Embed Size (px)
Citation preview

Molecular Genetics and Metabolism 104 (2011) 677–681
Contents lists available at SciVerse ScienceDirect
Molecular Genetics and Metabolism
j ourna l homepage: www.e lsev ie r .com/ locate /ymgme
Hepatorenal findings in obligate heterozygotes for autosomal recessive polycystickidney disease
Meral Gunay-Aygun a,b,⁎, Baris I. Turkbey c, Joy Bryant a, Kailash T. Daryanani d, Maya Tuchman Gerstein a,Katie Piwnica-Worms a, Peter Choyke c, Theo Heller e, William A. Gahl a,b
a Medical Genetics Branch, National Human Genome Research Institute, Bethesda, MD, USAb The Intramural Program of the Office of Rare Diseases, Bethesda, MD, USAc Molecular Imaging Program, National Cancer Institute, Bethesda, MD, USAd National Institutes of Health Clinical Center, Bethesda, MD, USAe National Institute of Diabetes and Digestive and Kidney Diseases, USA
⁎ Corresponding author at: NHGRI, NIH, 10 Center Dr.MD 20892, USA.
E-mail address: [email protected] (M. Gunay-A
1096-7192/$ – see front matter. Published by Elsevier Idoi:10.1016/j.ymgme.2011.09.001
a b s t r a c t
a r t i c l e i n f oArticle history:Received 29 July 2011Received in revised form 1 September 2011Accepted 1 September 2011Available online 7 September 2011
Keywords:Autosomal recessive polycystic kidneydiseaseCongenital hepatic fibrosisPKHD1Polycytsic liver diseaseNephrocalcinosisMedullary sponge kidney
Autosomal recessive polycystic kidney disease (ARPKD), characterized by progressive cystic degeneration of thekidneys and congenital hepaticfibrosis (CHF), is themost common childhood onset ciliopathy,with an estimatedfrequency of 1 in 20,000 births. It is caused by mutations in PKHD1. The carrier frequency for ARPKD in the gen-eral population is estimated at 1 in 70. Given the recessive inheritance pattern, individuals who are heterozygousfor PKHD1mutations are not expected to have clinical findings. We performed ultrasound (USG) evaluations on110 parents from 64 independent ARPKD families and identified increased medullary echogenicity in 6 (5.5%)and multiple small liver cysts in 10 parents (9%). All ARPKD parents with these abnormal imaging findingswere asymptomatic; kidney and liver function tests were unremarkable. Complete sequencing of PKHD1 in the16 ARPKD parents with abnormal imaging confirmed the mutation transmitted to the proband, but did not re-veal any other pathogenic variants. Our data suggest that carrier status for ARPKD is a predisposition to polycysticliver disease and renal involvement associatedwith increasedmedullary echogenicity on USG.Whether some ofthese individuals become symptomatic as they age remains to be determined.
Bldg 10, Rm 10C103, Bethesda,
ygun).
nc.
Published by Elsevier Inc.
1. Introduction
Autosomal recessive polycystic kidney disease (ARPKD) is charac-terized by progressive cystic degeneration of the kidneys resulting inkidney failure and congenital hepatic fibrosis (CHF) often complicatedwith portal hypertension [1–3]. Renal cysts in ARPKD originate from di-lated collecting ducts. Most ARPKD patients present perinatally or inchildhood; a minority present in adulthood.
ARPKD is caused by mutations in the PKHD1 gene that encodesfibrocystin/polyductin, a protein that functions on primary non-mo-tile cilia [4,5]. ARPKD is the most common childhood-onset ciliopathywith an estimated frequency of 1 in 20,000. The carrier frequency forpathogenic PKHD1mutations is estimated to be approximately 1 in 70[6]. Given the recessive pattern of inheritance, parents of ARPKD pa-tients are not expected to develop clinical features. However, thishas not been systematically studied.
We performed ultrasound (USG) evaluations on 110 parents and amaternal grandmother from 64 independent ARPKD families. We iden-tified various abnormalities, includingmultiple liver cysts and increased
renal medullary echogenicity. Here we present, the imaging, clinicaland molecular findings in this group of ARPKD family members.
2. Methods
2.1. Patients
All patients and their parents were enrolled in the protocol, “Clin-ical Investigations into the Kidney and Liver Disease in Autosomal Re-cessive Polycystic Kidney Disease/Congenital Hepatic Fibrosis andother Ciliopathies” (www.clinicaltrials.gov, trial NCT00068224), ap-proved by the NHGRI Institutional Review Board and gave written in-formed consent. Patients who carried a clinical diagnosis of ARPKDmade by a nephrologist were qualified to enroll. Evaluations of theindex cases at the NIH Clinical Center included complete abdominalstandard probe and high-resolution ultrasound (HR-USG) and mag-netic resonance imaging (MRI), comprehensive biochemical testingof blood and urine and sequencing of the PKHD1 gene. The clinical di-agnosis of ARPKD for each index case at NIH was based upon estab-lished criteria [2,7] including typical kidney and liver involvementon imaging and/or biopsy and autosomal recessive inheritance. Allparents were evaluated by standard and HR-USG; abdominal MRI

678 M. Gunay-Aygun et al. / Molecular Genetics and Metabolism 104 (2011) 677–681
and magnetic resonance cholangiopancreatography (MRCP) wereperformed on parents with abnormalities on standard probe USG.
2.2. Sequencing and analysis
Complete sequencing of PKHD1 was performed in all patients.When DNA samples were available, mutation analysis in parentswas performed to determine the parental origin of the mutationsidentified in the proband. Complete sequencing of the PKHD1 genewas performed in selected parents with imaging abnormalities.
For the longest open reading frame of PKHD1, coding exons (2–67)and their intronic boundaries were sequenced in two directions using aBeckman CEQ 8000 system (Beckman Coulter, Inc., Fullerton, CA) and acontract with Agencourt (Beverly, MA). Sequencher Software (Gene-Codes, AnnArbor,MI)was used to analyzeDNAvariants. The pathogenic-ity of missense variants was evaluated as described [8] using segregationanalysis, general population frequencies, 3 computational predictiontools (Align GVGD [http://agvgd.iarc.fr/agvgd_input.php]; PolyPhen[http://coot.embl.de/PolyPhen/]; and SNAP [http://cubic.bioc.columbia.edu/services/SNAP/]) and the splice variant interpretation software Net-Gene2 Server (http://www.cbs.dtu.dk/services/NetGene2/).
2.3. Imaging studies
Complete abdominal USG evaluations were performed using stan-dard (4 MHz) and high resolution (7 MHz) ultrasonographic probesby a single technologist (K.T.D.) (AVI Sequoia Inc, Mountain View,CA). Magnetic resonance imaging (MRI) was performed on a 1.5 or3 Tesla machine (Philips Medical Systems, NA, Bothell, Washington;General Electric Healthcare, Waukesha, WI, USA) without intrave-nous contrast media. USG, MRI and MRCP images were evaluated bya team of 2 radiologists (B.I.T and P.C).
3. Results
3.1. Patient characteristics
In 93 patients the clinical diagnosis of ARPKD was confirmed afterNIH evaluations. One family contributed 4 affected siblings, 7 familiescontributed 2 siblings, and one family contributed an aunt and niece
Table 1Kidney and liver imaging findings in parents of children with ARPKD.
Parent no. Diagnosis in offspring PKHD1 mutation
1 ARPKD-mutation confirmed p.Arg1624Trp2 ARPKD-clinical diagnosis –
3 ARPKD-mutation confirmed p.Thr3035fs or p.Ala293Vala
4 ARPKD-mutation confirmed p.Thr36Met or p.Ile222Vala
5 ARPKD-mutation confirmed p.Thr36Met6 ARPKD-clinical diagnosis –
7 ARPKD-mutation confirmed p.Thr36Met8 ARPKD-mutation confirmed p.Thr36Met9 ARPKD-clinical diagnosis –
10 ARPKD-mutation confirmedb –
11 ARPKD-mutation confirmed p.Thr36Met12 ARPKD-mutation confirmed p.Phe2374fs13 ARPKD-mutation confirmed p.Thr36Met14 ARPKD-mutation confirmed p.Val1741Met15 ARPKD-mutation confirmed p.Ile246Thr16 ARPKD-mutation confirmed p.Trp2690Arg or IVS55+1 GNAa
17 ARPKD-mutation confirmed p.Arg2573Cys or unknowna
18 ARPKD-mutation confirmed p.Tyr486X19 ARPKD-mutation confirmed p.Thr3035fs or p.Ala293Vala
20 ARPKD-mutation confirmed p.Ala1254fs21 ARPKD-mutation confirmed p.Thr36Met22 ARPKD-clinical diagnosis –
F: female, M: male.a In these families parental origin of the mutations could not be determined since parenb In this patient only one PKHD1 mutation that was inherited from the father was identi
pair leaving 82 independent families. In 73 patients from 63 familiesthe diagnosis was confirmed molecularly; clinical and mutationaldata from these 73 patients were previously published [8,9].
A total of 110 parents (62 mothers and 48 fathers) and a maternalgrandmother from 63 independent ARPKD families were available forevaluation. Eighty five parents were frommolecularly confirmed familiesand 25 were from ARPKD families in which the diagnosis wasmade based on clinical criteria. Mothers' ages ranged from 27 to66 years (39±7.2), fathers' ages ranged from 29 to 58 years (40±6.3)and ages of the total group ranged from 27 to 66 years (39.5±6.8).
3.2. Imaging findings
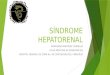
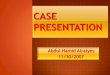
Kidney USG showed increased medullary echogenicity in 6 mothers(5.5%) whose ages ranged from 30 to 62 years (38.8±11.8) (Table 1,Figs. 1A–G). Multiple small liver cysts were identified in 10 parents(9%) including 5mothers and 5 fathers (Figs. 2 A–L). The ages of the par-ents with multiple liver cysts ranged from 36 to 49 years (44.2±4.1).These liver cysts were mostly small and peripherally located. The find-ings of increased medullary echogenicity and liver cysts in all patientswere detected by both standard and high resolution ultrasound probes.MRCP imageswere inconclusive in terms of the connectivity of the cyststo the biliary system (Figs. 2A–F).
A 44 year old father with multiple liver cysts (Table 1, parent no.:16, Fig. 2A) also had unilateral multiple parapelvic kidney cysts(Fig. 1H). Multiple unilateral kidney cysts were detected in anotherparent (#17). A moderately increased liver echo pattern associatedwith coarse texture suggestive of CHF, was detected in 4 parents(Table 1, parents 12, 14, 18 and 19, Fig. 2L) including 2 with multipleliver cysts (parents 12 and 14) and two with splenomegaly (parents14 and 19) [10]. A total of 9 parents had mild splenomegaly (spleenlengths 15–16 cm); in 5, this was in the absence of fatty changes ofthe liver. Incidentally, fatty changes in the liver suggested by in-creased echogenicity in association with smooth echo texture weredetected in 20 parents [10].
Two other parents with multiple liver cysts (Table 1, parent nos.11 and 15) at ages 41 and 46, also had 2 kidney cysts each. Fiveother fathers ages 38 to 46 had single liver cysts. Two mothers atages 41 and 46 and a father at age 36 had 2 renal cysts and singlerenal cysts were detected in 7 parents ages 36 to 49.
Sex Age Affected status
F 62 Bilateral nephrocalcinosisF 33 Bilateral nephrocalcinosisF 36 Bilateral nephrocalcinosisF 39 Bilateral nephrocalcinosisF 30 Bilateral nephrocalcinosisF 33 Bilateral nephrocalcinosisF 45 Multiple liver cystsM 49 Multiple liver cystsM 49 Multiple liver cystsF 42 Multiple liver cystsF 41 Multiple liver cysts, 2 kidney cystsM 36 Multiple liver cysts, moderately hyperechoic liverM 42 Multiple liver cysts, gall bladder polypF 48 Multiple liver cysts, moderately hyperechoic liver, splenomegalyF 46 Multiple liver cysts, splenomegaly, 2 kidney cystsM 44 Multiple liver cysts, unilateral multiple kidney cystsF 40 Unilateral multiple kidney cystsM 46 Moderately hyperechoic liver, single liver cyst, single kidney cystM 36 Moderately hyperechoic liver, splenomegalyM 41 Gall bladder polypM 44 Gall bladder polypsM 30 Splenomegaly
tal DNA was not available.fied.

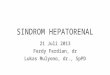
A B
C D
E F
G H
Fig. 1. KidneyUSG images of parents of patientswith ARPKD. Standard probe (A) and highresolution (B) renal USG images of 62 year oldmother (Table 1, parent no. 1), showing in-creasedmedullary echogenicity consistent with nephrocalcinosis. Standard probe (C) andhigh resolution (D) renal USG images of 33 year old mother (Table 1, parent no. 6) show-ing medullary nephrocalcinosis occupying the outer rim of the medulla creating a donutlike appearance involving the medullary pyramids. E. Renal USG of 33 year old mother(Table 1, parent no. 2) demonstrating echogenic medulla consistent with nephrocalcino-sis. F. Multiple echogenic foci within renal medulla of 39 year old mother (Table 1, parentno. 4). G. Increased medullary echogenicity of 30 year old mother (Table 1, parent no. 5).H. Multiple parapelvic cysts of left kidney of 44 year old father (Table 1, parent no. 16),who also had innumerable small liver cysts (see Fig. 2A).
679M. Gunay-Aygun et al. / Molecular Genetics and Metabolism 104 (2011) 677–681
Other findings, which may be purely coincidental included gallbladder polyps in 3 parents, liver hemangioma in 3 mothers and a fa-ther, left duplicated collecting system in one mother and gall stonesin one mother. The remainder of the abdominal USG examinations,including pancreas, were normal in all parents.
3.3. Case of maternal grandmother
A 76 year-old maternal grandmother was evaluated because shewas documented to have CHF on liver biopsy performed at age 75prompted by the incidental CT finding of abnormal liver parenchyma.USG imaging at NIH (Fig. 2M) showed markedly increased liver echo-genicity with moderately coarse echotexture; spleen volume wasnormal at 100 ml and kidneys were unremarkable.
3.4. Biochemical findings
Liver and kidney-related serum and urine chemistries includingserum cystatin C, PTH, and measurements of calcium and creatinine in24 hour urines were performed in 6 patients including 3 motherswith increased medullary echogenicity (Table 1, parent nos.: 1, 3 and5), 2 mothers with multiple liver cysts (Table 1, parents #10 and 11),and the maternal grandmother. All were within normal limits exceptfor elevated alanine aminotransferase (44 U/L, normal 6–41), aspartateaminotransferase (43 U/L, normal 9–34) and gamma glutamyl transfer-ase (151 U/L, normal 7–38) in the grandmother. Specifically, there wasno evidence for hypercalciuria, hyperparathyroidism, or renal tubularacidosis.
3.5. PKHD1 sequencing findings
Complete sequencing of the coding exons of PKHD1 was per-formed on 16 parents with abnormal imaging findings and the mater-nal grandmother in an effort to identify additional mutations. Thesesequences confirmed the mutation transmitted to the proband butdid not reveal any other pathogenic variants. The maternal grand-mother was heterozygous for the p.Thr36Met mutation in PKHD1.
4. Discussion
Our findings on 110 ARPKD parents and a maternal grandmothersuggest that carrier status for PKHD1 mutations creates a predisposi-tion to multiple liver cysts and renal involvement associated with in-creased medullary echogenicity on USG.
The ultrasound finding of increased medullary echogenicity is com-monly reported as “nephrocalcinosis”, a term that describes the deposi-tion of radiologically-demonstrable calcium salts in renal parenchyma[11,12]. The differential diagnosis of “nephrocalcinosis” diagnosed ra-diologically includes true histopathological nephrocalcinosis and med-ullary sponge kidney (MSK), which itself can be associated withcalcium depositions (Table 2) [11,13]. Most cases of MSK are sporadic;the presence of rare dominantly inherited forms of MSK, and its associ-ation with different malformation syndromes, suggest that MSK is aninherited developmental disorder [14–16]. The molecular basis ofMSK remains largely unknown, two sequence variants of the GDNFgene were recently reported in a fewMSK patients [14]. While intrave-nous pyelography is the gold standard for the diagnosis of MSK, com-puterized tomography has become the preferred diagnostic modality.MSK is clinically symptomatic in only a subset of patients and, therefore,is probably under-diagnosed [15]. The prevalence of MSK is estimatedat 5 in 10,000–100,000 [14,15]. Based upon our findings, we speculatethat carrier (heterozygous) status for PKHD1mutationsmay be one un-derlying molecular cause of MSK. Supporting this hypothesis, the mi-croscopic pathology of MSK resembles that of ARPKD; both arecharacterized by dilated collecting ducts, although MSK involves onlythe precalyceal collecting ducts [14,15]. Furthermore, MSK has beenreported in patients with autosomal dominant polycystic kidney dis-ease [17] and congenital hepatic fibrosis [18], most commonly causedby homozygous mutations in PKHD1. Given that the estimated carrierfrequency for PKHD1 mutations is 1 in 70 and 5% of ARPKD parentshave increased medullary echogenicity, our data suggest that the fre-quency of PKHD1-related MSK would be approximately 7 in 10,000.
Polycystic liver disease (PLD) occurs most commonly as a part ofADPKD. PLD without renal cysts, often referred to as isolated PLD, isgenetically distinct from ADPKD [19,20]. Clinical diagnostic criteriafor PLD are available only for at-risk individuals [21]; in patientsyounger than 40 years, the presence of any liver cysts is consideredto be diagnostic of PLD, while in those older than 40, 4 or morecysts are required to differentiate PLD from simple liver cysts [20].These criteria, however, need to be further vetted in a larger cohortof PCLD patients. Isolated PLD is genetically heterogeneous [19];

A
H
D E F G B C
I J K L M N
Fig. 2.MRCP and USG images of parents of patients with ARPKD showing multiple liver cysts. A. Innumerable small liver cysts ranging from a fewmm to 1 cm are visible throughoutthe liver of 44 year old father (Table 1, parent no. 16), who also had multiple parapelvic cysts of the left kidney (see Fig. 1H); his right kidney appeared normal. B. MRCP of 41 yearold mother (Table 1, parent no. 11) showing innumerable small liver cysts; the majority are less than a half cm, a few are about a cm, the largest is about 2 cm. C. Multiple liver cysts,the largest about 1.3 cm adjacent to the gallbladder, others less than a centimeter in a 42 year old father (Table 1, parent no.: 13). D. Innumerable small cysts present in both lobes ofthe liver of a 36 year old father (Table 1, parent no.: 12). E. Multiple subcentimeter cysts throughout the liver of 46 year old mother (Table 1, parent no.: 15). MRCP (F) and USGimages (G and H) of a 42 year old mother (Table 1, parent no.: 10) demonstrating multiple liver cysts, the largest measuring 3 cm. I. Multiple liver cysts on USG of 49 year old father(Table 1, parent no.: 8). J. Fourty nine year old father (Table 1, parent no.: 9) with multiple liver cysts. K. Forty five year old mother (Table 1, parent no.: 7) with multiple liver cystson USG. L. USG of a 48 year old mother (Table 1, parent no.: 14) demonstrating moderately echogenic liver with multiple cysts. M. Liver USG of the 76 year old grandmother show-ing heterogeneous appearance of the liver parenchyma with increased echogenicity in comparison to normal (N).
680 M. Gunay-Aygun et al. / Molecular Genetics and Metabolism 104 (2011) 677–681
approximately 20 to 30% of the isolated cases are due to mutations ineither PRKCSH [22] or SEC63; the molecular cause of the remainder ofisolated PLD is unknown. PRKCSH encodes the beta-subunit of gluco-sidase II, an ER glucosidase that is involved in quality control of newlysynthesized glycoproteins. SEC63 encodes Sec63, an integral ER mem-brane protein that is a part of the multi-protein translocon, the trans-location machinery for integral membrane and secreted proteins. Itwas recently shown that glucosidase IIβ and Sec63p are required inmice for adequate expression of a functional complex of the polycys-tic kidney disease gene products, polycystin-1, polycystin-2 andfibrocystin/polyductin encoded by Pkhd1 [23], [24]. This is supportedby the fact that the histopathological features of isolated PLD are verysimilar to those of the PLD in ADPKD; in both disorders cysts originatefrom biliary microhamartomas, also termed von Meyenburg's com-plexes [25,26]. However, the reason why defects in glucosidase IIβand Sec63 do not cause renal cystic disease is unknown.
Table 2Conditions associated with the radiological diagnosis of nephrocalcinosis.
Primary hyperparathyroidism (OMIM #145000 and #145001)Distal (type I) renal tubular acidosis (OMIM #179800)Medullary sponge kidneyNeonatal furosemide therapyX-linked hypophosphatemic rickets (phosphate and vitamin D) (OMIM #307800)Cystinosis (OMIM #219800)HyperphosphatasiaHypomagnesemiaIdiopathic hypercalciuriaVitamin D intoxicationHyperoxaluria (OMIM #259900)HypothyroidismCushing's syndromeProlonged immobilizationBartter's syndrome (OMIM #607364)Glycogen storage disease Type 1 (OMIM #232200)Lowe's oculocerebrorenal syndrome (OMIM #309000)Dent's disease (OMIM #300009)AcetazolamideTuberculosisSarcoidosisCarrier status for autosomal recessive polycystic kidney disease
The majority of PLD patients are clinically asymptomatic, withnormal liver enzymes and intact synthetic function [21,27]. The inci-dence of isolated PLD in autopsy series [26,28,29] (2–3 in 10,000) ishigher than its estimated clinical incidence (b1 in 10,000), suggestingthat most cases remain undetected. Our data suggest that heterozy-gous carriers of PKHD1 mutations are predisposed to PLD. In allARPKD parents with multiple liver cysts, these cysts were initiallydetected by standard probe ultrasound; in every case the number ofcysts on initial evaluation exceeded 4. Based on the estimated carrierfrequency for PKHD1 mutations of 1 in 70, and our finding that 9% ofARPKD parents have PLD, the frequency of PKHD1-related PLD wouldbe approximately 1 in 1000. Given the small size of the liver cysts andnormal liver-related blood chemistries in ARPKD parents, this condi-tion is more likely to remain undiagnosed, explaining the discrepancybetween disease frequencies.
In addition to CHF, ARPKD patients might have liver cysts that arein continuity with the biliary tree, differing form the isolated cysts inPLD. MRCP images of the ARPKD parents were not conclusive in termsof the connectivity of the cysts to biliary ducts. However, the smallsize and peripheral location of these cysts suggest that they are isolat-ed from the biliary tree, similar to the PLD cysts. This difference in thecharacteristics of liver cysts between children with ARPKD and theirparents is surprising. The increased liver echogenicity associatedwith coarse echotexture identified in some parents and the biopsyproven CHF in the maternal grandmother presented suggest somePKHD1 carriers are also prone to CHF.
To exclude the possibility that these parents had two PKHD1 mu-tations, we performed complete sequencing of the gene. However,we found no additional PKHD1 mutations in these individuals. Othergenes, including those encoding ciliary proteins, may contribute tocyst formation through synergistic heterozygosity [30,31]; this couldexplain why only a subset of PKHD1 mutation carriers develop theseliver and or kidney findings.
In summary, our data suggest that carrier status for ARPKD is apredisposition to renal involvement associated with increased med-ullary echogenicity on USG (possibly MSK), and liver involvement inthe form of asymptomatic PLD and CHF in some cases. All thesePKHD1 mutation carriers with abnormal kidney and/or liver imagingwere clinically asymptomatic.
It remains to be determined if some of these individuals might be-come symptomatic as they age.

681M. Gunay-Aygun et al. / Molecular Genetics and Metabolism 104 (2011) 677–681
Acknowledgments
We thank the ARPKD Alliance for their extensive support and thepatients and their families who generously participated in this inves-tigation. This study is supported by the Intramural Research Programsof the National Human Genome Research Institute, National CancerInstitute and the NIH Clinical Center.
References
[1] K. Zerres, S. Rudnik-Schoneborn, F. Deget, et al., Autosomal recessive polycystic kid-ney disease in 115 children: clinical presentation, course and influence of gender.Arbeitsgemeinschaft fur Padiatrische, Nephrologie, Acta Paediatr. 85 (4) (Apr 1996)437–445.
[2] L.M. Guay-Woodford, R.A. Desmond, Autosomal recessive polycystic kidney disease:the clinical experience in North America, Pediatrics 111 (5 Pt 1) (May 2003)1072–1080.
[3] M. Gunay-Aygun, E.D. Avner, R.L. Bacallao, et al., Autosomal recessive polycystickidney disease and congenital hepatic fibrosis: summary statement of a first Na-tional Institutes of Health/Office of Rare Diseases conference, J. Pediatr. 149 (2)(Aug 2006) 159–164.
[4] L.F. Onuchic, L. Furu, Y. Nagasawa, et al., PKHD1, the polycystic kidney and hepaticdisease 1 gene, encodes a novel large protein containing multiple immunoglobu-lin-like plexin-transcription-factor domains and parallel beta-helix 1 repeats, Am.J. Hum. Genet. 70 (5) (May 2002) 1305–1317.
[5] C.J. Ward, M.C. Hogan, S. Rossetti, et al., The gene mutated in autosomal recessivepolycystic kidney disease encodes a large, receptor-like protein, Nat. Genet. 30 (3)(Mar 2002) 259–269.
[6] K. Zerres, S. Rudnik-Schoneborn, C. Steinkamm, J. Becker, G. Mucher, Autosomalrecessive polycystic kidney disease, J Mol Med. 76 (5) (Apr 1998) 303–309.
[7] K. Zerres, M.C. Volpel, H. Weiss, Cystic kidneys. Genetics, pathologic anatomy,clinical picture, and prenatal diagnosis, Hum. Genet. 68 (2) (1984) 104–135.
[8] M. Gunay-Aygun, M. Tuchman, E. Font-Montgomery, L. Lukose, H. Edwards, A.Garcia, S. Ausawarat, S. Ziegler, K. Piwnica-Worms, J. Bryant, I. Bernardini, R. Fischer,M. Huizing, L. Guay-Woodford, W. Gahl, PKHD1 sequence variations in 78 childrenand adults with autosomal recessive polycystic kidney disease and congenital hepaticfibrosis, Mol. Genet. Metab. 99 (2) (Feb 2010) 160–173.
[9] M. Gunay-Aygun, E. Font-Montgomery, L. Lukose, et al., Correlation of kidney func-tion, volume and imaging findings, and PKHD1mutations in 73 patients with auto-somal recessive polycystic kidney disease, Clin. J. Am. Soc. Nephrol. 5 (6) (Jun 2010)972–984.
[10] H. Tchelepi, P.W. Ralls, R. Radin, E. Grant, Sonography of diffuse liver disease, J. Ul-trasound Med. 21 (9) (Sep 2002) 1023–1032 quiz 1033–1024.
[11] F. Manz, W. Jaschke, G. van Kaick, R. Waldherr, E. Willich, Nephrocalcinosis in radio-graphs, computed tomography, sonography and histology, Pediatr. Radiol. 9 (1)(1980) 19–26.
[12] H.A. Stout, R.H. Akin, E. Morton, Nephrocalcinosis in routine necropsies; its rela-tionship to stone formation, J. Urol. 74 (1) (Jul 1955) 8–22.
[13] B. Hoppe, M.J. Kemper, Diagnostic examination of the child with urolithiasis ornephrocalcinosis, Pediatr. Nephrol. 25 (3) (Mar 2010) 403–413.
[14] R. Torregrossa, F. Anglani, A. Fabris, et al., Identification of GDNF gene sequencevariations in patients with medullary sponge kidney disease, Clin. J. Am. Soc.Nephrol. 5 (7) (Jul 2010) 1205–1210.
[15] G. Gambaro, G.P. Feltrin, A. Lupo, L. Bonfante, A. D'Angelo, A. Antonello, Medullarysponge kidney (Lenarduzzi–Cacchi–Ricci disease): a Padua Medical School dis-covery in the 1930s, Kidney Int. 69 (4) (Feb 2006) 663–670.
[16] J.J. Kuiper, Medullary sponge kidney in three generations, N. Y. State J. Med. 71 (22)(Nov 1971) 2665–2669.
[17] V.E. Torres, S.B. Erickson, L.H. Smith, D.M. Wilson, R.R. Hattery, J.W. Segura, Theassociation of nephrolithiasis and autosomal dominant polycystic kidney disease,Am. J. Kidney Dis. 11 (4) (Apr 1988) 318–325.
[18] D.N. Kerr, C.K. Warrick, J. Hart-Mercer, A lesion resembling medullary sponge kid-ney in patients with congenital hepatic fibrosis, Clin. Radiol. 13 (Apr 1962) 85–91.
[19] P. Tahvanainen, E. Tahvanainen, H. Reijonen, L. Halme, H. Kaariainen, K. Hocker-stedt, Polycystic liver disease is genetically heterogeneous: clinical and linkagestudies in eight Finnish families, J. Hepatol. 38 (1) (Jan 2003) 39–43.
[20] Q. Qian, Isolated polycystic liver disease, Adv. Chronic Kidney Dis. 17 (2) (Mar 2010)181–189.
[21] Q. Qian, A. Li, B.F. King, et al., Clinical profile of autosomal dominant polycysticliver disease, Hepatology 37 (1) (Jan 2003) 164–171.
[22] A. Li, S. Davila, L. Furu, et al., Mutations in PRKCSH cause isolated autosomal dom-inant polycystic liver disease, Am. J. Hum. Genet. 72 (3) (Mar 2003) 691–703.
[23] S.V. Fedeles, X. Tian, A.R. Gallagher, et al., A genetic interaction network of fivegenes for human polycystic kidney and liver diseases defines polycystin-1 asthe central determinant of cyst formation, Nat. Genet. 43 (7) (2011) 639–647.
[24] J.P. Drenth, J.A. Martina, R. van de Kerkhof, J.S. Bonifacino, J.B. Jansen, Polycysticliver disease is a disorder of cotranslational protein processing, Trends Mol.Med. 11 (1) (Jan 2005) 37–42.
[25] V.J. Desmet, Congenital diseases of intrahepatic bile ducts: variations on thetheme “ductal plate malformation”, Hepatology 16 (4) (Oct 1992) 1069–1083.
[26] P.J. Karhunen, M. Tenhu, Adult polycystic liver and kidney diseases are separateentities, Clin. Genet. 30 (1) (Jul 1986) 29–37.
[27] G.T. Everson, A. Scherzinger, N. Berger-Leff, et al., Polycystic liver disease:quantitation of parenchymal and cyst volumes from computed tomographyimages and clinical correlates of hepatic cysts, Hepatology 8 (6) (Nov-Dec 1988)1627–1634.
[28] P.J. Melnick, Polycystic liver; analysis of seventy cases, AMA Arch. Pathol. 59 (2)(Feb 1955) 162–172.
[29] M. Feldman, Polycystic disease of the liver, Am. J. Gastroenterol. 29 (1) (Jan 1958)83–86.
[30] K.M. Dipple, E.R. McCabe, Phenotypes of patients with “simple” Mendelian disor-ders are complex traits: thresholds, modifiers, and systems dynamics, Am. J. Hum.Genet. 66 (6) (Jun 2000) 1729–1735.
[31] J. Vockley, P. Rinaldo, M.J. Bennett, D. Matern, G.D. Vladutiu, Synergistic heterozy-gosity: disease resulting from multiple partial defects in one or more metabolicpathways, Mol. Genet. Metab. 71 (1–2) (Sep–Oct 2000) 10–18.