakeexceeds the expected background uptake in adjacent braintissue (Fig 4114) Under these conditions the sensitivity andspecificity of [18F]FDG PET to differentiate between tumorrecurrence (gliomas and metastases) and radiation necrosis isabout 75ndash80 and 85ndash90 respectively (Chao et al 2001Goacutemez-Riacuteo et al 2008 Wang et al 2006) As in primarytumors shortcomings of [18F]FDG PET may be overcome byamino acid PET (see Fig 4114) Reported sensitivity and spe-cificity of [11C]MET PET range 75ndash100 and 60ndash100 respec-tively (Glaudemans et al 2013) The specificity of [18F]FETPET is probably somewhat higher since [18F]FET shows lessuptake in inflammatory changes (Herholz et al 2012) A
LGG during follow-up (as an indicator of de-differentiation)is associated with worse prognosis opposed to persistent lowuptake (De Witte et al 1996 Schifter et al 1993) PrimaryCNS lymphoma (PCNSL) usually show an extraordinary high[18F]FDG uptake making [18F]FDG PET a powerful method fordetecting cerebral lymphoma (Fig 4113) and for distinguish-
ing them from nonmalignant CNS lesions (eg in acquiredimmunodeficiency syndrome patients) Moreover [18F]FDGuptake was found to be an independent predictor of progres-sion free survival in PCNSL (Kasenda et al 2013) Given theassociation between metabolic activity and tumor grade as well as prognosis incorporating [18F]FDG PET into biopsyplanning increases the diagnostic yield particularly in HGG with heterogenic tissue composition (Goldman et al 1997Pirotte et al 1994) Furthermore [18F]FDG PET can targetsurgical resection to hypermetabolicanaplastic areas in HGGto improve patient outcome (Pirotte et al 2006 2009) Withthe same rationale [18F]FDG PET was also used for radiationtreatment planning in HGG (eg tumor volume definitiontargeting dose escalation) albeit initial results were disap-pointing (Douglas et al 2006 Gross et al 1998) Of note
aforementioned approaches are primarily only applicable totumors showing an increased [18F]FDG uptake (ie usuallyonly HGG)
This limitation can be overcome by PET studies usingamino acid tracers like [18F]FET or [11C]MET which are avidlytaken by most LGG (~80) and virtually all HGG (gt90)tumors while physiological brain uptake is low (see Figs 4111 and 4112) In line with this a recent meta-analysisdescribed a high accuracy of [18F]FET PET for differentiationbetween neoplastic and non-neoplastic brain lesions (sensitiv-ity 82 specificity 76) (Dunet et al 2012) This also com-pares favorably with MRI or MRI plus magnetic resonancespectroscopy (MRS) (Moumlller-Hartmann et al 2002) Specifi-city may be compromised by non-neoplastic amino aciduptake in inflammatory cells gliosis surrounding hemato-
mas and ischemic areas (Herholz et al 2012) It has beenshown that amino acid PET significantly improves tumordelineation for biopsy planning or surgical resection com-pared to MRI or [18F]FDG PET with amino acid PET typicallyshowing larger tumor volumes (Pauleit et al 2005 Pirotte et al 2004 2006) (see Fig 4112) Furthermore completeresection of tissue with increased PET tracer uptake ([11C]METor [18F]FDG) was associated with better survival in HGG whileresection of contrast enhancement on MRI was not (Pirotte et al 2009) Likewise amino acid PET has been shown toimprove gross tumor volume definition for radiation treat-ment planning in gliomas This is particularly true after surgery when specificity of MRI is compromised by postoperative
Fig 4113 [
18
F]FDG and [
18
F]FET PET in a primary CNS lymphoma(PCNSL) PCNSL usually show a very intense [18F]FDG uptake (middle)
while metabolism of surrounding brain tissue is suppressed by exten-
sive tumor edema (see MRI left ) [18F]FET uptake (right) of cerebral
lymphoma can also be high (Courtesy Karl-Josef Langen MD Insti-
tute of Neuroscience and Medicine Research Center Juelich
Germany)
Fig 4114 [18F]FDG and [18F]FET PET in a recurrent high-grade
astrocytoma (WHO grade III) [18F]FDG uptake (middle) is clearly
increased above expected background in several areas of suspected
tumor recurrence on MRI (left) confirming viable tumor tissue In
comparison to [18F]FDG PET [18F]FET PET (right) more clearly und
extensively depicts the area of active tumor (Courtesy Karl-Josef
Langen MD Institute of Neuroscience and Medicine Research Center
Juelich Germany)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
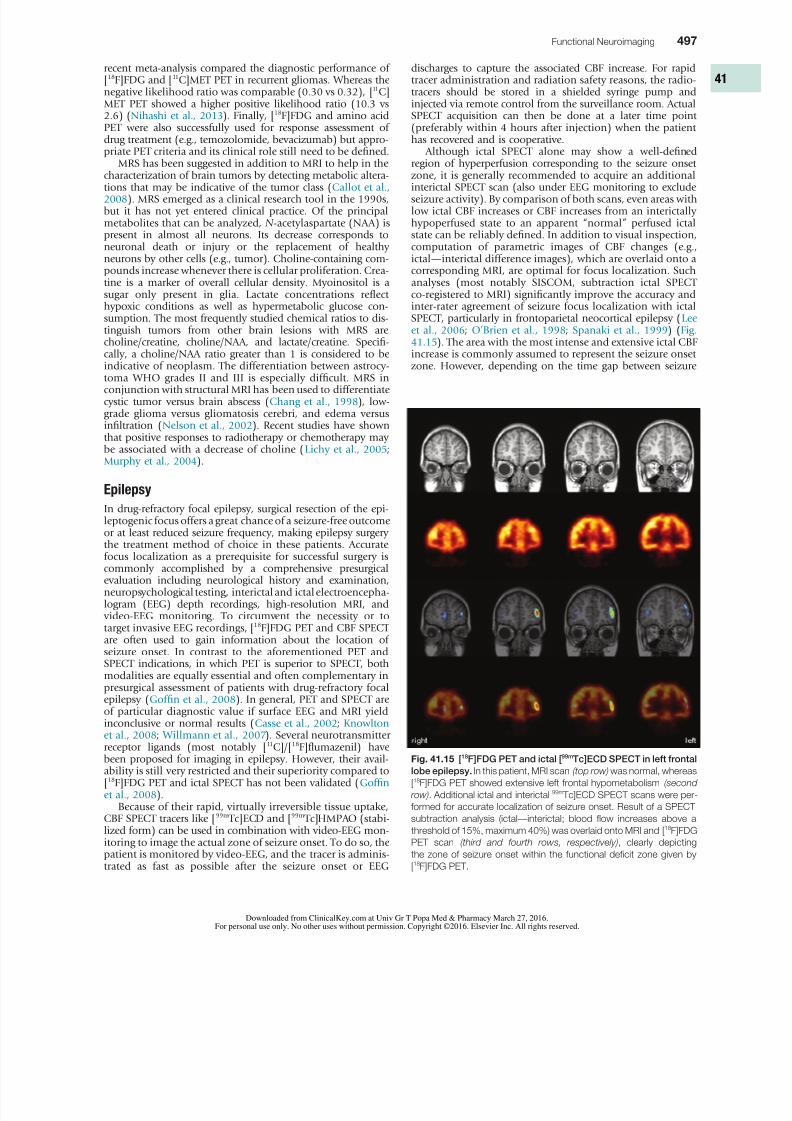
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1223
Functional Neuroimaging 497
discharges to capture the associated CBF increase For rapidtracer administration and radiation safety reasons the radio-tracers should be stored in a shielded syringe pump andinjected via remote control from the surveillance room ActualSPECT acquisition can then be done at a later time point(preferably within 4 hours after injection) when the patienthas recovered and is cooperative
Although ictal SPECT alone may show a well-definedregion of hyperperfusion corresponding to the seizure onsetzone it is generally recommended to acquire an additionalinterictal SPECT scan (also under EEG monitoring to excludeseizure activity) By comparison of both scans even areas withlow ictal CBF increases or CBF increases from an interictallyhypoperfused state to an apparent ldquonormalrdquo perfused ictalstate can be reliably defined In addition to visual inspectioncomputation of parametric images of CBF changes (egictalmdashinterictal difference images) which are overlaid onto acorresponding MRI are optimal for focus localization Suchanalyses (most notably SISCOM subtraction ictal SPECTco-registered to MRI) significantly improve the accuracy andinter-rater agreement of seizure focus localization with ictalSPECT particularly in frontoparietal neocortical epilepsy (Lee et al 2006 OrsquoBrien et al 1998 Spanaki et al 1999) (Fig 4115) The area with the most intense and extensive ictal CBFincrease is commonly assumed to represent the seizure onset
zone However depending on the time gap between seizure
recent meta-analysis compared the diagnostic performance of[18F]FDG and [11C]MET PET in recurrent gliomas Whereas thenegative likelihood ratio was comparable (030 vs 032) [11C]MET PET showed a higher positive likelihood ratio (103 vs26) (Nihashi et al 2013) Finally [18F]FDG and amino acidPET were also successfully used for response assessment ofdrug treatment (eg temozolomide bevacizumab) but appro-priate PET criteria and its clinical role still need to be defined
MRS has been suggested in addition to MRI to help in thecharacterization of brain tumors by detecting metabolic altera-tions that may be indicative of the tumor class (Callot et al 2008) MRS emerged as a clinical research tool in the 1990sbut it has not yet entered clinical practice Of the principalmetabolites that can be analyzed N -acetylaspartate (NAA) ispresent in almost all neurons Its decrease corresponds toneuronal death or injury or the replacement of healthyneurons by other cells (eg tumor) Choline-containing com-pounds increase whenever there is cellular proliferation Crea-tine is a marker of overall cellular density Myoinositol is asugar only present in glia Lactate concentrations reflecthypoxic conditions as well as hypermetabolic glucose con-sumption The most frequently studied chemical ratios to dis-tinguish tumors from other brain lesions with MRS arecholinecreatine cholineNAA and lactatecreatine Specifi-cally a cholineNAA ratio greater than 1 is considered to be
indicative of neoplasm The differentiation between astrocy-toma WHO grades II and III is especially difficult MRS inconjunction with structural MRI has been used to differentiatecystic tumor versus brain abscess (Chang et al 1998) low-grade glioma versus gliomatosis cerebri and edema versusinfiltration (Nelson et al 2002) Recent studies have shownthat positive responses to radiotherapy or chemotherapy maybe associated with a decrease of choline (Lichy et al 2005Murphy et al 2004)
Epilepsy
In drug-refractory focal epilepsy surgical resection of the epi-leptogenic focus offers a great chance of a seizure-free outcomeor at least reduced seizure frequency making epilepsy surgery
the treatment method of choice in these patients Accuratefocus localization as a prerequisite for successful surgery iscommonly accomplished by a comprehensive presurgicalevaluation including neurological history and examinationneuropsychological testing interictal and ictal electroencepha-logram (EEG) depth recordings high-resolution MRI and video-EEG monitoring To circumvent the necessity or totarget invasive EEG recordings [18F]FDG PET and CBF SPECTare often used to gain information about the location ofseizure onset In contrast to the aforementioned PET andSPECT indications in which PET is superior to SPECT bothmodalities are equally essential and often complementary inpresurgical assessment of patients with drug-refractory focalepilepsy (Goffin et al 2008) In general PET and SPECT areof particular diagnostic value if surface EEG and MRI yield
inconclusive or normal results (Casse et al 2002 Knowlton et al 2008 Willmann et al 2007) Several neurotransmitterreceptor ligands (most notably [11C][18F]flumazenil) havebeen proposed for imaging in epilepsy However their avail-ability is still very restricted and their superiority compared to[18F]FDG PET and ictal SPECT has not been validated (Goffin et al 2008)
Because of their rapid virtually irreversible tissue uptakeCBF SPECT tracers like [99m Tc]ECD and [99m Tc]HMPAO (stabi-lized form) can be used in combination with video-EEG mon-itoring to image the actual zone of seizure onset To do so thepatient is monitored by video-EEG and the tracer is adminis-trated as fast as possible after the seizure onset or EEG
Fig 4115 [18F]FDG PET and ictal [99mTc]ECD SPECT in left frontal
lobe epilepsy In this patient MRI scan (top row) was normal whereas
[18F]FDG PET showed extensive left frontal hypometabolism (second
row) Additional ictal and interictal 99m Tc]ECD SPECT scans were per-
formed for accurate localization of seizure onset Result of a SPECT
subtraction analysis (ictalmdashinterictal blood flow increases above a
threshold of 15 maximum 40) was overlaid onto MRI and [18F]FDG
PET scan (third and fourth rows respectively) clearly depicting
the zone of seizure onset within the functional deficit zone given by
[18F]FDG PET
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1323
498 PART II Neurological Investigations and Related Clinical Neurosciences
onset and cerebral tracer fixation ictal SPECT not only depictsthe onset zone but also the propagation zone Therefore accu-rate knowledge about the timing of tracer injection is crucialfor ictal SPECT interpretation CBF increases may propagate to various cortical areas during seizure progression including thecontralateral temporal lobe insula basal ganglia and frontallobe in patients with temporal lobe epilepsy (TLE) reflectingseizure semiology (Shin et al 2002) In patients with focaldysplastic lesions distinct ictal perfusion patterns have beenobserved with seizure propagation during which the area ofmost intense CBF increase may migrate away from the seizureonset zone (Dupont et al 2006) This underlines the need forrapid tracer injection after seizure onset to localize the actualonset zone An injection delay of 20 to 45 seconds enablesoptimal localization results (Lee et al 2006 OrsquoBrien et al 1998) At later time points a so-called postictal switch occursleading to a hypoperfusion of the onset zone Within 100seconds from seizure onset about two-thirds of ictal SPECTstudies can be expected to show hyperperfusion after that(gt100 seconds postictally) hypoperfusion will be observed( Avery et al 1999)
The diagnostic sensitivity of ictal SPECT to correctly local-ize the seizure focus (usually with reference to surgicaloutcome) is about 85 to 95 in TLE and 70 to 90 inextratemporal lobe epilepsy (ETLE) (Devous et al 1998
Newton et al 1995 Weil et al 2001 Zaknun et al 2008)Focus localization can also be successful by postictal tracerinjection capturing postictal hypoperfusion However locali-zation accuracy will be lower (about 70ndash75 in TLE and50 in ETLE) (Devous et al 1998 Newton et al 1995) Incontrast interictal SPECT to detect interictal hypoperfusion isinsufficient for focus localization (sensitivity about 50 in TLE of no diagnostic value in ETLE) (Newton et al 1995Spanaki et al 1999 Zaknun et al 2008)
In contrast to ictal SPECT [18F]FDG PET studies are per-formed in the interictal state to image the functional deficitzone which shows abnormal metabolism between seizuresand is generally assumed to contain also the seizure onsetzone The etiology of this hypometabolism is not fully under-stood and probably relates to functional (eg surround inhi-
bition of areas of seizure onset and propagation as a defensemechanism) and structural changes (eg neuronal or synapticloss due to repeated seizures) Hypometabolism appearsto increase with duration frequency and severity of seizuresand usually extends considerably beyond the actual seizureonset zone occasionally involving contralateral mirror regions(Kumar and Chugani 2013) A direct comparison of ictalperfusion abnormalities detected by SISCOM and interictal[18F]FDG PET hypometabolism in TLE patients demonstratedhigh concordance suggesting that seizures are generated andspread in metabolically abnormal regions (Bouilleret et al 2002) To ensure an interictal state the patient should ideallybe seizure free for at least 24 hours before PET and be moni-tored by EEG after [18F]FDG injection to rule out possiblesubclinical epileptic activity Side-to-side asymmetry may be
calculated by region-of-interest analysis to support visualinterpretation whereby an asymmetry ge10 is commonlyused as threshold for regional pathology Furthermore voxel- wise statistical analyses are strongly recommended Visualanalyses by an experienced observer is at least as accurate in TLE patients (Fig 4116) but accuracy and interobserver agree-ment of focus localization is considerably improved by addi-tional voxel-wise statistical analyses in ETLE (Drzezga et al 1999) (Fig 4117) Finally PETMRI co-registration is veryhelpful for detecting PET abnormalities in regions with appar-ently normal anatomy (eg caused by subtle focal corticaldysplasia FCD) and to disclose the extent of PET findings inrelation to structural abnormalities (eg in epileptogenic
Fig 4116 [18F]FDG PET in left temporal lobe epilepsy Diagnostic
benefit of [18F]FDG PET is greatest in patients with normal MRI (lefttop row) in which [18F]FDG PET still detects well-lateralized temporal
lobe hypometabolism ( second row left temporal lobe hypometabo-
lism) As in this patient with left mesial temporal lobe epilepsy the area
of hypometabolism often extends to the lateral cortex (functional deficit
zone third row PETMRI fusion) Right Results of voxel-based statisti-
cal analysis of [18F]FDG PET scan using Neurostat3D-SSP Given are
left lateral views (top image [18F]FDG uptake bottom image statistical
deviation of uptake from healthy controls color-coded as z score see
Fig 411 for additional details)
tumors or tuberous sclerosis) (Lee and Salamon 2009)However if structural abnormalities and the accompanying
hypometabolism are extensive (eg infarction contusionsurgery) ictal SPECT may be preferred to image the area ofseizure onset [18F]FDG PET may nevertheless be helpful toevaluate the functional integrity of the remaining brainregions
In meta-analyses the sensitivity of [18F]FDG PET for focuslateralization (rather than localization given the extent ofhypometabolism) in TLE was reported to be around 86 whereas false lateralization to the contralateral side of theepileptogenic focus rarely occurs (lt5) (Casse et al 2002 Willmann et al 2007) Consequently presurgical unilateraltemporal hypometabolism predicts a good surgical outcome(Engel Class IndashII) in 82 to 86 of total TLE cases and even80 and 72 in TLE patients with normal MRI and nonlocal-ized ictal scalp EEG respectively (Casse et al 2002 Willmann
et al 2007) In contrast asymmetrical thalamic metabolism(particularly in reverse direction to temporal lobe asymmetry)and extratemporal cortical hypometabolism (in particular ofthe contralateral hemisphere) are associated with poor post-operative seizure control (Choi et al 2003 Newberg et al 2000) In ETLE the sensitivity of [18F]FDG PET is lower pro- viding a seizure focus localization in about 67 of ETLEpatients (Casse et al 2002 Drzezga et al 1999) Againcorrect localization by [18F]FDG PET was demonstrated to bea significant predictor of a good surgical outcome in patients with neocortical epilepsy ( Yun et al 2006)
Few large-scale studies directly compared ictal SPECTand interictal [18F]FDG PET Comparing rates of correct
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
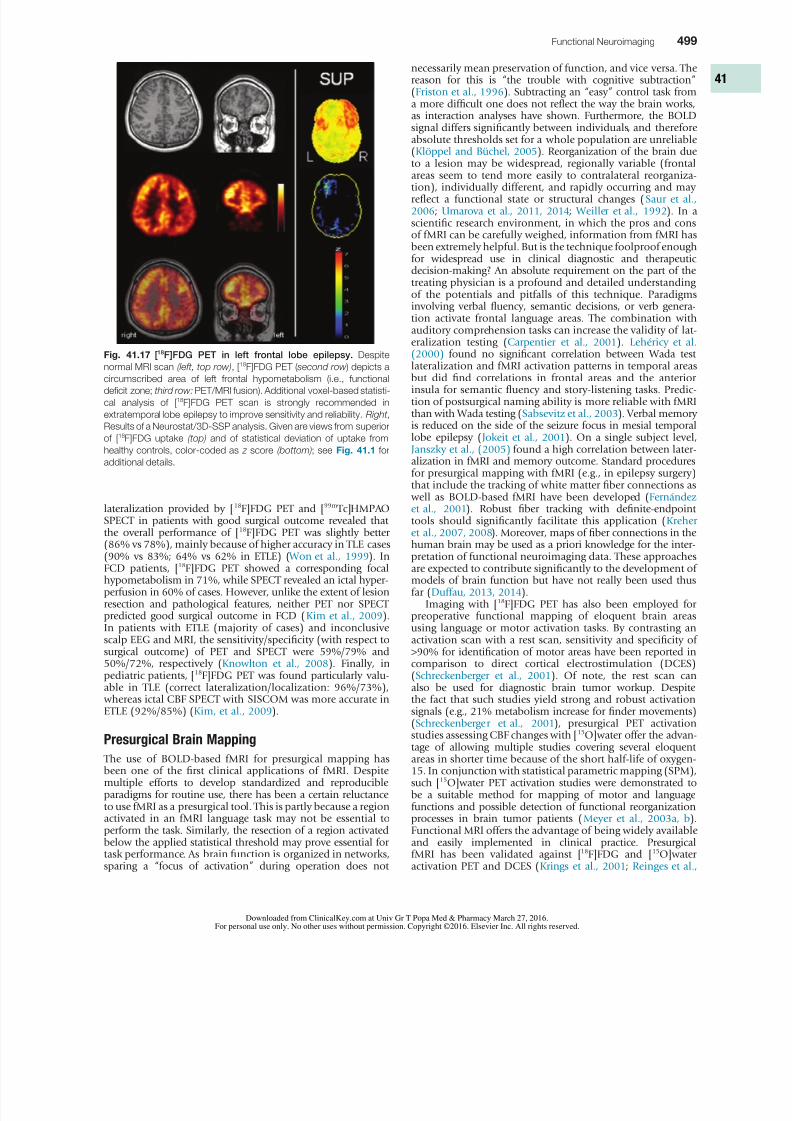
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1423
Functional Neuroimaging 499
necessarily mean preservation of function and vice versa Thereason for this is ldquothe trouble with cognitive subtractionrdquo(Friston et al 1996) Subtracting an ldquoeasyrdquo control task froma more difficult one does not reflect the way the brain worksas interaction analyses have shown Furthermore the BOLDsignal differs significantly between individuals and thereforeabsolute thresholds set for a whole population are unreliable(Kloumlppel and Buumlchel 2005) Reorganization of the brain dueto a lesion may be widespread regionally variable (frontalareas seem to tend more easily to contralateral reorganiza-tion) individually different and rapidly occurring and mayreflect a functional state or structural changes (Saur et al 2006 Umarova et al 2011 2014 Weiller et al 1992) In ascientific research environment in which the pros and consof fMRI can be carefully weighed information from fMRI hasbeen extremely helpful But is the technique foolproof enoughfor widespread use in clinical diagnostic and therapeuticdecision-making An absolute requirement on the part of thetreating physician is a profound and detailed understandingof the potentials and pitfalls of this technique Paradigmsinvolving verbal fluency semantic decisions or verb genera-tion activate frontal language areas The combination withauditory comprehension tasks can increase the validity of lat-eralization testing (Carpentier et al 2001) Leheacutericy et al (2000) found no significant correlation between Wada test
lateralization and fMRI activation patterns in temporal areasbut did find correlations in frontal areas and the anteriorinsula for semantic fluency and story-listening tasks Predic-tion of postsurgical naming ability is more reliable with fMRIthan with Wada testing (Sabsevitz et al 2003) Verbal memoryis reduced on the side of the seizure focus in mesial temporallobe epilepsy (Jokeit et al 2001) On a single subject levelJanszky et al (2005) found a high correlation between later-alization in fMRI and memory outcome Standard proceduresfor presurgical mapping with fMRI (eg in epilepsy surgery)that include the tracking of white matter fiber connections as well as BOLD-based fMRI have been developed (Fernaacutendez et al 2001) Robust fiber tracking with definite-endpointtools should significantly facilitate this application (Kreher et al 2007 2008) Moreover maps of fiber connections in the
human brain may be used as a priori knowledge for the inter-pretation of functional neuroimaging data These approachesare expected to contribute significantly to the development ofmodels of brain function but have not really been used thusfar (Duffau 2013 2014)
Imaging with [18F]FDG PET has also been employed forpreoperative functional mapping of eloquent brain areasusing language or motor activation tasks By contrasting anactivation scan with a rest scan sensitivity and specificity ofgt90 for identification of motor areas have been reported incomparison to direct cortical electrostimulation (DCES)(Schreckenberger et al 2001) Of note the rest scan canalso be used for diagnostic brain tumor workup Despitethe fact that such studies yield strong and robust activationsignals (eg 21 metabolism increase for finder movements)
(Schreckenberger et al 2001) presurgical PET activationstudies assessing CBF changes with [15O]water offer the advan-tage of allowing multiple studies covering several eloquentareas in shorter time because of the short half-life of oxygen-15 In conjunction with statistical parametric mapping (SPM)such [15O]water PET activation studies were demonstrated tobe a suitable method for mapping of motor and languagefunctions and possible detection of functional reorganizationprocesses in brain tumor patients (Meyer et al 2003a b)Functional MRI offers the advantage of being widely availableand easily implemented in clinical practice PresurgicalfMRI has been validated against [18F]FDG and [15O]wateractivation PET and DCES (Krings et al 2001 Reinges et al
lateralization provided by [18F]FDG PET and [99m Tc]HMPAOSPECT in patients with good surgical outcome revealed thatthe overall performance of [18F]FDG PET was slightly better
(86 vs 78) mainly because of higher accuracy in TLE cases(90 vs 83 64 vs 62 in ETLE) ( Won et al 1999) InFCD patients [18F]FDG PET showed a corresponding focalhypometabolism in 71 while SPECT revealed an ictal hyper-perfusion in 60 of cases However unlike the extent of lesionresection and pathological features neither PET nor SPECTpredicted good surgical outcome in FCD (Kim et al 2009)In patients with ETLE (majority of cases) and inconclusivescalp EEG and MRI the sensitivityspecificity (with respect tosurgical outcome) of PET and SPECT were 5979 and5072 respectively (Knowlton et al 2008) Finally inpediatric patients [18F]FDG PET was found particularly valu-able in TLE (correct lateralizationlocalization 9673) whereas ictal CBF SPECT with SISCOM was more accurate inETLE (9285) (Kim et al 2009)
Presurgical Brain Mapping
The use of BOLD-based fMRI for presurgical mapping hasbeen one of the first clinical applications of fMRI Despitemultiple efforts to develop standardized and reproducibleparadigms for routine use there has been a certain reluctanceto use fMRI as a presurgical tool This is partly because a regionactivated in an fMRI language task may not be essential toperform the task Similarly the resection of a region activatedbelow the applied statistical threshold may prove essential fortask performance As brain function is organized in networkssparing a ldquofocus of activationrdquo during operation does not
Fig 4117 [18F]FDG PET in left frontal lobe epilepsy Despite
normal MRI scan (left top row) [18F]FDG PET ( second row ) depicts acircumscribed area of left frontal hypometabolism (ie functional
deficit zone third row PETMRI fusion) Additional voxel-based statisti-
cal analysis of [18F]FDG PET scan is strongly recommended in
extratemporal lobe epilepsy to improve sensitivity and reliability Right
Results of a Neurostat3D-SSP analysis Given are views from superior
of [18F]FDG uptake (top) and of statistical deviation of uptake from
healthy controls color-coded as z score (bottom) see Fig 411 for
additional details
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
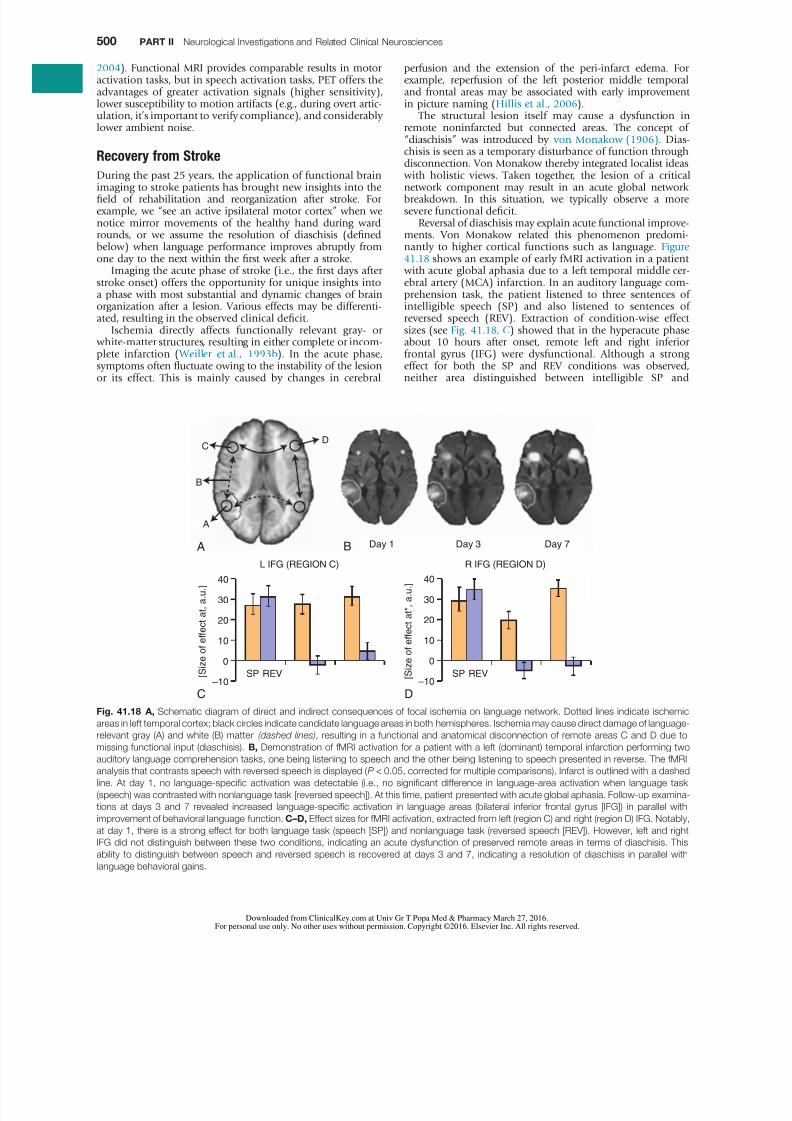
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1523
500 PART II Neurological Investigations and Related Clinical Neurosciences
perfusion and the extension of the peri-infarct edema Forexample reperfusion of the left posterior middle temporaland frontal areas may be associated with early improvementin picture naming (Hillis et al 2006)
The structural lesion itself may cause a dysfunction inremote noninfarcted but connected areas The concept ofldquodiaschisisrdquo was introduced by von Monakow (1906) Dias-chisis is seen as a temporary disturbance of function throughdisconnection Von Monakow thereby integrated localist ideas with holistic views Taken together the lesion of a criticalnetwork component may result in an acute global networkbreakdown In this situation we typically observe a moresevere functional deficit
Reversal of diaschisis may explain acute functional improve-ments Von Monakow related this phenomenon predomi-nantly to higher cortical functions such as language Figure 4118 shows an example of early fMRI activation in a patient with acute global aphasia due to a left temporal middle cer-ebral artery (MCA) infarction In an auditory language com-prehension task the patient listened to three sentences ofintelligible speech (SP) and also listened to sentences ofreversed speech (REV) Extraction of condition-wise effectsizes (see Fig 4118 C) showed that in the hyperacute phaseabout 10 hours after onset remote left and right inferiorfrontal gyrus (IFG) were dysfunctional Although a strong
effect for both the SP and REV conditions was observedneither area distinguished between intelligible SP and
2004) Functional MRI provides comparable results in motoractivation tasks but in speech activation tasks PET offers theadvantages of greater activation signals (higher sensitivity)lower susceptibility to motion artifacts (eg during overt artic-ulation itrsquos important to verify compliance) and considerablylower ambient noise
Recovery from Stroke
During the past 25 years the application of functional brainimaging to stroke patients has brought new insights into thefield of rehabilitation and reorganization after stroke Forexample we ldquosee an active ipsilateral motor cortexrdquo when wenotice mirror movements of the healthy hand during wardrounds or we assume the resolution of diaschisis (definedbelow) when language performance improves abruptly fromone day to the next within the first week after a stroke
Imaging the acute phase of stroke (ie the first days afterstroke onset) offers the opportunity for unique insights intoa phase with most substantial and dynamic changes of brainorganization after a lesion Various effects may be differenti-ated resulting in the observed clinical deficit
Ischemia directly affects functionally relevant gray- or white-matter structures resulting in either complete or incom-plete infarction ( Weiller et al 1993b) In the acute phase
symptoms often fluctuate owing to the instability of the lesionor its effect This is mainly caused by changes in cerebral
Fig 4118 A Schematic diagram of direct and indirect consequences of focal ischemia on language network Dotted lines indicate ischemic
areas in left temporal cortex black circles indicate candidate language areas in both hemispheres Ischemia may cause direct damage of language-relevant gray (A) and white (B) matter (dashed lines) resulting in a functional and anatomical disconnection of remote areas C and D due to
missing functional input (diaschisis) B Demonstration of fMRI activation for a patient with a left (dominant) temporal infarction performing two
auditory language comprehension tasks one being listening to speech and the other being listening to speech presented in reverse The fMRI
analysis that contrasts speech with reversed speech is displayed (P lt 005 corrected for multiple comparisons) Infarct is outlined with a dashed
line At day 1 no language-specific activation was detectable (ie no significant difference in language-area activation when language task
(speech) was contrasted with nonlanguage task [reversed speech]) At this time patient presented with acute global aphasia Follow-up examina-
tions at days 3 and 7 revealed increased language-specific activation in language areas (bilateral inferior frontal gyrus [IFG]) in parallel with
improvement of behavioral language function CndashD Effect sizes for fMRI activation extracted from left (region C) and right (region D) IFG Notably
at day 1 there is a strong effect for both language task (speech [SP]) and nonlanguage task (reversed speech [REV]) However left and right
IFG did not distinguish between these two conditions indicating an acute dysfunction of preserved remote areas in terms of diaschisis This
ability to distinguish between speech and reversed speech is recovered at days 3 and 7 indicating a resolution of diaschisis in parallel with
language behavioral gains
A
C D
Day 1
A
B
CD
Day 3 Day 7B
ndash10SP REV SP REV
L IFG (REGION C)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
ndash10
R IFG (REGION D)
0
10
20
[ S i z e
o f e f f e c t a t a u ]
30
40
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
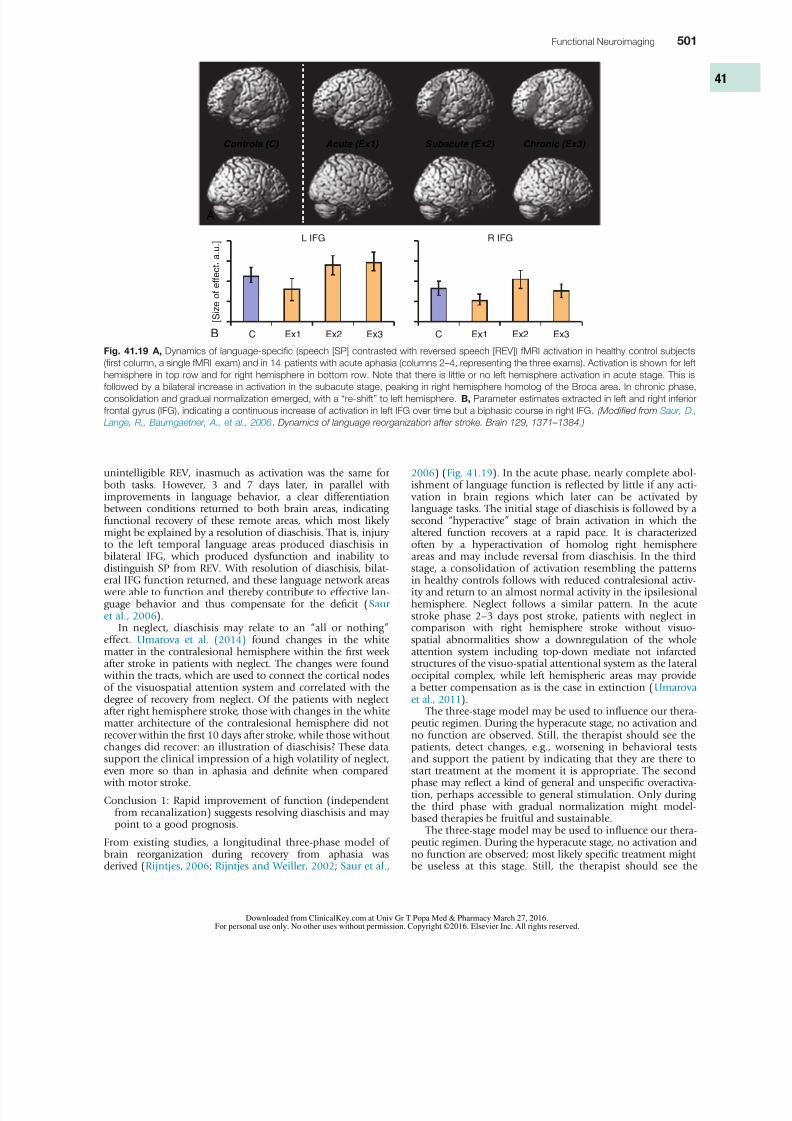
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1623
Functional Neuroimaging 501
2006) (Fig 4119) In the acute phase nearly complete abol-ishment of language function is reflected by little if any acti- vation in brain regions which later can be activated bylanguage tasks The initial stage of diaschisis is followed by asecond ldquohyperactiverdquo stage of brain activation in which thealtered function recovers at a rapid pace It is characterized
often by a hyperactivation of homolog right hemisphereareas and may include reversal from diaschisis In the thirdstage a consolidation of activation resembling the patternsin healthy controls follows with reduced contralesional activ-ity and return to an almost normal activity in the ipsilesionalhemisphere Neglect follows a similar pattern In the acutestroke phase 2ndash3 days post stroke patients with neglect incomparison with right hemisphere stroke without visuo-spatial abnormalities show a downregulation of the wholeattention system including top-down mediate not infarctedstructures of the visuo-spatial attentional system as the lateraloccipital complex while left hemispheric areas may providea better compensation as is the case in extinction (Umarova et al 2011)
The three-stage model may be used to influence our thera-
peutic regimen During the hyperacute stage no activation andno function are observed Still the therapist should see thepatients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Only duringthe third phase with gradual normalization might model-based therapies be fruitful and sustainable
The three-stage model may be used to influence our thera-peutic regimen During the hyperacute stage no activation andno function are observed most likely specific treatment mightbe useless at this stage Still the therapist should see the
unintelligible REV inasmuch as activation was the same forboth tasks However 3 and 7 days later in parallel withimprovements in language behavior a clear differentiationbetween conditions returned to both brain areas indicatingfunctional recovery of these remote areas which most likelymight be explained by a resolution of diaschisis That is injury
to the left temporal language areas produced diaschisis inbilateral IFG which produced dysfunction and inability todistinguish SP from REV With resolution of diaschisis bilat-eral IFG function returned and these language network areas were able to function and thereby contribute to effective lan-guage behavior and thus compensate for the deficit (Saur et al 2006)
In neglect diaschisis may relate to an ldquoall or nothingrdquoeffect Umarova et al (2014) found changes in the whitematter in the contralesional hemisphere within the first weekafter stroke in patients with neglect The changes were found within the tracts which are used to connect the cortical nodesof the visuospatial attention system and correlated with thedegree of recovery from neglect Of the patients with neglectafter right hemisphere stroke those with changes in the white
matter architecture of the contralesional hemisphere did notrecover within the first 10 days after stroke while those withoutchanges did recover an illustration of diaschisis These datasupport the clinical impression of a high volatility of neglecteven more so than in aphasia and definite when compared with motor stroke
Conclusion 1 Rapid improvement of function (independentfrom recanalization) suggests resolving diaschisis and maypoint to a good prognosis
From existing studies a longitudinal three-phase model ofbrain reorganization during recovery from aphasia wasderived (Rijntjes 2006 Rijntjes and Weiller 2002 Saur et al
Fig 4119 A Dynamics of language-specific (speech [SP] contrasted with reversed speech [REV]) fMRI activation in healthy control subjects
(first column a single fMRI exam) and in 14 patients with acute aphasia (columns 2ndash4 representing the three exams) Activation is shown for lefthemisphere in top row and for right hemisphere in bottom row Note that there is little or no left hemisphere activation in acute stage This is
followed by a bilateral increase in activation in the subacute stage peaking in right hemisphere homolog of the Broca area In chronic phase
consolidation and gradual normalization emerged with a ldquore-shiftrdquo to left hemisphere B Parameter estimates extracted in left and right inferior
frontal gyrus (IFG) indicating a continuous increase of activation in left IFG over time but a biphasic course in right IFG (Modified from Saur D
Lange R Baumgaetner A et al 2006 Dynamics of language reorganization after stroke Brain 129 1371ndash1384)
Controls (C) Acute (Ex1) Subacute (Ex2) Chronic (Ex3)
A
L IFG
C Ex1 Ex2 Ex3 C Ex1 Ex2 Ex3
[ S i z e
o f e f f e c t a u ] R IFG
B
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
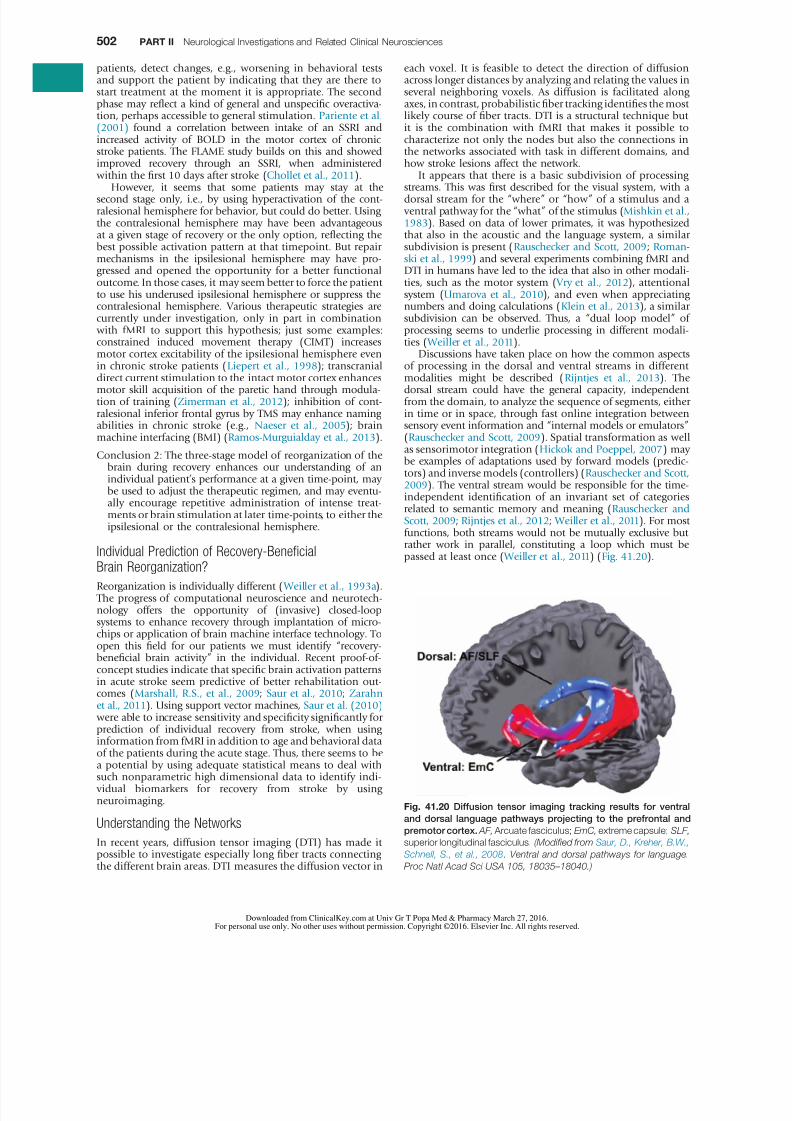
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1723
502 PART II Neurological Investigations and Related Clinical Neurosciences
each voxel It is feasible to detect the direction of diffusionacross longer distances by analyzing and relating the values inseveral neighboring voxels As diffusion is facilitated alongaxes in contrast probabilistic fiber tracking identifies the mostlikely course of fiber tracts DTI is a structural technique butit is the combination with fMRI that makes it possible tocharacterize not only the nodes but also the connections inthe networks associated with task in different domains andhow stroke lesions affect the network
It appears that there is a basic subdivision of processingstreams This was first described for the visual system with adorsal stream for the ldquowhererdquo or ldquohowrdquo of a stimulus and a ventral pathway for the ldquowhatrdquo of the stimulus (Mishkin et al 1983) Based on data of lower primates it was hypothesizedthat also in the acoustic and the language system a similarsubdivision is present (Rauschecker and Scott 2009 Roman-ski et al 1999) and several experiments combining fMRI andDTI in humans have led to the idea that also in other modali-ties such as the motor system ( Vry et al 2012) attentionalsystem (Umarova et al 2010) and even when appreciatingnumbers and doing calculations (Klein et al 2013) a similarsubdivision can be observed Thus a ldquodual loop modelrdquo ofprocessing seems to underlie processing in different modali-ties ( Weiller et al 2011)
Discussions have taken place on how the common aspects
of processing in the dorsal and ventral streams in differentmodalities might be described (Rijntjes et al 2013) Thedorsal stream could have the general capacity independentfrom the domain to analyze the sequence of segments eitherin time or in space through fast online integration betweensensory event information and ldquointernal models or emulatorsrdquo(Rauschecker and Scott 2009) Spatial transformation as wellas sensorimotor integration (Hickok and Poeppel 2007) maybe examples of adaptations used by forward models (predic-tors) and inverse models (controllers) (Rauschecker and Scott 2009) The ventral stream would be responsible for the time-independent identification of an invariant set of categoriesrelated to semantic memory and meaning (Rauschecker and Scott 2009 Rijntjes et al 2012 Weiller et al 2011) For mostfunctions both streams would not be mutually exclusive but
rather work in parallel constituting a loop which must bepassed at least once ( Weiller et al 2011) (Fig 4120)
patients detect changes eg worsening in behavioral testsand support the patient by indicating that they are there tostart treatment at the moment it is appropriate The secondphase may reflect a kind of general and unspecific overactiva-tion perhaps accessible to general stimulation Pariente et al (2001) found a correlation between intake of an SSRI andincreased activity of BOLD in the motor cortex of chronicstroke patients The FLAME study builds on this and showedimproved recovery through an SSRI when administered within the first 10 days after stroke (Chollet et al 2011)
However it seems that some patients may stay at thesecond stage only ie by using hyperactivation of the cont-ralesional hemisphere for behavior but could do better Usingthe contralesional hemisphere may have been advantageousat a given stage of recovery or the only option reflecting thebest possible activation pattern at that timepoint But repairmechanisms in the ipsilesional hemisphere may have pro-gressed and opened the opportunity for a better functionaloutcome In those cases it may seem better to force the patientto use his underused ipsilesional hemisphere or suppress thecontralesional hemisphere Various therapeutic strategies arecurrently under investigation only in part in combination with fMRI to support this hypothesis just some examplesconstrained induced movement therapy (CIMT) increasesmotor cortex excitability of the ipsilesional hemisphere even
in chronic stroke patients (Liepert et al 1998) transcranialdirect current stimulation to the intact motor cortex enhancesmotor skill acquisition of the paretic hand through modula-tion of training (Zimerman et al 2012) inhibition of cont-ralesional inferior frontal gyrus by TMS may enhance namingabilities in chronic stroke (eg Naeser et al 2005) brainmachine interfacing (BMI) (Ramos-Murguialday et al 2013)
Conclusion 2 The three-stage model of reorganization of thebrain during recovery enhances our understanding of anindividual patientrsquos performance at a given time-point maybe used to adjust the therapeutic regimen and may eventu-ally encourage repetitive administration of intense treat-ments or brain stimulation at later time-points to either theipsilesional or the contralesional hemisphere
Individual Prediction of Recovery-BeneficialBrain Reorganization
Reorganization is individually different ( Weiller et al 1993a) The progress of computational neuroscience and neurotech-nology offers the opportunity of (invasive) closed-loopsystems to enhance recovery through implantation of micro-chips or application of brain machine interface technology Toopen this field for our patients we must identify ldquorecovery-beneficial brain activityrdquo in the individual Recent proof-of-concept studies indicate that specific brain activation patternsin acute stroke seem predictive of better rehabilitation out-comes (Marshall RS et al 2009 Saur et al 2010 Zarahn et al 2011) Using support vector machines Saur et al (2010) were able to increase sensitivity and specificity significantly for
prediction of individual recovery from stroke when usinginformation from fMRI in addition to age and behavioral dataof the patients during the acute stage Thus there seems to bea potential by using adequate statistical means to deal withsuch nonparametric high dimensional data to identify indi- vidual biomarkers for recovery from stroke by usingneuroimaging
Understanding the Networks
In recent years diffusion tensor imaging (DTI) has made itpossible to investigate especially long fiber tracts connectingthe different brain areas DTI measures the diffusion vector in
Fig 4120 Diffusion tensor imaging tracking results for ventral
and dorsal language pathways projecting to the prefrontal and
premotor cortex AF Arcuate fasciculus EmC extreme capsule SLF
superior longitudinal fasciculus (Modified from Saur D Kreher BW
Schnell S et al 2008 Ventral and dorsal pathways for language
Proc Natl Acad Sci USA 105 18035ndash18040)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1823
Functional Neuroimaging 503
Experiments like these again raise the philosophical ques-tion as to whether humans have a free will or that the things we are aware of are just the surface of a pool of unconsciousprocesses that we can only partly influence Such experimentshave also led to a public discussion about responsibility if asuspect shows ldquopathologicalrdquo activations is his culpabilityreduced In these discussions care should be taken to realizethat arguments concern three levels of representation thebrain level the personal level and the societal level The con-clusions about such experiments should be drawn at eachseparate level the relevance for society should be judged bysociety itself and cannot be in the realm of neurology orpsychiatry
At the moment there is hardly a state of mind in diseaseand health that is not investigated with functional imagingEven religious feelings have been ldquocapturedrdquo in the scanner Ithas long been known that some patients with temporal epi-lepsy report strong religious experiences and it is possible toevoke such feelings with magnetic fields in healthy subjects(Booth et al 2005) Using functional imaging it appears thatbrain areas active during a religious experience in believers( Azari et al 2001 Beauregard and Paquette 2006 Kapogian-nis et al 2009) are also involved in ethical decisions empathyfor the feelings of other persons (ldquotheory of mindrdquo) andstrong emotions (Greene et al 2004 Hein and Singer 2008
Young et al 2007) Again very divergent conclusions fromthese findings are possible For some they point to the pos-sibility that religion evolved from processes that developedduring evolution and that must be applied in daily life for aperson to function properly as a member of society (Boyer 2008) In this interpretation religion could be a product ofevolution However for those who believe in divine revela-tion the information that religious feelings are processed bybrain areas that are competent for them will be whollyunspectacular
In general caution should prevail in interpreting experi-ments about psychopathology and ldquounconsciousrdquo contribu-tions to behavior As with most other ethical questions theappraisal of psychological and psychopathological findings will surely depend on the prevailing wisdom of those defining
these issues
REFERENCES
The complete reference list is available online at httpsexpertconsultinklingcom
First-lesion studies in patients based on this dual-loopmodel seem to explain deficits after stroke For example adeficit in understanding seems to be associated with a lesionin the ventral pathway through the extreme capsule whereasdeficits in repetition correlate more with lesions in the dorsalpathway (Kuumlmmerer et al 2013) These new insights in func-tional organization are essential for understanding why adeficit after a certain lesion occurs and for developing reha-bilitation models
Conscious and Unconscious Processes
If the intention to grab a pencil leads to an appropriate motionof the hand brain activations occurring before and duringthis time will be interpreted as responsible for this goal-directed movement However several recent experiments havehighlighted the difference between conscious and uncon-scious processes and that both are not necessarily alwayscongruent
Sleeping subjects show enhanced activity in those parts ofthe brain that were active while the individual was awake(Maquet et al 2000) Patients with apallic syndrome (vegeta-tive states) do not show meaningful responses to outsidestimuli which is usually interpreted to mean that they are notcapable of conscious thought However surprisingly some of
them still seem to understand at least some tasks when lyingin a scanner and instructed to imagine walking around athome they sometimes show activations in areas that aresimilar to healthy subjects doing the same task (Owen et al 2006) It should be asked therefore to what extent is con-sciousness preserved in these patients In conscious personsunconscious processes can be visualized with functionalimaging For example in patients with chronic pain theso-called placebo effect leads to activations in regions in thebrainstem and spinal cord that correlate with the pain-relievingimpact of the placebo (Eippert et al 2009a b)
Functional imaging has also been used to investigate moralquestions It is possible to correlate activation patterns withdeliberate lying (Langleben et al 2005) or with psychopathictraits (Fullam et al 2009) Some investigators call this foren-
sic imaging In certain experimental settings an investigatorcan recognize from the pattern of activation whether a promise will subsequently be broken even if subjects report that theyhad not yet reached a decision at that time point (Baum-gartner et al 2009)
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 1923
Functional Neuroimaging 503e1
REFERENCES
Alavi JB Alavi A Chawluk J et al 1988 Positron emission tom-ography in patients with glioma A predictor of prognosis Cancer62 1074ndash1078
Albert MS DeKosky ST Dickson D et al 2011 The diagnosis ofmild cognitive impairment due to Alzheimerrsquos disease recommen-dations from the National Institute on Aging-Alzheimerrsquos Associa-tion workgroups on diagnostic guidelines for Alzheimerrsquos disease Alzheimers Dement 7 270ndash279
Albin RL Minoshima S DrsquoAmato CJ et al 1996 Fluoro-deoxyglucose positron emission tomography in diffuse Lewy bodydisease Neurology 47 462ndash466
Amtage F Hellwig S Kreft A et al 2014 Neuronal correlates ofclinical asymmetry in progressive supranuclear palsy Clin NuclMed 39 319ndash325
Anchisi D Borroni B Franceschi M et al 2005 Heterogeneity ofbrain glucose metabolism in mild cognitive impairment and clini-cal progression to Alzheimer disease Arch Neurol 621728ndash1733
Avery RA Spencer SS Spanaki MV et al 1999 Effect of injectiontime on postictal SPET perfusion changes in medically refractoryepilepsy Eur J Nucl Med 26 830ndash836
Azari NP Nickel J Wunderlich G et al 2001 Neural correlatesof religious experience Eur J Neurosci 13 1649ndash1652
Baumgartner T Fischbacher U Feierabend A et al 2009 Theneural circuitry of a broken promise Neuron 64 756ndash770
Beauregard M Paquette V 2006 Neural correlates of a mysticalexperience in Carmelite nuns Neurosci Lett 405 186ndash190
Benamer TS Patterson J Grosset DG et al 2000 Accurate dif-ferentiation of parkinsonism and essential tremor using visualassessment of [123I]-FP-CIT SPECT imaging the [123I]-FP-CIT studygroup Mov Disord 15 503ndash510
Benitez-Rivero S Marin-Oyaga VA Garcia-Solis D et al 2013Clinical features and 123I-FP-CIT SPECT imaging in vascular parkin-sonism and Parkinsonrsquos disease J Neurol Neurosurg Psychiatry84 122ndash129
Bohnen NI Djang DS Herholz K et al 2012 Effectiveness andsafety of 18F-FDG PET in the evaluation of dementia a review ofthe recent literature J Nucl Med 53 59ndash71
Bohnen NI Koeppe RA Minoshima S et al 2011 Cerebralglucose metabolic features of Parkinson disease and incidentdementia longitudinal study J Nucl Med 52 848ndash855
Booth JN Koren SA Persinger MA 2005 Increased feelings ofthe sensed presence and increased geomagnetic activity at the timeof the experience during exposures to transcerebral weak complexmagnetic fields Int J Neurosci 115 1053ndash1079
Borgwardt L Hoslashjgaard L Carstensen H et al 2005Increased fluorine-18 2-fluoro-2-deoxy-d-glucose (FDG) uptake inchildhood CNS tumors is correlated with malignancy grade a study with FDG positron emission tomographymagnetic resonanceimaging coregistration and image fusion J Clin Oncol 233030ndash3037
Bouilleret V Valenti MP Hirsch E et al 2002 Correlationbetween PET and SISCOM in temporal lobe epilepsy J Nucl Med43 991ndash998
Boyer P 2008 Being human Religion bound to believe Nature 4551038ndash1039
Calcagni ML Galli G Giordano A et al 2011 Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine (F-18 FET) PET for glioma gradingassessment of individual probability of malignancy Clin NuclMed 36 841ndash847
Callot V Galanaud D Le Fur Y et al 2008 (1)H MR spectroscopyof human brain tumours a practical approach Eur J Radiol 67268ndash274
Carpentier A Pugh KR Westerveld M et al 2001 Functional MRIof language processing dependence on input modality and tempo-ral lobe epilepsy Epilepsia 42 1241ndash1254
Casse R Rowe CC Newton M et al 2002 Positron emissiontomography and epilepsy Mol Imaging Biol 4 338ndash351
Catana C Drzezga A Heiss WD et al 2012 PETMRI for neuro-logic applications J Nucl Med 53 1916ndash1925
Chang KH Song IC Kim SH et al 1998 In vivo single-voxelproton MR spectroscopy in intracranial cystic masses Am J Neu-roradiol 19 401ndash405
Chao ST Suh JH Raja S et al 2001 The sensitivity and specifi-city of FDG PET in distinguishing recurrent brain tumor from radi-onecrosis in patients treated with stereotactic radiosurgery Int JCancer 96 191ndash197
Cherry SR Blowey RW Phelps ME 2003 Physics in NuclearMedicine third ed Saunders Philadelphia
Choi JY Kim SJ Hong SB et al 2003 Extratemporal hypome-tabolism on FDG PET in temporal lobe epilepsy as a predictor ofseizure outcome after temporal lobectomy Eur J Nucl Med MolImaging 30 581ndash587
Chollet F Tardy J Albucher JF et al 2011 Fluoxetine for motorrecovery after acute ischaemic stroke (FLAME) a randomisedplacebo-controlled trial Lancet Neurol 10 (2) 123ndash130
De Witte O Lefranc F Levivier M et al 2000 FDG-PET as a prog-nostic factor in high-grade astrocytoma J Neurooncol 49157ndash163
De Witte O Levivier M Violon P et al 1996 Prognostic valuepositron emission tomography with [18F]fluoro-2-deoxy-d-glucosein the low-grade glioma Neurosurgery 39 470ndash476
Delbeke D Meyerowitz C Lapidus RL et al 1995 Optimalcutoff levels of F-18 fluorodeoxyglucose uptake in the differentia-tion of low-grade from high-grade brain tumors with PET Radiol-ogy 195 47ndash52
Devous MD Sr Thisted RA Morgan GF et al 1998 SPECTbrain imaging in epilepsy a meta-analysis J Nucl Med 39285ndash293
Di Chiro G DeLaPaz RL Brooks RA et al 1982 Glucose utiliza-tion of cerebral gliomas measured by [18F] fluorodeoxyglucose andpositron emission tomography Neurology 32 1323ndash1329
Diehl J Grimmer T Drzezga A et al 2004 Cerebral metabolicpatterns at early stages of frontotemporal dementia and semanticdementia A PET study Neurobiol Aging 25 1051ndash1056
Djang DS Janssen MJ Bohnen N et al 2012 SNM practiceguideline for dopamine transporter imaging with 123I-ioflupaneSPECT 10 J Nucl Med 53 154ndash163
Donaghy P Thomas AJ OrsquoBrien JT 2015 Amyloid PET imagingin Lewy body disorders Am J Geriatr Psychiatry 23 23ndash37
Dougall NJ Bruggink S Ebmeier KP 2004 Systematic review ofthe diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia AmJ Geriatr Psychiatry 12 554ndash570
Douglas JG Stelzer KJ Mankoff DA et al 2006 [F-18]-fluoro-deoxyglucose positron emission tomography for targeting radiationdose escalation for patients with glioblastoma multiforme clinicaloutcomes and patterns of failure Int J Radiat Oncol Biol Phys64 886ndash891
Drzezga A Arnold S Minoshima S et al 1999 18F-FDG PETstudies in patients with extratemporal and temporal epilepsy evalu-ation of an observer-independent analysis J Nucl Med 40737ndash746
Drzezga A Grimmer T Riemenschneider M et al 2005 Predic-tion of individual clinical outcome in MCI by means of geneticassessment and (18)F-FDG PET J Nucl Med 46 1625ndash1632
Duffau H 2013 Brain mapping in tumors intraoperative or extra-operative Epilepsia 54 (Suppl) 979ndash983
Duffau H 2014 The conceptual limitation to rely on intraoperativeMRI in Glioma Surgery World Neurosurg 14 S1878ndashS8750
Dunet V Rossier C Buck A et al 2012 Performance of 18F-fluoro-ethyl-tyrosine (18F-FET) PET for the differential diagnosis ofprimary brain tumor a systematic review and Metaanalysis J NuclMed 53 207ndash214
Dupont P Van Paesschen W Palmini A et al 2006 Ictal perfusionpatterns associated with single MRI-visible focal dysplastic lesionsimplications for the noninvasive delineation of the epileptogeniczone Epilepsia 47 1550ndash1557
Eckert T Barnes A Dhawan V et al 2005 FDG PET in the dif-ferential diagnosis of parkinsonian disorders Neuroimage 26912ndash921
Eckert T Tang C Ma Y et al 2008 Abnormal metabolic networksin atypical parkinsonism Mov Disord 23 727ndash733
Eckert T Van Laere K Tang C et al 2007 Quantification of Par-kinsonrsquos disease-related network expression with ECD SPECT EurJ Nucl Med Mol Imaging 34 496ndash501
Eippert F Bingel U Schoell ED et al 2009a Activation of theopioidergic descending pain control system underlies placebo anal-gesia Neuron 63 533ndash543
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2023
503e2 PART II Neurological Investigations and Related Clinical Neurosciences
Eippert F Finsterbusch J Bingel U et al 2009b Direct evidencefor spinal cord involvement in placebo analgesia Science 326 404
Fernaacutendez G de Greiff A von Oertzen J et al 2001 Languagemapping in less than 15 minutes real-time functional MRI duringroutine clinical investigation Neuroimage 14 585ndash594
Floeth FW Pauleit D Sabel M et al 2007 Prognostic value ofO-(2-18F-fluoroethyl)-L-tyrosine PET and MRI in low-grade gliomaJ Nucl Med 48 519ndash527
Foster NL Heidebrink JL Clark CM et al 2007 FDG-PETimproves accuracy in distinguishing frontotemporal dementia and Alzheimerrsquos disease Brain 130 2616ndash2635
Frisoni GB Bocchetta M Cheacutetelat G et al 2013 Imaging markersfor Alzheimer disease which vs how Neurology 81 487ndash500
Friston KJ Price CJ Fletcher P et al 1996 The trouble withcognitive subtraction Neuroimage 4 97ndash104
Fujishiro H Iseki E Kasanuki K et al 2012 Glucose hypome-tabolism in primary visual cortex is commonly associated withclinical features of dementia with Lewy bodies regardless of cogni-tive conditions Int J Geriatr Psychiatry 27 1138ndash1146
Fujishiro H Iseki E Kasanuki K et al 2013 A follow up study ofnon-demented patients with primary visual cortical hypometabo-lism prodromal dementia with Lewy bodies J Neurol Sci 33448ndash54
Fullam RS McKie S Dolan MC 2009 Psychopathic traits anddeception functional magnetic resonance imaging study Br J Psy-chiatry 194 229ndash235
Galldiks N Stoffels G Ruge MI et al 2013 Role of O-(2-18F-fluoroethyl)-L-tyrosine PET as a diagnostic tool for detection ofmalignant progression in patients with low-grade glioma J NuclMed 54 2046ndash2054
Garcia-Garcia D Clavero P Gasca Salas C et al 2012 Posteriorparietooccipital hypometabolism may differentiate mild cognitiveimpairment from dementia in Parkinsonrsquos disease Eur J NuclMed Mol Imaging 39 1767ndash1777
Garraux G Phillips C Schrouff J et al 2013 Multiclass classifica-tion of FDG PET scans for the distinction between Parkinsonrsquosdisease and atypical parkinsonian syndromes Neuroimage Clin 2883ndash893
Garraux G Salmon E Degueldre C et al 1999 Comparison ofimpaired subcortico-frontal metabolic networks in normal agingsubcortico-frontal dementia and cortical frontal dementia Neu-roimage 10 149ndash162
Gauthier S Reisberg B Zaudig M et al 2006 International Psy-chogeriatric Association Expert Conference on mild cognitiveimpairment Mild cognitive impairment Lancet 367 1262ndash1270
Glaudemans AW Enting RH Heesters MA et al 2013 Value of11C-methionine PET in imaging brain tumours and metastases EurJ Nucl Med Mol Imaging 40 615ndash635
Goffin K Dedeurwaerdere S Van Laere K et al 2008 Neuronu-clear assessment of patients with epilepsy Semin Nucl Med 38227ndash239
Goldman S Levivier M Pirotte B et al 1997 Regional methio-nine and glucose uptake in high-grade gliomas a comparative studyon PET-guided stereotactic biopsy J Nucl Med 38 1459ndash1462
Goacutemez-Riacuteo M Rodriacuteguez-Fernaacutendez A Ramos-Font C et al2008 Diagnostic accuracy of 201Thallium-SPECT and 18F-FDG-PET in the clinical assessment of glioma recurrence Eur J NuclMed Mol Imaging 35 966ndash975
Gorno-Tempini ML Hillis AE Weintraub S et al 2011 Classifi-cation of primary progressive aphasia and its variants Neurology76 1006ndash1014
Greene JD Nystrom LE Engell AD et al 2004 The neural basesof cognitive conflict and control in moral judgment Neuron 44389ndash400
Gross MW Weber WA Feldmann HJ et al 1998 The value ofF-18-fluorodeoxyglucose PET for the 3-D radiation treatment plan-ning of malignant gliomas Int J Radiat Oncol Biol Phys 41989ndash995
Grosu AL Weber WA Riedel E et al 2005 L-(methyl-11C)methionine positron emission tomography for target delineation inresected high-grade gliomas before radiotherapy Int J RadiatOncol Biol Phys 63 64ndash74
Hein G Singer T 2008 I feel how you feel but not always theempathic brain and its modulation Curr Opin Neurobiol 18153ndash158
Hellwig S Amtage F Kreft A et al 2012 [18F]FDG-PET is superiorto [123I]IBZM-SPECT for the differential diagnosis of parkinsonismNeurology 79 1314ndash1322
Herholz K 2003 PET studies in dementia Ann Nucl Med 1779ndash89
Herholz K Langen KJ Schiepers C et al 2012 Brain tumorsSemin Nucl Med 42 356ndash370
Herholz K Salmon E Perani D et al 2002a Discriminationbetween Alzheimer dementia and controls by automated analysisof multicenter FDG PET Neuroimage 17 302ndash316
Herholz K Schopphoff H Schmidt M et al 2002b Direct com-parison of spatially normalized PET and SPECT scans in Alzheimerrsquosdisease J Nucl Med 43 21ndash26
Hickok G Poeppel D 2007 The cortical organization of speechprocessing Nat Rev Neurosci 8 393ndash402
Higuchi M Tashiro M Arai H et al 2000 Glucose hypometabo-lism and neuropathological correlates in brains of dementia withLewy bodies Exp Neurol 162 247ndash256
Hillis AE Kleinman JT Newhart M et al 2006 Restoring cere-bral blood flow reveals neural regions critical for naming J Neuro-sci 26 8069ndash8073
Hirano S Eckert T Flanagan T et al 2009 Metabolic networksfor assessment of therapy and diagnosis in Parkinsonrsquos disease MovDisord 24 S725ndashS731
Holtbernd F Gagnon JF Postuma RB et al 2014 Abnormalmetabolic network activity in REM sleep behavior disorder Neurol-ogy 82 620ndash627
Hosokai Y Nishio Y Hirayama K et al 2009 Distinct patterns ofregional cerebral glucose metabolism in Parkinsonrsquos disease with and without mild cognitive impairment Mov Disord 24 854ndash862
Hu MT Taylor-Robinson SD Chaudhuri KR et al 2000 Corticaldysfunction in non-demented Parkinsonrsquos disease patients a com-bined (31)P-MRS and (18)FDG-PET study Brain 123 340ndash352
Huang C Mattis P Perrine K et al 2008 Metabolic abnormalitiesassociated with mild cognitive impairment in Parkinson diseaseNeurology 70 1470ndash1477
Imamura T Ishii K Hirono N et al 1999 Visual hallucinationsand regional cerebral metabolism in dementia with Lewy bodies(DLB) Neuroreport 10 1903ndash1907
Ishii K Imamura T Sasaki M et al 1998a Regional cerebralglucose metabolism in dementia with Lewy bodies and Alzheimerrsquosdisease Neurology 51 125ndash130
Ishii K Sakamoto S Sasaki M et al 1998b Cerebral glucosemetabolism in patients with frontotemporal dementia J NuclMed 39 1875ndash1878
Ishii K Soma T Kono AK et al 2007 Comparison of regionalbrain volume and glucose metabolism between patients with milddementia with Lewy bodies and those with mild Alzheimerrsquosdisease J Nucl Med 48 704ndash711
Jagust W Reed B Mungas D et al 2007 What does fluorodeoxy-glucose PET imaging add to a clinical diagnosis of dementia Neu-rology 69 871ndash877
Jansen NL Suchorska B Wenter V et al 2014 Dynamic 18F-FETPET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients J Nucl Med 55 198ndash203
Jansen FP Vanderheyden JL 2007 The future of SPECT in a timeof PET Nucl Med Biol 34 733ndash735
Janszky J Jokeit H Kontopoulou K et al 2005 Functional MRIpredicts memory performance after right mesiotemporal epilepsysurgery Epilepsia 46 244ndash250
Jokeit H Okujava M Woermann FG 2001 Memory fMRI lateral-izes temporal lobe epilepsy Neurology 57 1786ndash1793
Josephs KA Duffy JR Fossett TR et al 2010 FluorodeoxyglucoseF18 positron emission tomography in progressive apraxia of speechand primary progressive aphasia variants Arch Neurol 67596ndash605
Juh R Kim J Moon D et al 2004 Different metabolic patternsanalysis of Parkinsonism on the 18F-FDG PET Eur J Radiol 51223ndash233
Kapogiannis D Barbey AK Su M et al 2009 Cognitive andneural foundations of religious belief Proc Natl Acad Sci USA106 4876ndash4881
Kasenda B Haug V Schorb E et al 2013 18F-FDG PET is anindependent outcome predictor in primary central nervous systemlymphoma J Nucl Med 54 184ndash191
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2123
Functional Neuroimaging 503e3
Kempster PA Williams DR Selikhova M et al 2007 Patterns oflevodopa response in Parkinsonrsquos disease a clinico-pathologicalstudy Brain 130 2123ndash2128
Kertesz A McMonagle P 2011 The overlapping syndromes of thepick complex Curr Alzheimer Res 8 224ndash228
Kertesz A McMonagle P Blair M et al 2005 The evolution andpathology of frontotemporal dementia Brain 128 1996ndash2005
Kim CK Alavi JB Alavi A et al 1991 New grading system ofcerebral gliomas using positron emission tomography with F-18fluorodeoxyglucose J Neurooncol 10 85ndash91
Kim DW Lee SK Chu K et al 2009 Predictors of surgicaloutcome and pathologic considerations in focal cortical dysplasiaNeurology 72 211ndash216
Kim JT Bai SJ Choi KO et al 2009 Comparison of variousimaging modalities in localization of epileptogenic lesion usingepilepsy surgery outcome in pediatric patients Seizure 18504ndash510
Kipps CM Hodges JR Fryer TD et al 2009 Combined magneticresonance imaging and positron emission tomography brainimaging in behavioural variant frontotemporal degeneration refin-ing the clinical phenotype Brain 132 2566ndash2578
Klein E Moeller K Glauche V et al 2013 Processing pathways inmental arithmeticndashevidence from probabilistic fiber tracking PLoSONE 8 (1) e55455
Kloumlppel S Buumlchel C 2005 Alternatives to the Wada test a critical view of functional magnetic resonance imaging in preoperative useCurr Opin Neurol 18 418ndash423
Knowlton RC Elgavish RA Bartolucci A et al 2008 Functionalimaging II Prediction of epilepsy surgery outcome Ann Neurol64 35ndash41
Kouri N Whitwell JL Josephs KA et al 2011 Corticobasaldegeneration a pathologically distinct 4R tauopathy Nat RevNeurol 7 263ndash272
Kreher BW Hennig J Ilrsquoyasov KA 2007 Reduction of false-positive valued areas by combining probability maps Joint AnnualMeeting ISMRM- ESMRMB Berlin p 1554
Kreher BW Schnell S Mader I et al 2008 Connecting andmerging fibres pathway extraction by combining probability mapsNeuroimage 43 81ndash89
Krings T Schreckenberger M Rohde V et al 2001 Metabolic andelectrophysiological validation of functional MRI J Neurol Neu-rosurg Psychiatry 71 762ndash771
Kuhl DE Edwards RQ 1964 Cylindrical and section radioisotopescanning of the liver and brain Radiology 83 926ndash936
Kumar A Chugani HT 2013 The role of radionuclide imaging inepilepsy Part 1 Sporadic temporal and extratemporal lobe epilepsyJ Nucl Med 54 1775ndash1781
Kuumlmmerer D Hartwigsen G Kellmeyer P et al 2013 Damage to ventral and dorsal language pathways in acute aphasia Brain 136(Pt 2) 619ndash629
Langleben DD Loughead JW Bilker WB et al 2005 Tellingtruth from lie in individual subjects with fast event-related fMRIHum Brain Mapp 26 262ndash272
Langleben DD Segall GM 2000 PET in differentiation of recur-rent brain tumor from radiation injury J Nucl Med 411861ndash1867
Lee KK Salamon N 2009 [18F] fluorodeoxyglucose-positron-emission tomography and MR imaging coregistration for presurgi-cal evaluation of medically refractory epilepsy Am J Neuroradiol30 1811ndash1816
Lee SK Lee SY Yun CH et al 2006 Ictal SPECT in neocorticalepilepsies clinical usefulness and factors affecting the pattern ofhyperperfusion Neuroradiology 48 678ndash684
Leheacutericy S Cohen L Bazin B et al 2000 Functional MR evalua-tion of temporal and frontal language dominance compared withthe Wada test Neurology 54 1625ndash1633
Lehmann M Ghosh PM Madison C et al 2013 Diverging pat-terns of amyloid deposition and hypometabolism in clinical vari-ants of probable Alzheimerrsquos disease Brain 136 844ndash858
Lichy MP Plathow C Schulz-Ertner D et al 2005 Follow-upgliomas after radiotherapy 1H MR spectroscopic imaging forincreasing diagnostic accuracy Neuroradiology 47 826ndash834
Liepert J Miltner WH Bauder H et al 1998 Motor cortex plastic-ity during constraint-induced movement therapy in stroke patientsNeurosci Lett 250 5ndash8
Lim SM Katsifis A Villemagne VL et al 2009 The 18F-FDG PETcingulate island sign and comparison to 123I-beta-CIT SPECT fordiagnosis of dementia with Lewy bodies J Nucl Med 501638ndash1645
Ling H OrsquoSullivan SS Holton JL et al 2010 Does corticobasaldegeneration exist A clinicopathological re-evaluation Brain 1332045ndash2057
Lippa CF Duda JE Grossman M et al 2007 DLB and PDDboundary issues diagnosis treatment molecular pathology andbiomarkers Neurology 68 812ndash819
Litvan I Goldman JG Troumlster AI et al 2012 Diagnostic criteriafor mild cognitive impairment in Parkinsonrsquos disease MovementDisorder Society Task Force guidelines Mov Disord 27349ndash356
Lyoo CH Jeong Y Ryu YH et al 2010 Cerebral glucose metabo-lism of Parkinsonrsquos disease patients with mild cognitive impair-ment Eur Neurol 64 65ndash73
Ma Y Tang C Spetsieris PG et al 2007 Abnormal metabolicnetwork activity in Parkinsonrsquos disease test-retest reproducibilityJ Cereb Blood Flow Metab 27 597ndash605
McKeith I OrsquoBrien J Walker Z et al 2007 Sensitivity and specifi-city of dopamine transporter imaging with 123I-FP-CIT SPECT indementia with Lewy bodies a phase III multicentre study LancetNeurol 6 305ndash313
McKeith IG Dickson DW Lowe J et al 2005 Diagnosis andmanagement of dementia with Lewy bodies third report of the DLBConsortium Neurology 65 1863ndash1872
McKhann GM Knopman DS Chertkow H et al 2011 The diag-nosis of dementia due to Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 263ndash269
Madhavan A Whitwell JL Weigand SD et al 2013 FDG PETand MRI in logopenic primary progressive aphasia versus dementiaof the Alzheimerrsquos type PLoS ONE 8 e62471
Maquet P Laureys S Peigneux P et al 2000 Experience-dependentchanges in cerebral activation during human REM sleep Nat Neu-rosci 3 831ndash836
Marshall RS Zahran E Alon L et al 2009 Early imaging corre-lates of subsequent motor recovery after stroke Ann Neurol 65596ndash602
Marshall VL Reininger CB Marquardt M et al 2009 Parkinsonrsquosdisease is overdiagnosed clinically at baseline in diagnosticallyuncertain cases a 3-year European multicenter study with repeat[123I]FP-CIT SPECT Mov Disord 24 500ndash508
Meyer PT Frings L Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 2 biomarker imaging of cognitive impairmentin Lewy-body diseases Curr Opin Neurol 27 398ndash404
Meyer PT Hellwig S 2014 Update on SPECT and PET inparkinsonismmdashpart 1 imaging of differential diagnosis CurrOpin Neurol 27 390ndash397
Meyer PT Sattler B Winz OH et al 2008 Kinetic analyses of[123I]IBZM SPECT for quantification of striatal dopamine D2receptor binding a critical evaluation of the single-scan approachNeuroimage 42 548ndash558
Meyer PT Schreckenberger M Spetzger U et al 2001 Compari-son of visual and ROI-based brain tumour grading using 18F-FDGPET ROC analyses Eur J Nucl Med 28 165ndash174
Meyer PT Sturz L Sabri O et al 2003a Preoperative motorsystem brain mapping using positron emission tomography andstatistical parametric mapping hints on cortical reorganisationJ Neurol Neurosurg Psychiatry 74 471ndash478
Meyer PT Sturz L Schreckenberger M et al 2003b Preoperativemapping of cortical language areas in adult brain tumour patientsusing PET and individual non-normalised SPM analyses Eur JNucl Med Mol Imaging 30 951ndash960
Mielke R Herholz K Grond M et al 1992 Severity of vasculardementia is related to volume of metabolically impaired tissue Arch Neurol 49 909ndash913
Minoshima S Foster NL Sima AA et al 2001 Alzheimerrsquosdisease versus dementia with Lewy bodies cerebral metabolicdistinction with autopsy confirmation Ann Neurol 50358ndash365
Minoshima S Frey KA Koeppe RA et al 1995 A diagnosticapproach in Alzheimerrsquos disease using three-dimensional
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2223
503e4 PART II Neurological Investigations and Related Clinical Neurosciences
stereotactic surface projections of fluorine-18-FDG PET J NuclMed 36 1238ndash1248
Minoshima S Giordani B Berent S et al 1997 Metabolic reduc-tion in the posterior cingulate cortex in very early Alzheimerrsquosdisease Ann Neurol 42 85ndash94
Mishkin M Ungerleider L Macko KA 1983 Object vision andspatial vision two visual pathways Trends Neurosci 6 414ndash417
Moumlller-Hartmann W Herminghaus S Krings T et al 2002 Clini-cal application of proton magnetic resonance spectroscopy in thediagnosis of intracranial mass lesions Neuroradiology 44371ndash381
Mosconi L Brys M Switalski R et al 2007 Maternal familyhistory of Alzheimerrsquos disease predisposes to reduced brain glucosemetabolism Proc Natl Acad Sci USA 104 19067ndash19072
Mosconi L Mistur R Switalski R et al 2009 Declining brainglucose metabolism in normal individuals with a maternal historyof Alzheimer disease Neurology 72 513ndash520
Mosconi L Tsui WH De Santi S et al 2005 Reduced hippocam-pal metabolism in MCI and AD automated FDG-PET image analy-sis Neurology 64 1860ndash1867
Mosconi L Tsui WH Herholz K et al 2008 Multicenter stand-ardized 18F-FDG PET diagnosis of mild cognitive impairment Alzheimerrsquos disease and other dementias J Nucl Med 49390ndash398
Murphy PS Viviers L Abson C et al 2004 Monitoring temozolo-mide treatment of low-grade glioma with proton magnetic reso-nance spectroscopy Br J Cancer 90 781ndash786
Naeser MA Martin PI Nicholas M et al 2005 Improved picturenaming in chronic aphasia after TMS to part of right Brocarsquos areaan open-protocol study Brain Lang 93 95ndash105
Nelson SJ Graves E Pirzkall A et al 2002 In vivo molecularimaging for planning radiation therapy of gliomas an applicationof 1H MRSI J Magn Reson Imaging 16 464ndash476
Nestor PJ Graham NL Fryer TD et al 2003 Progressive non-fluent aphasia is associated with hypometabolism centered on theleft anterior insula Brain 126 2406ndash2418
Newberg AB Alavi A Berlin J et al 2000 Ipsilateral and contral-ateral thalamic hypometabolism as a predictor of outcome aftertemporal lobectomy for seizures J Nucl Med 41 1964ndash1968
Newton MR Berkovic SF Austin MC et al 1995 SPECT in thelocalisation of extratemporal and temporal seizure foci J NeurolNeurosurg Psychiatry 59 26ndash30
Nihashi T Dahabreh IJ Terasawa T 2013 Diagnostic accuracy ofPET for recurrent glioma diagnosis a meta-analysis Am J Neuro-radiol 34 944ndash950 S1ndashS11
OrsquoBrien TJ So EL Mullan BP et al 1998 Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of SPECTin localizing the surgical seizure focus Neurology 50 445ndash454
OrsquoSullivan SS Massey LA Williams DR et al 2008 Clinicaloutcomes of progressive supranuclear palsy and multiple systematrophy Brain 131 1362ndash1372
Owen AM Coleman MR Boly M et al 2006 Detecting aware-ness in the vegetative state Science 313 1402
Padma MV Said S Jacobs M et al 2003 Prediction of pathologyand survival by FDG PET in gliomas J Neurooncol 64 227ndash237
Papathanasiou ND Boutsiadis A Dickson J et al 2012 Diagnos-tic accuracy of 123I-FP-CIT (DaTSCAN) in dementia with Lewybodies a meta-analysis of published studies Parkinsonism RelatDisord 18 225ndash229
Pappatagrave S Santangelo G Aarsland D et al 2011 Mild cognitiveimpairment in drug-naive patients with PD is associated with cer-ebral hypometabolism Neurology 77 1357ndash1362
Pariente J Loubinoux I Carel C et al 2001 Fluoxetine modulatesmotor performance and cerebral activation of patients recoveringfrom stroke Ann Neurol 50 (6) 718ndash729
Patronas NJ Di Chiro G Kufta C et al 1985 Prediction of sur- vival in glioma patients by means of positron emission tomographyJ Neurosurg 62 816ndash882
Pauleit D Floeth F Hamacher K et al 2005 O-(2-[18F]fluoroethyl)-L -tyrosine PET combined with MRI improves thediagnostic assessment of cerebral gliomas Brain 128 (Pt 3)678ndash687
Pauleit D Stoffels G Bachofner A et al 2009 Comparison of(18)F-FET and (18)F-FDG PET in brain tumors Nucl Med Biol36 779ndash787
Peppard RF Martin WR Carr GD et al 1992 Cerebral glucosemetabolism in Parkinsonrsquos disease with and without dementia Arch Neurol 49 1262ndash1268
Petersen RC Smith GE Waring SC et al 1999 Mild cognitiveimpairment clinical characterization and outcome Arch Neurol56 303ndash308
Phelps ME Hoffman EJ Mullani NA et al 1975 Applicationof annihilation coincidence detection to transaxial reconstructiontomography J Nucl Med 16 210ndash224
Pirotte B Goldman S Brucher JM et al 1994 PET in stereotacticconditions increases the diagnostic yield of brain biopsy StereotactFunct Neurosurg 63 144ndash149
Pirotte B Goldman S Dewitte O et al 2006 Integrated positronemission tomography and magnetic resonance imaging-guidedresection of brain tumors a report of 103 consecutive proceduresJ Neurosurg 104 238ndash253
Pirotte B Goldman S Massager N et al 2004 Combined use of18F-fluorodeoxyglucose and 11C-methionine in 45 positron emis-sion tomography-guided stereotactic brain biopsies J Neurosurg101 476ndash483
Pirotte BJ Levivier M Goldman S et al 2009 Positron emissiontomography-guided volumetric resection of supratentorial high-grade gliomas a survival analysis in 66 consecutive patients Neu-rosurgery 64 471ndash481
Poumlpperl G Kreth FW Herms J et al 2006 Analysis of18F-FET PET for grading of recurrent gliomas is evaluation ofuptake kinetics superior to standard methods J Nucl Med 47393ndash403
Poston KL Tang CC Eckert T et al 2012 Network correlates ofdisease severity in multiple system atrophy Neurology 781237ndash1244
Pressman PS Miller BL 2014 Diagnosis and management ofbehavioral variant frontotemporal dementia Biol Psychiatry 75574ndash581
Rabinovici GD Jagust WJ Furst AJ et al 2008 A-beta amyloidand glucose metabolism in three variants of primary progressiveaphasia Ann Neurol 64 388ndash401
Ramos-Murguialday A Broetz D Rea M et al 2013 Brain-machine interface in chronic stroke rehabilitation a controlledstudy Ann Neurol 74 (1) 100ndash108
Rascovsky K Hodges JR Knopman D et al 2011 Sensitivity ofrevised diagnostic criteria for the behavioural variant of frontotem-poral dementia Brain 134 2456ndash2477
Rauschecker JP Scott SK 2009 Maps and streams in the auditorycortex nonhuman primates illuminate human speech processingNat Neurosci 12 718ndash724
Reiman EM Caselli RJ Chen K et al 2001 Declining brainactivity in cognitively normal apolipoprotein E epsilon 4 heterozy-gotes A foundation for using positron emission tomography toefficiently test treatments to prevent Alzheimerrsquos disease Proc Natl Acad Sci USA 98 3334ndash3339
Reiman EM Caselli RJ Yun LS et al 1996 Preclinicalevidence of Alzheimerrsquos disease in persons homozygous for theepsilon 4 allele for apolipoprotein E N Engl J Med 334752ndash758
Reiman EM Chen K Alexander GE et al 2004 Functional brainabnormalities in young adults at genetic risk for late-onset Alzhe-imerrsquos dementia Proc Natl Acad Sci USA 101 284ndash289
Reinges MH Krings T Meyer PT et al 2004 Preoperativemapping of cortical motor function prospective comparison offunctional magnetic resonance imaging and [15O]-H2O-positronemission tomography in the same co-ordinate system Nucl MedCommun 25 987ndash997
Rijntjes M 2006 Mechanisms of recovery in stroke patients withhemiparesis or aphasia new insights old questions and themeaning of therapies Curr Opin Neurol 19 76ndash83
Rijntjes M Weiller C 2002 Recovery of motor and language abili-ties after stroke the contribution of functional imaging Prog Neu-robiol 66 109ndash122
Rijntjes M Weiller C Bormann T Musso M 2012 The dual loopmodel its relation to language and other modalities Front EvolNeurosci 4 9
Rijntjes M Weiller C 2013 Introduction The dual loop model inlanguage and other modalities an interdisciplinary approach BrainLang 127 (2) 177ndash180
Downloaded from ClinicalKeycom at Univ Gr T Popa Med amp Pharmacy March 27 2016For personal use only No other uses without permission Copyright copy2016 Elsevier Inc All rights reserved
8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189

8182019 Functional Neuroimaging Functional Magnetic Resonance Imaging Positron Emission Tomography and Single-Phhellip
httpslidepdfcomreaderfullfunctional-neuroimaging-functional-magnetic-resonance-imaging-positron-emission 2323
Functional Neuroimaging 503e5
Rinne JO Laine M Kaasinen V et al 2002 Striatal dopaminetransporter and extrapyramidal symptoms in frontotemporaldementia Neurology 58 1489ndash1493
Romanski LM Tian B Fritz J et al 1999 Dual streams of audi-tory afferents target multiple domains in the primate prefrontalcortex Nat Neurosci 2 1131ndash1136
Sabsevitz DS Swanson SJ Hammeke TA et al 2003 Use ofpreoperative functional neuroimaging to predict language deficitsfrom epilepsy surgery Neurology 60 1788ndash1792
Salmon E Garraux G Delbeuck X et al 2003 Predominant ven-tromedial frontopolar metabolic impairment in frontotemporaldementia Neuroimage 20 435ndash440
Salmon E Lespagnard S Marique P et al 2005 Cerebral meta-bolic correlates of four dementia scales in Alzheimerrsquos disease JNeurol 252 283ndash290
Saur D Kreher BW Schnell S et al 2008 Ventral and dorsalpathways for language Proc Natl Acad Sci USA 10518035ndash18040
Saur D Lange R Baumgaetner A et al 2006 Dynamics of lan-guage reorganization after stroke Brain 129 1371ndash1384
Saur D Ronneberger O Kuumlmmerer D et al 2010 Early functionalmagnetic resonance imaging activations predict language outcomeafter stroke Brain 133 (Pt 4) 1252ndash1264
Schifter T Hoffman JM Hanson MW et al 1993 Serial FDG-PETstudies in the prediction of survival in patients with primary braintumors J Comput Assist Tomogr 17 509ndash561
Schreckenberger M Spetzger U Sabri O et al 2001 Localisationof motor areas in brain tumour patients a comparison of preopera-tive [18F]FDG-PET and intraoperative cortical electrostimulationEur J Nucl Med 28 1394ndash1403
Shin WC Hong SB Tae WS et al 2002 Ictal hyperperfusionpatterns according to the progression of temporal lobe seizuresNeurology 58 373ndash380
Silverman DH Small GW Chang CY et al 2001 Positron emis-sion tomography in evaluation of dementia Regional brain metab-olism and long-term outcome JAMA 286 2120ndash2127
Small GW Ercoli LM Silverman DH et al 2000 Cerebral meta-bolic and cognitive decline in persons at genetic risk for Alzheimerrsquosdisease Proc Natl Acad Sci USA 97 6037ndash6042
Small GW Mazziotta JC Collins MT et al 1995 Apolipopro-tein E type 4 allele and cerebral glucose metabolism in relatives atrisk for familial Alzheimer disease JAMA 273 942ndash947
Smits A Westerberg E Ribom D 2008 Adding 11C-methioninePET to the EORTC prognostic factors in grade 2 gliomas Eur JNucl Med Mol Imaging 35 65ndash71
Sokoloff L 1977 Relation between physiological function andenergy metabolism in the central nervous system J Neurochem29 13ndash26
Spanaki MV Spencer SS Corsi M et al 1999 Sensitivity andspecificity of quantitative difference SPECT analysis in seizure local-ization J Nucl Med 40 730ndash736
Spehl TS Hellwig S Amtage F et al 2014 Syndrome-specificpatterns of regional cerebral glucose metabolism in posterior corti-cal atrophy in comparison to dementia with Lewy bodies and Alzheimerrsquos disease-A [F-18]-Fdg Pet Study J Neuroimagingdoi101111jon12104
Sperling RA Aisen PS Beckett LA et al 2011 Toward definingthe preclinical stages of Alzheimerrsquos disease recommendationsfrom the National Institute on Aging-Alzheimerrsquos Association work-groups on diagnostic guidelines for Alzheimerrsquos disease AlzheimersDement 7 280ndash292
Tang CC Poston KL Eckert T et al 2010a Differential diagnosisof parkinsonism a metabolic imaging study using pattern analysisLancet Neurol 9 149ndash158
Tang CC Poston KL Dhawan V et al 2010b Abnormalities inmetabolic network activity precede the onset of motor symptomsin Parkinsonrsquos disease J Neurosci 30 1049ndash1056
Teune LK Bartels AL de Jong BM et al 2010 Typical cerebralmetabolic patterns in neurodegenerative brain diseases MovDisord 25 2395ndash2404
Tolosa E Wenning G Poewe W 2006 The diagnosis of Parkinsonrsquosdisease Lancet Neurol 5 75ndash86
Tripathi M Dhawan V Peng S et al 2013 Differential diagnosisof parkinsonian syndromes using F-18 fluorodeoxyglucose positronemission tomography Neuroradiology 55 483ndash492
Umarova RM Reisert M Beier TU et al 2014 Attention-networkspecific alterations of structural connectivity in the undamaged white matter in acute neglect Hum Brain Mapp 35 4678ndash4692
Umarova RM Saur D Schnell S et al 2010 Structural connectiv-ity for visuospatial attention significance of ventral pathwaysCereb Cortex 20 121ndash129
Umarova RM Saur D Kaller CP et al 2011 Acute visual neglectand extinction distinct functional state of visuospatial attentionsystem Brain 134 3310ndash3325
Vander Borght T Minoshima S Giordani B et al 1997 Cerebralmetabolic differences in Parkinsonrsquos and Alzheimerrsquos diseasesmatched for dementia severity J Nucl Med 38 797ndash802
Von Monakow C 1906 Aphasie und Diaschisis NeurologischesCentralblatt 25 1026ndash1038
Vry MS Saur D Rijntjes M et al 2012 Ventral and dorsal fibersystems for imagined and executed movement Exp Brain Res 219203ndash216
Wadia PM Lang AE 2007 The many faces of corticobasal degen-eration Parkinsonism Relat Disord 13 S336ndashS340
Wang SX Boethius J Ericson K 2006 FDG-PET on irradiatedbrain tumor ten yearsrsquo summary Acta Radiol 47 85ndash90
Weil S Noachtar S Arnold S et al 2001 Ictal ECD-SPECT dif-ferentiates between temporal and extratemporal epilepsy confirma-tion by excellent postoperative seizure control Nucl MedCommun 22 233ndash237
Weiller C Bormann T Saur D et al 2011 How the ventral pathwaygot lost and what its recovery might mean Brain Lang 11829ndash39
Weiller C Chollet F Friston KJ et al 1992 Functional reorgani-zation of the brain in recovery from striatocapsular infarction inman Ann Neurol 31 (5) 463ndash472
Weiller C Ramsay SC Wise RJ et al 1993a Individual patternsof functional reorganization in the human cerebral cortex aftercapsular infarction Ann Neurol 33 181ndash189
Weiller C Willmes K Reiche W et al 1993b The case of aphasiaof neglect after striatocapsular infarction Brain 116 1509ndash1525
Willmann O Wennberg R May T et al 2007 The contribution of18F-FDG PET in preoperative epilepsy surgery evaluation forpatients with temporal lobe epilepsy A meta-analysis Seizure 16509ndash520
Won HJ Chang KH Cheon JE et al 1999 Comparison of MRimaging with PET and ictal SPECT in 118 patients with intractableepilepsy Am J Neuroradiol 20 593ndash599
Yong SW Yoon JK An YS et al 2007 A comparison of cerebralglucose metabolism in Parkinsonrsquos disease Parkinsonrsquos diseasedementia and dementia with Lewy bodies Eur J Neurol 141357ndash1362
Young L Cushman F Hauser M et al 2007 The neural basis ofthe interaction between theory of mind and moral judgment ProcNatl Acad Sci USA 104 8235ndash8240
Yuan Y Gu ZX Wei WS 2009 Fluorodeoxyglucose-positron-emission tomography single-photon emission tomography andstructural MR imaging for prediction of rapid conversion to Alzhe-imer disease in patients with mild cognitive impairment a meta-analysis Am J Neuroradiol 30 404ndash410
Yun CH Lee SK Lee SY et al 2006 Prognostic factors in neocorti-cal epilepsy surgery multivariate analysis Epilepsia 47 574ndash579
Zaknun JJ Bal C Maes A et al 2008 Comparative analysis ofMR imaging ictal SPECT and EEG in temporal lobe epilepsy aprospective IAEA multi-center study Eur J Nucl Med Mol Imaging35 107ndash115
Zalewski N Botha H Whitwell JL et al 2014 FDG-PET in patho-logically confirmed spontaneous 4R-tauopathy variants J Neurol261 710ndash716
Zarahn E Alon L Ryan SL et al 2011 Prediction of motor recov-ery using initial impairment and fMRI 48 h poststroke CerebCortex 21 2712ndash2721
Zhang S Han D Tan X et al 2012 Diagnostic accuracy of 18F-FDG and 11 C-PIB-PET for prediction of short-term conversion to Alzheimerrsquos disease in subjects with mild cognitive impairment IntJ Clin Pract 66 185ndash198
Zimerman M Heise KF Hoppe J et al 2012 Transcranial directcurrent stimulation to the intact motor cortex enhances motor skillacquisition of the paretic hand through modulation of trainingStroke 43 (8) 2185ndash2189