Upload
william-l-mcgill
View
219
Download
0
Embed Size (px)
Citation preview
8/11/2019 Pleura a&P and Disorders
1/20
Pleura: AnatomyPhysiology and
DisordersJoseph S Friedberg and John C. Kucharczuk
Anatomy 1551Physiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1553Disorders of the Pleura . . . . . . . . . . . . . . . . . . . . . . . . . . . 1554Gas-Phase Disorders of the Pleural Space . . . . . . . . . . . . 1554
D isorders of the pleura and pleural space reflect someof the oldest diseases encountered in surgical history.Hippocrates described the symptoms of empyema
2400 years ago: Empyema may be recognized by the following symptoms: In the first place the fever is constant, lessduring the day and greater at night, and copious sweats supervene. There is a desire to cough and the patient expectoratesnothing worth mentioning. He also described an open drainage procedure: When the fifteenth day after rupture has
appeared, prepare a warm bath, set him upon a stool, whichis not wobbly, someone should hold his hands, then shakehim by the shoulders and listen to see on which side a noiseis heard. And right at this place, preferably on the left, makean incision, then it produces death more rarely.,,1,2 Beyondproviding less-wobbly stools, few advances were made formore than 2000 years that allowed surgeons to routinely enterthe pleural cavity, the fear being a potentially fatal pneumothorax. With the advent of positive pressure ventilati on in theearly 1900s, pneumothorax was no longer a prohibitive risk,and the era of surgical intervention in the pleural cavity hadbegun. 3
Empyema represents just one of many disorders of thepleural space that the practicing surgeon may encounter. Dis
orders of the pleural space may result from a pathologicalchange in the pleura itself or may reflect disease in adjacentor distant organs. The problems span the spectrum from abenign effusion of cardiac origin to mesothelioma, a deadlyprimary malignancy of the pleura. Despite vastly differentetiologies, the presentation and radiographic images of thesetwo conditions may appear very similar. Thus, it is importantfor the clinician to be familiar with the normal anatomy andphysiology of this space as well as the numerous disorders ofit. The goal of this chapter is to provide such a backgroundand to give a review of the diagnostic and therapeutic procedures currently employed for pleural diseases.
Liquid-Phase Disorders of the Pleural Space . . . . . . . . . . 1558Solid Disorders of the Pleural Space . . . . . . . . . . . . . . . . . 1565References 1568
Anatomy
Embryology and Microscopic Anatomy
Embryologically, the pleural cavity is created during a month,starting in the third week of gestation. Initially, the lateralplate forms two layers, the splanchnopleura and the soma opleura, which subsequently develop into the visceral and parietal pleura, respectively. Eventually, it is the visceral pleura
that surrounds the lung and the parietal pleura that lines theremainder of the chest cavity. The different embryologicalorigins of the visceral and parietal pleura are responsible forthe separate vascular, lymphatic, and neu ral supplies of thesetwo structures as seen in the adult. By the end of the seventhweek of gestation, the diaphragm has separated the thoraciccavity from the peritoneal cavity, and by the third month ofgestation the two pleural cavities have expanded sufficientlyto encase the pericardium. 4
In the adult, both pleural surfaces are approximately 30to 40l1m thick and are composed of a single layer of mesothelial cells with an underlying layer of connective tissue.Depending on their location, the mesothelial cells may beflat, cuboidal, or columnar. Mesothelial cells characteristi
cally have numerous microvilli that playa role in phagocytosis as well as contributing to the lubricious nature of thepleural surfaces. Surfactant molecules, produced by the mesothelium, line the pleural surfaces and, secondary to similarelectrical charge, repulse each other and facilitate sliding,analogous to the lubrication achieved with graphite. It isthese apposing layers of mesothelial cells that form the potential space of the pleural cavity and that glide over each otherduring respiration.
The connective tissue layer contains the neurovascularand lymphatic supply of the pleura. There are ce rtain important differences in this layer between the visceral and parietal
1551
8/11/2019 Pleura a&P and Disorders
2/20
1552 C H A P T E R 74
pleura. For the visceral pleura, the connective tissue layer isfunctionally continuous with the fibroelastic network of thelung itself. Functionally, it is this relationship that preventsthe visceral pleura from being surgically separated from thesurface of a normal lung. Pathological disruption of this connection, however, may result in subpleural air collectionsknown as blebs. s The connective tissue layer for the parietalpleura may also be tightly adherent to the underlying structures, as is characteristic of the diaphragmatic pleura. Around
the skeletal portion of the thorax, however, the pleura isbound to the underlying tissue by another connective tissuelayer called the endothoracic fascia, which forms a naturalcleavage plane. It is this plane that the surgeon develops whenperforming an extrapleural dissection.
The blood supply to the visceral pleura in humans isthought to reflect that of the lung itself, with a dual arterialsupply from both the pulmonary and bronchial arteries andsingular venous drainage into the pulmonary veins. The bloodsupply to the parietal pleura is from systemic arteries onlyand drains, predominantly, into peribronchial and intercostalveins, but it may also drain directly into the azygous vein andvena cava.
The visceral pleura is innervated by vagal and sympathetic fibers but has no somatic innervation and is thereforeinsensate. The parietal pleura is also innervated with sympathetic and parasympathetic fibers, but it is also somaticallyinnervated. Thus, the parietal pleura is capable of sensing andtransmitting the sensation of pain. Pleurisy from inflammation and pain from chest tubes, during insertion and subsequently as well, are attributable to the somatic interventionof the parietal pleura.
There are also differences in the lymphatic drainagebetween the two pleural layers. The visceral pleura drainsthrough a lymphatic network into the pulmonary lymphatics, which eventually flow toward the pulmonary hilum.This lymphatic system is richer in the lower lobes than the
upper lobes. The parietal pleural lymphatics drain to differentlocations. The mediastinal pleura drains to the mediastinaland tracheobronchial nodes. The chest wall drains anteriorlyto the internal thoracic chain and posteriorly toward theintercostal nodes near the heads of the ribs. The diaphragmatic pleura drains to the parasternal, middle phrenic, andposterior mediastinal lymph nodes. There are also transdiaphragmatic lymphatic communications that allow somedegree of lymphatic flow from the peritoneum to the pleuralspace.
The parietal pleura also differs from the visceral pleuraby virtue of the presence of Kampmeier foci and stomata.Kampmeier foci are collections of activated mesothelial andlymphoreticular cells, centered about a lymphatic core, that
augment the pleura defensive capabilities. They are concentrated in the lower mediast inal region of the parietal pleura. 6 ,7Stomata are 2- to ~ mpores that communicate directly withthe parietal pleural lymphatics. During inspiration, thesepores have the capacity to stretch, and their architecture issuch that they form functional one-way valves. Thus, theyprovide for a very effective system for draining both fluid andparticles, including both red blood cells and macrophages. Itis the presence of these pores on the parietal pleural surfacethat makes it predominantly, i f not exclusively, responsiblefor clearance of cells and particulate matter from the pleuralspace. I t should be noted that although stomata are well
studied and characterized in sheep and other mammals, thedefinitive presence of stomata in humans is less well established.
Gross AnatomyIn each hemithorax, the visceral pleura is a continuous surfacethat completely envelops the entire lung, including the fissures. At the pulmonary hilum, it continues on as the parietal
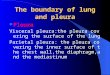
pleura to line the mediastinum, chest wall, diaphragm, andcupola of the ches t cavity. In humans, the pleural cavities arecompletely separate, coming into contact with each other fora short distance behind the upper half of the body of thesternum Fig. 74.1). It is this pleural separation of the rightand left chest cavities that prevents bilateral pneumothoracesfrom occurring as the result of a unilateral chest injury. Atthe costophrenic and costomediastinal sinuses, the parietalpleural folds back on itself, providing a potential space intowhich the lungs can expand during inspiration. 8
Superiorly, the pleura extends above the bony thorax in tothe base of the neck Fig. 74.2). This fact explains why pneumothorax may complicate internal jugular central line placement as well as subclavian central line placement. Anteriorly,the pleura extends to the sixth rib, to the ninth rib laterally,and to the twelfth rib posteriorly Fig. 74.2). In the livingpatient, the lung can fill the entire posterior recess. In areview of 100 chest radiographs, 80% of patients were foundto have lung present a t or below the level of the 12th rib, andin 18% it was seen at the level of the first lumbar vertebra. 9These external landmarks of the pleural space are of practicalclinical significance, particularly when evaluating a patientwith penetrating trauma.
The pulmonary ligament is a double fold of the mediastinal pleura that tapers down from the root of the lung, whereit is in continuity with the visceral pleura, to the caudalmediastinum. This ligament is one of the structures that
must be divided to perform a pneumonectomy or lower
FIGUR 74.1. Relationship of the thoracic skeleton to the heart(line), pleura (light gray), and lungs (dark gray). (Adapted with permission from Gray's Anatomy.76 1980 W.B. Saunders Co.)
8/11/2019 Pleura a&P and Disorders
3/20
P L E U R A : A N AT O M Y, P H Y S I O L O G Y, A N D D I S O R D E R S 1553
Horizontal fissure
Oblique fissure
Infe rior borderof right lung
Cardiac notchin left lung
Costodiaphragmaticline of reflexion ofleft pleura
Costodiaphragmaticline of refiexion ofright pleura
FIGUR 74.2. Relationship of the lung (dark gray) and the parietalpleural envelope, which extends down beyond the edge of the lung(light gray). (Reprinted with permission from Gray's Anatomy.76 1980, W.B. Saunders Co.)
lobectomy. I t is also routinely divided to its superior border,the inferior pulmonary vein, when attempting to providemobility to the lower lobe after resecting the upper or middlelobes. The lymph nodes within the pulmonary ligament arethe level 9 nodes, which are N2 lymph nodes, and should beroutinely harvested when performing a resection for lungcancer.
Physiology
The pleura has both mechanical and physiological functions.It transmits negative pressure from the thorax to the lung,
thereby opposing the lung's natural elastic recoil and maintaining pulmonary expansion. During respiration, this function is performed in an environment of very low friction,thereby allowing the lungs to glide smoothly over the internalthoracic surfaces as they expand and contract. The pleura alsocontrols the environment of the chest cavity by maintainingfluid homeostasis, preventing or removing air collections andkeeping the space sterile.
Under normal conditions, the pleural cavity is a potentialspace with a thickness ranging from 10 to 20f..Lm. The lung ismaintained in an expanded state by the maintenance of negative pressure in the pleural space; th is allows the expandablechest cavity to overcome the opposing forces exerted by thenatural elastic recoil of the lung. The resting pressure in the
pleural space, when the lung is at its functional residualcapacity, is slightly negative at -2 to -5 cm H 20 . When measured in an upright posture, there is more negative pressurein the apex of the chest than at the diaphragm, likely agravitational effect. The negative pressure continues toincrease through inspiration, with the pressure ranging from-25 to -35 cm H 20 at the vital capacity. Disorders thatdecrease the compliance of the lung or increase airway resistance further increase the negative pressure in the pleuralspace with inspiration. 5,9
Initially, it would seem curious that gas is not drawn outof solution into the pleural space by the negative pressure in
the space. It is the lower partial pressure of gases on thevenous side of the pleural circulation, as opposed to the arterial side, that prevents spontaneous pneumothorax fromoccurring under normal conditions. This difference in partialpressures between the two sides of the circulation is mainlya result of oxygen absorption. Unless the pressure in thepleural space decreases to significantly less than -SOcm H 20 ,the sum total of the forces under normal conditions favorsabsorption of gas out of the pleural space.
This diffusion gradient also accounts for reabsorption ofgas that is introduced into the pleural space. The clearancerate of gases introduced into the pleural space is dependenton the concentrations of those gases with respect to theirpartial pressures in the pleural circulation. As the partial pressure of nitrogen is the greatest in the air we breathe, it therefore constitutes the highest partial pressure of the gases thatform a pneumothorax. Nitrogen also has the highest partialpressure of the gases in our circulation; this can be decreasedby altering the composition of inspired gases. Thus, administration of supplemental oxygen decreases the partial pressureof nitrogen in the bloodstream and thereby increases thenitrogen pressure gradient between the circulation andthe pneumothorax, favoring more rapid reabsorption of thetrapped gas. This relationship serves as the rationale forplacing a patient on supplemental oxygen to facilitate reabsorption of a pneumothorax that is not being externallyevacuated. 10
Under normal conditions, the pleural space contains verylittle fluid, estimated at approximately 0.3 mL/kg. The fluidis generally hypooncotic, with a protein content of approximate ly 1 g/dL. The mechanisms of fluid production and reabsorption are complicated and not completely understood.Numerous forces interact from both the parietal and visceralpleura, including their respective hydrostatic and on co ticpressures. Respiratory movement and gravity are boththought to have roles in maintaining the fluid dynamics of
the pleural cavity. The predominant factor, however, isthought to be the uptake of fluid into the parietal pleurallymphatics. These lymphatics tend to be concentrated in thedependent portions of the chest cavity. Unde r normal conditions, this flow rate has been estimated at 0.1 to O.lSmL/kg/h. The lymphatic flow rate has the capacity to increase andhas been estimated to reach as high as 30mL/h, approximately 700mL/day in an average-size individual. When thedynamics of this equilib rium are unbalanced beyond the rateat which the lymphatics are able to compensate, pleural effusion accumulates. 7,9,11
It is interesting to note that the exact purpose of thepleura is still not fully understood. Empirically, it is clear thatthe pleura maintains fluid and gas homeostasis, mechan ically
couples the lungs to the bellows mechanism for respiration,and maintains sterility in its described space. To accomplishthis, however, it is not clear how important it is to have theconfiguration of two opposing layers with a small amount ofintervening fluid. It has been observed, for instance, that thereis littl e change in pulmonary function tests in patient s beforeand after fusion of the pleural space. 12 It is interesting to notethat some mammals do not have a pleural space, similar topatients who have undergone pleurodesis, but that theseanimals clearly function normally. Thus, the exact necessityfor having two pleural membranes defining a potent ial spaceremains somewhat of a mystery.
8/11/2019 Pleura a&P and Disorders
4/20
1554 C H A P T E R 74
Disorders of the Pleura
There are a large number of pleural disorders. The majoritylead to symptoms as a result of mechanical compression ofthe lung, although many may be asymptomatic or may presentwith constitutional symptoms or pain. In most cases, thepathology results from the presence of something in thepleural space, which as previously described, is normally apotential space. Therefore, in an effort to organize this large
number of disorders, they are grouped according to whatabnormal phase of material is occupying the pleural space,that is, gas, liquid, or solid. When gas enters the pleural space,it is referred to as a pneumothorax. When liquid enters thepleural space, it may sometimes be broadly referred to as anexudative or transudative effusion but is frequently classifiedaccording to the type of liquid, such as hemothorax, chylothorax, or empyema. Last, solid masses may occupy thepleural space. Most benign masses are pleural plaques, butthere are also rare benign tumors of the pleura, some of whichmay reach enormous size. Malignant masses of the pleura areusually cancers that have metastasized to the pleura, butthere are also some rare primary tumors, most commonlymesothelioma. Sometimes, the groups may overlap, withmore tha n one abnormal phase of material filling the pleuralspace. Such examples include air and blood, a hemopneumo-thorax, after trauma or air and pus, a hydropneumothorax,which may be seen with empyemas resulting from a bronchopleural fistula. Frequently, however, there is a predominant,if not sole, etiology for the abnormal accumulation; thus, thefollowing sec tions review disorders of the pleura according tothe state of matter that is abnormally occupying the spacegas, liquid, or solid.
Gas-Phase Disorders of th Pleural Space
PneumothoraxPneumothorax is defined as air in the pleural space. It mayoccur traumatically, iatrogenically, or spontaneously. Spontaneous pneumothorax may be subclassified as primary orsecondary, with primary spontaneous pneumothorax arisingin an otherwise healthy patient and secondary spontaneouspneumothorax arising as a complication in a patient withknown underlying pulmonary disease. Essentially any pneumothorax resulting from pleural disruption can present as atension pneumothorax. This condition represents a trueemergency and is discussed separately.
PNEUMOTHORAX PRESENTATION A ND DIAGNOSIS
Pneumothorax may cause pain or dyspnea, or it may beasymptomatic, depending on its size and the underlying pulmonary function of the patient. Physical findings may rangefrom none to the classic findings seen with a tension pneumothorax: contralateral tracheal deviation, ipsilateral absentbreath sounds, and percussive hyperresonance. Electrocardiographic changes may be present, including diminished voltage,right-axis deviation, or T-wave changes that may mimic asubendocardial myocardial infarction. '3
Except for tension pneumothorax, most cases require anupright chest radiograph to establish the diagnosis. As the
pneumothorax occupies a greater proportion of the chestcavity at expiration than inspiration, the former is more sensitive for detecting the diagnostic pleural line. A computedtomographic CT) scan of the chest is the most sensitive testand may demonstrate a small amount of air in the pleuralspace that is not visible on the plain radiograph.
PNEUMOTHORAX TREATMENT OPTIONS
For all pneumothoraces, the common goal is removal of airfrom the pleural space. Depending on the etiology, however,prevention of recurrence may also be an objective of the treatment. Options for treatment range from observation to thoracotomy. Selection of the appropriate modality depends ona number of factors, including, but not limited to, presentation, previous history, comorbidities, need for positive pressure ventilation, associated effusion, and even the patient'slifestyle. In addition, the size of the pneumothorax canalso play a significant role in determining the appropriatetreatment.
The following sections review the basic technique andindications for the different treatment options that are available and give specific recommendations for different pneumo
thoraces to be described in the following section.
OBSERVATION
Observation is generally reserved for patients who areasymptomatic and are diagnosed with a small primary spontaneous pneumothorax or a simple iatrogenic pneumothorax.In such situations, the patient is followed with serial radiographs to ensure that the pneumothorax is decreasing in size.When a patient is breathing room air, gas is absorbed fromthe pleural cavity at approximately 1.25% of the pleuralvolume/day, approximately 50 to 70mL/day.'4 Supplementaloxygen, by mechanisms reviewed in the physiology section,can increase this rate up to 4.2 %/day.IS As it is a minimal
intervention, it is reasonable to place all hospitalized patientson supplemental oxygen if they are being observed for apneumothorax.
There are several factors to weigh when considering observation alone for a patient with a pneumothorax. The first isthat deaths have been reported in patients with pneumothorax who were being observed. Development of umecognizedtension pneumothorax was believed to have played a role inthese cases. 16 This fact highlights the selectivity and judgment required to simply follow these patients, particularly onan outpatient basis. Another consideration is that a lung thathas not fully expanded by 2 weeks is at risk for fibrous peeldeposition and subsequent entrapment. Correction of thissituation commits the patient to a surgical procedure that
might have been avoided by initial evacuation of thepneumothorax.
It is recommended that observation be considered only forpatients with a simple pneumothorax whose size involves15% or less of the volume of the chestY If the pneumothoraxhas no t resolved within 1 to 2 weeks, intervention to achievefull expansion should be instituted. Another factor to consider, particularly with primary spontaneous pneumothorax,is that observation alone does nothing to decrease the chanceof recurrence. Last, in this age of economic constraints , it maybe more cost-effective to definitively treat a pneumothoraxon presentation.
8/11/2019 Pleura a&P and Disorders
5/20
PLEURA : A N A T O M Y , P H Y S I O L O G Y , A N D D I S O R D E R S 1555
SIMPLE ASPIRATION
Simple aspi rat ion can be considered in the case of a s implepneumothorax in which there is no suspicion of an ongoingair leak and the patient is not on positive pressure ventilation.Some authors believe that in select situations aspiration isthe treatment of choice . The goal of aspiration is to removeair from the pleural space . It conveys no protection from anongoing leak or recurrence in the future . The procedure isperformed in a manner similar to that used for decompressing
a tension pneumothorax . After steri lely preparing the skinand infiltrating with a local anesthetic, a 16- or l8-gaugeintravenous catheter is placed into the pleura l space in themidclavicular line over the superior surface of the second rib.The needle is then withdrawn , and the catheter is connectedto a short length of int ravenous tubing capped with a threeway stopcock. A 60-mL syringe is then used to aspirate airfrom the chest cav ity . When air can no longer be aspirated ,the catheter is withdrawn , and the first chest x-ray is obtained.If 4 L of air are aspirated and no res istance is met, there is anongoing air leak , and a chest tube should be placed .
PERCUTANEOUS TUBE THORACOSTOMY
Percutaneous tube thoracostomy is a goodoption for a simplepneumothorax . Many consider this the procedure of choicefor simple pneumothoraces . Cited advantages are therapeuticand cost-effectiveness as well as less t rauma compared tostandard tube thoracostomy . Depending on the size and etiology of the pneumothorax, success rates for these catheters arereported in the 85 % to 90 % range . The catheters range insize from 9 to 16 French and are placed using a catheter-overneedle or Seldinger technique . The kits (e .g., Arrow Pneumothorax Kit , Arrow International , Reading , PA) are usuallyequipped with all the necessary supplies to insert the catheters and an adapter such that the catheter can be connectedto a Heimlich valve or a standard suction device such asPleur-evac (DSP Worldwide , Fall River , MAl . Thes e tubes are
limited by their size and would be a poor choice for a patientwith a large air leak . The principal factor in determining theflow rate through a tube is the diameter of the tube . Thus, apatient with a mass ive air leak , especially on positive pressure ventilation , should have a standard chest tube placed . Asa general guide, it takes at least a 28-French tube to accom-
modate approximately l5L/min of flow at -lOcm H suction .
TUBE THORA COSTOMY
A standard chest tube should be placed for failure of a percutaneous tube, a pneumothorax associated with significantfluid collection , or a pneumothorax for which the leak isexpected to ov erwhelm a small-caliber tube , more l ikely inthe setting of posit ive pressure venti lation . Such tubes are
generally placed under local anesthesia and sedation, employing sterile technique . Apical tubes, as employed for drainageof air, are bes t placed in the mid- or anter ior axil lary l ine inthe third or fourth intercostal space . I t is generally recommended to tunnel the tube subcutaneous up one interspacebefore entering the pleural cavity. The tunnel serves twopurposes . First, it forms a flap valve that helps prevententrance of air into the chest after the tube is removed .Second , the tunnel allows the surgeon to control the directionof the tube, anteriorly when placed for air or posteriorly whenplaced to drain fluid . The tube can then be placed for passiveor active drainage . Passive drainage may be achieved by connecting the tube to a Heimlich f lu tter valve or watersea l ona Pleur-evac. For active drainage, most surgeons use a threebottle system (Fig . 74.31, generally unified as a commerciallyavailable unit such as Pleur-evac . Active drainage expeditesand facilitates full expansion of the lung . Although alsoreported with passive drainage, the rare complication of reexpansion pulmonary edema appears to be more common withactive suction .21,22
Generally viewed as a floor procedure, chest tube placement should be given all the consideration of a major operation . Although it can be performed with minimal discomfort ,utilizing intravenous sedation and strategic local anesthesia ,a chest tube placed by an inexperienced operator withoutexpert supervision can be a horrific experience for a patient .In addition to the discomfort , chest tube placement may be
accompanied by a number of complications includingempyema, lung injury and bleeding, and death . Therefore ,coagulation profiles and immunocompetency should be takeninto consideration for all patients considered for this procedure . Intravenous analgesia, a short-acting benzodiazepine, orboth should be used for an elective ches t tube p lacement .
Atmosphe ric Vent
Wall S uctionAir Air... .....;. ir ir
Drainage f rom Pat ien t Airand Fluid . : : ~ . . . .
FIGURE 74.3. Three -bott le suc tionsetup for pleural drainage .
Co llected Fluid
tWater SealChamber(prevents airfrom refluxngback to patient
8/11/2019 Pleura a&P and Disorders
6/20
1556 C H A P T E R 74
Proper use of local anesthesia is cri tical for patient comfortduring the procedure. The amoun t of local anesthetic thatcan be administered is l imited by toxicity. A small amountof anesthetic is injected for the skin incision, and the remainder is accurately injected along the course of the tunnel thatwill be created to place the tube. This step allows the surgeonboth to locate the superior surface of the rib and, by aspirating, to identify the parietal pleura. A small bolus of anesthesia can be injec ted at the level of the parietal pleura, and if
adequate t ime is a llowed after injec tion of the pleura, thediscomfort of the tube placement can be limited to pressureand not sharp pain. As with all procedures under local anesthesia, it is also impor tant to prepare the pat ient for anyanticipated sensations, particularly the entrance into thepleura l space as well as the possibility for triggering severecoughing if a collapsed lung is rapidly reexpanded.
SURGERY
With the exception of those patients with a large open pneumothorax, essentially all patients considered for surgicalt reatment for a pneumothorax already have a chest tube inplace. With a progressive air leak, tension physiology is immi
nent once posit ive pressure venti lation is insti tuted unlessthere is a pathway for egress of air from the pleural space orintubation is performed directly with a double-lumen endotracheal tube such that the leaking lung can be immediatelyisolated. Specific surgical procedures are discussed under th eappropriate sections, but it is wor th not ing that there are twosurgical approaches available, video-assisted thoracoscopicsurgery VATS) or standard thoracotomy.
General indications for surgical intervention for a pneumothorax are failure of less-invasive therapy or occurrence ofthe pneumothorax in the context of additional indications forchest exploration. A VATSapproach can be employed, at leastinitially, for most pneumothoraces. Examples of contraindications to a VATS approach are a pneumothorax secondaryto an esophageal perforation, major airway disruption, or apneumothorax accompanied by significant ongoing bleedingor concomitant trauma to other thoracic organs.
TYPES OF PNEUMOTHORAX
Pneumothoraces can be broadly grouped as spontaneous ortraumatic. Spontaneous pneumothoraces can be further subclassified as primary or secondary, with primary arising inpatients with no known underlying pulmonary disease andsecondary spontaneous pneumothoraces arising as a complication of known underlying pulmonary disease. Traumaticpneumothoraces can be subclassified as those that are the
result of blunt or penetrating trauma to the chest or thosethat are iatrogenically induced secondary to an invasive procedure or barotrauma from positive pressure ventilation. Inthis chapter, the former are referred to as traumatic pneumothoraces and the latter as iatrogenic pneumothoraces.
PRIMARY SPONTANEOUS PNEUMOTHORAX
Primary spontaneous pneumothorax most commonly occursin tall young men but may occur in anyone at any age. Thepeak incidence has been reported to occur for both me n andwomen 25 to 34 years old. It is approximately six times morecommon in men than women.
It is thought t ha t t he final common pathway for mostprimary spontaneous pneumothoraces is rupture of subpleural blebs. It is also thought that inflammation of the distalairways plays a significant role in the pathogenesis of thisdisorder. The lack ofcommunication between these blebs andthe distal airways, and hence the inability to rapidly decompress, may explain the increased incidence of primary spontaneous pneumothorax associated with significant drops inatmospheric pressure. The role of inflammation may explain
why spontaneous pneumothorax is much more common insmokers. In fact, there appears to be a dose-response relationship, with light smokers (fewer than 13cigarettes/day) runninga risk 7 times that of nonsmokers and those smoking morethan 22 cigarettes/day at least 100 times more likely to havea spontaneous pneumothorax than nonsmokers. It is generally accepted that recurrent spontaneous pneumothoracesbecome increasingly likely with each successive occurrence.The exact statistics vary, but it is est imated t ha t the risk ofrecurrence in the absence of aggressive preventive measuresis in the range of 25 % after the first recurrence and 50 % afterthe second recurrence.P The chance of recurrence is verymuch related to the treatment undertaken for the initial spontaneous pneumothorax. Cessation of smoking also decreasesthe risk of recurrence.
Selection of treatment remains an area of controversy. Aconsensus s ta tement was released to provide guidance intreatment selection. Observation alone should be selectedfor treatment on the initial presentation of a small , asymptomatic primarypneumothorax in a patient without any associated comorbidities. It should be reserved for patients whohave no barot rauma risks and have ready access to medicalhelp. This t reatment may be particular ly appropriate forpat ients who present with heavy cigarette abuse and arewilling to stop smoking. Aspiration is another option, but itconfers no significant protection from recurrence. Once thedecision has been made to violate the pleura for aspiration, it
is probably worthwhile leaving a catheter through which aircan be continuously aspirated and subsequent pleurodesis canbe performed. If a large air leak is ant ic ipa ted or if there issignificant effusion associated w it h t he pneumothorax, thena s tandard 28-French chest tube should be placed. Nei thertechnique, without pleurodesis, seems to convey significantprotection from recurrence.
Surgical treatment remains the gold standard in preventing recurrence of spontaneous pneumothorax. Some of theindications for surgical treatment of a spontaneous pneumothorax include a second pneumothorax (ipsilateral recurrenceor a new pneumothorax on the contralateral side); tensionphysiology; synchronous bilateral pneumothoraces; associated hemothorax (likely secondary to a to m adhesion and
complicating approximately 5% of spontaneous pneumothoraces); failure of tube thoracostomy; and lifestyle factors.Surgery should be considered if a leak persists for more than48h. Lifestyle issues that are accepted indications for surgicaltherapy at the initial presentation of a primary spontaneouspneumothorax include occupational exposure to barotrauma(scuba diving or flying nonpressurized high-altitude aircraft)and poor accessibility to medical care.
The surgical procedure for spontaneous pneumothorax isresection of the blebs that are usually present, most commonly located in the apex of the upper lobe or the superiorsegment ofthe lower lobe. Resection of the blebs is performed
8/11/2019 Pleura a&P and Disorders
7/20
PLEURA : A N AT O M Y, P H Y S I O L O G Y, A ND D IS OR DE RS 1557
FIGURE 74.4 . Typical arrangement of videothoracoscopyports. Thecamera, and eventually the chest tube, are introduced through thelowestport (left I. The remaining two incisions (right) are placed alonga potential thoracotomy incision . Outline of the scapula is seenonthe right . Reprinted with permission from Friedberg and Kniger. 1998 Greenwich Medical MediaLtd. andby permission of CambridgeUniversity Press.I
with a pulmonary stapling device . Most surgeons also performa mechanical pleurodesis of the pleura, utilizing an abrasivematerial such as an elect rocautery scratch pad, or performparietal pleurectomy. Currently, VATS is considered the preferred surgical approach .
A standard t riad of video ports can be employed in mostcases (Fig . 74.4) . Use of a 30 thoracoscope facilitates visualiza tion at the apex of the chest . The thoracoscope is introduced through the inferior port with a grasping device, andthe thoracoscopic stapler is introduced through the twosuperior ports. A sponge stick or folded electrocautery scratchpad can be used for the pleurodesis, with or without a pari
etal pleurectomy of the bony hemithorax . At the conclusionof the operation, a single 28-French chest tube , with additional ports cut through the radioopaque line , can be placedposteriorly to the apex of the ches t . A rongeur is useful forcut ti ng extra holes in chest tubes. If the surgeon is morecomfortable placing an anterior and posterior chest tube, twovideo ports can be created low in the chest at the futurechest tube sites, and a single port can be placed in line witha potential thoracotomy incision for grasping and stapling.In skil led hands, the ent ire lung can be well visualized andmobilized for stapler application, mechanical pleurodesis,and i f necessary , pleurectomy (Fig . 74.5) . For most of thesecases, thoracotomy offers l it tle advantage with respect tovisualization or performance of the bleb resections, pleurec
tomy, and pleurodesis .
SECONDARY SPONTANEOUS PNEUMOTHORAX
Secondary spontaneous pneumothorax is a more seriouscondition than primary spontaneous pneumothorax becauseof its occurrence in pat ients who l ikely have s ignif icantlyless pulmonary reserve than the typical patient presentingwith a primary spontaneous pneumothorax . As opposed toprimary spontaneous pneumothoraces, secondary spontaneous pneumothoraces are associated with a significant mortality . Historically, the most common cause of secondaryspontaneous pneumothorax has been chronic obstructive
pulmonary disease (COPD). There are many other causes ofsecondary spontaneous pneumothorax, including, bu t notl imited to , cystic fibrosis, asthma, cancer, many types ofinfection, sarcoid , collagen vascular diseases, and catamenialpneoumothorax .
The principal factor affecting choice of treatment in thesepatients is the nature of the underlying pulmonary disease. Ifthe patient is symptomatic, which is far more likely with thispatient population, there is no role for observation . Further
more, an increase in the pneumothorax could possibly placethe patient's life in jeopardy . Therefore, observation of a secondary spontaneous pneumothorax is not recommended.Tension physiology is frequently unnecessary to cause clinical decompensation in these patients. Any consideration ofemploying posit ive pressure venti lation in a patient with asecondary pneumothorax should serve as an indication forthoracostomy tube placement .
Earnest consideration should be given to sclerosis for prevention in most of these cases . An important exception is thepatient who is awaiting lung transplantation because adhesions resulting from sclerosis can significantly complicateexplantation of the native lung at the time of transplantation .Another consideration is the nature of the underlying pulmonary disease. If the pneumothorax occurs in the set ting of adisease, such as certain malignancies or infections, it may notbe possible to staple the lung or to achieve total lung expansion . In these cases, particularly i f the patient is terminallyill, consideration should be given to sending the patient homewith a chest tube and a Heimlich valve if this provides adequate palliation .
IATROGENIC PNEUMOTHORAX
Iatrogenic pneumothorax may be the most common cause ofpneumothorax. The most common causes include transthoracic needle biopsy, central line placement, thoracentesis,
FIGURE 74 .5. Intraoperative photograph taken through the videothoracoscope demonstrates an apical bleb (within th e graspingforceps Iin a patientpresenting with a recurrentprimaryspontaneouspneumothorax. The bleb was then resected with a thoracoscopicstapling device, introduced through the third port incision . Subsequently, a parietalpleurectomy of the entire chest wall pleuraand amechanical pleurodesis of the mediastinal and diaphragmatic pleurawere performed. A single chest tube was then inserted through thelowest incision , which had been used for the videothoracoscopeduringthe procedure.
8/11/2019 Pleura a&P and Disorders
8/20
1558 C H A P T E R 74
transbronchial pulmonary biopsy, and positive pressure ventilation. The management of an iatrogenic pneumothoraxmust take into accoun t a number of factors, including theetiology, symptoms, and size of the pneumothorax and ventilatory status of the pat ient . It is logical to consider thosepatients with pneumothorax secondary to positive pressureventi lation, barotrauma, separately from those who developed pneumothorax secondary to violation of the visceralpleura.
The development of a pneumothorax as a result of barotrauma is an indication for immediate placement of astandard chest tube. This indication is also true for aprocedure- induced pneumothorax in a venti la ted pat ientbecause positive pressure venti la tion can rapidly lead to atension pneumothorax. The clinician should always considerpneumothorax as a cause for instability in a ventilated patientwho recently underwent thoracentesis or central lineplacement.
The majority of iatrogenic pneumothoraces are procedureinduced. These pneumothoraces differ from spontaneouspneumothoraces in t ha t the patient is no t at an increased riskfor recurrence. For small, asymptomatic pneumothoraces,observation is appropriate, and thoracostomy tube placementand sclerosis are no t indicated. For larger pneumothoraces orsymptomatic pneumothoraces in ambulatory patients, simpleaspiration or temporary placement of a small percutaneouscatheter is the preferred approach of many clinicians.
TENSION PNEUMOTHORAX
Any closed pneumothorax arising from visceral pleural disruption has the potential to develop into a tension pneumothorax. Tension pneumothorax occurs when air accumulatesin the pleural space in excess of int rapleura l pressure andactively compresses the ipsilateral lung. This tension physiology will eventually lead to contralateral medias tina l shi ftand, in addition to pulmonary embarrassment, can severely
limit venous return and compromise cardiac output.Untreated, tension pneumothorax may lead to cardiopulmonary arrest and for this reason is a life-threateningemergency.
Tension pneumothorax is believed to occur when a pleuraldisruption forms a functional one-way valve allowing air toescape from the lung bu t no t reenter. Such physiology isoccasionally well tolerated in a healthy adult and can awaitchest tube placement under urgent, bu t controlled, conditions. If, however, the patient is in distress and the diagnosisis suspected, placement of a 16- or IS-gauge intravenous catheter over the second rib, in the midclavicular line, will convertthe tension pneumothorax to an open pneumothorax. Afterdecompression has been achieved, a chest tube can then be
placed in the usual manner. This procedure should always beperformed immediately in any patient who is decompensating and for whom tension pneumothorax is in the differentialdiagnosis. It is a mis take to wai t for a confi rmatory chest xray in such a s itua tion .
Blebs and Bullae
Although pneumothorax is a disorder of air that has enteredinto the pleural space, blebs and bullae are also disorders ofabnormal air collections, bu t still contained within the lung.Only blebs can be considered a true pleural disorder. Blebs
arise when air escapes from the pulmonary parenchyma andis trapped in the visceral pleura. Simply stated, blebs aresubpleural collections of air. They are usually small, less than2 em, and tend to occur at the apex of the upper lobe orth e apex of the superior segment. The significance of blebs isuncertain. By themselves, it is doubtful that they cause anysignificant effect on pulmonary function. Their primary clinical significance lies in the fact that they appear to be involvedin the pathogenesis of spontaneous pneumothorax. No spe
cific treatment is indicated for th e finding of pulmonary blebsin th e absence of pneumothorax. Cessation of smoking, asalways, is recommended.
Bullae are air collections measuring at least 1em, bu t maybecome so large that they occupy the greater part of the hemithorax. As opposed to blebs, bullae are formed by destructionand coalescence of alveoli. They may demonstrate trabeculated lumens formed by the residual structural elements fromthe lung parenchyma they replaced. Blebs may be an incidental finding in patients with otherwise normal lungs, bu t bullaeare likely to be associated with some form of pulmonarydisease, most likely emphysema.
Bullous disease is also frequently asymptomatic. In suchcases, cessation of smoking and annual chest x-rays are sufficient. In the setting of known underlying lung disease, treatment of that disorder is the priority. Pneumothorax, infection,or hemoptys is can prompt surgical intervent ion. Surgicalintervention can also be indicated for compression of normallung tissue to improve pulmonary function. Generally, verygood results can be anticipated if the bulla is occupying morethan 500/0 of the hemithorax, compressing well-perfusedparenchyma. 29
Liquid-Phase Disorders of th Pleural Space
Pleural effusions are a very common disorder encountered by
the clinician. There are many potential causes of effusions(Table 74.1).Occasionally, it is possible to deduce the etiologyin the context of the patient 's chest radiograph and concurrent morbidities. Frequently, however, the fluid must besampled to yield a diagnosis. There is a normal compositionof pleural fluid (Table 74.2) and a hos t of t est s that can beperformed on the fluid in pursuit of a diagnosis (Table 74.3).Once the fluid is sampled, it wil l fall i nto one of two categories, t ransudat ive or exudative, and 990/0 of exudativeeffusions will demonstrate at least one of th e following characteristics: pleural fluid protein/serum protein ratio greaterthan 0.5, pleural fluid lactate dehydrogenase (LDH)/serumLDH greater than 0.6, or pleural fluid LDH more than twothirds of the upper normal limit for serum LDH. 30
Transudative effusions result from a perturbation in thehydrostatic or oncotic forces that affect fluid formation andturnover in the pleural space, as described in the physiologysection. This imbalance results in fluid accumulation in thepleural space. For transudative effusions, the goal is to drainthe effusion for symptomatic relief, if necessary, bu t to focuson the systemic disease.
Exudative effusions result from diseases that involve thepleura and may be broadly grouped as benign or malignant.The treatment of an exudative effusion is disease specific.
Pleural effusions may be asymptomatic or may cause thepat ient to present with shortness of breath, secondary to
8/11/2019 Pleura a&P and Disorders
9/20
P LE UR A : A N ATO M Y, P H YS IO L OG Y, A N D D I S O R D E R S 155 9
TABLE 74.1. Differential Diagnoses of Pleural Effusion. TABLE 74.2. Normal Composition of Pleural Fluid.
TABLE 74.3. Useful Tests in th e Evaluation of Pleural Effusion.
Data from humans and animals.
Source: Reprinted with permission from Fishman. 1998 McGraw Hill.
compress ion of pulmonary parenchyma, as wel l as othersymptoms. A nonspecific sign that is compatible with aneffusion is th e presence of a nonproductive cough. If th e disorder causing the effusion has provoked an inflammatoryresponse in the parietal pleura, t he pat ient may complain ofpain with respiration, known as pleuritic chest pain.
Restricted chest wall movement or change in the contourof the hemithorax may be evident, depending on the natureof the effusion and its effect on pleural pressure. If the effusion is unilateral and massive, the trachea may deviate to th econtralateral side. Absence of vocal fremitus, dullness to percussion, and decreased breath sounds are all characteristic
apF/S,pleural fluid-to-serum ratio.
bIU, concentration in international units.
0.1-0.2mL/kg1000-500030/0-700/0300/0-75%2%-30%10%1-2g/dl50%-700/0
plasma level1PositivePositive
Amylase, PF/SBacteriologicalCytology
AbnormalTest value
Red blood cells/rum >100,000
White blood cells/mrrr' >10,000Neutrophils 0/0 >50Lymphocytes 0/0 >90
Eosinophilia 0/0 >10
Mesothelial cells AbsentProtein, PF/S a >0.5LDH, PF/S >0.6LDH, IU b >200Glucose, mg/dl
8/11/2019 Pleura a&P and Disorders
10/20
156 C H A P T E R 74
findings on physical examination. If the pleura is inflamed,there may be an audible rub. A rub is likely to precede asignificant effusion that will separate the roughened pleuralsurfaces and diminish or resolve the rub. In the case of ahydropneumothorax, there may be an audible splash, asoriginally described by Hippocrates.
Plain radiographs of the chest remain t he mos t commontest obtained to evaluate a suspected effusion. If the effusionis free flowing, the lateral costophrenic angle may be blunted
on an upright posteroanterior radiograph. The lateral radiograph is more sensitive t ha n t he posteroanterior view, bu tnei ther is as sensitive as the lateral decubitus projection.Additional studies that are commonly used to obtain moreinformation about a suspected effusion include ultrasoundand CT scan. Ultrasound is helpful in distinguishing pleuralthickening from pleural fluid and determining if an effusionis complex or simple, and it has the advantage of portability.It can be used to help direct the clinician to the best area toperform a thoracentesis at the bedside. CT scans give themost information with respect to exact location ofan effusionand may be particularly helpful in distinguishing effusionfrom pleural disease or parenchymal disease.
If the clinical scenario warrants diagnosis of the effusion,t hen the nex t step is to perform a thoracentesis to obtain aspecimen for analysis and, possibly, to drain the effusion forrelief of symptoms. The decision to perform such a procedureshould be taken seriously for the complications can be significant and include pneumothorax, hemothorax, and conversion of a steri le effusion into an empyema. Thus, it isimportant to make sure the patient is not coagulopathic, andif there is any question regarding the appropriate site to insertthe needle, a bedside ultrasound should be performed.
Sterile technique must be observed. The procedure ismost easily accomplished with the patient in the sitting posit ion and leaning over a bedside table that has been paddedwith one or two pillows. For a diagnostic tap, a long 25-gauge
needle can be used to infiltrate with lidocaine and can be usedas a finder needle. A 22-gauge needle is then used to performthe aspiration.
If a therapeuti c tap is indicated, a simila r t echnique isemployed, except that a catheter is placed into the chestcavity and connected via tub ing to a three-way stopcock,which in tu m is connected to a syringe or a vacuum bot tle.A number of commercial kits are available for this purpose.
Regardless of the technique, it is generally recommendedthat not more than 1L offluid shouldbe aspirated at one timeas this increases the chances of developing reexpansion pulmonary edema. The exact e tio logy of this syndrome is notfully understood and may be accompanied by 200/0 mortality. Treatment for reexpansion edema is supportive care.
Transudative EffusionsIf the effusion is transudative, then it is most likely secondaryto congestive heart failure, hepatic insufficiency, or renalinsufficiency. Pleural effusions secondary to congestive failureare the most common transudative effusions.f Most of theseeffusions are bilateral. The presence of a unilateral effusionor bilateral effusions of significantly different sizes does notexclude this diagnosis, bu t would be unusual. The disorder isthought to result from increased pressure at the pulmonarycapillary level secondary to left heart failure. The treatment
is th e same as for other transudative effusions and is directedat the underlying cause, in this case, congestive failure. If theetiology is unclear or if the effusion remains unchanged afterthe congestive heart failure has improved, a diagnostic thoracentesis should be performed. Occasionally, it is necessary toperform a therapeutic tap for symptomatic relief.
Approximately 5 % of patients with hepatic cirrhosis willdevelop pleural effusions as a result of their disease. Twothirds of cirrhotic pleural effusions are right sided. Usually,
the pat ient wil l have asci tes in addit ion to the pleural effusion. The pleural effusion is thought to result from a one-waycommunication and fluid flow from the peritoneum, acrossthe diaphragm, to the pleural space. The treatment should bedirected at the liver failure and ascites, with diuresis and saltrestriction as the initial steps in management. Decompression of the portal circulation, percutaneously or surgically,may be indicatedto treat the underlying disease. If the pleuraleffusion is unresponsive to these measures, or if pulmonarysymptoms necessitate intervention, the options includedrainage and pleurodesis. Sometimes surgical intervention isindicated, combining closure of a demonstrated peritonealpleural communication with pleurodesis, t hi s has beenaccomplished using VATS techniques as well as thoracotomy.34,35 Shunting ascites to the venous sys tem is anotheroption; however, these patients are generally poor surgicalcandidates unless their liver failure is corrected. It is best toavoid placement of a chest tube for drainage of a pleural effusion secondary to cirrhosis as the high drainage rates fromdecompression of ascites across the diaphragm can makethese tubes difficult to remove.
Nephrotic syndrome is another disorder associated withpleural transudates. These effusions tend to be bilateral andresult from decreased plasma oncotic pressure. Again, treatment shou ld be a imed at the primary disorder. In severelysymptomatic patients, drainage and sclerosis can be considered. Other conditions that may provoke a transuda tive
effusion include, bu t are not l imited to, pulmonaryembolism, superiorvena cava obstruction, peritoneal dialysis,myxedema, glomerulonephritis, Meigs syndrome, andsarcoidosis.
Exudative EffusionsExudative effusions can be broadly grouped into benign andmalignant effusions. The malignant effusions arise most commonly from metastatic disease bu t can also herald the presence ofa primary malignancy of the pleura. The benign causesof exudative effusion include a long list of conditions, including, but not limited to, infectious diseases, pulmonary embolism, collagen vascular diseases, drug-induced disorders,bleeding, chyle leak, subdiaphragmatic infections, pancreatitis, and esophageal perforation. If the cause is not obvious,then a thoracentesis should be the next step in diagnosing theetiology of the effusion. The following sections discuss theconditions most likely to be encountered by the surgeon.
MALIGNANT EFFUSIONS
Malignant effusions represent one of the most common indications for chest tube placement. The tumors most frequentlyassociated with a pleural effusion include lung cancer, breastcancer, ovarian cancer, and lymphoma. Dyspnea from pulmo-
8/11/2019 Pleura a&P and Disorders
11/20
8/11/2019 Pleura a&P and Disorders
12/20
1562 C H A P T E R 74
vides good palliation. Commercial kits such as the Pleurexcatheter (Denver Biomedical, Denver CO) are available.Another opt ion would be placement of a pleuroperi tonealshunt for internal drainage of the pleural space and decompression of the lung. Internal drainage can be accomplishedby implanting a shunt, s uch as the Denver Shunt (DenverBiomaterials), which has a pumping chamber t ha t the patientcan press to transfer fluid across the negative pressure gradient from the pleural cavity to th e peritoneal cavity. There are
a number of downsides to this option. Placement requires anoperation, usually under general anesthesia; a small percentage of the shunts will obstruct; and the patient must activelypump the shunt to transfer fluid.
Thoracotomy with decortication, in the presence of amalignant effusion, is rarely indicated. Although highly variable, the average survival of a patient with a malignant effusion from lung cancer is on the order of 4 months, whereasfor breast or ovarian cancer it may be more in the range of 7to 9 months.f Thus, recovery from such an operation is likelyto result in decreased quali ty of life for a significant portionof the patient's remaining time.
BENIGN EFFUSIONS
Effusions associated with pneumonia (parapneumonic effusions) are the most common cause of benign exudative effusions. They result from visceral pleural inflammation thatalters the normal fluid balance of the pleural space. Theseeffusions may initial ly be steri le, bu t if the parenchymalinfection spreads to the effusion, an empyema results. Thereis a continuum that reflects th e natural history of untreatedparapneumonic effusions, from a thin, clear sterile collectionto an infected fibrous peel encasing the lung.
The first stage is the exudative stage, characterized byfluid exuding from the lung into the pleural space, likely fromthe pulmonary interst it ial space. This stage should resolve
with antibiotic therapy and generally does no t require drainage. Normal pH and glucose with a low LDH and white bloodcell count are characteristic of the fluid at this stage.
Untreated, the effusion is likely to progress to the [ibto-purulent stage, characterized by increased fluid that is heavilyladen with white blood cells, microorganisms, and cellulardebris. Fibrin is deposited on the pleural surfaces, and th estage is set for pulmonary entrapment. At this point, the fluidpH and glucose level fall, and th e LDH rises. Chest tube drainage is indicated bu t becomes more difficult as the effusionloculates with fibrinous septae.
The final stage is th e organizational stage, during whichfibroblasts grow into th e effusion, laying down a thick fibrouspeel that encases th e lung and resul ts in ent rapment. Theremaining effusion is thick and infected and may necessitatethrough the chest wall or into the lung.
The presentationofa parapneumonic effusion or empyemadepends, to a ce rta in extent, on the organism causing theinfection. For aerobic organisms, the presence of the effusionhas l it tl e impac t on the clinical picture, which is that of abacterial pneumonia: fever, chest pain, and a productivecough. An anaerobic infection, frequently as a result ofaspiration, is more likely to present in a subacute manner. A patientwith an anaerobic empyema may have symptoms for morethan a week before seeking medical help, and significantweight loss may be a chief component of their presentation.
DIAGNOSIS
True empyema thoracis is simply defined aspus in the pleuralspace, a clear indication for drainage. For a small simple parapneumonic effusion in a patie nt being treated with andresponding to appropriate antibiotics, there is no indicationfor drainage. The issue is how to identify the effusion that isnot yet frankly purulent bu t will require drainage to resolve.If the patient with pneumonia continues to have a large orincreasing effusion, then a thoracentesis should be per
formed.The fluid from the tap should be sent for analysis of
glucose, pH, LDH, amylase, protein, complete blood countwith differential, Gram stain, aerobic/anaerobic bacterial cultures, and if indicated, special microorganism cultures andstains. If malignancy is suspected, cytology should also besent. As seen in Table 74.5 from the American College ofChest Physicians Parapneumonic Effusions Panel EvidenceBased Guideline, th e risk outcome can be stratified and usedto determine whether drainage is warranted. These remain,however, only guidelines, and sound cl inical judgment isessential.
TREATMENT
Once the decision has been made to drain the fluid collection,a number of options are available: aspiration, ches t tubedrainage, VATS drainage, l imited thoracotomy and opendrainage, or full thoracotomy with drainage and decortication. For diagnosis and ini tial t reatment of a free-flowingpleural effusion, aspiration is an appropriate initial step. If theclinical situation mandates further drainage, then the clinician has several options. If the effusion is free flowing, thenplacement of a standard chest tube is a reasonable option. Ifthe effusion is loculated, ultrasound guidance may be helpfuleither for marking th e ideal location for thoracentesis or thoracostomy tube placement or for placement of a percutaneousdrainage catheter. The use of intrapleural streptokinase or
urokinase has been advocated if drainage fails due to loculations. In several well-constructed studies, however, it hasbeen shown that enzymatic treatment will increase thevolume ofchest tube output bu t not affect the clinical course.The role of these agents for treatment of empyema remainsundefined.
There are several surgical options for patients with anempyema. The goals of surgical therapy are to establish drainage and, depending on the situation, to eliminate space in thepleura l cavity. Space elimination can be accomplished bydecortication to allow the lung to expand, collapsing the chestwall with a thoracoplasty, or transposing muscle flaps to fillthe space. A critical component is always to establish drainage. The least-invasive option is to explore the chest cavitythoracoscopically, disrupt loculations, debride the visceralpleura, and strategically place chest tubes. Frequently, it ispossible to accomplish this procedure utilizing the patient'sexist ing chest tube sites as video ports. This opt ion is mostl ikely to be successful if performed in the exudative or earlyfibrinopurulent stages.
Once in the organizational stage, the lung is encased in afibrous peel that most often requires an open thoracotomy toadequately remove. If the pat ient is able to tolerate such aprocedure, then this represents the most effective treatmentof the problem. The goal in such a situation is to drain theinfec tion and obl iterate any space with reexpanded lung
8/11/2019 Pleura a&P and Disorders
13/20
P L E U R A : A N ATO M Y, P H YS IO L OG Y, A ND D I S O R D E R S 1563
TABLE74.5. Categorizing Risk for Poor Outcome in Patients with Parapneumonic Effusions.
Pleural fluid Risk of poorPleural space anatomy Pleural fluid bacteriology chemistry Category outcome Drainage
Av minimal, free-flowing effusion AND Bx: culture and Gram AND pH unknown Very low Noe[cl Omm on lateral decubitus]: stain results
unknown
Al small-to-moderate free- AND Bo: negative culture AND Co: pH > 7.20 2 Low Noeflowing effusion (>10mm and and Gram stain< 1/ 2 hemithorax)
A2 l a r g e free-flowing effusion OR B1: positive culture or OR C 1: pH < 7.20 3 Moderate Yes(>1.2 hemithorax,' loculated Gram staineffusion, g or effusion withthickened parietal pleura] B2: pus 4 High Yes
1' H is the preferred pleural fluid chemistry test, and pH must be determined using a blood gas analyzer. If a blood gas analyzer is not available, pleural fluid glucoseshould be used Po glucose> 60mgjdL; Pi glucose < 60mgjdL). The panel cautions that the clinical ut il ity and decision thresholds for pH and glucose have notbeen well established. Clinical experience indicates that effusions of this size do not require thoracentesis for evaluation bu t will resolve.
elf thoracentesis were performed in a patient with o category pleural anatomy and Pi and B i status found, clinical experience suggests that the Pi or B, f indingsmight be a false-positive result. Repeat thoracentesis should be considered if effusion enlarges or clinical condition deteriorates.dRegardless of prior use of antibiotics.
elf clinical condition deteriorates, repeat thoracentesis and drainage should be considered.'Larger effusions are more resistant to effective drainage, possibly because of the increased likelihood that large effusions will also be loculated.
gPleuralloculations suggest a worse prognosis.
Thickened parietal pleura on contrast-enhanced CT suggests presence of empyema.
Source: From Colice et al.,43 with permission from Chest.
t issue. If a portion of the lung has already been removed or ifthe infection has rendered portions nonviable, mandatingresection, then space may become an issue. The favoredopt ion is to t ranspose muscle flaps into the chest cavity toobliterate any residual space that exists after the lung hasbeen decorticated and reexpanded. The commonly usedmuscle flaps are serratus, latissimus, and pectoralis. Omentumis also a good option. A good approach in these cases is toenter the chest through a vertically oriented muscle-sparing
thoracotomy such that both serratus and latissimus are sparedand can be harvested if necessary.After a drainage procedure, the clinician is faced with the
management of the chest tubes. The classic treatment of achest tube placed into an empyema is to leave it to closedsuction drainage for 2 to 3 weeks. Thereafter, the tubes aretaken off suction and converted to open drainage, slowlywithdrawing them over the course of several more weeks.Ano the r op tion is to leave the tubes in place for approximately 1 week on suction. If the lung is fully expanded, drainage is minimal SOmL/day), and the pat ient has no fur thersigns of infection, then the tubes may be removed. The critical point is t ha t t he lung must be fully expanded. Cases inwhich this strategy is safe and effective usually demonstrate
full expansion of the lung on the chest x-ray and walling offof the chest tube, characterized by essentially no drainage andlack of respiratory variation in the waterseal chamber of thePleur-evac.
For patients with chronic empyema or empyema withbronchopleural fistula or patients unable to tolerate thoracotomy, an open drainage procedure may represent the bestoption. These procedures involve localizing the most dependent portion of the empyema cavity and resecting a portionof the overlying rib. The cavity is then entered, the pleuralspace debrided, and if possible, the lung decorticated. Depending on the size of the cavity, it may close spontaneously or
may require reconstruction, usually with a muscle flap. In anelderly or infirm patient, the cavity may be left open. Givenenough time, even cavities of substantial size will commonlyclose.
BENIGN EFFUSIONS, EFFUSIONS FROM OTHER CAUSES
INFECTIOUS NONBACTERIAL
Almost any organism can cause an infection associated with
a pleural effusion. Tuberculosis may cause a pleural effusionthat tends to be unilateral and of moderate size. They can bedifficult to diagnose based on chemical and microbiologicalevaluation of the pleural fluid bu t usually demonstrate granulomatous pleuritis on closed pleural biopsy if the diagnosisis in doubt. The effusion usually responds to appropriateantibiotic therapy and, unless symptomatic or part ofa mixedempyema, usually does not require drainage or surgery.
Viral effusions usually elude diagnosis and are self-limited.Human immunodeficiency virus HIV) does no t appear tocause pleural effusions, but patients with HIV are more likelyto develop pleural complications associated with a bacterialpneumonia.
Effusions may accompany any of a number of fungal pulmonary infections. The primary treatment is appropriate antibiotic therapy and, depending on the infection, drainage. Ofnote, Aspergillus empyemas are almost always associatedwith a bronchopleural fistula, or a history of previoustreatment of tuberculosis with artificial pneumothorax, andalmost always requi re surgical evacuat ion as par t of theirtreatment.
Although relatively uncommon in the United States, theclinician should be aware that pleural effusions frequentlyaccompany a number of parasitic infections. Again, appropriate drug therapy is essent ial. Of note, rupture of pleural orhepatic cysts into the pleural space can present with acute
8/11/2019 Pleura a&P and Disorders
14/20
1564 C H A P T E R 74
symptoms and, as in th e case of Echinococcus, may representan indication for urgent thoracotomy to debride and drain thepleural space and to drain the original cyst.
PULMONARY EMBOLI
Pleural effusions may accompany pulmonary emboli in 300/0to 500/0 of cases. Although the majority of these effusions areexudative, approximately one-quarter may be transudative.This is l ike ly to be determined by the re lat ive contr ibut ion
to the effusion by the two mechanisms thought to be primarily responsible for the effusion. Transudative effusions arethought to exude from the parietal pleura secondary to rightheart failure. Exudative effusions are thought to arise fromthe visceral pleural secondary to release of local factors fromthe emboli that increase capillary permeability. The treatment for pulmonary emboli with effusion is the same as forpulmonary emboli without effusion, and as always, the keyfactor is to consider the diagnosis in a patient with any of thesymptoms suggestive of pulmonary embolus.
SUBDIAPHRAGMATIC PATHOLOGY
Inflammation or malignancy below the diaphragm can causeexudative pleural effusions as well as transudative effusionssecondary to hepatic or renal dysfunction, as discussed in thetransudative effusion section. Acute pancreatitis generallyleads to a left-sided effusion, l ikely as a resul t of transdiaphragmatic transfer of exudative ascites arising from pancreatic inflammation. The fluid almost always has an elevatedamylase, and that amylase is frequently higher than the serumamylase. The fluid generally resolves with resolution of thepancreatic inflammation. Pancreatic abscess can also cause apleural effusion; again, the t reatment is the usual treatmentof a pancreatic abscess. A pancreatic pseudocyst can decompress into the pleura l space, forming a pancreaticopleura lfistula. These effusions tend to be large, usual ly left sided,very high in amylase, and usually accompanied by chest, not
abdominal, symptoms. This finding is thought to be secondary to decompression of th e pseudocyst into the thorax. Treatment of this disorder is conservative, th e same as the initialtreatment of any pancreatic pseudocyst. The role of drainageof the effusion remains controversial, and the clinician shouldbe aware of the risk ofinfection and the fact that the drainageis l ikely to be massive and to reaccumulate rapidly unt i l thefistula has closed. Should conservative treatment fail, a percutaneous or surgical drainage procedure should be planned.Subphrenic abscess from any number of intr aabdomina lsources can lead to an exudative effusion. The effusions rarelyare cul tu re positive and tend to have a very high whit e cellcount, yet the pH is usually above 7.20, and the glucose isusually greater than 60mgjdl. Treatment of the effusionshould be symptomatic as th e approach is treatment of theabscess and its underlying cause. The effusion usually resolveswith these measures.
The clinician is advised always to consider esophagealperforation in the diagnosis of a pleural effusion, particularlyafter instrumentation of the esophagus or retching. Iatrogenicinjuryaccounts for two-thirds ofthese injuries, and the patientfrequently complains of chest pain. The condition usuallypresents with a left-sided effusion, bu t it may be e ithe r sideor bilateral and accompanied by, or replaced with, a pneumothorax. The fluid is almost always high in amylase from salivathat has leaked into the pleural space. The mortali ty rate is
high, up to 600/0, which underscores th e imperative of promptdiagnosis. If the diagnosis is being entertained, a contras tswallow study should be obta ined. Treatment depends onhow early the disruption is diagnosed and ranges from primaryrepair to esophageal exclusion. Pleural drainage, cessation ofongoing pleural soilage, nutritional support and antibioticsare necessary components of the treatment strategy.
CHYLOTHORAX
Chylothorax is an exudative effusion caused by disruption ofthe lymphatics in the chest, most commonly the thoracicduct, and subsequent drainage of chyle into the pleural space.The initial presentation of a chylothorax is determined by thesize of effusion and its mechanical effects within the hemithorax. Once a chest tube is in place, the symptoms aredetermined by the persistence of the drainage. The longer thedrainage continues, the more dangerous it becomes, with theconsequences being dehydration, nutritional depletion, andimmunocompromise.
More than 50% of chylothoraces are secondary to ductalobstruction and disruption by tumor, with lymphomaaccounting for 75% of these cases. Approximately 250/0 ofchyle leaks are traumatic, with iatrogenic t rauma the mostcommon. Of the iatrogenic causes, esophageal resection is theleading cause and is more common with transhiatal esophagectomies than transthoracic esophagectomies. The diagnosisis established by analysis of the fluid. Although classicallythought ofas milky in appearance, chyle may appear serosanguinous, particularly in the fasting state. A triglyceride levelin the fluid greater than 110mgjdL is highly suggestive ofchyle, whereas a level below 50mgjdL essentially excludesthe diagnosis of chylothorax. Intermediate values require alipoprotein analysis to prove the presence of chylomicrons toestablish the diagnosis. Some believe t ha t the most reliabletes t is to give an oral challenge of cream and to observe thetube drainage for gross changes.
The treatment of chylothorax remains controversial;some authors advocate a generous period of conservat ivetreatment, while others recommend early intervention. Allagree that a prolonged, high-output leak can be devastating.Conservative therapy involves pleural drainage and total parenteral nut ri tion . If the leak is secondary to a malignancy,then chemotherapy or radiation therapy may be the treatmentof choice.
For other chylothoraces, surgical intervention is indicatedwhen conservative measures have failed. The timing of suchintervention is debatable, bu t most authors agree it is unwiseto wa it more than 1 week in the setting of an unremitt ingleak. It is important not to wai t unt i l the patient is immunocompromised and nutritionally depleted before deciding to
operate as this would unnecessari ly increase the risk of thesurgery. At the time of surgery, heavy cream is administeredvia nasogastric tube immediately after intubation; this makesthe duct more visible and may also identify the area ofleakage.A number of surgical options are available, including parietalpleurectomy, direct ligation of th e leak, and mass ligation ofthe duct. Mass ligation offersat least an 800/0 chance of resolving t he l eak. Many advocate performing a ligation of theduct on the right side, just as it emerges from the diaphragm,regardless of the side of the chylothorax. This liga tion hastraditionally been performed through a small thoracotomyincision in the sixth or seventh interspace. This procedure is
8/11/2019 Pleura a&P and Disorders
15/20
PLEURA: A N AT O M Y , PH Y S I O L O G Y, A N D D I S O R D E R S 1565
FIGUR 74.6. Intraoperative photograph through a video thoracoscope shows probe under the thoracic duct, which has been dissectedfree at the level of the diaphragm on the right side. Note thoracicduct, aorta, lung, and diaphragm . This duct was clipped and ligatedvia this VATS(video-assisted thoracoscopicsurgery]approach throughthree lO-mm incisions that resul ted in immediate and completeresolution of the patient's chyle leak.
readily accomplished thoracoscopically , utilizing three 1 .0- to1.S-cmport incisions Fig. 74.6) . This procedure seems to offerless morbidity and equal efficacy to the open procedure . If theexpertise exists , occlusion of the duct by interventional radiologists may be an option and would be the intermediate stepto consider between failure of conservative therapy and surgical l igation of the duct . Should all other measures fail, or ifthe right chest is host ile, the duct can be approached transabdominally in the aortic hiatus .
HEMOTHORAX
The overwhelming majority of hemothoraces are caused by
trauma, including iatrogenic trauma. There are other, significantly less common, causes, including bleeding from metas ta ti c tumors involving the pleura, hemorrhage duringanticoagulation therapy for pulmonary emboli, and catamenial hemothorax . The potential consequences of an undrainedhemothorax include conversion to an empyema , provocationof a pleural effusion, and conversion to a fibrothorax withlung entrapment . The ini tial t reatment of any hemothoraxshould be pleural drainage with a large-bore (32-or 36-French)chest tube. If the tube becomes clogged or is inadequate ,additional tubes should be strategically placed .
Up to 4 % of hemothoraces will become infected . Thiscomplication is more common in patients admitted in shock ,with gross contamination of the pleura at the time of injury ,with prolonged chest tube drainage , and with concomitantabdominal injuries . The pleural effusion associated withhemothoraces may occur after the blood has been evacuatedand the chest tubes are removed . If the fluid is infec ted , itshould be treated accordingly. If not , these effusions tend tobe self-limited and require no further intervention . Use ofVATSis safe and effective in evacuating blood from the chestcavity. In a prospective randomized trial , early VATS drainageof re ta ined hemothorax was found to decrease durat ion oftube drainage, hospital stay, and cost . The earlier clot evacuation is attempted, the more likely VATS evacuation willbe completely successful. In addition, if intervention is insti -
tuted early, the entire operation can frequently be performedthrough the existing chest tube incisions, occasionally requiring one additional videoscopic port incision.
MISCELLANEOUS
Collagen vascular disorders may be associated with pleuraleffusions. In each case, the treatment of the effusion is symptomatic, with the primary therapy treatment of the underlying disorder. The two most common diseases are rheumatoid
a rthri ti s and systemic lupus e rythema tous . Rheumato iddisease may involve the pulmonary parenchyma as well asthe pleura.
There are numerous other causes of exudative effusions.These include but are not l imi ted to cardiac surgery, lungtransplantation, asbestos exposure, Dressler's syndrome,Meigs syndrome, yellow nail syndrome, sarcoid, postpartumstate, trapped lung, radiation exposure, ovarian hyperstimulation, amyloidosis, acute respiratorydistress syndrome ARDS),electrical bums, and uremia .
Solid Disorders of the Pleural Space
A limited number of benign and mal ignant solid disordersaffect the pleura . The most common benign conditions arefibrothorax, pleural plaques, diffuse pleural thickening, andbenign fibrous tumors of the pleura. The mos t commonmalignancies are tumors metastatic to the pleura. The primarymalignancy of the mesothelium is mesothelioma, and numerous cancers, such as liposarcoma and fibrosarcoma, may arisefrom any of the elements forming the connective tissue layerof the pleura.
Benign Disorders
Fibrothorax results from deposition of a thick fibrous layer
along the pleural surface . This layer may cause entrapmentof the lung as well as contraction and immobility of the skeletal hemithorax . The most common causes of fibrothorax arehemothorax, tuberculosis, and bacterial pneumonia.
The treatment of fibrothorax is decortication, which isgenerally a major operation requiring a full thoracotomy .Patients who are being considered for decortication should below -risk surgical candidates who are symptomatic from theirrestriction and have pulmonary parenchyma that is anticipated to expand on release . Generally, the indication issignificant pulmonary compromise in a patient whosefibrothorax is stable or has been worsening for at least severalmonths (Fig . 74.7).
The pathogenesis of pleural plaques remains unclear.They are thought to be predominant ly caused by asbestos,perhaps secondary to release of local factors in response tothe foreign body after macrophage phagocytosis. Pleuralplaques are hard, raised , discrete areas involving the parietalpleura, par ticular ly in the lateral, pos ter ior por tion of thehemithorax ; 80% of pleural plaques that are due to asbestosare bilateral, with the majority of unilateral plaques thoughtto be secondary to other causes. Pleural plaques do not appearto be predecessors of mesothelioma. f
Diffuse pleural thickening, like pleural plaques, appearsto be predominan tly related to asbestos exposure. O thercauses, such as drug reaction, hemothorax, and tuberculosis
8/11/2019 Pleura a&P and Disorders
16/20
1566 C H A P T E R 74
A
FIGURE 74.7. Anteroposterior radiograph of the chest (AI demonstrates scoliosis and volume loss resulting from a flbrothorax causedby a tuberculous empyema . Computed tomographic cross section B)demonstrates the thick parietal pleural peel entrapping healthy lung
have been reported . Unlike pleural plaques , however, diffusepleural thickening affects the visceral pleura . Its exact etiology also remains unclear , bu t it is thought that inflammatoryfactors are like ly to play a major role, particularly in thesetting of a resolving asbestos -induced pleural effusion. Thereappears to be an initial decrease in pulmonary function associated with diffuse pleural thickening that tends to remainstable over time. Again, there is no specific treatment recommended, just routine surveillance .
The benign fibrous tumor of the pleurais rare and primary .These tumors arise from the visceral pleura, are not associated with asbestos, and are frequently discovered incidentally
on chest x-ray . These tumors may reach enormous size,thereby causing symptoms by virtue of compression of otherstructures (Fig . 74.8). Surgery is the treatment of choice andis almost always curative .52
Solid Malignancies of th e PleuraThe most common malignancies of the pleura are metastatic,predominantly from lung, breast , or colon primaries Fig.74.9) . There are rare primary sarcomas arising from the connective tissue elements of the pleura , but the most commonprimary malignancy of the pleura is mesothelioma . Essentially all malignancies of the pleura portend a grim prognosisas a resul t of e ither the ir conferment of metas ta tic s ta tus orthe recalcitrance of the vast majority of de novo pleural malignancies to current treatments.
Mesothelioma is a rare tumor, with only 1500 to 3000cases per year in the United States, bu t is thought to be onthe rise in both the United States and intemationally. This isthought to be primarily related to the 20- to SO-year lagbetween asbestos exposure, with which there is a clear causallink, and the relatively recent or lax restrictions on the useof asbestos .P ' Another epidemiological factor of greatconcern is the link between the simian vacuolating virus 40 SV40) and mesothelioma . The virus has been demonstratedin human mesotheliomas and is capable of inducing meso-
B
parenchyma. Notice contraction and overlapping of ribs in bothradiographs . The patient underwent a decortication with dramaticimprovement of her scoliosis and pulm onary funct ion .
thelioma by itself in animal models . It has been identified asa contaminant in mill ions of vaccines adminis tered in theUnited States and may be a predisposing factor to mesothelioma formation in humans .
Pleural mesothelioma is almost always unilateral and isdiagnosed by pleural biopsy. From the time of diagnosis, themedian survival is 4 to 12 months . The tumor usually presents with dyspnea secondary to a pleural effusion bu t mayalso present with chest pain or constitutional symptoms . Thecancer tends to l ine the chest cavity as a thick, plaque-likemass, fusing the two pleural layers and invaginating betweenthe lobes of the lung Fig. 74.10) . It progresses inexorably in
a locoregional manner, invading lung , diaphragm, pericardium, and chest wall. Contrary to popular belief, the diseasealso has the capacity to metastasize, bu t the lethali ty of thelocoregional disease tends to preclude the clinical manifestat ion of any metastat ic disease unless the natural h is tory ofthe cancer is altered by a successfullocoregional treatment .
Al though a number of staging syst ems exist, none hasbeen universally adopted, although most incorporate theusual characteristics of the TN M system . This is likely areflection of the small number of patients and even smallernumber of centers investigating this disease. A staging systemshou ld accurately stratify prognosis, and thi s aspect of astaging system continues to evade researchers . As an example,cell type of mesothelioma (epithelial, sarcomatous, or mixed)is not currently part of any staging system, although some ofthe best results to date have been reportedin patientsrestrictedto the epithelial cell type, with 39% 5-year survival forpatients treated with surgery, radiation, and chemotherapy. Asa result ofthis deficiency in macroscopic staging , researchers are looking toward innovative technologies, like geneticprofiling, in an effort to bet te r dete rmine prognosis andwhich pa ti en ts migh t benefit from aggressive t reatmentprotocols.
There remains no accepted treatment for mesothelioma .Because of the tumor's diffuse nature, complex anatomic presentation, and inhe rent recalcitrance to most t reatment
8/11/2019 Pleura a&P and Disorders
17/20
P L E U R A : A NA T O M Y , P H Y S I O L O G Y , A ND D I S O R D E R S 1567
A
c
B
FIGUR 74.8. Coronal A) and sagittal [B] MRI images demonstrate a large benignfibrous tumor of the pleura occupying the greater part of the right hemithorax .This patient presented with compla ints ofbilateral lower-extremity swelling thatproved secondary to inferior vena cava compression . Photograph (e) shows theresected mass that arose from the visceral pleura ofthe right middle lobe and thatwas readily separated from the remainder ofthe lung with a sm all wedge resectionof the affected area.
modalities, it is an extremely difficult cancer to treat. Becauseof encasement of the lung and potential pulmonary toxicity ,there is no role for radiation as single -modality definitivetreatment . Radiation can be used with curative intent, as an
FIGUR 74.9. Intraoperative photograph through a videothoracoscope shows metastatic cancer implants on the parietal pleura on thechest wall. (Reprinted with permission from Friedberg and Kniger . 1998 Greenwi ch Medical Media Ltd . and by permiss ion of Cambridge University Press .]
adjuvant treatment combined with surgery in which the lunghas been removed , or in a palliative manner for localized areasof symptomatic invasion . Mesothelioma has proven to be oneof the mos t chemoresi st an t tumors tha t oncologists face .Cytotoxic agents have rarely yielded response rates greaterthan 30% . There have, however, been some encouragingresults with newer chemotherapeutic agents , especially antimetabolites , which have shown response rates as high as 45%when used in combination with platinum-based conventionalchemotherapy .
To date, the t reatments that have me t with the greatestmeasure of success for pleural mesothelioma are those thatcombine surgery, for debulking, and o ther modali ties toaddress the residual disease that almost certainly exists, even
after the most complete resection . The adjuvant treatmentsthat have been performed , some intraoperatively, includeradiation, photodynamic therapy , and hyperthermic chemotherapy intracorporeal lavage . Systemic chemotherapy orimmunotherapy have been used in adjuvant and neoadjuvantcapacities .50 Almost all surgery-based multimodality strategies that are performed with curative intent mandate removalof the lung as part of the debulking and preparation for theadjuvant treatments . Some strategies, such as employment ofphotodynamic therapy for killing residual local disease aftersurgical debulking, may permit the option of performing lungsparing procedures .
8/11/2019 Pleura a&P and Disorders
18/20
1568 C H A P T E R 7 4
A
FIGURE 74 .10. Coronal MRI image (Al demonstrates typical appearance of a mesotheliom a. No t e th e thick rind lining the right hemithorax and invaginating between the lobes of the lung . Photograph
Many cancers can metastasize to the pleural space, bu tone of the most frequently encountered is non-small cell lungcancer (NSCLC) , as either bulky disease or a malignancy.t - In the absence of distant metastases, the presence of pleuraldissemination confers an International System for StagingLung Cancer stage of IIIB based on the pleural disease beingconsidered a T4 tumor. The median survival for patientswith this subset of stag