Embed Size (px)
Citation preview
Sant’Anna School of Advanced Studies
PhD Thesis
Organizational Climate for BetterPerformance in Healthcare
Diana Rojas Torres
A dissertation submitted to Sant’Anna School of Advanced Studies
in partial fulfillment of the requirements for the degree ofDoctor of Philosophy in Management, Innovation, Services and
Sustainability
November 8, 2013
Pisa, Italy
Sant’Anna School of Advanced Studies
PhD Thesis
Organizational Climate for BetterPerformance in Healthcare
Candidate:
Diana Rojas Torres
Tutor:
Prof. Sabina Nuti
Supervisor:
PhD. Chiara Seghieri
November 8, 2013
Pisa, Italy
c© 2013, Diana Rojas Torres
All rights reserved.
Printed in Pisa, Italy.
Sant’Anna School of Advanced Studies, Institute of Management -
MeS.
Piazza Martiri della Liberta, 33, 56127
Pisa, Italy

Acknowledgement
Thinking about how to write this last part of the thesis, I remember when I started
my new Italian adventure three years ago. Retrospectively, I think it was one of
the experiences that have made me grow as a person, as professional and has led to
push myself to be better every day and this would not have been possible without
the help of all the people that have surrounded me from the first moment.
I feel very lucky with my supervisor Professors Sabina Nuti and Chiara Seghieri.
I am truly indebted to Professor Sabina Nuti for giving me the opportunity to
work with her, for her valuable guidance and research inputs; and with Chiara
Seghieri for her patience and guidance through the “statistics world”, she patiently
addressed my questions and doubts, and very generously shared her knowledge with
me. They continuously encouraged me to give the best.
I would like to express my sincere gratitude to MeS colleagues for their support and
collaboration, because they did the MeS Lab a pleasant place to work, in particular
I would like to thank: Anna Maria Murante, Milena Vainieri, Francesca Sanna,
Domenico Cerasuolo and Francesco Niccolai for their insights in the correct moment
and I extend my thanks to all faculty members at Stant’Anna School of Advance
Studies.
Over time, many more people made my PhD time unforgettable. I would like
to thank my partners: Lorena, Filippo, Francesco, Elisa, Maria Rosa, Francesca,
Elisabetta, Barbara, Nicola, Eleonora, Kamran, Claudia and Elena. I wish to
thank specially to Lorena, Milagros, Serena, Ilaria and Lorenzo for offered me their
friendship in the right moment.
Agradezco a mi familia, por tenerme presente todos los das sin importar que nos
separen kilmetros de distancia, a mi mami por mostrarme el camino del amor, a mi
papi por su apoyo y cercana, a la familia de Marco por su ayuda en momentos de
ii
necesidad, a mis amigas y amigos Sol, Maria, Jury, Laura, Eliana, Carolina, Alvaro,
Alonso, Drochss y David por su ayuda incondicional. Finalmente a mi hija por ser
la luz en mi camino porque este reto no hubiese sido posible sin la ayuda de ella y
a Marco por su apoyo para sacar este proyecto de vida adelante.

Contents
Organizational Climate in healthcare: An Introduction 1
1 Mapping the Organizational Climate concept with scientific cita-
tion networks 7
1.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1.2 Scientific citation networks methodology . . . . . . . . . . . . . . . 9
1.3 Organizational climate: Review of concepts . . . . . . . . . . . . . . 10
1.4 Data collection and methodology . . . . . . . . . . . . . . . . . . . 15
1.5 Citation networks in organizational climate papers . . . . . . . . . . 17
1.6 Concluding remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
2 Are there gender differences in perceived organizational climate?:
The case of Tuscan healthcare system. 24
2.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
2.2 Data and Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
2.3 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
2.4 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
2.5 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
2.A Questionnaires . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
3 Organizational climate: Comparing private and public hospitals
within professional roles 40
3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
3.2 The context . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
3.3 Data and Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
3.4 Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
3.5 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
4 Does feedback from patient-experience surveys change behavior
of health professionals and improve communication with patients?
The Italian experience 50
Contents iv
4.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
4.2 Study Data And Methods . . . . . . . . . . . . . . . . . . . . . . . 52
4.2.1 Surveys . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
4.2.2 Measures . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
4.2.3 Analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
4.3 Study Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
4.4 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
4.5 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
4.A Multilevel statistics . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
List of Tables
1.1 Most cited authors in Organizational Climate topic . . . . . . . . . 18
1.2 The longest sequence of papers on the main path . . . . . . . . . . 23
2.1 Descriptive statistics in healthcare managers and staff by gender. . 29
2.2 Gender differences of perceived organizational climate at managerial
level. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
2.3 Distribution of male/female respondents by selected questions within
dimension of communication and information processing at manage-
rial level. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
2.4 Gender differences of perceived organizational climate and profes-
sional roles at staff level. . . . . . . . . . . . . . . . . . . . . . . . . 32
2.5 Distribution of male/female respondents by selected questions about
career opportunities . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
2.6 Questionnaire A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
2.7 Questionnaire B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
3.1 Descriptive statistics within hospital status . . . . . . . . . . . . . . 45
3.2 Public Vs. Private differences at professional roles of perceived
climate and job satisfaction . . . . . . . . . . . . . . . . . . . . . . 46
4.1 Mean Patient Experience with Communication (PEC) values across
Tuscan hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
4.2 Model coefficients and variance at the patient and hospital levels . . 58
4.3 Statistics about explanatory variables introduced in the multilevel
model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
4.4 Multilevel empty model . . . . . . . . . . . . . . . . . . . . . . . . . 62
List of Figures
1.1 Calculation of SPNP . . . . . . . . . . . . . . . . . . . . . . . . . . 10
1.2 Number of publications each ten years . . . . . . . . . . . . . . . . 16
1.3 Number of publications per type of journal . . . . . . . . . . . . . . 17
1.4 Main path for organizational climate network . . . . . . . . . . . . 19
4.1 Mean Patient Experience . . . . . . . . . . . . . . . . . . . . . . . . 56
4.2 Awareness of inpatient survey data . . . . . . . . . . . . . . . . . . 59

This thesis is dedicated to the memory of my mom,
who teach me the benefits of love and be loved.
Thanks mom, I love you!
Organizational Climate in healthcare:An Introduction
“Hospitals act in an environment which is characterized not only
by limited financial resources but also by actively involved and edu-
cated health care consumers. Hospitals need to employ and coordinate
specialized knowledge, skills and abilities embedded in their employees
to deliver quality care to patients. As in other service organizations,
intangible resources are particularly relevant to provide high quality
services. It could be argued that among the most important intangible
resources in hospitals are structural knowledge, social competence,
staff motivation, and patient satisfaction. In such human-capital
intensive organizations as hospitals, the overall performance of the
organization depends on the performance of its employees based on
intelligent behavior and their motivation.”
Zigan, Macfarlane, and Desombre (2007)
This doctoral research is a compilation of four essays discussing the issue of organi-
zational climate as a tool for improving performance in healthcare. We studied four
problems in human resource management, first, is the evolution of organizational
climate concept; second, is the gender differences at managerial level; third, the
difference between private and public internal climate and last one the importance
of disseminate surveys results to improve communication between patients and
healthcare providers.
In chapter 1 we seek to analyze the literature in organizational climate topic
investigating the development of the concept and describing the evolution of the
literature during the last fifty years, understanding the central constructs and their
relationships with the existing theory , this paper suggests implications for further
research.
Organizational Climate in healthcare: An Introduction 2
Chapter 2 reveals that there are gender differences in how health workers perceived
the organizational climate considering the professional role, it was found that males
rather higher satisfaction with the work environment than females at managerial
level and at staff level women report higher satisfaction in all organizational climate
dimensions.
Chapter 3 compares the organizational climate within professional roles in private
and public institutions, employees in private hospitals are more satisfied than
employees in public ones demonstrating the hypothesis than in private institutions
are motivated by their economic well-being while in public sector the managers
are more object-oriented and they have a desire to serve the public interest and
strongly oriented towards the common good.
Chapter 4 explores the relationship between feedback and task performance with a
special emphasis on analysis of inpatient survey data that have been disclosed for
public scrutiny. In particular, this study aims to quantify the impact of professional
awareness of patient experience showing that patient experience index significantly
improved by 0.35 points (scale: 0-100) when professionals knowledge of survey
results increased by 1%.
Human resources theories developed mostly by psychologists more than sixty years
ago addressed the issue of motivation in the workplace. Maslow (1943) in his paper
”A theory of human motivation”, he organized human needs in five general levels:
a) Physiological needs (food, water, sex, shelter); b) Safety needs (protection); c)
Social needs (belonging, acceptance); d) Ego needs (status, appreciation) and e)
Self-actualization needs (need to exploit their own potential), where (a), (b) and
(c) are basic or deficit needs and (d) and (e) are follow up when deficit needs are
satisfied. (Maslow, 1943)
Herzberg et al. (1959) in his paper ”The motivation to work” divided need satis-
faction into extrinsic and intrinsic factors; extrinsic factors depend on the salary,
working conditions and job security but there is no correlation with job satisfaction.
The intrinsic factors as recognition, status and achievements are the driving force to
satisfy the worker’s needs for psychological growth and it shows a direct relationship
with job satisfaction and motivation. However, Herzberg’s work has been examined
from methodological point of view because in his analysis not is clear the difference
between job satisfaction and motivation. (Vroom, 1966; House and Wigdor, 1967)
Organizational Climate in healthcare: An Introduction 3
For a long time the concept of organizational climate was ambiguous and it was
important to recognize the difference between organizational culture and organi-
zational climate, because they focus on diverse aspects of organizational analysis.
The term organizational climate began to appear in management literature in the
1970s but at the beginning the concepts of organizational climate and culture were
commonly undifferentiated in the literature, for example Porter et al. (1975) defined
organizational climate or culture like a set of customs and typical patterns of ways
of doing things. (Porter et al., 1975)
James and Jones (1974) presented their essay about ”Organizational climate: A
review of theory and research” in this paper, they defined organizational climate
as a construct referred to the manner in which organizational members perceive
the work environment within that organization and its impact on their individual
psychological well being. In 1990 Payne treated climate as a way of measuring
culture. (James and Jones, 1974; Payne, 1991)
In a meta-analysis of 88 studies, Spector (1986) found positive results in the
organizational climate associated with high levels of perceived control, including
job satisfaction, commitment, participation, performance and motivation levels and
negative results with stress, role stress, absenteeism, intention to leave a job, and
the turnover. (Spector, 1986)
Employee satisfaction has a direct, positive impact on functioning of whole organi-
zation. It strongly affects the institution’s global performance and it is often the key
element that makes the difference (Schneider, 1987; Nuti and Macchia, 2005; Dawson
et al., 2008; Judge et al., 2001). Several literature shows a strong association among
high performance, customer satisfaction and organizational climate and positive
correlation between climate and rewards. Goleman affirmed that ”Organizational
climate is not the only driver of performance. Economic conditions and competitive
dynamics matter enormously. But our analysis suggests that climate accounts for
nearly a third of the results”. (Goleman, 2000)
Several studies have outlined the importance of organizational climate in the
healthcare context, see e.g. (Appelbaum, 1984; Clarke et al., 2002; Gershon et al.,
2004; Jackson-Malik, 2005; Mok and Au-Yeung, 2002; Sleutel, 2000; Stone et al., 2006;
Wienand et al., 2007a). Among organizational factors related to climate, continuing
training and education (Spath, 2002), leadership style, project management, staff

Organizational Climate in healthcare: An Introduction 4
recognition, dedicated time and resources for improvement projects (Thomson et al.,
2002) all have been identified as important factors for health care staff’s commitment
and loyalty toward the organization.
Recently, a renewed interest about the importance of intangible resource in de-
termining organizational performances has increased, in particular some authors
have discussed their relevance as drivers of outstanding performances in hospi-
tals (Douglas and Ryman, 2003; Habersam and Piber, 2003; Zigan et al., 2007).
Meanwhile, other authors are specifically addressed the organizational climate as
predictor of good performance (Brown and Leigh, 1996; Patterson et al., 2005),
it is particular valuable for healthcare services where organizational climate is
therefore, a multidimensional distinctive feature of organization, which results from
a synergic combination of several intangible elements related to human, relational
and structural dimensions of the organization. (Carlucci et al., 2009)
Healthcare organizations are usually considered complex institutions and they have
a particular structure due to the diversity of organizational forms, hospital status,
hospital size and wards that are evolving, this parameters also render difficult their
managerial control.
Clarke et al. (2002) found that staffing and organizational climate influence hospital
nurses’ likelihood of sustaining needlestick injuries, (Clarke et al., 2002). Stone et al.
(2006) found that negative perceptions of organizational climate predicted nurses’
intention to leave within intensive care units (Stone et al., 2006). Dimensions of
organizational climate seem also depending on the particular characteristics of the
work environment (Tovey and Adams, 1999). Cumbey and Alexander (1998), for
instance, found that organizational structure was a crucial determining variable in
predicting job satisfaction among nurses, (Cumbey and Alexander, 1998). Moreover,
some important differences between teaching and community hospitals have been
found for different groups of nurses: nurses working in teaching hospitals reported
lower levels of role tension, and higher levels of job stress and job satisfaction than
their colleagues in the community sites (Hall et al., 2006)
Organizational Climate in healthcare: An Introduction 5
Research Context
The Italian health care system is a National Health Service (Beveridge-like model)
accessible to the full population providing preventive and curative services. The
system is organized at three levels: national, regional and local. The national level
is responsible for ensuring the general objectives and fundamental principles of the
National Health Service. The regional governments are responsible for ensuring
the delivery of the health care through a network of population-based healthcare
organizations (health authorities).
The strong policy of decentralization, which has been taking place since the early
1990s, has gradually transferred several important administrative and organizational
responsibilities from the state to the 21 Italian regions with the aim of making
regions more sensitive to the need to control expenditure and promote efficiency,
quality, and citizen satisfaction.
This devolution process provided regions with significant autonomy in organizing
healthcare services, allocating financial resources to their Local Health Authorities
(LHAs), and in monitoring and in assessing performance (Nuti, 2008; Antonini
and Pin, 2009). Whereas, the central government retains overall responsibility for
ensuring that services, care and assistance are equitably distributed to citizens
across the country.
Since the 1980s the introduction of ”New Public Management” (NPM) (Kettl,
2000; Pollitt, 1995) principles has promoted a number of reforms in public services
organizations in order to improve the performance in the public sector but especially
have started to focus on customer satisfaction and more effective management
(Mouritsen et al., 2005).
The Tuscany region has approximately 3,7 million inhabitants in an area of 22,994
km2 in the center of Italy. It’s healthcare system currently counts about 51,000
employees, including nurses, physicians, technicians and administrative staff, for
a total public expenditure of 6,6 billion Euros. The regional government works
through a network of seventeen public health authorities of which five are teaching
hospitals (THs), integrated with the Universities of Florence, Pisa and Siena (among
them, one is a paediatric hospital and another is a highly specialized hospital on

Organizational Climate in healthcare: An Introduction 6
cardiovascular diseases) and twelve are Local Health Authorities (LHAs). In 2000
the Tuscany region began a process of reorganization of the system that allow them
to work in three operating structures called ”Area Vasta” (AV). Each AV includes a
network of these LHAs grouped by geographic proximity. /citepnuti2013variation.
Since 2004 the Laboratory MeS on behalf of Tuscany region created the ”Multi-
dimensional Performance Evaluation System in healthcare. The system consists
of 50 composite and more than 130 simple indicators. Indicators are classified in
the following six dimensions: population health status; capacity to pursue regional
strategies (i.e. to guarantee that strategic regional goals are pursued in the indicated
time and manner); clinical performance (i.e. quality, appropriateness, effectiveness,
clinical risk management and primary care); patient satisfaction; organizational
climate and finally efficiency and financial performance”. (Nuti et al., 2013).
1
Mapping the Organizational Climateconcept with scientific citation
networks 1
In this research we present the results of an earlier pilot study about citation
networks applied to organizational climate topic. We use citation networks to
study the dynamics of the organizational climate concept in scientific papers
from 1983 to 2012. We identify the most significant papers, then we analyze
the structure of the top path of citation networks to understand the main
scientific trajectory in this field. Our results suggest that these scientific
trajectories are characterized by the presence of a number of papers analyzing
the definition and difference between organizational culture and climate.
1.1 Introduction
This research has the purpose to understand the evolution of organizational climate
concept until 2013. The term ”organizational climate” began to appear in man-
agement literature in the decade of 70’s and the first interpretations confounded
the expression with the definition of ”organizational culture” making the two terms
almost interchangeable (Porter et al., 1975). We focus on studying the development
of this topic in the literature and point out the most representative authors in this
field.
1Acknowledgements:The author wish to thank to David Barbera and Alessandro Nuvolari tomotivate this work.

Introduction 8
We can see an extensive literature about the importance of motivation at work
in human resource management (Maslow, 1943; Herzberg et al., 1959; James and
James, 1989; Glick, 1985); this literature suggest that satisfied employees tend to
be more productive, creative and enthusiastic to their employers. In particular,
it has been pointed out that proper organizational climate has a direct, positive
impact on functioning of the team and is correlated with the performance in the
organization (Spector, 1986).
Organizational climate was defined in 1968 by Tagiuri as a ”quality of the internal
environment of an organization that: (a) is experienced by its members, (b) influ-
ences their behaviour and (c) can be described in terms of the values of a particular
set of characteristics (or attributes) of the organization” (Tagiuri R, 1968). From
a human resources management, this definition present several points of interest.
First, the importance of organizational culture and climate in the organization
because it has been shown that there is an important relationship between them and
organizational performance outcomes (Schneider et al., 2002). Second, the concept
is ambiguously defined and it is important to recognize the difference between
organizational culture and organizational climate. Third, few studies examine the
importance of the climate in healthcare sector and additional research is needed to
understand this complex organizations.
Citation to scientific articles analysis (citation networks) is applied to estimate the
importance of a scientific publication as the number of times that which has been
cited by other authors (Vieira and Gomes, 2010). Our premise is that citation to
scientific articles analysis is a good indicator of prior knowledge that have a positive
impact on the scientific community.
Our discussion relies on the study of an exploratory analysis of citations links among
scientific papers in organizational climate context within Thomson Reuters (Web
of Science, WoS) database. Therefore, we can identify the main paths through
examination of the citation network structure, which concept has been developed
over time.
We adopt the methodology follows by Hummon and Dereian (1989), who have
suggested certain criteria for the identification of the main paths of ”connectivity”
in a network. This methodology is applied to several studies about citation networks
and patent citation networks that used citations to obtain a sequence of patents
Scientific citation networks methodology 9
to follow the technological evolution (Dosi, 1982) in a particular field (Verspagen,
2007; Fontana et al., 2009; Barbera-Tomas et al., 2011).
The structure of the paper is as follows. Section 1.2 illustrates the scientific
citation network methodology. In Section 1.3 we provide a review of concepts in
organizational climate. In Section 1.4 we describe the construction of our citation
analysis data-set and gives a preliminary descriptive analysis of its main properties.
In Section 1.5 we present a short insights of the evolution of the organizational
climate concept using citation networks. In Section 1.6 we conclude the study.
1.2 Scientific citation networks methodology
This research proposed a citation network as a collection of vertices and edges where
the network vertices are papers and a directed edge are connections from paper A to
paper B if A cites B in its bibliography. The analysis of the connectivity structure
allows to identify a set of scientific papers which constitutes the main flow of ideas
in a field of knowledge and link the thematic connections with important scientific
papers. We will consider direct edges, the direction will be from the cited to citing
article, it means from the earlier article to the later one.
We will follow the approach proposed by Hummon and Doreian (Hummon and
Dereian, 1989), they are interested in identifying the main paths of the network.
These main paths are the main flows of ideas in the structure of the network. They
assigned a weight to each citation link based on the position of this structure. In
Figure 1.1 (adapted from (Fontana et al., 2009)), paper A is cited by paper C, which
is cited by paper D. A search path is represented by the sequence A-C-D-F-H-J,
indicating knowledge flow from paper A to paper J through some intermediate
papers.
A complementary connectivity measure proposed by Hummon and Doreian is the
SPNP (Search Path Node Pair). Consider the edge C-D (fig 1). This edge connects
three vertices (A, B, C) to the final stop (D). At the same time, this edge connects
its origin (C) to seven other vertices (D, E, F, G, H, I and J). The SPNP value is
the product of these values (3×7 = 21).
Organizational climate: Review of concepts 10
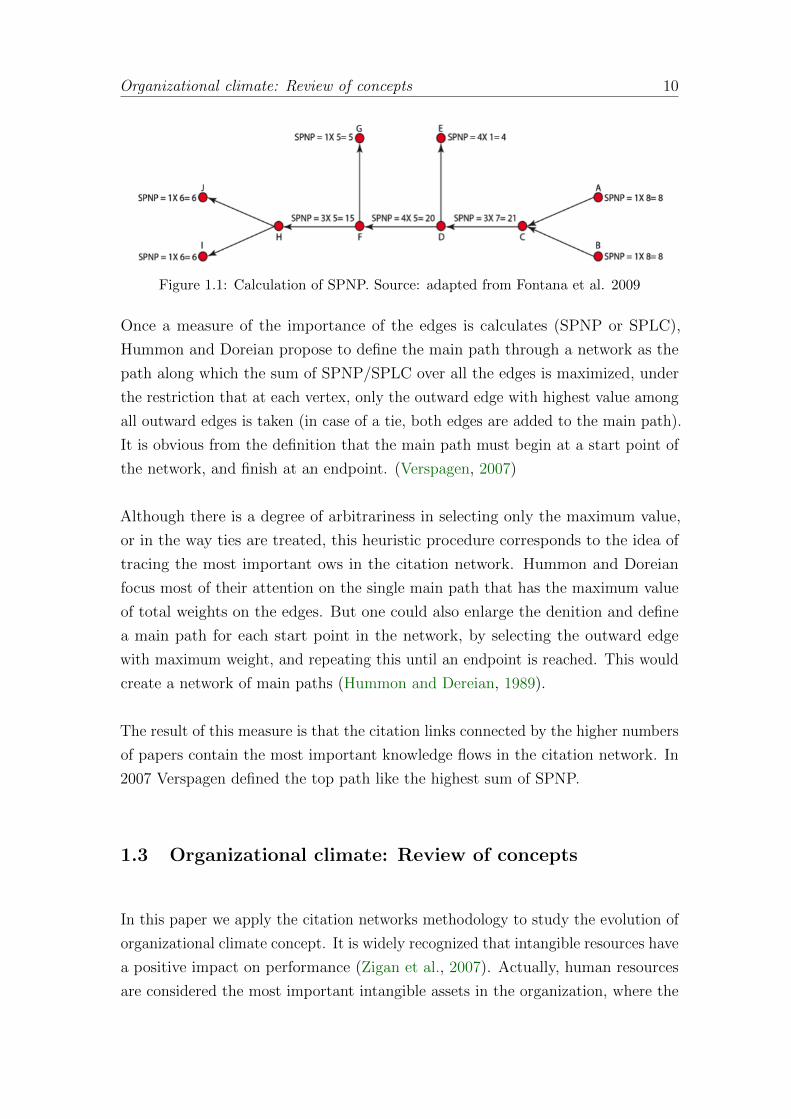
Figure 1.1: Calculation of SPNP. Source: adapted from Fontana et al. 2009
Once a measure of the importance of the edges is calculates (SPNP or SPLC),
Hummon and Doreian propose to define the main path through a network as the
path along which the sum of SPNP/SPLC over all the edges is maximized, under
the restriction that at each vertex, only the outward edge with highest value among
all outward edges is taken (in case of a tie, both edges are added to the main path).
It is obvious from the definition that the main path must begin at a start point of
the network, and finish at an endpoint. (Verspagen, 2007)
Although there is a degree of arbitrariness in selecting only the maximum value,
or in the way ties are treated, this heuristic procedure corresponds to the idea of
tracing the most important ows in the citation network. Hummon and Doreian
focus most of their attention on the single main path that has the maximum value
of total weights on the edges. But one could also enlarge the denition and define
a main path for each start point in the network, by selecting the outward edge
with maximum weight, and repeating this until an endpoint is reached. This would
create a network of main paths (Hummon and Dereian, 1989).
The result of this measure is that the citation links connected by the higher numbers
of papers contain the most important knowledge flows in the citation network. In
2007 Verspagen defined the top path like the highest sum of SPNP.
1.3 Organizational climate: Review of concepts
In this paper we apply the citation networks methodology to study the evolution of
organizational climate concept. It is widely recognized that intangible resources have
a positive impact on performance (Zigan et al., 2007). Actually, human resources
are considered the most important intangible assets in the organization, where the
Organizational climate: Review of concepts 11
organizational culture and climate constitutes the main organizations advantage
and permit differentiate between organizations within a society, particularly in
relation to different levels of effectiveness. (Schein, 1990)
Human resources theories highlight the importance of motivating employees in the
workplace and suggest that satisfied employees are more productive, innovative
and efficient (Maslow, 1943). The theory of motivation was the first attempt to
conceptualize the organizational climate theories.
Organizational climate theory is widely studied in industrial and organizational
psychology. Koffka (1935) studied the behavior environment, Murray (1938) ana-
lyzed the personality problems on a level of depth and concreteness usually found
only in the work of the psychiatrist or psychoanalyst. Lewin et al. (1939) analyzed
the relationship between leadership style and climate. However, in the beginning
the conceptual definition of organizational climate and measurement techniques
were inconsistent.
It was not until 1958 when the term organizational climate began to appear in
management literature with an study made by Argyris (1958) about Some problems
in conceptualizing organizational climate: A case study of a bank, this study
affirmed that organization is composed of elements representing many different
levels of analysis; the climate (or homeostatic state) and leadership represent the
personality level of analysis, norms and values represent the cultural level, employee
satisfaction or dissatisfaction are the interaction of multilevel variables and the
clusters of these variables are namely organizational behavior. (Argyris, 1958)
Forehand and Von Haller (1964) reviewed the organizational climate literature found
in psychology, sociology, administration and education studies until 1964 and they
worked on the problem of variation in the conceptualization of climate term. They
found that organizational climate term means different things to different writers
and they concluded that organizational climate refers to the set of characteristics
that describe an organization and that (a) distinguish the organization from other
organizations, (b) are relatively enduring over time, and (c) influence the behavior
of people in the organization. (Forehand and Von Haller, 1964)
In 1968 an early definition of organizational climate is made by Tagiuri R (1968)
which defines organizational climate as a ”quality of the internal environment of an
Organizational climate: Review of concepts 12
organization that (a) is experienced by its members, (b) influences their behavior
and (c) can be described in terms of the values of a particular set of characteristics
(or attributes) of the organization”. (Tagiuri R, 1968)
Pritchard and Karasick (1973) explored the validity of a measure of climate construct
and they presented data on the relationship between climate, job performance
and satisfaction. They concluded that satisfaction relates positively with climate
perceptions and job satisfaction (Pritchard and Karasick, 1973). However, Guion
(1973) conclude that organizational climate represent a fuzzy concept and reinforced
the idea that climate measurement often used the same instruments and techniques
apply to job satisfaction research.
James and Jones (1974) published their work about organizational climate: A
review of theory and research, where they defined organizational climate as a
construct referred to the manner in which organizational members perceive the work
environment within that organization and its impact on their individual psychological
well being. They recommended make a differentiation between climate regarded
to organizational attribute (organizational climate) and climate regarded to an
individual attribute (psychological climate). (James and Jones, 1974)
Schneider (1975) proposed an essay about organizational climate. He presents an
evidence regarding the importance of climate, which refers to the perception of the
people about their work settings, each work organization probably creates different
kinds of climates and is related to the outcome behavior (dimension) and the unit
of analysis (professional role, organization). An important conclusion in this work is
the different conceptualization between organizational climate and job satisfaction
(Schneider, 1975). In previous studies of climate research Litwin and Stringer Jr
(1968) found that different kinds of climate could directly influence levels of job
satisfaction, this result allowed some authors to propose that the two concepts were
the same. (Litwin and Stringer Jr, 1968)
At this point, it is important to discuss the concepts of organizational culture and
organizational climate due to the lack of clarity among themselves. For example,
Porter et al. (1975) defined organizational climate or culture as a set of customs and
typical patterns of ways of doing things. However, the organizational culture and
climate focus in two different aspects of organizational studies.(Porter et al., 1975)

Organizational climate: Review of concepts 13
Burke and Litwin (1992) defined climate as perceptions about the workplace of
organizational members and culture is defined by beliefs and values within the
organization, but where the two concepts are interrelated, it means climate is
affected by culture and it is view as reciprocal processes. (Burke and Litwin, 1992)
The term culture began to appear in management literature in the 1970s. Culture
can be conceived as a set of attitudes, values and beliefs that guide organizational
behavior but what really distinguishes culture is what the attitudes, values and
beliefs are about (Brown and Payne, 1990). The broad conclusion has been that
organizational culture develops through social learning mechanisms. (Schein, 1985;
Kilmann et al., 1985; Hofstede et al., 1991) Culture is the way that things are
done and no reference to participants is made. (Schein, 1985) pointed out that
organizational culture is a complex phenomenon and he defined Culture as (a)
a pattern of basic assumptions, (b) invented, discovered, or developed by a given
group, (c) as it learns to cope with its problems of external adaptation and internal
integration, (d) that has worked well enough to be considered valid and, therefore
(e) is to be taught to new members as the (f) correct way to perceive, think,
and feel in relation to those problems. Finally, the actions and behaviors that are
associated with favorable outcomes tend to be repeated, and become norms in the
organizational structure. (Gray, 2004)
The distinction between climate and culture derives from the fact that the two
concepts reinforce each other. According to Kangis et al. (2000) whilst the con-
structs of culture and climate have developed in parallel, they have been driven
by researchers from different disciplines using different methodologies. There has
been little cross-fertilization of methods and ideas and considerable debate among
researchers about the relatedness of the two constructs. (Kangis et al., 2000)
In fact, between the two fields of study still exist a divergence . First, psychological
constructs, particularly those constructs related to group behavior are highlights in
culture studies. But some researchers on organizational climate have also tended
towards a group. Lawthom et al. (1995), after reviewing a number of definitions,
came to the conclusion that a precise and unitary definition of climate is yet to be
found but is possible to distinguish climate as a concept. First, refers to individual
perceptions. Second, it is descriptive rather than evaluative in its orientation. At
the end the definition that fit for climate purposes is what it feels like to work here.
(Lawthom et al., 1995)
Organizational climate: Review of concepts 14
Svyantek and Bott (2004) proposed the definitions which help distinguish between
climate and culture. Organizational culture is defined as a set of shared values and
norms held by employees that guide their interactions with peers, management, and
clients. Organizational climate is more behaviorally oriented in that climates for
creativity, innovation, safety, or service, for example, may be found in the workplace.
These climates represent employees perceptions of organizational policies, practices,
and procedures, and subsequent patterns of interaction and behaviors that support
creativity, innovation, safety, or service in the organization. (Svyantek and Bott,
2004)
Researchers in this field have outline the importance of measuring climate and
the typical measure of organizational climate is through questionnaires; asking
individuals whether they are agree or disagree with a series of statements designed
to capture the perceptions about the organization. (Payne, 1991) In the literature
there are a huge number of instruments proposed to measure it, some authors
identify different climate dimensions like psychological leadership (Glick, 1985);
managerial attitudes (Payne and Mansfield, 1978); communication flow (Drexler,
1977); service quality (Schneider, 1980); equity and centrality (James, 1982; Joyce
and Slocum, 1979).
Some authors have proposed that organizational climate is associated with impor-
tant outcomes at diverse levels (individual, groups and organization). There is a
positive correlation between climate and turnover intentions (Rentsch, 1990), job
satisfaction (Mathieu et al., 1993; James and Tetrick, 1986; James and Jones, 1980),
individual job performance (Brown and Leigh, 1996): (Pritchard and Karasick,
1973), organizational performance (Lawler III et al., 1974; Patterson et al., 2004),
and innovation. (Patterson et al., 2005)
In healthcare context several studies have outline the importance of organizational
climate, there is an increasing interest in study the relationship between organiza-
tional constructs and health services outcomes (Clarke et al., 2002; Jackson-Malik,
2005; Mok and Au-Yeung, 2002; Sleutel, 2000; Stone et al., 2006; Wienand et al.,
2007b; Carlucci et al., 2009; Gershon et al., 2004; Appelbaum, 1984)
Regarding to healthcare services, there is a growing need to understand the employees
perceptions and climate generated by their healthcare organization because there is
a positive correlation between climate, high quality service and patient satisfaction.

Data collection and methodology 15
(Sleutel, 2000; Stone et al., 2006)
Clarke et al. (2002) found that staffing and organizational climate influence hospital
nurses’ likelihood of sustaining needlestick injuries. Stone et al. (2006)analyzed
the relationship between organizational climate and intensive care unit nurses’
intention to leave and demonstrated that a satisfactory organizational climate
ensure a stable and qualified workforce. Sleutel (2000) provides a literature review
about organizational factors that influence nursing practice, included organizational
climate. Mok and Au-Yeung (2002) explored the relationship between organizational
climate and empowerment among the nursing staff of a regional hospital in Hong
Kong. The results of their investigation show that organizational climate and
supportive leadership and teamwork are related to empowerment. (Clarke et al.,
2002; Stone et al., 2006; Sleutel, 2000; Mok and Au-Yeung, 2002)
1.4 Data collection and methodology
We propose an earlier pilot study about citation network applied to organizational
climate studies to understand the actual state of the art of this field. We search on
Thomson Reuters (Web of Science, WoS) database all articles about organizational
climate from 1985 to 2013. We restrict the search of the term in the title and refine
results for articles within web of science categories to management, psychology, busi-
ness, educational research, nursing, public administration and healthcare sciences.
We built our database using organizational climate as keyword on the title and we
found 252 articles published between 1985 - 2013 in journals indexed in the Web
of Science (WoS) and classied according to the Essential Science Indicators (ESI)
(Thomson Reuters, 2009a). The ESI is a compilation of statistical information
related with publications, citations and cites per paper for journals, scientists,
institutions and countries referring to 10 years of Thomson Reuters data.
We have information about authors, institutional addresses, number of pages,
journals and citing articles for each document classied as an article. We searched
citations among these 252 papers. Our final database includes 252 papers and 7904
citations (for methodological reasons we decided to take into account only papers
identified by DOI). For the citation network analysis we used pajek software; it is
a free software for noncommercial use. It is a common program used for drawing
Data collection and methodology 16
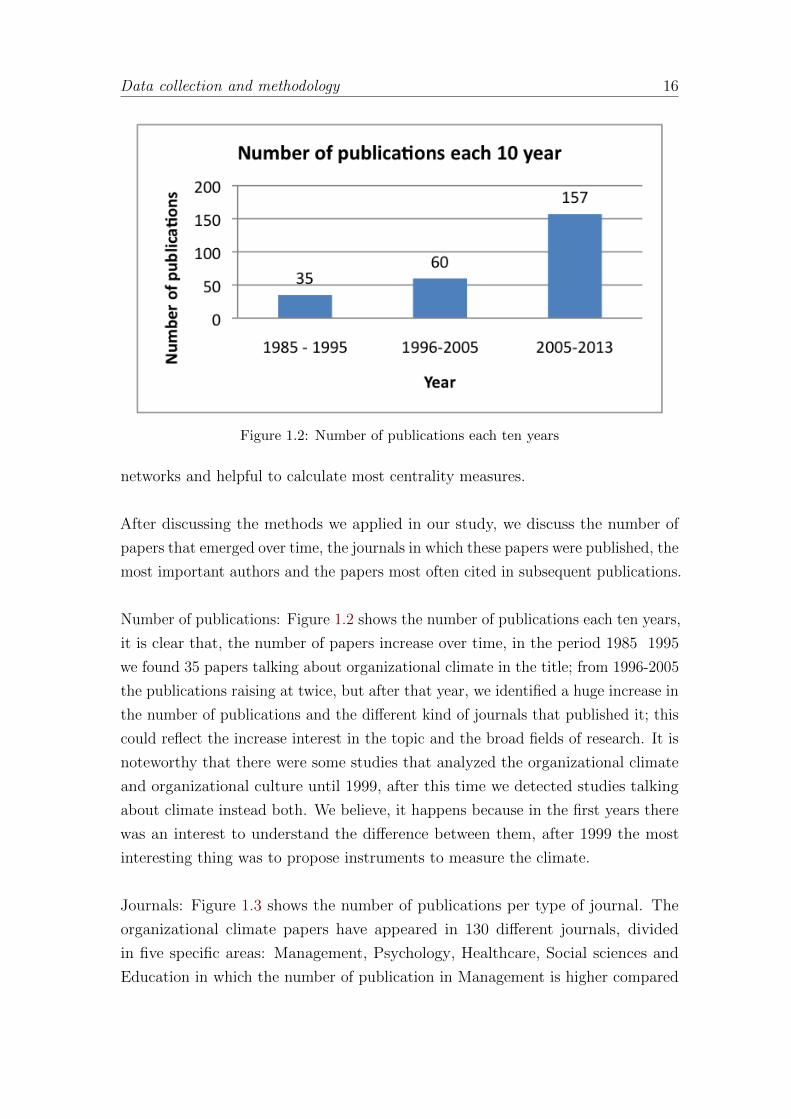
Figure 1.2: Number of publications each ten years
networks and helpful to calculate most centrality measures.
After discussing the methods we applied in our study, we discuss the number of
papers that emerged over time, the journals in which these papers were published, the
most important authors and the papers most often cited in subsequent publications.
Number of publications: Figure 1.2 shows the number of publications each ten years,
it is clear that, the number of papers increase over time, in the period 1985 1995
we found 35 papers talking about organizational climate in the title; from 1996-2005
the publications raising at twice, but after that year, we identified a huge increase in
the number of publications and the different kind of journals that published it; this
could reflect the increase interest in the topic and the broad fields of research. It is
noteworthy that there were some studies that analyzed the organizational climate
and organizational culture until 1999, after this time we detected studies talking
about climate instead both. We believe, it happens because in the first years there
was an interest to understand the difference between them, after 1999 the most
interesting thing was to propose instruments to measure the climate.
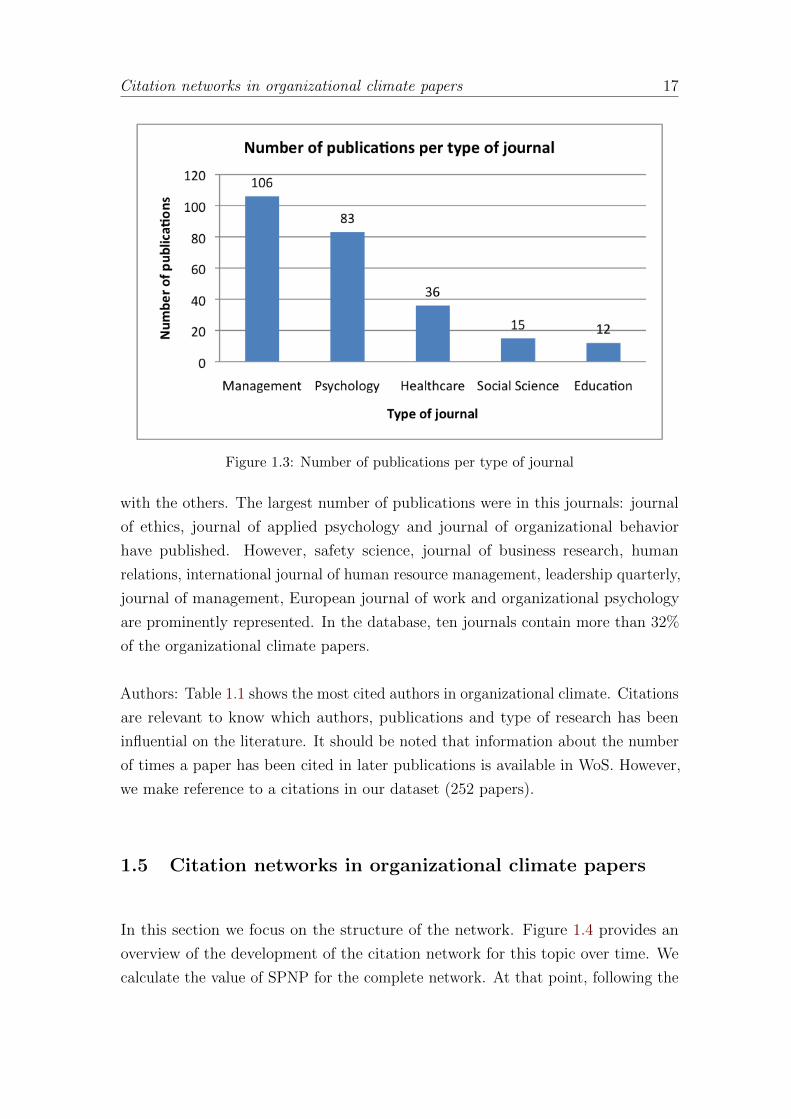
Journals: Figure 1.3 shows the number of publications per type of journal. The
organizational climate papers have appeared in 130 different journals, divided
in five specific areas: Management, Psychology, Healthcare, Social sciences and
Education in which the number of publication in Management is higher compared
Citation networks in organizational climate papers 17
Figure 1.3: Number of publications per type of journal
with the others. The largest number of publications were in this journals: journal
of ethics, journal of applied psychology and journal of organizational behavior
have published. However, safety science, journal of business research, human
relations, international journal of human resource management, leadership quarterly,
journal of management, European journal of work and organizational psychology
are prominently represented. In the database, ten journals contain more than 32%
of the organizational climate papers.
Authors: Table 1.1 shows the most cited authors in organizational climate. Citations
are relevant to know which authors, publications and type of research has been
influential on the literature. It should be noted that information about the number
of times a paper has been cited in later publications is available in WoS. However,
we make reference to a citations in our dataset (252 papers).
1.5 Citation networks in organizational climate papers
In this section we focus on the structure of the network. Figure 1.4 provides an
overview of the development of the citation network for this topic over time. We
calculate the value of SPNP for the complete network. At that point, following the
Citation networks in organizational climate papers 18
Table 1.1: Most cited authors in Organizational Climate topic
Reference Number of citations
Schneider B 430
James LR 230
Glisson CA 121
Rousseau DM 115
Schein EH 91
Hoffman DA 80
Reichers AE 71
Ostroff C 70
Podsakoff PM 69
Payne R 68
Meyer JP 64
Hofstede G 60
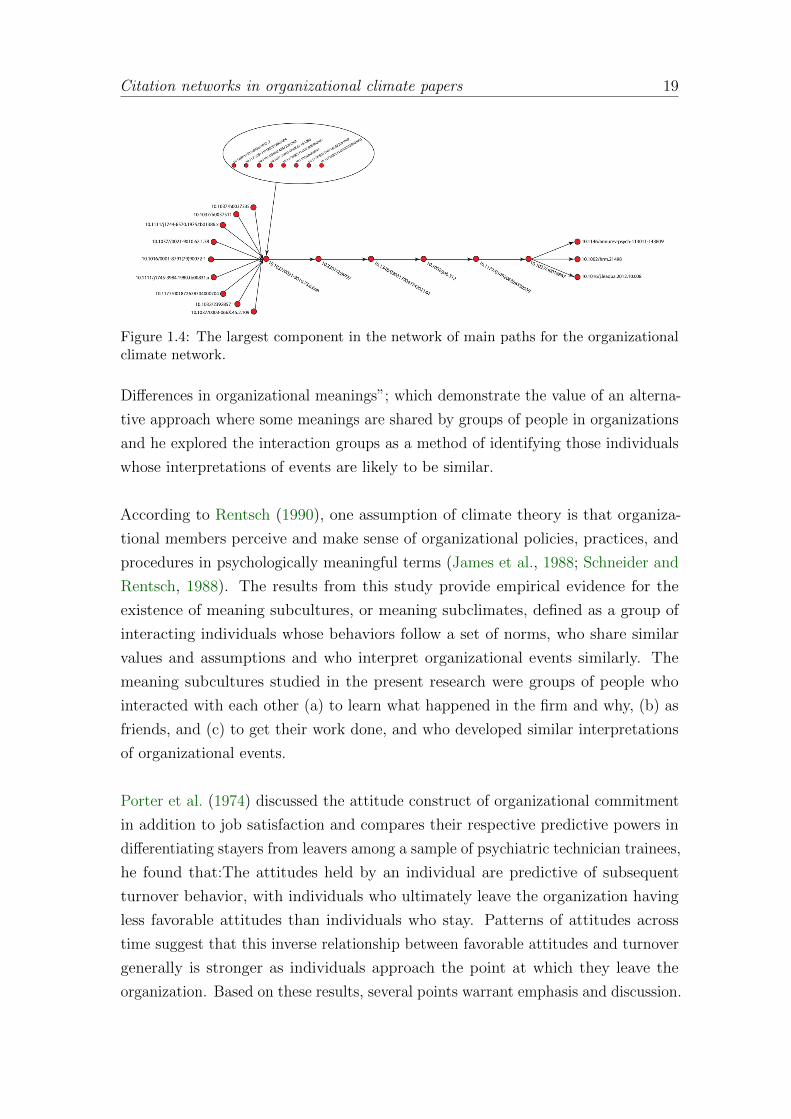
methodology proposed by Hummon and Dereian (1989), we built the network of
main paths as we explained in Section 1.2. Figure 1.4 shows the largest component
of this network of main paths. This network is characterized by a sequence of most
important articles cited in this topic and it were organized in chronological way.
In the bottom left part of the graph we identify a cluster composed by important
articles about school climate; it was possible to identify that there are several
literature, some of it empirical, that has dealt with understanding the construct of
school climate; this papers consider the development and current status of school cli-
mate research, major instruments and important findings; given that school climate
is a particular construct composed by two research fields; organizational climate
research and school effects research, school climate research can be distinguished as
a separate area of study (Anderson, 1982). We concluded that it was not consistent
with our research objectives and we decided to exclude it from our analysis.
The organizational climate citation network has only one component, which demon-
strates the accuracy and consistency of our keyword search. Citation network
analysis selects 18 papers to form the top path. The top path represented in Figure
1.4 shows the fundamental flow of knowledge in organizational climate field (science
trajectory) in the complete citation network. These articles are listed in more detail
in Table 1.2.
Paper (No. 10.1037/0021-9010.75.6.668) lies on the origin of the trajectory. This is
the paper by Rentsch (1990) ”Climate and Culture: Interaction and Qualitative
Citation networks in organizational climate papers 19
Figure 1.4: The largest component in the network of main paths for the organizationalclimate network.
Differences in organizational meanings”; which demonstrate the value of an alterna-
tive approach where some meanings are shared by groups of people in organizations
and he explored the interaction groups as a method of identifying those individuals
whose interpretations of events are likely to be similar.
According to Rentsch (1990), one assumption of climate theory is that organiza-
tional members perceive and make sense of organizational policies, practices, and
procedures in psychologically meaningful terms (James et al., 1988; Schneider and
Rentsch, 1988). The results from this study provide empirical evidence for the
existence of meaning subcultures, or meaning subclimates, defined as a group of
interacting individuals whose behaviors follow a set of norms, who share similar
values and assumptions and who interpret organizational events similarly. The
meaning subcultures studied in the present research were groups of people who
interacted with each other (a) to learn what happened in the firm and why, (b) as
friends, and (c) to get their work done, and who developed similar interpretations
of organizational events.
Porter et al. (1974) discussed the attitude construct of organizational commitment
in addition to job satisfaction and compares their respective predictive powers in
differentiating stayers from leavers among a sample of psychiatric technician trainees,
he found that:The attitudes held by an individual are predictive of subsequent
turnover behavior, with individuals who ultimately leave the organization having
less favorable attitudes than individuals who stay. Patterns of attitudes across
time suggest that this inverse relationship between favorable attitudes and turnover
generally is stronger as individuals approach the point at which they leave the
organization. Based on these results, several points warrant emphasis and discussion.

Citation networks in organizational climate papers 20
He affirmed that some attitudes and turnover can be explain by comparing the level
of expectations of employees with the perceived realities of the job environment.
James and Jones (1974) defined organizational climate like a organizational at-
tributes, main effects, or stimuli within the organization. As a first step in recon-
ceptualization, it is recommended that a differentiation be made between climate
regarded as an organizational attribute and climate regarded as an individual
attribute. When regarded as an organizational attribute, the term organizational
climate appears appropriate. When regarded as an individual attribute, it is
recommended that a new designation such as psychological climate be employed.
Schneider (1975) also summarized some ideas which suggests that climate research
has been concerned with a description of the forms or styles of behavior in orga-
nizations. He defined climate perceptions are psychologically meaningful molar
descriptions that people can agree characterize a systems practices and procedures.
By its practices and procedures a system may create many climates. People perceive
climates because the molar perceptions function as frames of reference for the attain-
ment of some congruity between behavior and the systems practices and procedures.
However, If the climate is one which rewards and supports the display of individual
differences people in the same system will not be have similarly. Further, because
satisfaction is a personal evaluation of a systems practices and procedures, people
in the system will tend to agree less on their satisfaction than on their descriptions
of the systems climate.
An important insight about Schneiders work is the difference between organizational
climate and job satisfaction, he proposed independent analysis and definitions for
the two constructs, he studied climate, as a perception of the external world, while
job satisfaction is defined as the study of mans internal affective state. Both clearly
fall in the domain of research called ’attitude research’, but is necessary to maintain
clear differentiation between affect and organizational description respect to the
units of analysis.
Drexler (1977) studied differences in climate among different organizations; differ-
ences in climate across different organizations using groups that serve the same
functions; differences in climate among departments within the same organization
and differences in the relative strengths of organization effects and department ef-
fects. With this study he concluded that organizational climate is an organizational

Citation networks in organizational climate papers 21
attribute, where there are differences in organizational climate across departments
in the same organization but the effect of the department is weaker compared
with organizational effects. This work is interesting because gives the idea that is
possible analyzed climate at different levels (leadership, group, or department) vs.
organizational structure.
Mowday et al. (1979) summarizes research aimed to developing and validating
a measure of employee commitment to work organizations. In this paper, they
defined commitment as a global construct, including its goals, values and is stable
over time, while job satisfaction reflects ones response either to ones job or to
certain aspects of ones job. Satisfaction, has been found to be a less stable
measure over time, reflecting more immediate reactions to specific and tangible
aspects of the work environment. This work pointed out the need to incorporate
commitment as a predictor of behavior and proposed an organizational commitment
as construct relates to employee behavior in work organizations. Nevertheless,
organizational commitment makes no reference to the issue of organizational climate
but it relates to the instrument called Organizational Commitment Questionnaire
(OCQ), answer this questions contribute to a broader understanding of the role of
employee attitudes determining employee behavior and organizational performance.
Furthermore, DeCotiis and Summers (1987) defined organizational commitment as
one dimension of organizational climate refers to avoidance and behavior.
According to Schein (1990), culture is a learned product of group experience and
is, therefore, to be found only where there is a definable group with a significant
history. For Schein, the organizations evolve from small groups. However, organi-
zations develop dynamics that go beyond those of the small group so small group
observations must be extrapolated to larger organizations”.
In the 1990s Schein (1990); Rentsch (1990); Denison (1996) wrote several papers for
address the difference between organizational climate and organizational culture.
The term organizational climate began to appear in management literature and it
was often used almost interchangeably with culture. (Denison, 1996) suggests that
a kind of reversal in the terminology took place so that studies which talked about
climate in the 1970s would be thought of as addressing culture by the late 80s. Its
important to distinguish between the two concepts because, although related, they
focus on quite distinct aspects of organizational life and, crucially, managers can
have more influence on climate than they can on culture.

Concluding remarks 22
1.6 Concluding remarks
This paper has analyzed the pattern of scientific change in organizational climate
issue by citation networks. It was possible to use a SPNP proposed by Hummon
and Dereian (1989) to identify the top path and the important characteristics in
the evolution of the concept.
In the case of organizational climate construct, our propose produce fruitful insights.
The top path showed a coherent evolution. Our research present that the concept is
divided by periods, where the first period try to conceptualized the organizational
climate term, the second period study the instruments to measure both, organi-
zational climate and organizational commitment; third, focus on the difference
between organizational culture and climate
With systematic reviews about organizational climate topic other researchers had
already identified the most important articles in this field and that we showed in the
main path. Thus our citation network employing empirical techniques is completely
consistent with the analysis of other researchers.

Concluding remarks 23
Table 1.2: The longest sequence of papers on the main path
DOI P. Year Authors Article Title
10.1037/h0037335 1974 Porter, Lyman;Steers, Richard;Mowday, Richard;Boulian, Paul
Organizational commitment, job satisfaction, andturnover among psychiatric technicians.
10.1037/h0037511 1974 James, Lawrence;Jones, Allan
Organizational climate: A review of theory and re-search
10.1111j.1744-6570.1975.tb01386.x
1975 Schneider, Ben-jamin
Organizational climates: An essay.
10.1037//0021-9010.62.1.38
1977 Drexler, John A. Organizational Climate: Its Homogeneity Within Or-ganizations
10.1016/0001-8791(79)90072-1
1979 Mowday, Richard;Steers, Richard;Porter, Lyman
The Measurement of Organizational Commitment
10.1111/j.1745-3984.1980.tb00831.x
1980 Sirotnik, KennethA.
Psychometric Implications of the Unit-of-AnalysisProblem (With Examples from the Measurement ofOrganizational Climate)
10.1177/001872678704000704 1987 DeCotiis,Thomas; Sum-mers, TimothyP
A Path Analysis of a Model of the Antecedents andConsequences of Organizational Commitment
10.2307/2392857 1988 Victor, Bart;Cullen, John
The Organizational Bases of Ethical Work Climates
10.1037/0003-066X.45.2.109
1990 Schein, Edgar H. Organizational Culture
10.1037/0021-9010.75.6.668
1990 Rentsch, Joan R. Climate and Culture: Interaction and Qualitative Dif-ferences in Organizational Meanings
10.2307/258997 1996 Denison, Daniel. What is the Difference Between Organizational Cul-ture and Organizational Climate? A Native’s Pointof View on a Decade of Paradigm Wars
10.1348/096317904774202144 2004 Patterson, Mal-colm; Warr,Peter; West,Michael
Organizational climate and company productivity:The role of employee affect and employee level
10.1002/job.312 2005 Patterson, Mal-colm; West,Michael; Shack-leton, Viv JDawson, Jeremy;Lawthom, Re-becca Maitlis,Sally; Robinson,David; Wallace,Alison
Validating the Organizational Climate Measure:Links to Managerial Practices, Productivity and In-novation
10.1177/0149206308330559 2009 Kuenzi, Mari-beth; Schminke,Marshal
Assembling Fragments Into a Lens: A Review, Cri-tique, and Proposed Research Agenda for the Organi-zational Work Climate Literature
10.1037/a0018867 2010 Walumbwa, Fred;Hartnell, Chad;Oke, Adegoke
Servant Leadership, Procedural Justice Climate, Ser-vice Climate, Employee Attitudes, and Organiza-tional Citizenship Behavior: A Cross-Level Investiga-tion
10.1146/annurev-psych-113011-143809
2012 Schneider, Ben-jamin; Ehrhart,Mark; Macey,William
Organizational Climate and Culture
10.1002/hrm.21498 2012 Zhang, Haina;Kwan, Ho Kwong;Everett, Andre;Jian, Zhaoquan
Servant leadership, organizational identification andwork to family enrichment: The moderating role ofwork climate for sharing family concerns.
10.1016/.leaqua.2012.10.008 2012 Sun, Li-Yun; Hau,Irene; Chow, Siu;Chiu, Randy;Pan, Wen
Outcome favorability in the link between leader-member exchange and organizational citizenship be-havior: Procedural fairness climate matters
2
Are there gender differences inperceived organizational climate?:
The case of Tuscan healthcare system.1
This study examines the organizational climate considering gender differences
in the professional role within healthcare organizations. Data came from
organizational-climate questionnaires administered in 2010 to 1498 health
managers and 19616 health staff in Tuscany Region (Italy). We applied
exploratory factor analysis to verify the validity and internal consistency
between items and t-test to compare mean perceptions regarding the dimen-
sions across different groups of respondents. We measured five dimensions
’training opportunities’, ’communication and information processing’, ’man-
agerial tools’, ’organization’ and ’management & leadership style’ and overall
job satisfaction. Gender differences in the professional roles were significant
between managers’ and staff’s perceptions (p ≤ 0.05).
2.1 Introduction
In the 20th century the condition of women has greatly improved in several aspects.
However, the gender gap is remarkable in the lack of access to power and leadership
1With: Chiara Seghieri1, Diana Rojas, Sabina Nuti. Acknowledgements: The authors wishto thank the researchers of the MesLab, in particular Manuela Furlan, Domenico Cerasuolo andFrancesca Sanna who are responsible for the management of the organizational climate surveys;Francesco Niccolai for his precious suggestions; the staff of all Tuscan healthcare organizationsand Tuscany region for the financial support of the project.
Introduction 25
positions compared with men, and women managers are still in a minority (Carli
and Eagly, 2001).
Generally, women are less frequently found in leadership positions compared to
men and more frequently in staff positions, consequently they have less opportunity
to demonstrate their competencies (Wiggins, 1996) and even in female-dominated
occupations, men have more opportunity to be promoted to the top (Broadbridge,
2010). The 2011 Catalyst Census showed that in 2010 women held 14.4 percent of
Executive Officer positions and 7.6 percent of Executive Officer top earner positions
(Soares et al., 2009).
When considering the healthcare sector, the promotion of women to senior man-
agement positions in healthcare organizations has been shown to be slower in
comparison with men even when most positions are held by women. The same
happens to financial benefits which seem to decrease for women and expand for men
as their respective careers advance. Moreover, researches in USA have demonstrated
that, in the last years, little has been made to close the gender gap in healthcare
leadership especially among the nation’s top hospitals (Branin, 2009).
The same evidences have been also found in Italy, where independently if public or
private organizations, women have more limited possibilities to advance in their
careers. The percentage of women on boards and senior-executive teams remains
one of the lowest among European countries (7% compared with 33% of women
in Scandinavian countries). Italy, in fact, ranks 74th out of 134 countries in the
Gender Gap Index 2010, immediately followed by Colombia, Vietnam and Peru.
35% of the Italian women in the age of 25-44 is unemployed (21% is the average
in the rest of Europe) and women who work, on average earn 20% less than men
(Commission et al., 2010). Within years, only few policies have been adopted at
national level to support women with young children, networks to help women
navigate their careers and formal sponsorship programs to ensure professional
development (www.womenomics.it).
With regard to the Italian healthcare sector, results from a survey administered
to a sample of 1821 physicians of Padova city (Italy) in 2010 showed that 37,84%
of the respondents declared to be not satisfied of the advancement in their career
and of these, 22% are women while 16% men (http://www.fnomceo.it). Whereas,
results from another survey to a sample of 1549 Italian physician women belonging
Introduction 26
to the medical association in 2011 showed that 27% of the respondents declared to
be discriminated in their work in general and 37.5% in their possibilities of reaching
high job positions. 39% of the women reported that their ideas and suggestions
were not taken in consideration by superiors and 80% reported that they have not
been involved in any training opportunities. Finally 4% of the sample declared to
have received a physical abuse and only 61% was satisfied with their job (Ordine
Provinciale di Roma dei Medici Chirurghi e degli Odontoiatri, (2011)).
Given these premises, the present study intends to contribute to the researches
on gender inequality at work by analyzing results from an organizational climate
survey administered in 2010 to professionals of twelve Local Health Authorities
(LHAs) of Tuscany region (Italy).
The purpose of this study is to determine whether organizational climate charac-
teristics such as training opportunities, communication & information processing,
managerial tools, organization structure and management & leadership style and
overall job satisfaction are differently perceived across men and women at managerial
and staff level within LHAs.
In particular the study aims to test the following hypothesis:
H1. ’Male and female employees of Tuscan healthcare organizations differ signifi-
cantly in terms of perceived organizational climate and job satisfaction’
H2. ’Male and female employees of Tuscan healthcare organizations differ signifi-
cantly in terms of perceived satisfaction in the relationship with their superiors in
terms of communication, motivation, and support’
This information can be used by organizations and human resource professionals
to better understand possible barriers and discriminations perceived by women
within the organization which can negatively affect their attitudes, behavior, and
organizational commitment.
Data and Methods 27
2.2 Data and Methods
Organizational climate is a distinct construct concerned with the way organizational
members perceive the work environment within that organization and its impact on
their individual psychological well being (Jones and James, 1979). This concept can
be traced back to several studies, which have showed the role of the organizational
climate survey to measure organizational characteristics perceived by employees
and better understand those factors which contribute to a work environment (or
climate) that is pleasant, and motivates all employees, regardless of their position,
status and gender, to be committed and effective performers (Lewin et al., 1939;
Koffka, 1935; Phillips et al., 1996).
Especially for those organizations requiring highly skilled employees, such as physi-
cians in hospitals, a working environment which enhance the knowledge, skills,
ability and motivation of employees have been demonstrated to have a greater
impact on the performance of organization.
With regard to the Tuscan healthcare system, organizational climate as perceived
by healthcare professionals, has been always considered an important dimension to
be constantly monitored through the Performance Evaluation System of the Tuscan
healthcare. This system, developed in 2004 by MeS on behalf of Tuscany region
intends to constantly measure and monitor the quality of services provided and
the capacity to meet citizens’ needs by healthcare organization in order to achieve
better health and quality of life standards on one side and, on the other, to preserve
financial equilibrium (Nuti, 2008; Nuti et al., 2009, 2013).
Since 2004, Tuscan healthcare top management and professionals are called to
participate to the organizational climate survey which is carried out about once
every two years within all Tuscan health organizations. This survey is based on two
questionnaires, formulated in 2004 by MeS researchers (Pizzini and Furlan, 2012)
following the international and national review on organizational climate.
Questionnaire ’A’ is directed to all managers with ’management/budget’ responsi-
bilities (i.e ward managers), and questionnaire ’B’ to health employees. The two
questionnaires were similar in size and items investigated.
Results 28
Regarding to the procedures for compiling and sending the survey, MeS Lab provided
the questionnaires on-line using the Computer Assisted Web Interviewing (CAWI)
system: each employee had a login and password that allowed him/her access to
the web platform for collecting data. Secure connection guaranteed the anonymity
of responses and the safety of data transmitted.
Independently from the questionnaire, all questions had a 5-point likert scale
format, ranging from 1 extremely unsatisfied to 5 extremely satisfied. The analysis
extracted information on the survey sample, job satisfaction and organizational
climate dimensions like communication and information processing, management &
leadership style (ward managers and top management for employees and managers
respectively), managerial tools (i.e. budget), company organization and training
opportunities. Along years both questionnaires were tasted and validated and
changes were made in order to assure the validity and reliability of the instrument.
With regard to 2010 survey data, we analyzed results from questionnaires A and
B independently (851, 12576 questionnaires). We calculated descriptive statistics
and the means item scores were quiet low suggesting a general negative staff’s
perception of the organizational climate.
Finally, we applied Factor Analysis to questionnaires A and B separately to obtain
the perception of managers and employees in terms of the dimensions mentioned
above. We performed descriptive statistics, factor analysis and two-tailed test to
examine gender differences in the LHAs. We used STATA software for statistical
analyses (Version12, Stata Corp, College Station, TX).
2.3 Results
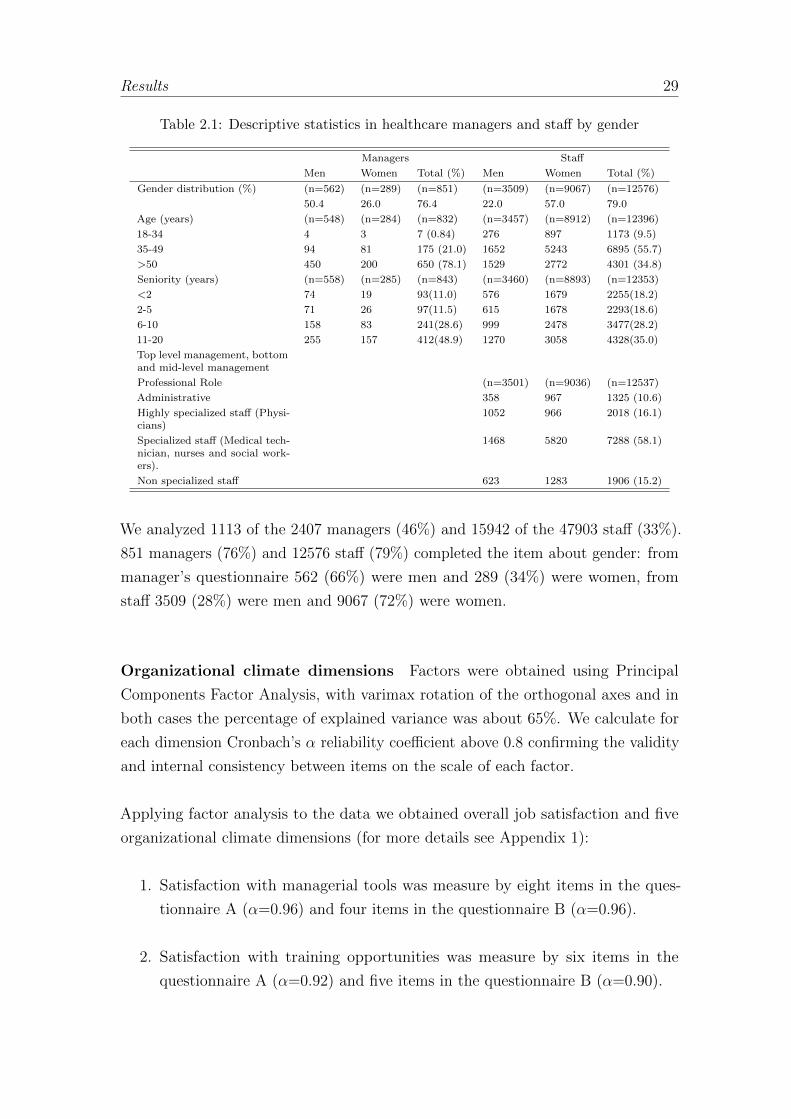
Respondents’ characteristics Table 2.1 shows descriptive statistics from gender
point of view. The percentage of responders were 46% for managers and 33% for
the staff. Most of the managers were male (66%), older than 50 years (54%) and
had more than 20 years of working experience (30%). On the contrary, the majority
of non managerial staff was female (72%), in the age class of 35-49 (42%) and had
11-20 years of working experience (25%).
Results 29
Table 2.1: Descriptive statistics in healthcare managers and staff by gender
Managers Staff
Men Women Total (%) Men Women Total (%)
Gender distribution (%) (n=562) (n=289) (n=851) (n=3509) (n=9067) (n=12576)
50.4 26.0 76.4 22.0 57.0 79.0
Age (years) (n=548) (n=284) (n=832) (n=3457) (n=8912) (n=12396)
18-34 4 3 7 (0.84) 276 897 1173 (9.5)
35-49 94 81 175 (21.0) 1652 5243 6895 (55.7)
>50 450 200 650 (78.1) 1529 2772 4301 (34.8)
Seniority (years) (n=558) (n=285) (n=843) (n=3460) (n=8893) (n=12353)
<2 74 19 93(11.0) 576 1679 2255(18.2)
2-5 71 26 97(11.5) 615 1678 2293(18.6)
6-10 158 83 241(28.6) 999 2478 3477(28.2)
11-20 255 157 412(48.9) 1270 3058 4328(35.0)
Top level management, bottomand mid-level management
Professional Role (n=3501) (n=9036) (n=12537)
Administrative 358 967 1325 (10.6)
Highly specialized staff (Physi-cians)
1052 966 2018 (16.1)
Specialized staff (Medical tech-nician, nurses and social work-ers).
1468 5820 7288 (58.1)
Non specialized staff 623 1283 1906 (15.2)
We analyzed 1113 of the 2407 managers (46%) and 15942 of the 47903 staff (33%).
851 managers (76%) and 12576 staff (79%) completed the item about gender: from
manager’s questionnaire 562 (66%) were men and 289 (34%) were women, from
staff 3509 (28%) were men and 9067 (72%) were women.
Organizational climate dimensions Factors were obtained using Principal
Components Factor Analysis, with varimax rotation of the orthogonal axes and in
both cases the percentage of explained variance was about 65%. We calculate for
each dimension Cronbach’s α reliability coefficient above 0.8 confirming the validity
and internal consistency between items on the scale of each factor.
Applying factor analysis to the data we obtained overall job satisfaction and five
organizational climate dimensions (for more details see Appendix 1):
1. Satisfaction with managerial tools was measure by eight items in the ques-
tionnaire A (α=0.96) and four items in the questionnaire B (α=0.96).
2. Satisfaction with training opportunities was measure by six items in the
questionnaire A (α=0.92) and five items in the questionnaire B (α=0.90).
Results 30
Table 2.2: Gender differences of perceived organizational climate at managerial level.
LHAs Men Women
(n=562) n=289)
Dimension Mean Sd Mean Sd
Communication & Infor-mation processing
0.258 0.948 0.073 0.989
p =< 0.05
3. Satisfaction with communication and information processing was measure by
five items in the questionnaire A and B (α=0.90, α=0.86) respectively.
4. Satisfaction with the organization was measure by fifteen items in the ques-
tionnaire A (α=0.96) and four items in the questionnaire B (α=0.90).
5. Satisfaction with management & leadership style was measure by five items
in the questionnaire A (α=0.88) and eighteen items in the questionnaire B
(α=0.96).
Overall job satisfaction dimension was measure by four items in questionnaire A
and B (α=0.80 in both cases) and it is defined as a positive emotional response to
the result of the work performed allowing the fulfillment of an individual’s value
(Locke et al., 1984).
Gender differences in the perception of Organizational Climate Factors
Phase two of the data analysis consists of studying differences between gender and
professional roles groups. We used t-test to compare mean perceptions regarding
the above mentioned dimensions across women and men in both managerial and
staff position. We also analyzed key questions separately which are relevant to
better explore gender inequalities at work. The probability level for all hypothesis
tests was set at p ≤ 0.05.
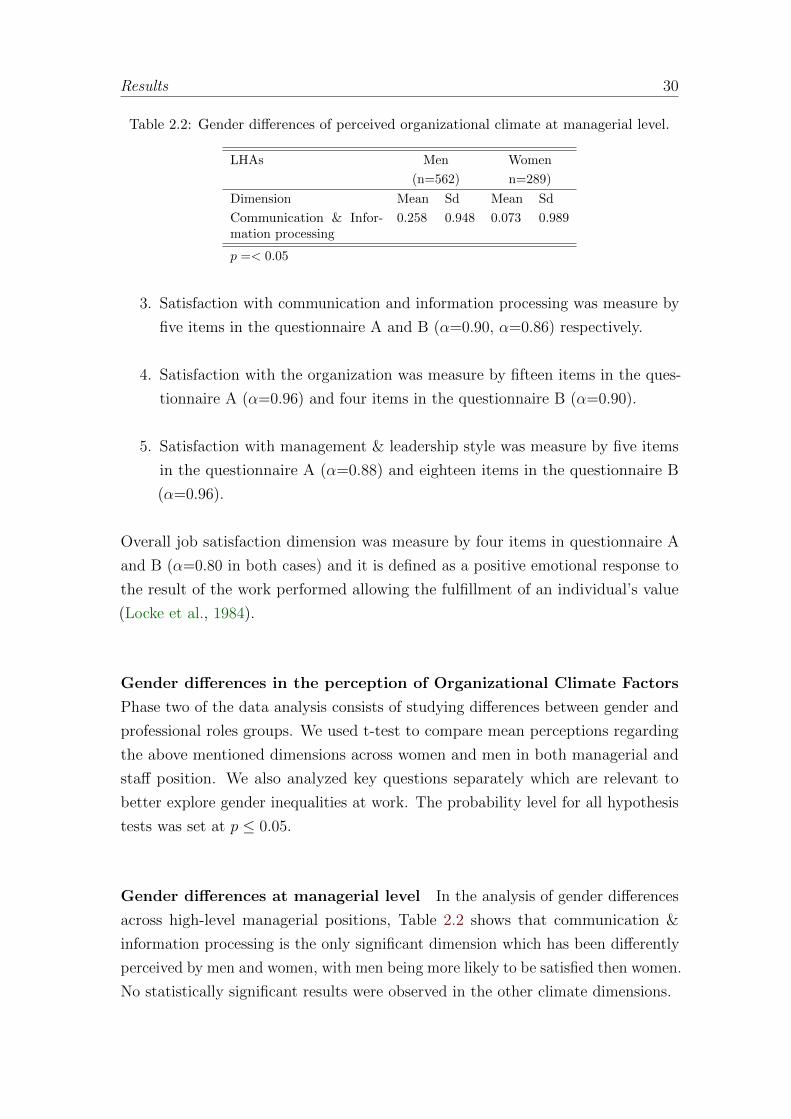
Gender differences at managerial level In the analysis of gender differences
across high-level managerial positions, Table 2.2 shows that communication &
information processing is the only significant dimension which has been differently
perceived by men and women, with men being more likely to be satisfied then women.
No statistically significant results were observed in the other climate dimensions.
Results 31
Table 2.3: Distribution of male/female respondents by selected questions within dimensionof communication and information processing at managerial level.
Communication and Infor-mation processing
Men Women
(n=562) n=289)
Mean Sd Mean Sd
Feedback informationabout the quality ofwork and achievementsperformed.
3,135 0,053 2,955 0,073
The CEO monitors theproper way in which theobjectives of the organiza-tion are followed.
3,377 0,053 3,059 0,077
To know the aims of theorganization.
3,776 0,043 3,581 0,068
To know the annual resultsof my organization (eco-nomic, health system, pa-tient satisfaction, etc.).
3,576 0,046 3,391 0,066
p =< 0.05
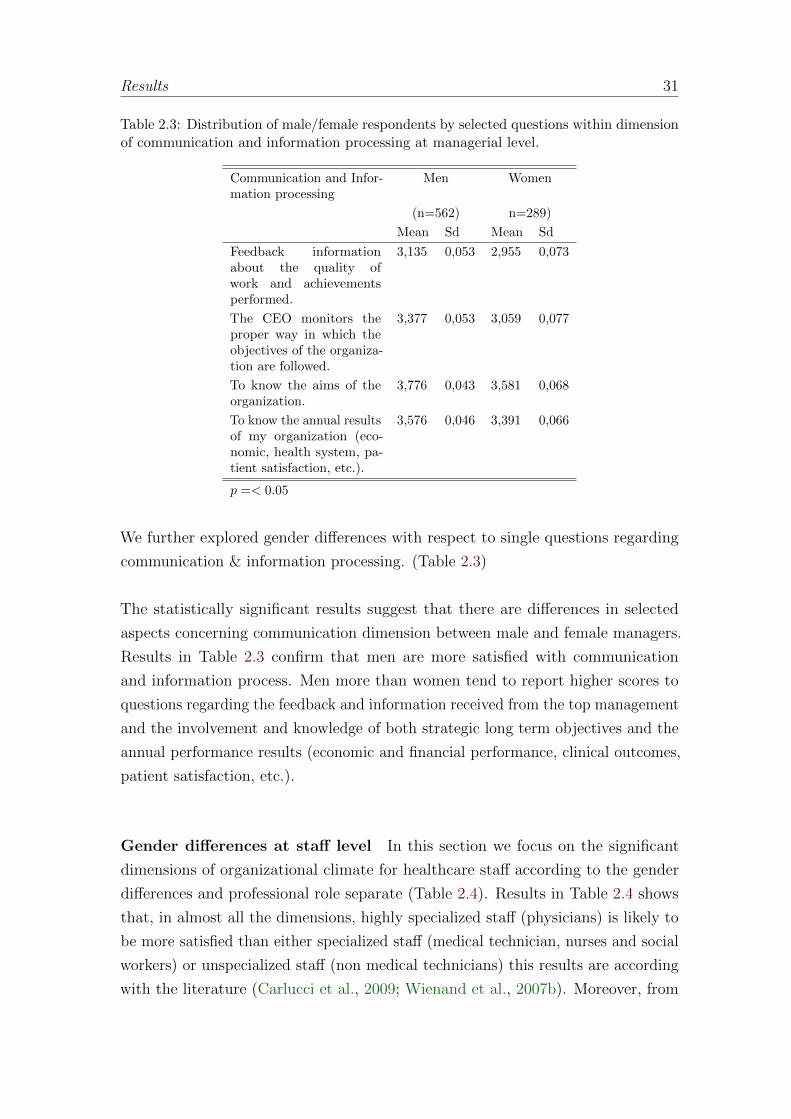
We further explored gender differences with respect to single questions regarding
communication & information processing. (Table 2.3)
The statistically significant results suggest that there are differences in selected
aspects concerning communication dimension between male and female managers.
Results in Table 2.3 confirm that men are more satisfied with communication
and information process. Men more than women tend to report higher scores to
questions regarding the feedback and information received from the top management
and the involvement and knowledge of both strategic long term objectives and the
annual performance results (economic and financial performance, clinical outcomes,
patient satisfaction, etc.).
Gender differences at staff level In this section we focus on the significant
dimensions of organizational climate for healthcare staff according to the gender
differences and professional role separate (Table 2.4). Results in Table 2.4 shows
that, in almost all the dimensions, highly specialized staff (physicians) is likely to
be more satisfied than either specialized staff (medical technician, nurses and social
workers) or unspecialized staff (non medical technicians) this results are according
with the literature (Carlucci et al., 2009; Wienand et al., 2007b). Moreover, from
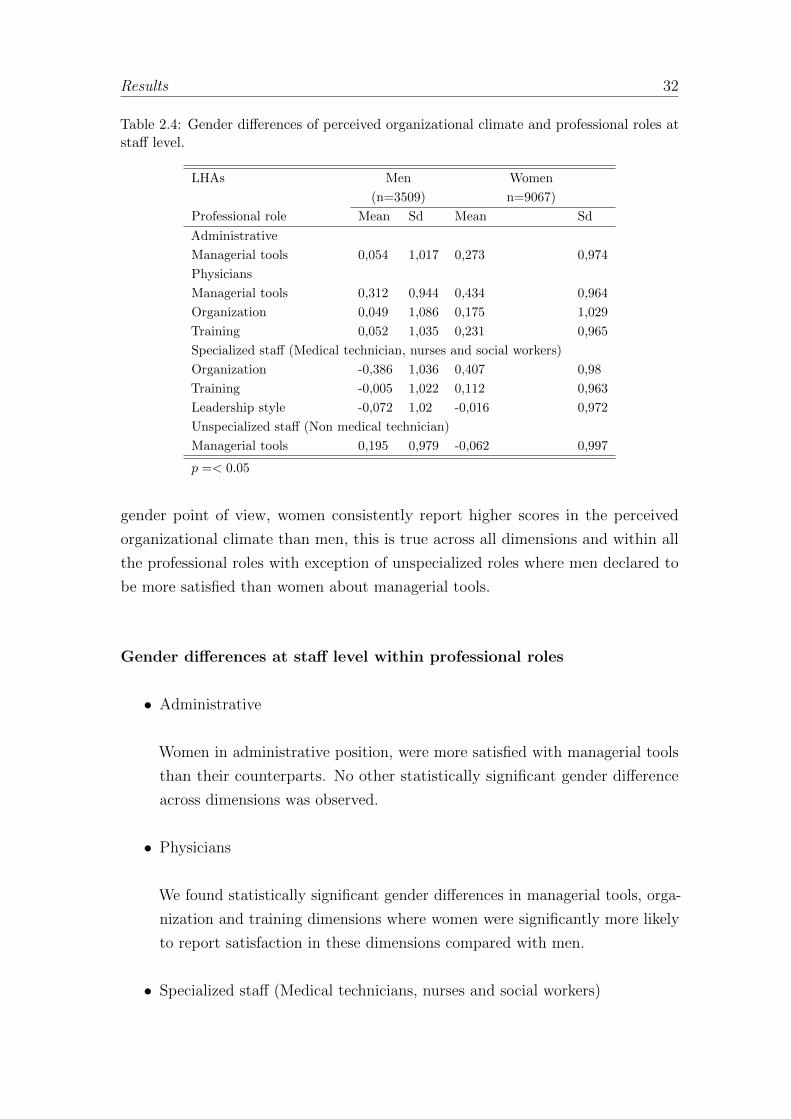
Results 32
Table 2.4: Gender differences of perceived organizational climate and professional roles atstaff level.
LHAs Men Women
(n=3509) n=9067)
Professional role Mean Sd Mean Sd
Administrative
Managerial tools 0,054 1,017 0,273 0,974
Physicians
Managerial tools 0,312 0,944 0,434 0,964
Organization 0,049 1,086 0,175 1,029
Training 0,052 1,035 0,231 0,965
Specialized staff (Medical technician, nurses and social workers)
Organization -0,386 1,036 0,407 0,98
Training -0,005 1,022 0,112 0,963
Leadership style -0,072 1,02 -0,016 0,972
Unspecialized staff (Non medical technician)
Managerial tools 0,195 0,979 -0,062 0,997
p =< 0.05
gender point of view, women consistently report higher scores in the perceived
organizational climate than men, this is true across all dimensions and within all
the professional roles with exception of unspecialized roles where men declared to
be more satisfied than women about managerial tools.
Gender differences at staff level within professional roles
• Administrative
Women in administrative position, were more satisfied with managerial tools
than their counterparts. No other statistically significant gender difference
across dimensions was observed.
• Physicians
We found statistically significant gender differences in managerial tools, orga-
nization and training dimensions where women were significantly more likely
to report satisfaction in these dimensions compared with men.
• Specialized staff (Medical technicians, nurses and social workers)
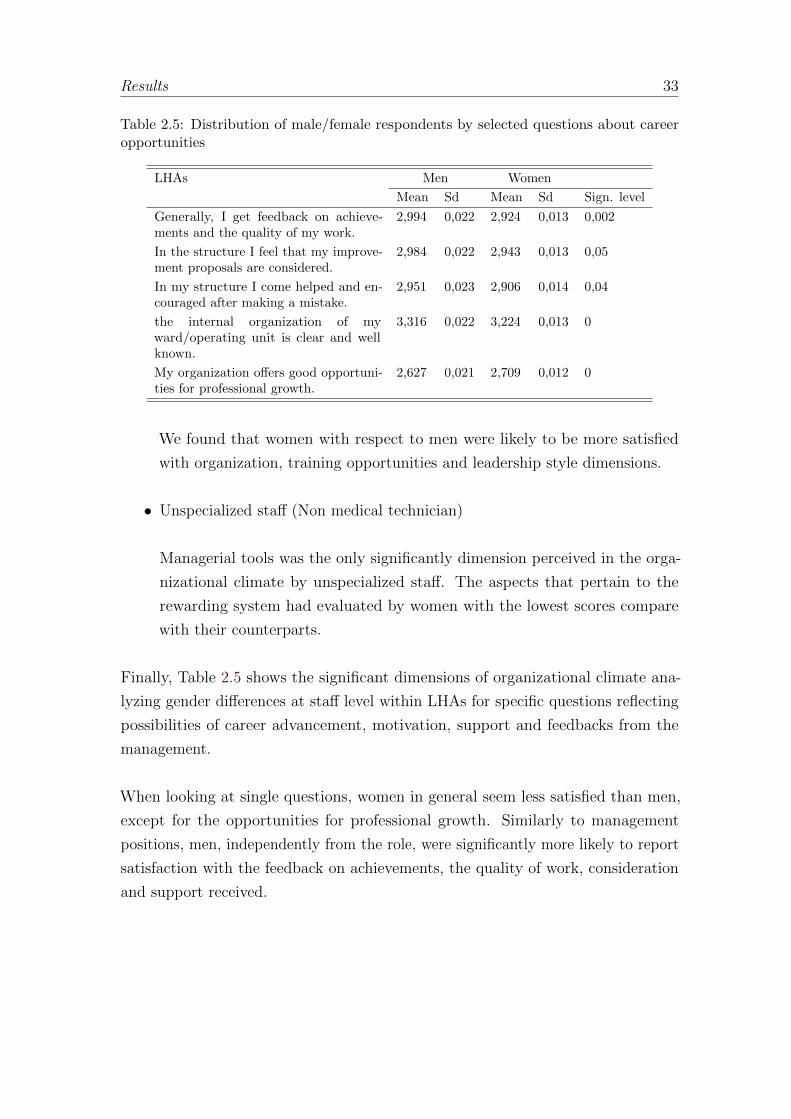
Results 33
Table 2.5: Distribution of male/female respondents by selected questions about careeropportunities
LHAs Men Women
Mean Sd Mean Sd Sign. level
Generally, I get feedback on achieve-ments and the quality of my work.
2,994 0,022 2,924 0,013 0,002
In the structure I feel that my improve-ment proposals are considered.
2,984 0,022 2,943 0,013 0,05
In my structure I come helped and en-couraged after making a mistake.
2,951 0,023 2,906 0,014 0,04
the internal organization of myward/operating unit is clear and wellknown.
3,316 0,022 3,224 0,013 0
My organization offers good opportuni-ties for professional growth.
2,627 0,021 2,709 0,012 0
We found that women with respect to men were likely to be more satisfied
with organization, training opportunities and leadership style dimensions.
• Unspecialized staff (Non medical technician)
Managerial tools was the only significantly dimension perceived in the orga-
nizational climate by unspecialized staff. The aspects that pertain to the
rewarding system had evaluated by women with the lowest scores compare
with their counterparts.
Finally, Table 2.5 shows the significant dimensions of organizational climate ana-
lyzing gender differences at staff level within LHAs for specific questions reflecting
possibilities of career advancement, motivation, support and feedbacks from the
management.
When looking at single questions, women in general seem less satisfied than men,
except for the opportunities for professional growth. Similarly to management
positions, men, independently from the role, were significantly more likely to report
satisfaction with the feedback on achievements, the quality of work, consideration
and support received.

Discussion 34
2.4 Discussion
The first aim of the study was to investigate gender differences in the perception of
organizational climate dimensions and job satisfaction across professional roles.
With regards to managerial positions no gender differences were found in both
job satisfaction and organizational climate dimensions except for communication
and information process where men managers seemed more satisfied then women
counterparts. On the contrary, when considering staff positions, women tend to
report in general significantly higher scores then men.
This last result might be due to a real difference in the type of work performed
among staff position. Clark (1985) argued that objectively, women’s jobs are worse
than men’s and those who expect less from working will be more satisfied with any
given work. In this case, greater satisfaction in the perceived organizational climate
may reflect women’ low expectations regarding to the work performed. Moreover,
women, more than men, might also expect to have to accommodate to the needs of
their family (Harriman, 1996; Spector, 1997).
Also, Eagly (1987) argued that gender differences in the work place are due to
the bias of individuals to behave consistently with their social roles. For example,
there are different expectations of behavior for social roles of physicians and nurse.
There is a greater representation of men in the physician’s role, and a greater
representation of women in the nurse’s role. Therefore, the gender differences in
the organizational climate between men and women in these roles can be a result of
differences in the distribution of physicians and nurses.
With regard to the second hypothesis of the study, gender differences were found
in the perception of selected aspects such as: the level of communication of the
organizational planning and strategic objectives between managers and CEOs, the
level of communication of the organizational unit objectives and work program
between staff members and managers, communication and ongoing feedbacks be-
tween staff members and managers on the quality of the work level of promotion
and motivation staff members’ own professional development goals. All of these
aspects are strictly related on the way one’s supervisor handles his workers in terms
of recognition one gets from doing the job, communication of organization/wards

Discussion 35
objectives and strategies, recognition of individual contribute.
Our analysis shows that with respect to these aspects, males are likely to be more
satisfied than their counterparts. This is true across all the professional positions
within the organization.
Even in a female dominated profession such as healthcare the number of women in
supervising positions is less in comparison with men (LaPierre and Zimmerman,
2012; Wiggins, 1996; Walsh and Borkowski, 1999). This masculine environment in
supervisory positions is likely to promote asymmetries that contribute to different
gender perceptions and behaviors in the organization. Females in the Tuscan
healthcare environment may face challenges in the supervision-human relations
aspects which in part maybe due to gender stereotypes that exists between men
and women in these supervisory relationships. Women are often considered by
men as less career-orientated, more committed to the family than their jobs, less
motivated by organizational rewards than their male counterparts and they have to
work harder to demonstrate their competence.
On the other hand women would like to be more involved in the communication
processes and for them is most important to know and to share with the management
staff the organizational goals. Indeed, males have been demonstrated to be dominant,
and unemotional and more task-oriented while females tend to be more emotional,
compassionate, emphatic and supportive, and more interpersonally oriented (Eagly
and Johannesen-Schmidt, 2001).
Burke et al. (1998) showed that women who supervise are more sensitive to the
needs of women on their staffs, they better able to develop closer relationships with
them, and more willing to invest in this relationship than male supervisors. As
a consequence one might expect that men in managerial position would interact
differently with those they supervise if men or women, supporting the fact findings
that females tend to be less satisfied then male in some aspects related to commu-
nication, information, and interaction with supervisors who are for the majority
males.

Conclusions 36
2.5 Conclusions
The results of the present study support the hypothesis that there are gender
difference in how the organizational climate is perceived by managers and employees
in Tuscan healthcare organizations. The analysis showed that the Tuscan organiza-
tional climate questionnaire is a reliable instrument used as a measurement tool for
evaluating working conditions and determining the different factors which satisfies
and motivates employees in the healthcare sector.
This study shows that there are gender differences in how individuals experience
satisfaction within work environment, especially across all professional roles within
healthcare staff. In terms of particular aspects of the job related it was found that
males rated higher than females the interaction with their supervisors.
Women want more from their leaders: they want to participate, to share respons-
abilities by adopting a team working approach. They tend to believe much more
than men in positive effects of training activities and personnel involvement in the
organizational performance. Men with management responsibilities in the health
sector should dedicate more time to their staff especially to women working in their
team in order to facilitate their involvement in the improvement process, and to
guarantying space and development to their contributions.
The use of an organizational climate survey helps management to identify the
critical points in the different dimensions and communicate more effectively within
the structures improving the effectiveness of total quality management programmes.
In fact, a valid internal climate survey can be an useful tool for supporting the
management to avoid perceptual discrepancy and tailor a motivational strategy
that is specific to the employee’s individual needs and aspirations.
Moreover, in order to assure its effectiveness it is important to share and discuss
the results of the internal climate survey with all the professionals being this the
most important prerequisite to support the organizational changes and it is what
the Tuscan health managers are used to do not only with regards to the internal
climate results but also to all the performance measures.
The current research has some limitation; first is a select sample and these results

Conclusions 37
may not extend to healthcare professionals populations; also it is not possible to
generalize the results regarding geographic or political context, second is due to
privacy reasons some respondents failed to report their gender introducing possible
selection biases in the results. Further, there are many other factors that can be
considered to determine employees satisfaction which can be added to expand the
study in future.
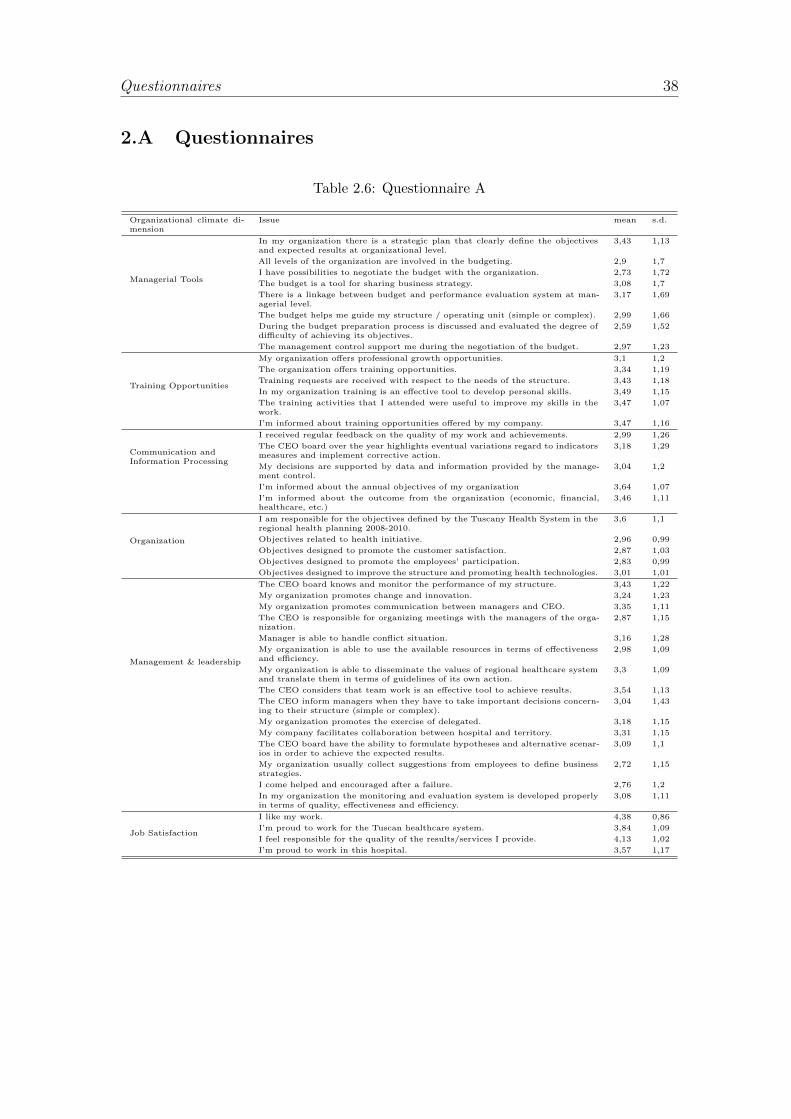
Questionnaires 38
2.A Questionnaires
Table 2.6: Questionnaire A
Organizational climate di-mension
Issue mean s.d.
Managerial Tools
In my organization there is a strategic plan that clearly define the objectivesand expected results at organizational level.
3,43 1,13
All levels of the organization are involved in the budgeting. 2,9 1,7
I have possibilities to negotiate the budget with the organization. 2,73 1,72
The budget is a tool for sharing business strategy. 3,08 1,7
There is a linkage between budget and performance evaluation system at man-agerial level.
3,17 1,69
The budget helps me guide my structure / operating unit (simple or complex). 2,99 1,66
During the budget preparation process is discussed and evaluated the degree ofdifficulty of achieving its objectives.
2,59 1,52
The management control support me during the negotiation of the budget. 2,97 1,23
Training Opportunities
My organization offers professional growth opportunities. 3,1 1,2
The organization offers training opportunities. 3,34 1,19
Training requests are received with respect to the needs of the structure. 3,43 1,18
In my organization training is an effective tool to develop personal skills. 3,49 1,15
The training activities that I attended were useful to improve my skills in thework.
3,47 1,07
I’m informed about training opportunities offered by my company. 3,47 1,16
Communication andInformation Processing
I received regular feedback on the quality of my work and achievements. 2,99 1,26
The CEO board over the year highlights eventual variations regard to indicatorsmeasures and implement corrective action.
3,18 1,29
My decisions are supported by data and information provided by the manage-ment control.
3,04 1,2
I’m informed about the annual objectives of my organization 3,64 1,07
I’m informed about the outcome from the organization (economic, financial,healthcare, etc.)
3,46 1,11
Organization
I am responsible for the objectives defined by the Tuscany Health System in theregional health planning 2008-2010.
3,6 1,1
Objectives related to health initiative. 2,96 0,99
Objectives designed to promote the customer satisfaction. 2,87 1,03
Objectives designed to promote the employees’ participation. 2,83 0,99
Objectives designed to improve the structure and promoting health technologies. 3,01 1,01
Management & leadership
The CEO board knows and monitor the performance of my structure. 3,43 1,22
My organization promotes change and innovation. 3,24 1,23
My organization promotes communication between managers and CEO. 3,35 1,11
The CEO is responsible for organizing meetings with the managers of the orga-nization.
2,87 1,15
Manager is able to handle conflict situation. 3,16 1,28
My organization is able to use the available resources in terms of effectivenessand efficiency.
2,98 1,09
My organization is able to disseminate the values of regional healthcare systemand translate them in terms of guidelines of its own action.
3,3 1,09
The CEO considers that team work is an effective tool to achieve results. 3,54 1,13
The CEO inform managers when they have to take important decisions concern-ing to their structure (simple or complex).
3,04 1,43
My organization promotes the exercise of delegated. 3,18 1,15
My company facilitates collaboration between hospital and territory. 3,31 1,15
The CEO board have the ability to formulate hypotheses and alternative scenar-ios in order to achieve the expected results.
3,09 1,1
My organization usually collect suggestions from employees to define businessstrategies.
2,72 1,15
I come helped and encouraged after a failure. 2,76 1,2
In my organization the monitoring and evaluation system is developed properlyin terms of quality, effectiveness and efficiency.
3,08 1,11
Job Satisfaction
I like my work. 4,38 0,86
I’m proud to work for the Tuscan healthcare system. 3,84 1,09
I feel responsible for the quality of the results/services I provide. 4,13 1,02
I’m proud to work in this hospital. 3,57 1,17

Questionnaires 39
Table 2.7: Questionnaire B
Organizational climate di-mension
Issue mean s.d.
Managerial Tools
In my organization the budget is used correctly. 2,13 1,71
The objectives defined in the budget are shared with employees. 2,11 1,77
The objectives defined in the budget are verified along the year. 2,05 1,75
The objectives of the budget help me to direct my job. 1,94 1,68
Training Opportunities
The organization offers training opportunities. 2,94 1,15
Training requests are received with regard to the needs of the structure. 2,91 1,19
In my organization training is an effective tool to develop personal skills. 3,05 1,21
The training activities that I attended were useful to improve my skills. 3,29 1,17
I think being informed about training opportunities offered by my company. 2,78 1,22
Communication andInformation Processing
I’m informed about the quality of services that we provide to users (patients, citizens). 3,48 1,07
I’m informed about customer satisfaction (patients, citizens). 3,03 1,07
I’m informed about the organization of my structure/operating unit. 2,88 1,08
I’m informed about the economic, financial or healthcare outcomes. 2,46 1,1
I’m informed about important decisions and strategies taken by the CEO. 2,24 1,11
Organization My organization offers opportunities for professional growth. 2,63 1,19
My organization supports change and innovation. 2,61 1,18
My organization promotes and facilitates collaboration between structures. 2,6 1,14
The Manager is interested in the situation of my hospital/operating units. 2,58 1,21
Management & leadership
I get feedback on achievements and the quality of my work. 2,91 1,25
Meetings are regularly organized in my internal structure. 3,2 1,38
My manager is easily contactable in case I need to talk to him. 3,83 1,23
In the structure I feel that my improvement proposals are considered. 2,9 1,27
In my work my boss and colleagues help me to develop my skills. 2,93 1,26
Employees have appropriate conditions to develop their work. 2,92 1,17
I come helped and encouraged after making a mistake. 2,87 1,31
My manager is able to delegate. 3,44 1,29
Managers informed employees when they have to take important decisions that affect thestructure.
2,83 1,34
In my work are recognized results achieved by the team. 2,92 1,28
My manager knows how to manage conflict situations. 2,8 1,34
I feel responsible for the quality of the results/services I provide. 3,59 1,2
My services are regularly verified. 3,18 1,23
I receive clear guidelines and instructions about activities I have to develop. 3,1 1,24
In my group, the work is well planned and this allows us to reach the objectives proposed. 3,12 1,22
My job is evaluated in an equitable manner. 2,92 1,26
In my structure objectives are clear and well defined. 3,03 1,24
The internal organization of my structure/operating unit is clear and well known. 3,21 1,24
Job Satisfaction
I like my work. 4,17 0,97
I’m happy to work in this hospital. 3,58 1,14
I’m proud to work in this hospital. 3,1 1,23
I’m proud to work for the Tuscan healthcare system. 3,66 1,15
3
Organizational climate: Comparingprivate and public hospitals within
professional roles1
This study compares the organizational climate differences within profes-
sional roles in private and public hospitals. We focus on how physicians,
administrative, healthcare and non healthcare staff either in the public and
in the private organizations perceived their work environment and each
organizational climate dimension. Data came from organizational-climate
questionnaires administered in 2010 and 2012 to 19616 and 1276 health
employees in public and private hospitals in the Tuscany Region respectively.
We applied exploratory factor analysis to verify the validity and internal
consistency between items in the questionnaire and t-test, one-way analysis
of variance to compare means perceptions regarding to the dimensions across
different groups of respondents. We measured four dimensions: ’training op-
portunities’, ’managerial tools’, ’organization’ and ’management & leadership
style’ and overall job satisfaction. Hospital status within staff perceptions by
professional roles was found significant at (p ≤ 0.05).
3.1 Introduction
It has been identified important elements for healthcare staff’s commitment and
loyalty toward the organization, examples of this elements are: continuing training
1Chiara Seghieri, Diana Rojas, Sabina Nuti

Introduction 41
and education (Spath, 2002), leadership style, project management, staff recognition,
dedicated time, and resources for improvement projects. (Thomson et al., 2002)
But, organizational climate seems to depend also on the particular characteristics
of the work environment (Tovey and Adams, 1999; Cumbey and Alexander, 1998).
Organizational climate is defined as the shared perceptions of the work environment
Jones and James (1979). In the present study we were able to analyze the difference
between hospital status (public or private) and professional roles with respect to
organizational climate dimensions like: Training opportunities, Managerial tools,
Organization Management & leadership style and overall job satisfaction within
twelve public general hospitals and eighteen accredited private hospitals. Our study
include physicians, administrative staff, healthcare employees and non healthcare
employees of the Tuscan healthcare system. There have been no recent studies of
this phenomenon, and none have compared and contrasted organizational climate
and professional roles at the hospital status. This paper is an attempt to address
this gap in the literature.
The general hypotheses developed was whether public and private hospitals within
professional role would differ significantly on how they perceived the organizational
climate. By studying a country like Italy with a particular health system we
hope to give an insight to better understand the persistent barriers restricting the
organizational climate in the professional roles at hospital status.
With regard to Italy, independently if public or private hospital is important the use
of performance measurement to promote a more efficient and effective administration.
With this premise, the Tuscany region with MeS laboratory in 2005 developed its
own Performance Evaluation System (PES) valued as a particularly innovative and
comprehensive system (Carinci et al., 2012; Censis, 2008) it was implemented in
order to follow up the regional objectives based on the needs of the Regional Health
Councillor. The PES measured the quality of services provided and the ability
to meet the needs of citizens in order to achieve better health and quality of life
standards and to preserve financial stability. The 130 indicators are classified in six
dimensions: Population health status; capacity to pursue regional strategies; clinical
performance; patient satisfaction; organizational climate and finally efficiency and
financial performance. (Nuti et al., 2009; Vainieri and Nuti, 2011; Nuti et al., 2013).
PES indicators are linked to the healthcare CEO’s rewarding system in public

The context 42
institutions where annual goals are set separately for each indicator and each
health authority, taking into account the performance level of the year for each
indicator and the standard to be reached /citepnuti2013variation and optional-
voluntary for private ones. Every year each public Health Authority receives its
own report explaining if it was able to reach the goals during the year and doing
a benchmarking comparison. In 2012 PES has been adopted by eighteen private
hospitals as a decision support tool at managerial level, it decision did possible
to apply the organizational climate questionnaire to private institutions, getting
interesting results to compare with the public context.
We reported a contribution on the debate of diversity in management of healthcare
by highlighting the way in which staff perceived the organizational climate and the
variation addressed in the professional roles and hospital status. The implications of
this study can be useful to policy makers, managers and professionals understanding
how the perception of the organizational climate fit as predictor of good performance.
3.2 The context
The Italian health care system is a National Health Service (Beveridge-like model)
accessible to the full population providing preventive and curative services. (Bev-
eridge, 1942) The system is organized at three levels: national, regional and local.
The national level is responsible for ensuring the general objectives and fundamental
principles of the National Health Service. The regional governments are responsible
for ensuring the delivery of the health care through a network of population-based
healthcare organizations (health authorities).
In Italy during the past two decades, the strong decentralization policy, in the
line with ’New-Public-Management’ (NPM) philosophy (Kettl, 2000; Pollitt, 1995)
which aims is that public organizations should import managerial processes and
behavior from the private sector (Box, 1999; Boyne, 2002). With this argument
the government have gradually transferred several important administrative and
organizational responsibilities from the state to the 21 Italian regions with the aim
of making regions more sensitive to the community needs, to control expenditure,
promote efficiency, quality, and citizen satisfaction but specially it has started to
focus on more effective management (Mouritsen et al., 2005).
Data and Methods 43
This model provided regions with significant autonomy in organizing healthcare
services, allocating financial resources to their Local Health Authorities (LHAs), mon-
itoring and assessing performance (Nuti, 2008; Antonini and Pin, 2009). Whereas,
the central government retains overall responsibility for ensuring that services, care
and assistance are equitably distributed to citizens across the country.
The Tuscany region have 3.7 beds for each 1000 inhabitants of which 95% correspond
to public beds and only 5% are privates. The healthcare system works through a
network of seventeen public health authorities of which five are teaching hospitals
(THs) and twelve are Local Health Authorities (LHAs) and eighteen private hospitals
with accreditation.
In 1999, the Region of Tuscany began the accreditation system (LR 8/1999, LR
51/2009). Institutional accreditation is the recognition by the Region of hospitals
that are authorized to provide and develop health services according to the National
Health Service (NHS). Accreditation is compulsory for public institutions and
optional-voluntary for private ones, but if private institutions does not have the
accreditation cannot provide benefits on behalf of the NHS. However, obtain
accreditation, does not allow to perform services on behalf of the NHS, is compulsory
an agreement between subject and accredited Local Health Authorities that specific
times, costs, terms and amounts of benefits payable in agreement with the NHS.
(Lenzi, 2012)
3.3 Data and Methods
In 2010 the Laboratory of Management e Sanita (MeS) with Tuscany region
administered the organizational climate survey to health care professionals in 16
Tuscan Health Authorities (12 General Hospitals1 and 4 Teaching Hospitals), with
a total population of 2407 managers and 47903 staff. In 2012 the survey was
administered to healthcare professionals in 18 private hospitals with accreditation.
The organizational climate is part of the six dimension within Performance Evalu-
ation System (PES). Regarding to the procedures for compiling and sending the
survey; we provided the questionnaires on-line using the Computer Assisted Web
Interviewing (CAWI) system; each employee had a login and password that allowed
Analysis 44
him/her access to the web platform for collecting data. Secure connection guaran-
teed the anonymity of responses and safety of data transmitted (Pizzini and Furlan,
2012).
Independently from the questionnaire, all questions had a 5-point likert scale
format, ranging from 1 extremely unsatisfied to 5 extremely satisfied. The analysis
extracted information on the survey sample, job satisfaction and organizational
climate dimensions like management & leadership style, managerial tools (i.e.
budget), hospital organization and training opportunities. We tasted and validated
both questionnaires and we assure the validity and reliability of the instrument.
We applied Factor Analysis to questionnaires to obtain the perception of managers
and employees in terms of the dimensions mentioned above. We performed descrip-
tive statistics, factor analysis, and two-tailed test to examine gender differences in
the General hospitals. We used STATA software for statistical analyses (Version12,
Stata Corp, College Station, TX).
3.4 Analysis
Respondents’ characteristics
Table 3.1 shows descriptive statistic. In public hospitals 17424 of the 34686 staff
(50.2%) returned the questionnaire while in private hospitals 1276 employees returned
it.
Organizational climate dimensions
Applying factor analysis to the data we obtained overall job satisfaction and four
organizational climate dimensions:
1. Satisfaction with managerial tools was measure by four items (α=0.94). Test-
ing the manager performance concerning to the budget responsibilities and
control system.
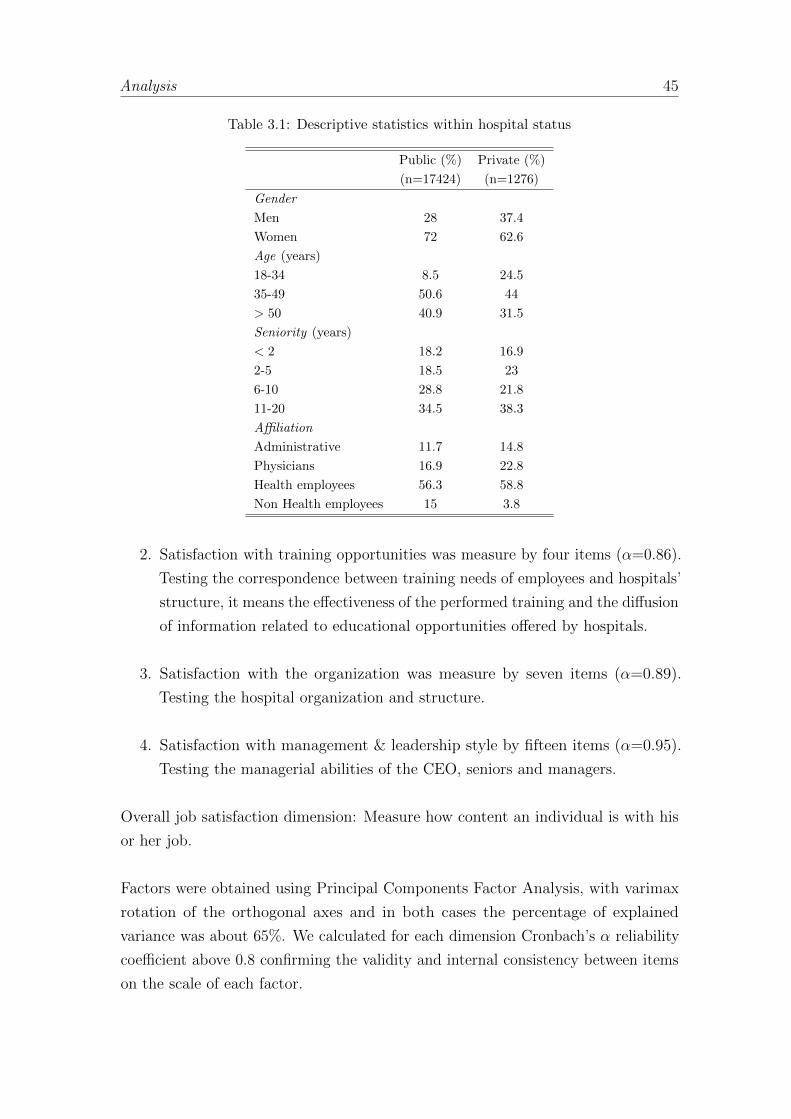
Analysis 45
Table 3.1: Descriptive statistics within hospital status
Public (%) Private (%)
(n=17424) (n=1276)
Gender
Men 28 37.4
Women 72 62.6
Age (years)
18-34 8.5 24.5
35-49 50.6 44
> 50 40.9 31.5
Seniority (years)
< 2 18.2 16.9
2-5 18.5 23
6-10 28.8 21.8
11-20 34.5 38.3
Affiliation
Administrative 11.7 14.8
Physicians 16.9 22.8
Health employees 56.3 58.8
Non Health employees 15 3.8
2. Satisfaction with training opportunities was measure by four items (α=0.86).
Testing the correspondence between training needs of employees and hospitals’
structure, it means the effectiveness of the performed training and the diffusion
of information related to educational opportunities offered by hospitals.
3. Satisfaction with the organization was measure by seven items (α=0.89).
Testing the hospital organization and structure.
4. Satisfaction with management & leadership style by fifteen items (α=0.95).
Testing the managerial abilities of the CEO, seniors and managers.
Overall job satisfaction dimension: Measure how content an individual is with his
or her job.
Factors were obtained using Principal Components Factor Analysis, with varimax
rotation of the orthogonal axes and in both cases the percentage of explained
variance was about 65%. We calculated for each dimension Cronbach’s α reliability
coefficient above 0.8 confirming the validity and internal consistency between items
on the scale of each factor.
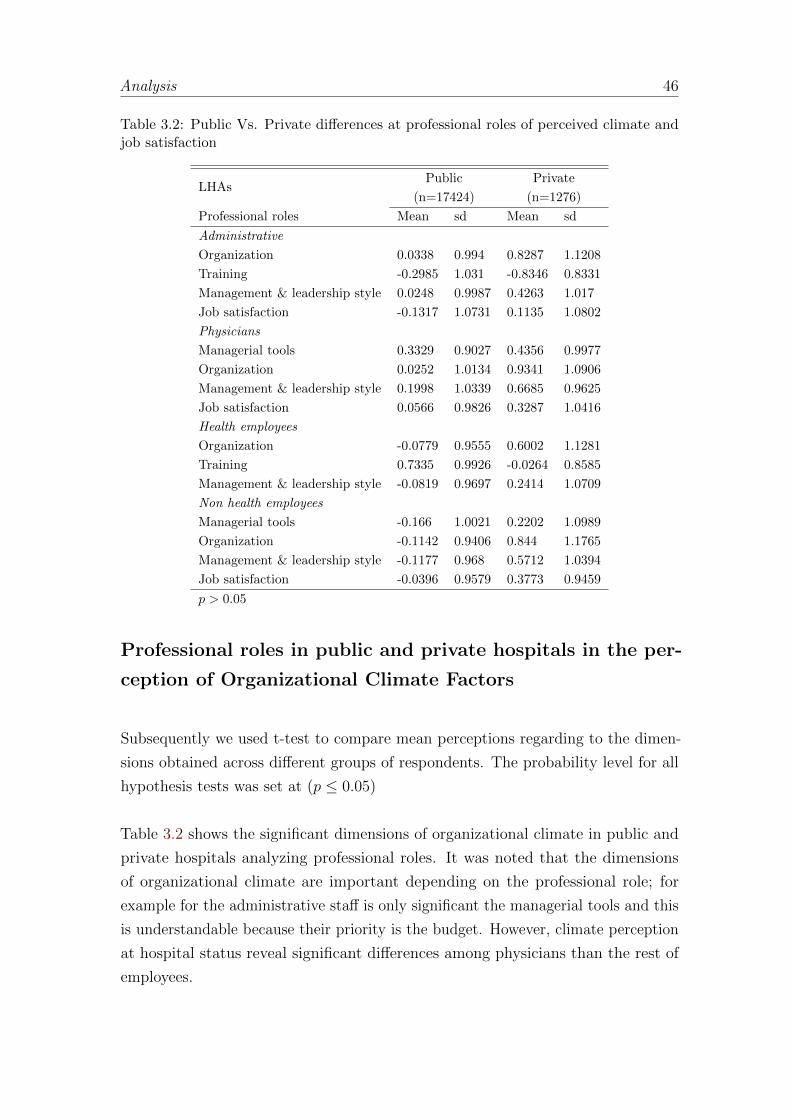
Analysis 46
Table 3.2: Public Vs. Private differences at professional roles of perceived climate andjob satisfaction
LHAsPublic Private
(n=17424) (n=1276)
Professional roles Mean sd Mean sd
Administrative
Organization 0.0338 0.994 0.8287 1.1208
Training -0.2985 1.031 -0.8346 0.8331
Management & leadership style 0.0248 0.9987 0.4263 1.017
Job satisfaction -0.1317 1.0731 0.1135 1.0802
Physicians
Managerial tools 0.3329 0.9027 0.4356 0.9977
Organization 0.0252 1.0134 0.9341 1.0906
Management & leadership style 0.1998 1.0339 0.6685 0.9625
Job satisfaction 0.0566 0.9826 0.3287 1.0416
Health employees
Organization -0.0779 0.9555 0.6002 1.1281
Training 0.7335 0.9926 -0.0264 0.8585
Management & leadership style -0.0819 0.9697 0.2414 1.0709
Non health employees
Managerial tools -0.166 1.0021 0.2202 1.0989
Organization -0.1142 0.9406 0.844 1.1765
Management & leadership style -0.1177 0.968 0.5712 1.0394
Job satisfaction -0.0396 0.9579 0.3773 0.9459
p > 0.05
Professional roles in public and private hospitals in the per-
ception of Organizational Climate Factors
Subsequently we used t-test to compare mean perceptions regarding to the dimen-
sions obtained across different groups of respondents. The probability level for all
hypothesis tests was set at (p ≤ 0.05)
Table 3.2 shows the significant dimensions of organizational climate in public and
private hospitals analyzing professional roles. It was noted that the dimensions
of organizational climate are important depending on the professional role; for
example for the administrative staff is only significant the managerial tools and this
is understandable because their priority is the budget. However, climate perception
at hospital status reveal significant differences among physicians than the rest of
employees.
Analysis 47
In general, staff working in private hospitals are more likely than those working in
public hospitals. Management & leadership style and organization are significant in
all professional roles regardless of the hospital status, but private hospitals staff are
more satisfy with both of them.
Satisfaction with the organization is the most significantly factor in private hospitals,
but at the same time the most critical one because of the higher gap between two
hospital status. Differences between public and private organizations have been
discussed broadly. The first difference is that private organizations are owned by
private partners while the nation is the owner of public organizations. Public sector
organizations are controlled mainly by the political forces, not market forces. For
this reason the main constraints are imposed by the political system, while in private
organizations, the owners have a direct monetary incentive to motivate managers to
provide better performance. Similarly, the managers themselves are likely to benefit
from improved performance, because their payment is linked with the profit.
The literature pointed out that there are several external aspects that make different
managing public organizations (Boyne, 2002; Arrow, 1974; Angelopoulou et al.,
1998; Bhatia and Cleland, 2004). Public hospitals are complex organizations, Met-
calfe (1993) argues that ’government operates through networks of interdependent
organizations rather than through independent organizations which simply pursue
their own objectives”. Moreover, in the public sector there is more bureaucracy
compared to the private one, also political conditions impacts the policy makers
changing the short-term outlook and pressing to achieve results so fast, results that
can help only for political purposes, whereas private organizations should pursue
the goal of profit.
The results with respect to Managerial & leadership style are significant in all
professional roles. Literature has shown that managerial & leadership style differ
significantly between private and public organizations, managers in private orga-
nizations are motivated more by their economic well-being (Khojasteh, 1993) and
public managers are more object-oriented and they have a desire to serve the public
interest and strongly oriented towards the ”common good”. Nevertheless, these
results support some studies that have found that public sector employees are less
satisfied with their work (Buchanan, 1974; Lachman, 1985).
Highly specialized staff responded more positively all items. Physicians and ad-
Conclusions 48
ministrative employees were more positive about how they perceived their hospital,
particularly the question about the adequacy of infrastructure and physical envi-
ronment.
Training opportunities is significantly less effective in private hospitals. Moreover
employees perceived that career opportunities are not equally guaranteed for all
and there is a lack of information about training opportunities provided by the
hospital. It seemed to be the most critical issue to be taken up.
We found the existence of a discreet difference in the perception of the managerial
tools among physicians and a large difference among non health employees. The
higher gap between professional roles concerned to the existence of a professional
hierarchy in healthcare well established in the literature.
3.5 Conclusions
The results of the present study support the hypothesis that there are differences in
how the organizational climate is perceived by employees within professional roles
and hospital status in the Tuscan healthcare organizations (General hospitals).
The analysis showed that the Tuscan organizational climate questionnaire is a
reliable instrument used as a measurement tool for evaluating working conditions
and determining the factors which satisfies and motivates employees in the health-
care sector. The four dimensions detected showed high variability and different
significance along diverse organizational structures, professional roles and hospital
status.
This study shows that there are major differences between public and private
hospitals in terms of how they perceive the internal climate where the employees in
private hospitals are more satisfied than employees in public ones. On the other
hand, our results suggest that in terms of job satisfaction physicians in private
institutions are in general more satisfied.
Training processes, however, within these organizations, are loosely coupled with
the rest of the organizational processes and often depend on the employee’s ability

Conclusions 49
and willing to ask for targeted training courses.
Finally the use of an organizational climate survey can help management to identify
the critical points in the factor dimensions and communicate more effectively within
the structures improving the effectiveness of total quality management programs.
In fact, a valid internal climate survey can be a useful tool in supporting the
management to make effective innovation process. Moreover, in order to assure its
effectiveness it is important to share and discuss the results of the internal climate
survey with all the professionals being this the most important prerequisite to
support the organizational changes and it is what the Tuscan health managers are
used to do not only with regards to the internal climate results but also to all the
performance measures.
4
Does feedback from patient-experiencesurveys change behavior of health
professionals and improvecommunication with patients? The
Italian experience. 1
Healthcare providers often solicit patient feedback through questionnaires. To
test if health-professional awareness of survey results improves communication
between patients and providers, we analyzed data from 26 Italian hospitals
that documented 8,942 organizational-climate questionnaires administered
in 2010 and 5,341 inpatient experiences in 2011. Statistical analysis showed
that patient experience index significantly improved by 0.35 points (scale:
0-100) when professionals’ knowledge of survey results increased by 1%.
These findings suggest that control systems should pay attention to the
dissemination phase of patient’s surveys among health professionals.
4.1 Introduction
Patient centeredness is seen as a strategic issue of health care systems and great
efforts are made to involve patient within the delivery process. Despite this great
relevance, patient satisfaction is not always included into the planning and control
1With: Anna Maria Murante, Milena Vainieri, Sabina Nuti and Diana Rojas.

Introduction 51
systems in health care because it is considered a difficult issue to be interpreted
(Fitzpatrick and Hopkins, 1983; Williams, 1994) and in turn linked to performance
of professionals and staff. More recently, new metrics have been devised that
incorporate the opinions that patients have about their experience in healthcare
settings (Patient Reported Experience Measure) and about outcome of care (Patient
Reported Outcome Measure). Such methods allow monitoring of process and
outcome during care (Coulter et al., 2009).
Some organizations have adopted multidimensional performance evaluation systems
and have included surveys measuring quality through the patient perspective
(Giordano et al., 2010) as well as comparisons of their results among organizations.
The working assumption in this process is that awareness of the opinions of patients
is a critical issue to be considered in order to strengthen weak areas of service and
thus enhance performance. Hence the systematic monitoring of patient experience
helps organizations to assess if health professionals, so informed of the patient’s
points of view, have adopted effective actions to improve quality of care.
However, survey of patient experience is not sufficient to induce change in behavior
of health professionals and staff. Indeed, Flamholtz et al. (1985) identified a number
of factors that affect organizational performance. Extrinsic factors such as culture
or climate influence performance while other factors are strictly linked to the
management-control system adopted by the organization. The measurement is only
one of the four control core mechanisms, the others are: planning, feedback and
evaluation. In fact, once the phenomenon is measured a critical role is played by
the feedback process.
Feedback in terms of how many employees are aware of their performance in health
care literature has been investigated indirectly: most of the studies in health care
include feedback into the measurement phase or into the public disclosure of data.
Indeed public disclosure can be considered as a way to give back results or feedback.
Reviews and studies on public disclosure in health care generally consider that the
public release is able to empower accountability (Fung et al., 2008) working with the
reputational damage of hospitals and professionals (Hibbard et al., 2005). Moreover,
some authors believe that public reporting reveals provider performance to patients
and thus allows patients to make informed choices (Schauffler and Mordavsky,
2001; Faber et al., 2009; Hibbard and Sofaer, 2010; Øvretveit, 1996). Others stress

Study Data And Methods 52
public disclosure heightens awareness that healthcare workers have of their own
performance which in turn stimulates quality-improvement efforts in health services
(Barr et al., 2006; Laschober et al., 2007; Hibbard et al., 2003; Elliott et al., 2010).
Our study further explores the relationship between feedback and task performance
with a special emphasis on analysis of inpatient survey data that have been disclosed
for public scrutiny. In particular, this study aims to quantify the impact of
professional awareness of patient experience surveys on the communication process;
we focus on communication because previous works have shown that communication
is the main component of patient satisfaction (Sitzia and Wood, 1997).
4.2 Study Data And Methods
In Italy there are few regional healthcare systems that include patient-survey
results in their performance evaluation systems. Regions such as Tuscany, for
example, return survey results directly to providers, while other Regions who
administer surveys do not incorporate patient feedback into the processes of setting
organizational priorities or establishing targets (Vainieri and Nuti, 2011).
As part of a multidimensional performance evaluation system that began in 2004,
Tuscany has periodically surveyed patient experience and employee opinion of
regional health services. This evaluation system monitors 130 indicators of health-
provider performance and is currently used, respectively, by regional administrators
and local managers to set organizational targets and to align budgets. Moreover,
data are reported in comparison and are also publicly disclosed via a website
(http://performance.sssup.it/toscana/) and annual reports (Nuti, 2008; Nuti et al.,
2009).
Fifteen of the indicators elucidate patient evaluation and experience with health
services such as primary care, emergency department service, home care, hospital
service, maternal care, and elderly services. Six of the remaining indicators relate
to the nature of the professional climate perceived by employees and thus focus on
worker training, relationships between workers and managers, and communication
within the organization and between employees. Both patient and worker surveys
are administered every two years according to the planning cycle and control scheme.
Study Data And Methods 53
In this study, we used data from the climate survey administered in 2010 and
the inpatient survey conducted in 2011. We investigated whether patients in 2011
showed improved inpatient experiences in those hospitals where one year before
healthcare workers reported to be more informed about the most recent survey of
inpatient experience.
Our analysis only considers data from each of the 26 general hospitals within
Tuscany that in the biennium 2010-2011 administered both patient and employee
surveys.
4.2.1 Surveys
In 2010, each of the 14,800 health professionals working among the 26 Tuscan
general hospitals was asked to answer the 80-question organizational-climate survey.
Questionnaires were administered on-line using the Computer Assisted Web Inter-
viewing technique (Pizzini and Furlan, 2012), and along with queries related to
involvement, communication, training and budgeting procedure, respondents were
also asked to comment on the extent to which they felt (on a 1-5 scale, where 1 is
’not at all’ and 5 is ’completely’) to be aware of patient-survey results.
We can address at least two limitations to organizational-climate survey. The first
concerns the well-known selection bias for organizational climate survey that occurs
when survey participation is voluntary (Brick, 2011). The second limitation is
that we were unable to separately survey healthcare professionals who had direct
relationship with patients during treatment from the other ones. For instance, we
cannot separately identified in our database pharmacists and laboratory specialists
and measure their indirect influence on the overall hospital experience of patients.
However, the proportion of all healthcare workers represented by these professions
is small relative to the total size of the sampled workers and thus any statistical
bias introduced thereby is probably slight.
In the following year the Inpatient Experience questionnaire (Murante et al., 2013)
was administered at home by mail, and on demand by phone or web, to patients
discharged by the 26 Tuscan general hospitals. Eligible patients were age 18
or older and had an inpatient stay of at least one night for medical, surgical, or

Study Data And Methods 54
maternity care. About 20,200 inpatients were invited to answer 32 questions on their
hospitalization experience (reporting style questions), 4 questions regarding overall
evaluations of their hospitalization (rating style questions), and 7 questions related
to patient socio-demographic characteristics including age, gender, educational level,
self-reported health status, job position, reports of chronic disease, and history of
previous hospitalization.
4.2.2 Measures
In accord with a patient-centred approach to healthcare, communication has to be
oriented to patient needs and has to allow patients and their families to participate
in medical decisions (Epstein et al., 2005; Brown, 1999). Thus, to examine the
extent to which communication between patients and professionals (e.g., physicians
or nurses), is better experienced in hospitals where healthcare workers are more
informed about patient feedback, we devised an indicator of Patient Experience
with Communication (PEC) process. In the PEC we considered nine items from
inpatient survey data: (i) information received during admission; (ii) the clearness
of answers from doctors and (iii) nurses; (iv) information about health status and
treatment; (v) information about treatment effects; (vi) information received by
the patients’ family members; (vii) privacy during consultation; (viii) concordance
of information received during hospitalization; and (ix) information received at
hospital discharge. They were report style questions (i.e., responses were ’never’,
’sometimes’ and ’always’ or ’no’,’partially’ and ’completely’).
The PEC indicator was created by averaging the score of each item after trans-
formation to a 0-100 scale with higher scores indicating a more satisfying patient
experience (Brown et al., 2008). The high loadings of factor analysis and the robust
Cronbach’s alpha reliability coefficient confirms the validity and reliability of the
PEC measure (see Appendix).
We next used results from the organizational-climate survey to measure healthcare
worker knowledge of inpatient views. Specifically, we asked health professionals the
question, ’Are you informed about findings from the patient-experience survey?’. As
above, 1-5 point likert scales were transformed to a 0-100 scale with higher scores
indicating a more substantial level of knowledge.

Study Results 55
4.2.3 Analyses
We performed a multilevel analysis to test if PEC varies across hospitals and the
extent to which patient experience is influenced by patient socio-demographics
characteristics such as age, gender, education, health status and hospitalization
ward (at patient level), and the level of healthcare worker knowledge of patient
feedback (at hospital level).
We used multilevel statistical modeling (Bosker and Snijders, 1999) because it
elucidates effects of both individual characteristics and hospital factors on patient
experience. Specifically, patients at the lower level of analysis are nested within
hospitals at the higher level. Due to this hierarchical structure we can therefore
estimate variability in patient experience within each hospital and among hospitals.
Thus, statistical adjustment for hospital characteristics permits comparison of
patient experiences among organizations.
4.3 Study Results
1. Patient experience with communication. Of the total 5,341 inpatients who
returned a completed questionnaire (26% response rate), 62% were women
and 57% had no more than a primary or secondary-school level of education.
Respondents were on average 55 years old and reported a fair (55%) or a good
(33%) perception of their health status versus a bad perception (12%), and
reported at least one stay in a surgical ward.
The PEC index in Figure 4.2 shows an average value of patient experience
of medium-high (mean = 80; SD = 19. In practice, inpatient reported that
nurses and doctors provide concordant information to patients and further
information were provided at discharge about medical therapy and how
to manage one’s own health status at home. However, patients perceive
that less effort is invested in providing information at admission and during
hospitalization about health status and about treatment effects (Table 4.1).
A larger variability is observed in the extent to which patients perceive the
effectiveness of communication at these stages of hospitalization.
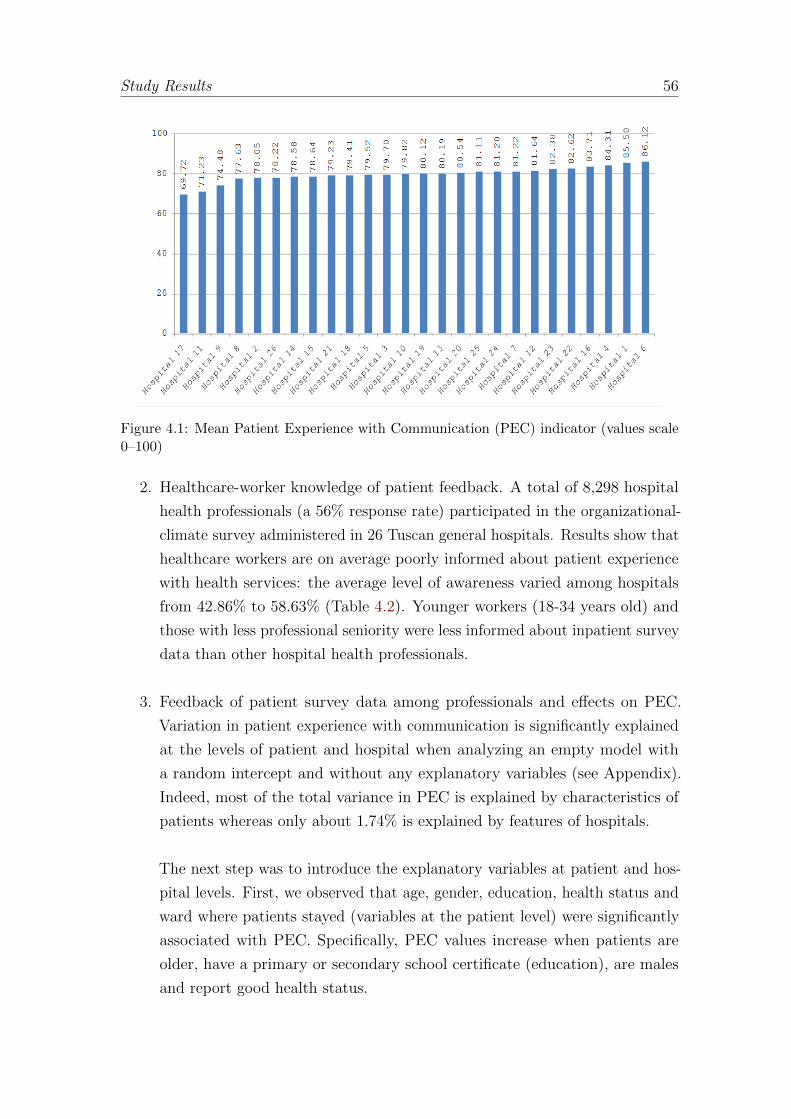
Study Results 56
Figure 4.1: Mean Patient Experience with Communication (PEC) indicator (values scale0–100)
2. Healthcare-worker knowledge of patient feedback. A total of 8,298 hospital
health professionals (a 56% response rate) participated in the organizational-
climate survey administered in 26 Tuscan general hospitals. Results show that
healthcare workers are on average poorly informed about patient experience
with health services: the average level of awareness varied among hospitals
from 42.86% to 58.63% (Table 4.2). Younger workers (18-34 years old) and
those with less professional seniority were less informed about inpatient survey
data than other hospital health professionals.
3. Feedback of patient survey data among professionals and effects on PEC.
Variation in patient experience with communication is significantly explained
at the levels of patient and hospital when analyzing an empty model with
a random intercept and without any explanatory variables (see Appendix).
Indeed, most of the total variance in PEC is explained by characteristics of
patients whereas only about 1.74% is explained by features of hospitals.
The next step was to introduce the explanatory variables at patient and hos-
pital levels. First, we observed that age, gender, education, health status and
ward where patients stayed (variables at the patient level) were significantly
associated with PEC. Specifically, PEC values increase when patients are
older, have a primary or secondary school certificate (education), are males
and report good health status.
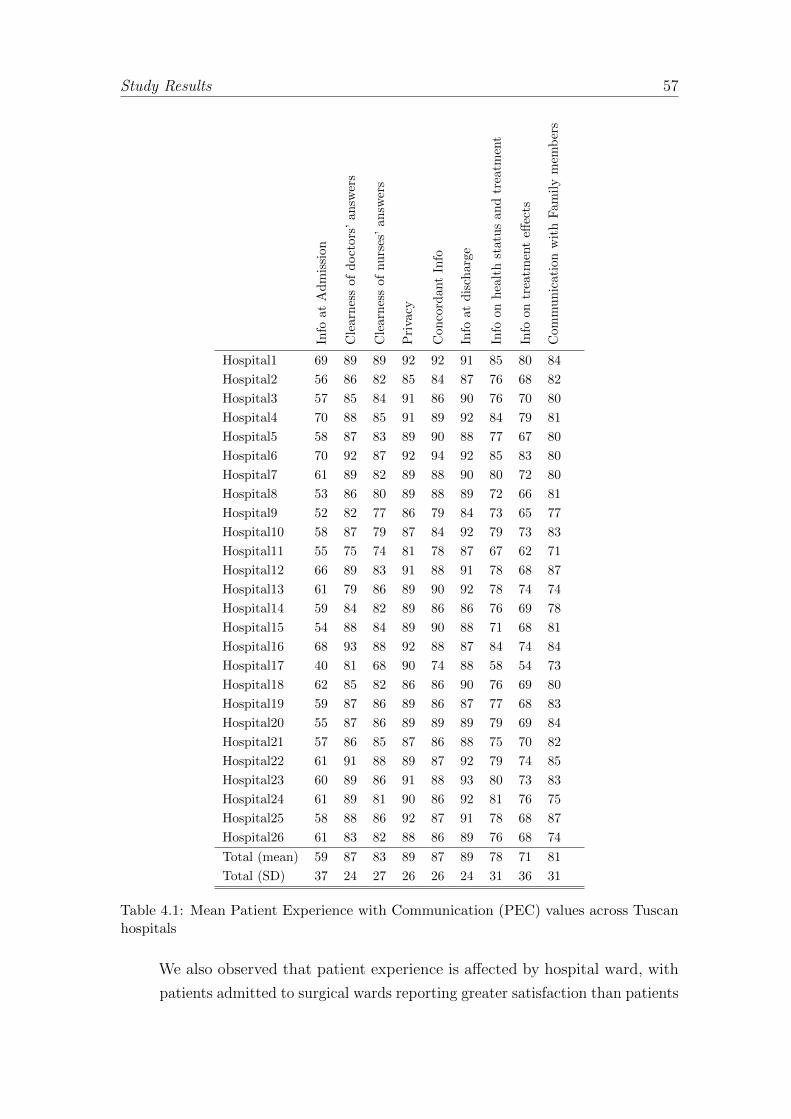
Study Results 57
Info
atA
dm
issi
on
Cle
arn
ess
ofd
oct
ors
’an
swer
s
Cle
arn
ess
ofnu
rses
’an
swer
s
Pri
vacy
Con
cord
ant
Info
Info
atd
isch
arge
Info
onh
ealt
hst
atu
san
dtr
eatm
ent
Info
ontr
eatm
ent
effec
ts
Com
mu
nic
atio
nw
ith
Fam
ily
mem
ber
s
Hospital1 69 89 89 92 92 91 85 80 84
Hospital2 56 86 82 85 84 87 76 68 82
Hospital3 57 85 84 91 86 90 76 70 80
Hospital4 70 88 85 91 89 92 84 79 81
Hospital5 58 87 83 89 90 88 77 67 80
Hospital6 70 92 87 92 94 92 85 83 80
Hospital7 61 89 82 89 88 90 80 72 80
Hospital8 53 86 80 89 88 89 72 66 81
Hospital9 52 82 77 86 79 84 73 65 77
Hospital10 58 87 79 87 84 92 79 73 83
Hospital11 55 75 74 81 78 87 67 62 71
Hospital12 66 89 83 91 88 91 78 68 87
Hospital13 61 79 86 89 90 92 78 74 74
Hospital14 59 84 82 89 86 86 76 69 78
Hospital15 54 88 84 89 90 88 71 68 81
Hospital16 68 93 88 92 88 87 84 74 84
Hospital17 40 81 68 90 74 88 58 54 73
Hospital18 62 85 82 86 86 90 76 69 80
Hospital19 59 87 86 89 86 87 77 68 83
Hospital20 55 87 86 89 89 89 79 69 84
Hospital21 57 86 85 87 86 88 75 70 82
Hospital22 61 91 88 89 87 92 79 74 85
Hospital23 60 89 86 91 88 93 80 73 83
Hospital24 61 89 81 90 86 92 81 76 75
Hospital25 58 88 86 92 87 91 78 68 87
Hospital26 61 83 82 88 86 89 76 68 74
Total (mean) 59 87 83 89 87 89 78 71 81
Total (SD) 37 24 27 26 26 24 31 36 31
Table 4.1: Mean Patient Experience with Communication (PEC) values across Tuscanhospitals
We also observed that patient experience is affected by hospital ward, with
patients admitted to surgical wards reporting greater satisfaction than patients
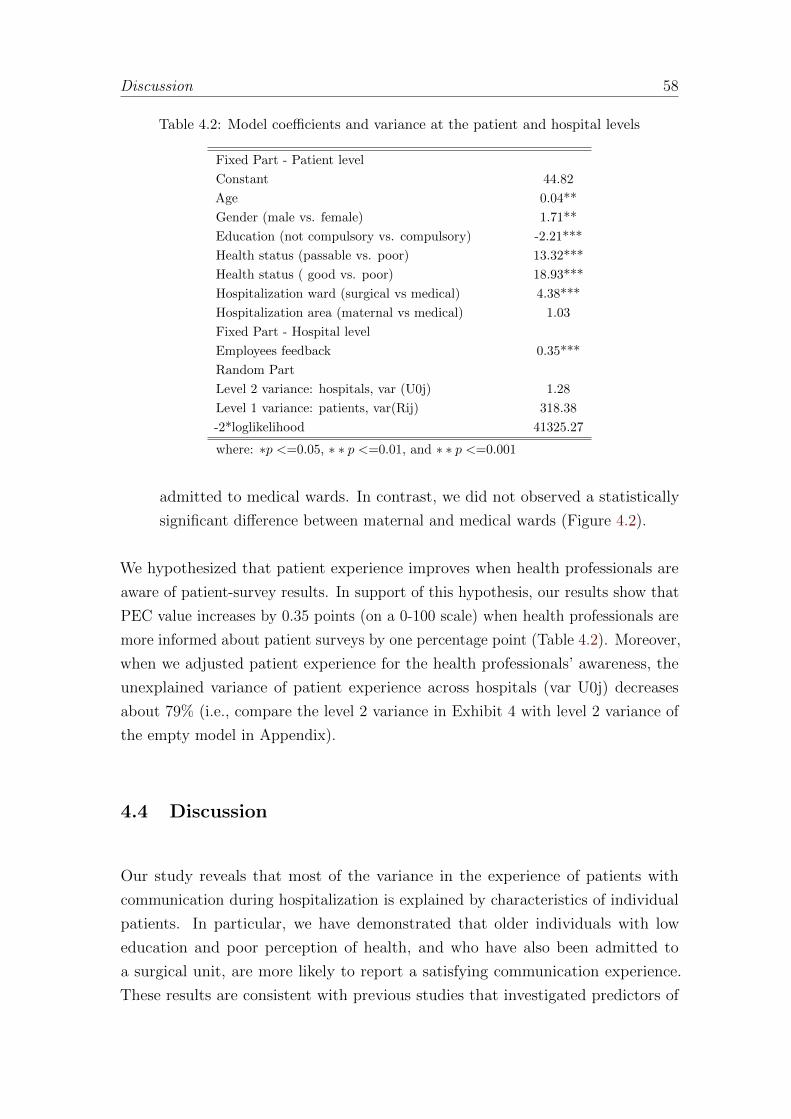
Discussion 58
Table 4.2: Model coefficients and variance at the patient and hospital levels
Fixed Part - Patient level
Constant 44.82
Age 0.04**
Gender (male vs. female) 1.71**
Education (not compulsory vs. compulsory) -2.21***
Health status (passable vs. poor) 13.32***
Health status ( good vs. poor) 18.93***
Hospitalization ward (surgical vs medical) 4.38***
Hospitalization area (maternal vs medical) 1.03
Fixed Part - Hospital level
Employees feedback 0.35***
Random Part
Level 2 variance: hospitals, var (U0j) 1.28
Level 1 variance: patients, var(Rij) 318.38
-2*loglikelihood 41325.27
where: ∗p <=0.05, ∗ ∗ p <=0.01, and ∗ ∗ p <=0.001
admitted to medical wards. In contrast, we did not observed a statistically
significant difference between maternal and medical wards (Figure 4.2).
We hypothesized that patient experience improves when health professionals are
aware of patient-survey results. In support of this hypothesis, our results show that
PEC value increases by 0.35 points (on a 0-100 scale) when health professionals are
more informed about patient surveys by one percentage point (Table 4.2). Moreover,
when we adjusted patient experience for the health professionals’ awareness, the
unexplained variance of patient experience across hospitals (var U0j) decreases
about 79% (i.e., compare the level 2 variance in Exhibit 4 with level 2 variance of
the empty model in Appendix).
4.4 Discussion
Our study reveals that most of the variance in the experience of patients with
communication during hospitalization is explained by characteristics of individual
patients. In particular, we have demonstrated that older individuals with low
education and poor perception of health, and who have also been admitted to
a surgical unit, are more likely to report a satisfying communication experience.
These results are consistent with previous studies that investigated predictors of

Discussion 59
Figure 4.2: Awareness of inpatient survey data among health professionals in Tuscanhospitals.
patient experience with hospital care (Murante et al., 2013; Veenstra and Hofoss,
2003; Stubbe et al., 2007).
Our findings also suggest that organizational factors influence communication
within hospitals. The effect of hospital context, which was revealed statistically
as moderate but significant variance in PEC among hospitals, indicates that the
systems of communication differ among hospitals and may be explained by variation
in methods of processing patients at admission and discharge (e.g., during processing
some hospitals may provide more information regarding care than others). Thus,
patient feedback plays a pivotal role in improving quality in the hospitals, where the
more effort that hospitals make in conveying the patient’s point of view to health
professionals, the better the experience on communication by patients. Indeed,
after taking into account the hospital characteristics, almost 80% of the variance
in patient-communication experience at hospital level is explained by feedback of
survey data to health professionals. We hypothesize that feedback facilitates change
in behavior of professionals by providing the information necessary for self-corrective
action.
It should be noted that even thought the survey data studied here has a focus
on average results at hospital level, in practice, survey results are transmitted to
healthcare professionals also comparing hospital wards. We suggest that future
studies account for more complex institutional structure than we analyzed here and
that more attention be devoted to directing survey results at the lower levels of
organization where feedback effects may be more powerful (Hekkert et al., 2009).

Conclusion 60
The proportion of health professionals who received feedback regarding patient-
survey results varied across health providers (from 43% to 59%). However, our
analysis shows that increasing awareness of survey results by only 1% among
health professionals has a statistically significant effect on patient experience with
communication. Since the PEC indicator was composed of factors related to
continuity and coordination of care, the effects of circulating patient surveys among
professionals may not only improve the experience of patients but may also stimulate
more professional assistance.
Future studies should consider the way to better communicate survey-feedback and
improve the awareness of patient experience by health professional. For instance, it
would have a different impact whether results are distributed by request to interested
professionals or if surveys are received as part of routine but unsolicited reports
on patient experience. Such differences in survey-feedback methodologies could
account for variation among hospitals in survey awareness which, in turn, explains
variation in patient satisfaction. Indeed, (Nuti et al., 2009) found that employees
who request feedback (i.e., the inquiry method) enhance performance more than
employees who do not make such requests or those who receive unsolicited reports
(i.e., the monitoring method).
Finally, this study confirms the value of multilevel modeling as a tool for exploring
the sources of variation in patient experience. This study estimates the influence
of hospitals and patient characteristics on communication process as perceived by
patient that are likely to be more realistic than results from previously published,
single-level studies.
4.5 Conclusion
This paper establishes a statistical link between the opinions that patients hold
about healthcare services and the extent to which health professionals are aware of
and modify their behavior in response to such opinions. Previous work has shown
that communication is the most important component of patient satisfaction,2 and
our analysis further demonstrates that patient perception of communication, in
terms of adequacy and effectiveness, depends on characteristics of both patients
2Regional Law 40 (2005).

Conclusion 61
and hospitals. Although characteristics such as age, gender and health status
strongly affect patient experience results, institutional features of hospitals also play
a moderate but statistically significant role in explaining the variance in patient
opinions about the quality of communication they received from health professionals.
Perhaps most striking is the result showing that a relatively minor increase in aware-
ness among doctors and nurses of patient opinion surveys has consistent feedback
effects on patient satisfaction. Given the benefits of improved patient experience,
planners and hospital administrators might wish to enhance and expand their
schemes for informing their staffs about patient opinion. When health professionals
are aware of evidence regarding the quality of communication perceived by patients,
they are better able to focus their efforts on improving the quality of care.
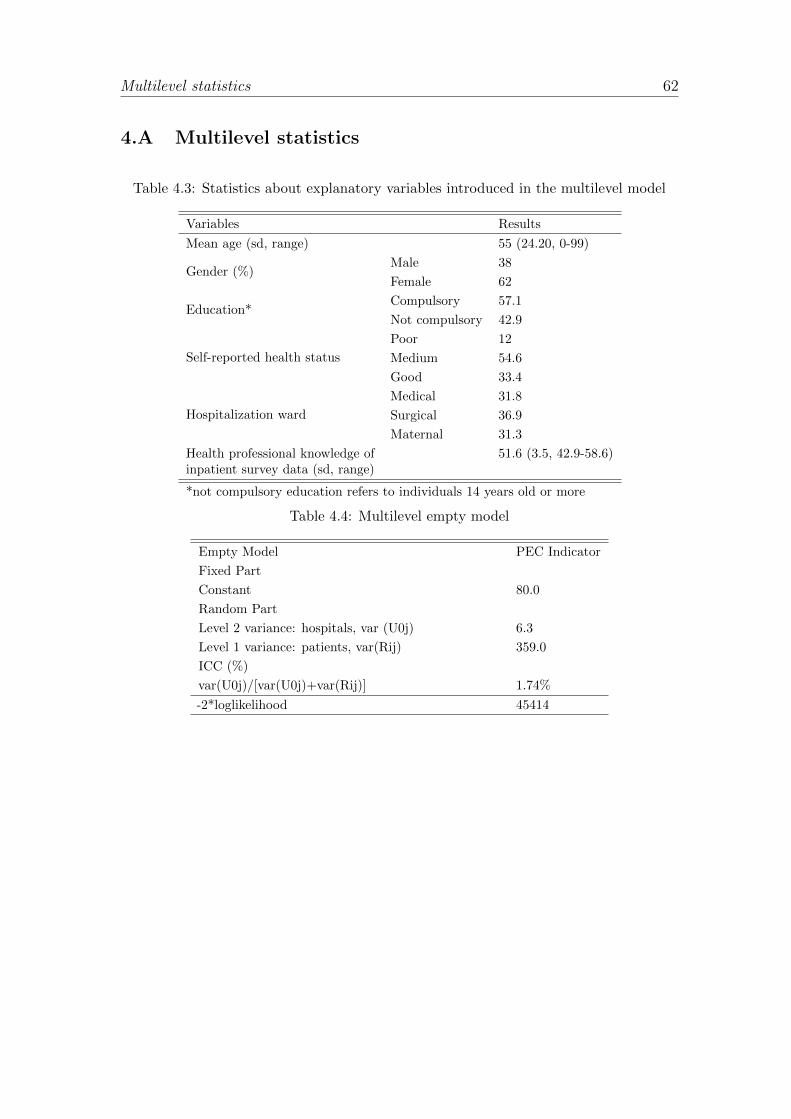
Multilevel statistics 62
4.A Multilevel statistics
Table 4.3: Statistics about explanatory variables introduced in the multilevel model
Variables Results
Mean age (sd, range) 55 (24.20, 0-99)
Gender (%)Male 38
Female 62
Education*Compulsory 57.1
Not compulsory 42.9
Self-reported health status
Poor 12
Medium 54.6
Good 33.4
Hospitalization ward
Medical 31.8
Surgical 36.9
Maternal 31.3
Health professional knowledge ofinpatient survey data (sd, range)
51.6 (3.5, 42.9-58.6)
*not compulsory education refers to individuals 14 years old or more
Table 4.4: Multilevel empty model
Empty Model PEC Indicator
Fixed Part
Constant 80.0
Random Part
Level 2 variance: hospitals, var (U0j) 6.3
Level 1 variance: patients, var(Rij) 359.0
ICC (%)
var(U0j)/[var(U0j)+var(Rij)] 1.74%
-2*loglikelihood 45414

Bibliography
Anderson, C. S. (1982). The search for school climate: A review of the research.
Review of educational research 52 (3), 368–420.
Angelopoulou, P., P. Kangis, and G. Babis (1998). Private and public medicine: a
comparison of quality perceptions. International Journal of Health Care Quality
Assurance 11 (1), 14–20.
Antonini, L. and A. Pin (2009). The italian road to fiscal federalism. Ital J Public
Law 1, 16.
Appelbaum, S. H. (1984). The organizational climate audit or how healthy is your
hospital? Hospital & health services administration 29 (1), 51.
Argyris, C. (1958). Some problems in conceptualizing organizational climate: A
case study of a bank. Administrative Science Quarterly , 501–520.
Arrow, K. (1974). The limits of organization.
Barbera-Tomas, D., F. Jimenez-Saez, and I. Castello-Molina (2011). Mapping the
importance of the real world: The validity of connectivity analysis of patent
citations networks. Research Policy 40 (3), 473–486.
Barr, J. K., T. E. Giannotti, S. Sofaer, C. E. Duquette, W. J. Waters, and M. K.
Petrillo (2006). Using public reports of patient satisfaction for hospital quality
improvement. Health services research 41 (3p1), 663–682.
Beveridge, B. W. H. B. (1942). Social insurance and allied services, Volume 6404.
Macmillan.
Bhatia, J. and J. Cleland (2004). Health care of female outpatients in south-
central india: Comparing public and private sector provision. Health Policy and
Planning 19 (6), 402–409.
Bosker, R. and T. Snijders (1999). Multilevel analysis: An introduction to basic
and advanced multilevel modeling. New York .
Box, R. C. (1999). Running government like a business implications for public
administration theory and practice. The American Review of Public Administra-
tion 29 (1), 19–43.
Boyne, G. A. (2002). Public and private management: whats the difference? Journal
of management studies 39 (1), 97–122.
Branin, J. J. (2009). Career attainment among healthcare executives: Is the gender
gap narrowing?. In Forum on Public Policy Online, Volume 2009. ERIC.
Brick, J. M. (2011). The future of survey sampling. Public opinion quarterly 75 (5),
872–888.
Broadbridge, A. (2010). Social capital, gender and careers: evidence from retail se-
nior managers. Equality, Diversity and Inclusion: An International Journal 29 (8),
815–834.
Brown, A. and R. Payne (1990). A human resource approach to the management of
organisational culture. Manchester Business School.
Brown, A. D., G. A. Sandoval, M. Murray, and B. Boissonnault (2008). Comparing
patient reports about hospital care across a Canadian-US border. International
Journal for Quality in Health Care 20 (2), 95–104.
Brown, S. J. (1999). Patient-centered communication. Annual review of nursing
research 17 (1), 85–104.
Brown, S. P. and T. W. Leigh (1996). A new look at psychological climate and
its relationship to job involvement, effort, and performance. Journal of applied
psychology 81 (4), 358.
Buchanan, B. (1974). Government managers, business executives, and organizational
commitment. Public Administration Review , 339–347.
Burke, R., L. Divinagracia, and E. Mamo (1998). Supervisors’ support received by
women managers: Country and sex of supervisors. Psychological reports 83 (1),
12–14.
Burke, W. W. and G. H. Litwin (1992). A causal model of organizational performance
and change. Journal of management 18 (3), 523–545.
Carinci, F., G. Caracci, F. Di Stanislao, and F. Moirano (2012). Performance
measurement in response to the tallinn charter: Experiences from the decentralized
italian framework. Health Policy .
Carli, L. L. and A. H. Eagly (2001). Gender, hierarchy, and leadership: An
introduction. Journal of Social Issues 57 (4), 629–636.
Carlucci, D., G. Schiuma, F. Sole, and R. Linzalone (2009). Assessing and managing
climate into healthcare organizations. In Proceedings of the International Scientific
Conference Insights into the sustainable growth of business, pp. 19–21.
Censis (2008). I modelli decisionali nella sanita locale.
Clark, K. B. (1985). The interaction of design hierarchies and market concepts in
technological evolution. Research policy 14 (5), 235–251.
Clarke, S. P., D. M. Sloane, and L. H. Aiken (2002). Effects of hospital staffing
and organizational climate on needlestick injuries to nurses. American Journal of
Public Health 92 (7), 1115–1119.
Commission, E. et al. (2010). Europe in figures. Eurostat yearbook .
Coulter, A., R. Fitzpatrick, and J. Cornwell (2009). Measures of patients’ experience
in hospital: purpose, methods and uses. King’s Fund.

Cumbey, D. A. and J. W. Alexander (1998). The relationship of job satisfac-
tion with organizational variables in public health nursing. Journal of Nursing
Administration 28 (5), 39–46.
Dawson, J. F., V. Gonzalez-Roma, A. Davis, and M. A. West (2008). Organizational
climate and climate strength in uk hospitals. European Journal of Work and
Organizational Psychology 17 (1), 89–111.
DeCotiis, T. A. and T. P. Summers (1987). A path analysis of a model of the an-
tecedents and consequences of organizational commitment. Human relations 40 (7),
445–470.
Denison, D. R. (1996). What is the difference between organizational culture and
organizational climate? a native’s point of view on a decade of paradigm wars.
Academy of Management review 21 (3), 619–654.
Dosi, G. (1982). Technological paradigms and technological trajectories: a suggested
interpretation of the determinants and directions of technical change. Research
policy 11 (3), 147–162.
Douglas, T. J. and J. A. Ryman (2003). Understanding competitive advantage
in the general hospital industry: Evaluating strategic competencies. Strategic
Management Journal 24 (4), 333–347.
Drexler, J. A. (1977). Organizational climate: Its homogeneity within organizations.
Journal of Applied Psychology 62 (1), 38.
Eagly, A. H. (1987). Sex differences in social behavior: A social-role interpretation.
Psychology Press.
Eagly, A. H. and M. C. Johannesen-Schmidt (2001). The leadership styles of women
and men. Journal of Social Issues 57 (4), 781–797.
Elliott, M. N., W. G. Lehrman, E. H. Goldstein, L. A. Giordano, M. K. Beckett,
C. W. Cohea, and P. D. Cleary (2010). Hospital survey shows improvements in
patient experience. Health Affairs 29 (11), 2061–2067.
Epstein, R. M., P. Franks, K. Fiscella, C. G. Shields, S. C. Meldrum, R. L. Kravitz,
and P. R. Duberstein (2005). Measuring patient-centered communication in
patient–physician consultations: theoretical and practical issues. Social science
& medicine 61 (7), 1516–1528.
Faber, M., M. Bosch, H. Wollersheim, S. Leatherman, and R. Grol (2009). Public
reporting in health care: How do consumers use quality-of-care information?: A
systematic review. Medical care 47 (1), 1–8.
Fitzpatrick, R. and A. Hopkins (1983). Problems in the conceptual framework of
patient satisfaction research: an empirical exploration. Sociology of health &
illness 5 (3), 297–311.

Flamholtz, E. G., T. Das, and A. S. Tsui (1985). Toward an integrative framework
of organizational control. Accounting, Organizations and Society 10 (1), 35–50.
Fontana, R., A. Nuvolari, and B. Verspagen (2009). Mapping technological trajecto-
ries as patent citation networks. an application to data communication standards.
Economics of Innovation and New Technology 18 (4), 311–336.
Forehand, G. A. and G. Von Haller (1964). Environmental variation in studies of
organizational behavior. Psychological bulletin 62 (6), 361.
Fung, C. H., Y.-W. Lim, S. Mattke, C. Damberg, and P. G. Shekelle (2008).
Systematic review: the evidence that publishing patient care performance data
improves quality of care. Annals of internal medicine 148 (2), 111–123.
Gershon, R. R., P. W. Stone, S. Bakken, and E. Larson (2004). Measurement of
organizational culture and climate in healthcare. Journal of Nursing Administra-
tion 34 (1), 33–40.
Giordano, L. A., M. N. Elliott, E. Goldstein, W. G. Lehrman, and P. A. Spencer
(2010). Development, implementation, and public reporting of the hcahps survey.
Medical Care Research and Review 67 (1), 27–37.
Glick, W. H. (1985). Conceptualizing and measuring organizational and psychologi-
cal climate: Pitfalls in multilevel research. Academy of Management review 10 (3),
601–616.
Goleman, D. (2000). Leadership that gets results. Harvard business review 78 (2),
78–93.
Gray, R. (2004). How people work: And how you can help them to give their best.
Pearson Education.
Guion, R. M. (1973). A note on organizational climate. Organizational Behavior
and Human Performance 9 (1), 120–125.
Habersam, M. and M. Piber (2003). Exploring intellectual capital in hospitals: two
qualitative case studies in italy and austria. European Accounting Review 12 (4),
753–779.
Hall, L. M., D. Doran, S. Sidani, and L. Pink (2006). Teaching and community
hospital work environments. Western journal of nursing research 28 (6), 710–725.
Harriman, A. (1996). Women Men Management. Greenwood Publishing Group.
Hekkert, K. D., S. Cihangir, S. M. Kleefstra, B. van den Berg, and R. B. Kool
(2009). Patient satisfaction revisited: a multilevel approach. Social science &
medicine 69 (1), 68–75.
Herzberg, F., B. Mausner, and B. B. Snyderman (1959). The motivation to work.
1959. A la recherche des motivations perdues .
Hibbard, J. and S. Sofaer (2010). Best practices in public reporting no. 1: How
to effectively present health care performance data to consumers. Agency for
Healthcare Research and Quality .
Hibbard, J. H., J. Stockard, and M. Tusler (2003). Does publicizing hospital
performance stimulate quality improvement efforts? Health Affairs 22 (2), 84–94.
Hibbard, J. H., J. Stockard, and M. Tusler (2005). Hospital performance reports:
impact on quality, market share, and reputation. Health Affairs 24 (4), 1150–1160.
Hofstede, G., G. J. Hofstede, and M. Minkov (1991). Cultures and organizations:
Software of the mind, Volume 2. McGraw-Hill London.
House, R. J. and L. A. Wigdor (1967). Herzberg’s dual-factor theory of job
satisfaction and motivation: a review of the evidence and a criticism. Personnel
Psychology 20 (4), 369–390.
Hummon, N. P. and P. Dereian (1989). Connectivity in a citation network: The
development of dna theory. Social Networks 11 (1), 39–63.
Jackson-Malik, P. J. (2005). Organizational climate and hospital nurses’ job
satisfaction, burnout, and intent to leave.
James, L. A. and L. R. James (1989). Integrating work environment perceptions: Ex-
plorations into the measurement of meaning. Journal of Applied Psychology 74 (5),
739.
James, L. R. (1982). Aggregation bias in estimates of perceptual agreement. Journal
of applied psychology 67 (2), 219.
James, L. R. and A. P. Jones (1974). Organizational climate: A review of theory
and research. Psychological bulletin 81 (12), 1096.
James, L. R. and A. P. Jones (1980). Perceived job characteristics and job satis-
faction: An examination of reciprocal causation. Personnel Psychology 33 (1),
97–135.
James, L. R., W. F. Joyce, and J. W. Slocum (1988). Comment: Organizations do
not cognize. Academy of Management Review 13 (1), 129–132.
James, L. R. and L. E. Tetrick (1986). Confirmatory analytic tests of three
causal models relating job perceptions to job satisfaction. Journal of Applied
Psychology 71 (1), 77.
Jones, A. P. and L. R. James (1979). Psychological climate: Dimensions and relation-
ships of individual and aggregated work environment perceptions. Organizational
behavior and human performance 23 (2), 201–250.
Joyce, W. F. and J. W. Slocum (1979). Climates in organizations. Organizational
behavior 317, 333.
Judge, T. A., C. J. Thoresen, J. E. Bono, and G. K. Patton (2001). The job
satisfaction–job performance relationship: A qualitative and quantitative review.

Psychological bulletin 127 (3), 376.
Kangis, P., D. Gordon, and S. Williams (2000). Organisational climate and corporate
performance: an empirical investigation. Management Decision 38 (8), 531–540.
Kettl, D. F. (2000). Public administration at the millennium: The state of the field.
Journal of public administration research and theory 10 (1), 7–34.
Khojasteh, M. (1993). Motivating the private vs. public sector managers. Public
Personnel Management 22 (3), 391–401.
Kilmann, R. H., M. J. Saxton, and R. Serpa (1985). Gaining control of the corporate
culture. Jossey-Bass Inc Pub.
Koffka, K. (1935). Principles of gestalt psychology.
Lachman, R. (1985). Public and private sector differences: Ceos’ perceptions of
their role environments. Academy of Management Journal 28 (3), 671–680.
LaPierre, T. A. and M. K. Zimmerman (2012). Career advancement and gender
equity in healthcare management. Gender in Management: An International
Journal 27 (2), 100–118.
Laschober, M., M. Maxfield, S. Felt-Lisk, and D. J. Miranda (2007). Hospital re-
sponse to public reporting of quality indicators. Health care financing review 28 (3),
61.
Lawler III, E. E., D. T. Hall, and G. R. Oldham (1974). Organizational climate:
Relationship to organizational structure, process and performance. Organizational
Behavior and Human Performance 11 (1), 139–155.
Lawthom, R., M. Patterson, M. West, M. Staniforth, and D. Maitlis (1995). Orga-
nizational climate. conference paper - occupational psychology conference.
Lenzi, F. (2012). Il nuovo accreditamento sanitario.
Lewin, K., R. Lippitt, and R. K. White (1939). Patterns of aggressive behavior in
experimentally created social climates. The Journal of Social Psychology 10 (2),
269–299.
Litwin, G. H. and R. A. Stringer Jr (1968). Motivation and organizational climate.
Locke, E. A., E. Frederick, C. Lee, and P. Bobko (1984). Effect of self-efficacy, goals,
and task strategies on task performance. Journal of applied psychology 69 (2),
241.
Maslow, A. H. (1943). A theory of human motivation. Psychological review 50 (4),
370.
Mathieu, J. E., D. A. Hofmann, and J. L. Farr (1993). Job perception–job satisfaction
relations: An empirical comparison of three competing theories. Organizational
Behavior and Human Decision Processes 56 (3), 370–387.
Metcalfe, L. (1993). Public management: from imitation to innovation. Australian

Journal of Public Administration 52 (3), 292–304.
Mok, E. and B. Au-Yeung (2002). Relationship between organizational climate and
empowerment of nurses in hong kong. Journal of nursing management 10 (3),
129–137.
Mouritsen, J., S. Thorbjørnsen, P. N. Bukh, and M. R. Johansen (2005). Intellectual
capital and the discourses of love and entrepreneurship in new public management.
Financial Accountability & Management 21 (3), 279–290.
Mowday, R. T., R. M. Steers, and L. W. Porter (1979). The measurement of
organizational commitment. Journal of vocational behavior 14 (2), 224–247.
Murante, A. M., C. Seghieri, A. Brown, and S. Nuti (2013). How do hospitalization
experience and institutional characteristics influence inpatient satisfaction? a
multilevel approach. The International journal of health planning and manage-
ment .
Murray, H. A. (1938). Explorations in personality.
Nuti, S. (2008). La valutazione della performance in sanita. Il mulino.
Nuti, S., A. Bonini, A. M. Murante, and M. Vainieri (2009). Performance assess-
ment in the maternity pathway in tuscany region. Health Services Management
Research 22 (3), 115–121.
Nuti, S. and A. Macchia (2005). The employees point of view in the performance
measurement system in tuscany health authorities in r. tartaglia, s. albolino, t.
bellandi, s. bagnara (a cura di) healthcare systems ergonomics and patient safety.
Nuti, S., C. Seghieri, and M. Vainieri (2013). Assessing the effectiveness of a perfor-
mance evaluation system in the public health care sector: some novel evidence
from the tuscany region experience. Journal of Management & Governance 17 (1),
59–69.
Øvretveit, J. (1996). Informed choice? health service quality and outcome informa-
tion for patients. Health policy 37 (2), 75–90.
Patterson, M., P. Warr, and M. West (2004). Organizational climate and com-
pany productivity: The role of employee affect and employee level. Journal of
Occupational and Organizational Psychology 77 (2), 193–216.
Patterson, M. G., M. A. West, V. J. Shackleton, J. F. Dawson, R. Lawthom,
S. Maitlis, D. L. Robinson, and A. M. Wallace (2005). Validating the organiza-
tional climate measure: links to managerial practices, productivity and innovation.
Journal of organizational behavior 26 (4), 379–408.
Payne, R. (1991). Taking stock of corporate culture. Personnel Management 23 (7),
26–29.
Payne, R. and R. Mansfield (1978). Correlates of individual perceptions of organi-

zational climate. Journal of Occupational Psychology 51 (3), 209–218.
Phillips, S. D., B. R. Little, and L. A. Goodine (1996). Organizational climate and
personal projects: Gender differences in the public service. Canadian Centre for
Management Development.
Pizzini, S. and M. Furlan (2012). L’esercizio delle competenze manageriali e il
clima interno. il caso del servizio sanitario della toscana. Psicologia sociale 7 (3),
429–446.
Pollitt, C. (1995). Justification by works or by faith? evaluating the new public
management. Evaluation 1 (2), 133–154.
Porter, L. W., E. E. Lawler, and J. R. Hackman (1975). Behavior in organizations.
Porter, L. W., R. M. Steers, R. T. Mowday, and P. V. Boulian (1974). Organizational
commitment, job satisfaction, and turnover among psychiatric technicians. Journal
of applied psychology 59 (5), 603.
Pritchard, R. D. and B. W. Karasick (1973). The effects of organizational climate
on managerial job performance and job satisfaction. Organizational behavior and
human performance 9 (1), 126–146.
Rentsch, J. R. (1990). Climate and culture: Interaction and qualitative differences
in organizational meanings. Journal of applied psychology 75 (6), 668.
Schauffler, H. H. and J. K. Mordavsky (2001). Consumer reports in health care: do
they make a difference? Annual review of public health 22 (1), 69–89.
Schein, E. H. (1985). Defining organizational culture. Classics of organization
theory 3, 490–502.
Schein, E. H. (1990). Organizational culture. American psychologist 45 (2), 109.
Schneider, B. (1975). Organizational climates: An essay1. Personnel Psychol-
ogy 28 (4), 447–479.
Schneider, B. (1980). The service organization: climate is crucial. organizational
Dynamics 9 (2), 52–65.
Schneider, B. (1987). Le persone fanno il posto. Psicologia e Lavoro 66 (67), 19–39.
Schneider, B. and J. Rentsch (1988). Managing climates and cultures: A futures
perspective.
Schneider, B., A. N. Salvaggio, and M. Subirats (2002). Climate strength: a new
direction for climate research. Journal of Applied Psychology 87 (2), 220.
Sitzia, J. and N. Wood (1997). Patient satisfaction: a review of issues and concepts.
Social science & medicine 45 (12), 1829–1843.
Sleutel, M. R. (2000). Climate, culture, context, or work environment?: Organi-
zational factors that influence nursing practice. Journal of Nursing Administra-
tion 30 (2), 53–58.
Soares, R., N. M. Carter, and J. Combopiano (2009). Catalyst census: Fortune 500
women board directors. Retrieved April 3, 2010.
Spath, P. (2002). Guide to effective staff development in health care organizations:
a systems approach to successful training. Jossey-Bass/AHA Press.
Spector, P. E. (1986). Perceived control by employees: A meta-analysis of studies
concerning autonomy and participation at work. Human relations 39 (11), 1005–
1016.
Spector, P. E. (1997). Job satisfaction: Application, assessment, causes, and
consequences, Volume 3. Sage.
Stone, P. W., E. L. Larson, C. Mooney-Kane, J. Smolowitz, S. X. Lin, and A. W.
Dick (2006). Organizational climate and intensive care unit nurses’ intention to
leave*. Critical care medicine 34 (7), 1907–1912.
Stubbe, J., W. Brouwer, and D. Delnoij (2007). Patients’ experiences with quality
of hospital care: the consumer quality index cataract questionnaire. BMC
ophthalmology 7 (1), 14.
Svyantek, D. and J. Bott (2004). Organizational culture and organizational cli-
mate measures: an integrative review. Comprehensive handbook of psychological
assessment: industrial and organizational assessment. Hoboken (NJ): Wiley ,
507–24.
Tagiuri R, Litwin G, B. L. (1968). Organizational climate: Explorations of a concept.
Division of Research, Graduate School of Business Administration, Harvard
University.
Thomson, O., N. Freemantle, A. Oxman, F. Wolf, D. Davis, and J. Herrin (2002).
Continuing education meetings and workshops: Effects on professional practice
and health care outcomes. Evidence-Based Nursing 5 (1), 26.
Tovey, E. J. and A. E. Adams (1999). The changing nature of nurses job satisfaction:
An exploration of sources of satisfaction in the 1990s. Journal of Advanced
Nursing 30 (1), 150–158.
Vainieri, M. and S. Nuti (2011). Performance measurement features of the italian
regional healthcare systems: Differences and similarities. Health management:
Different approaches and solutions , 299–312.
Veenstra, M. and D. Hofoss (2003). Patient experiences with information in a
hospital setting: a multilevel approach. Medical care 41 (4), 490–499.
Verspagen, B. (2007). Mapping technological trajectories as patent citation networks:
A study on the history of fuel cell research. Advances in Complex Systems 10 (01),
93–115.
Vieira, E. S. and J. A. Gomes (2010). Citations to scientific articles: Its distribution

and dependence on the article features. Journal of Informetrics 4 (1), 1–13.
Vroom, V. (1966). Some observations regarding herzberg’s two-factor theory. In
American Psychological Association Convention, New York.
Walsh, A. M. and S. C. Borkowski (1999). Cross-gender mentoring and career
development in the health care industry. Health Care Management Review 24 (3),
7–17.
Wienand, U., R. Cinotti, A. Nicoli, and M. Bisagni (2007a). Evaluating the
organisational climate in italian public healthcare institutions by means of a
questionnaire. BMC Health Services Research 7 (1), 1–13.
Wienand, U., R. Cinotti, A. Nicoli, and M. Bisagni (2007b). Evaluating the
organisational climate in italian public healthcare institutions by means of a
questionnaire. BMC health services research 7 (1), 73.
Wiggins, C. (1996). Counting gender: does gender count? The Journal of health
administration education 14 (3), 379.
Williams, B. (1994). Patient satisfaction: a valid concept? Social science &
medicine 38 (4), 509–516.
Zigan, K., F. Macfarlane, and T. Desombre (2007). Intangible resources as perfor-
mance drivers in european hospitals. International Journal of Productivity and
Performance Management 57 (1), 57–71.





























