-
8/3/2019 Respiratory Tract Infections 12
1/43
RESPIRATORY TRACT
INFECTIONS
Presenter: Katisa Godwin MD
-
8/3/2019 Respiratory Tract Infections 12
2/43
Introduction
Infections of the upper and lower respiratorytract continue to
be a major cause of morbidityand mortality throughout the
world,
patients at the extremes of age or with pre-existing lung
disease or immune suppressionbeing at particular risk.
Viruses are the most frequent cause of upper
respiratory illnesses, with bacteria beingresponsible for the
majority of community- andhospital-acquired pneumonia in adults
-
8/3/2019 Respiratory Tract Infections 12
3/43
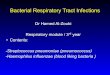
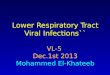
Anatomy of the Respiratory System
-
8/3/2019 Respiratory Tract Infections 12
4/43
URT
nose
nasal cavity
ethmoidal air cells frontal sinuses
maxillary sinuses
Sphenoidal sinuses
Pharynx
larynx
-
8/3/2019 Respiratory Tract Infections 12
5/43
LRT
trachea
Bronchi
bronchioles alveoli
Lung parenchyma
-
8/3/2019 Respiratory Tract Infections 12
6/43
TYPES OF RTIs
Upper respiratory tract infections
Lower respiratory tract infections
-
8/3/2019 Respiratory Tract Infections 12
7/43
URTIs
Burden
Predisposing factors
Aetiology pathogenesis
Types
Clinical features management
-
8/3/2019 Respiratory Tract Infections 12
8/43
Burden ofURTI
Up to of all symptomatic illness
Significant morbidity and direct health care
costs Children may have six to ten episodes a
year. Adult two to four
Occasionally leads to fatal illness Excessive use of antibiotics
a major issue
-
8/3/2019 Respiratory Tract Infections 12
9/43
Predisposing factors
Age,
Mucociliary functions: cystic fibrosis, immotile
cilia syndrome.
Systemic dis., immune deficiency.: DM, AIDS,
CRF
Allergy: Nasal poliposis, asthma
Neoplasia
Environmental: smoking, air pollution,
-
8/3/2019 Respiratory Tract Infections 12
10/43
Aetiological agents
Viral 60% 90%
Bacterial
fungal
-
8/3/2019 Respiratory Tract Infections 12
11/43
Pathogenesis
Before a respiratory disease can beestablished, the following
conditions need to
be met
There must be a sufficient number orsufficient "dose" of
infectious agent inhaled.
The infectious particles must be airborne.
The infectious organism must remain alive
and viable while in the air. The organism must be deposited
on
susceptible tissue in the host.
-
8/3/2019 Respiratory Tract Infections 12
12/43
Pathogenesis
Pathogenic mechanisms:-
Bacterial adherence factors = F and M proteins of
Strep. pyogenes, Hemagglutinins ofB. pertussis.
Extracellular toxins = diphtheria toxin; pertussistoxin.
Growth in host tissue = viruses, chlamydia sp.
Evasion of host defense mechanism = capsules of
Strep. pyogenes (also M protein), S. pneumoniaeand H. influenza
by inhibiting phagocytes
-
8/3/2019 Respiratory Tract Infections 12
13/43
Types ofURTI
Common upper respiratory tract infections
include
Common cold Influenza
Sinusitis
pharyngitis/pharyngotonsilitis
Epiglottitis
laryngitis
-
8/3/2019 Respiratory Tract Infections 12
14/43
Common cold
Most common
Rhinoviruses are the most common viralagents
Other viruses implicated included
coronaviruses,
influenza C,
parainfluenza virus, adenoviruses,
and respiratory syncytial virus
-
8/3/2019 Respiratory Tract Infections 12
15/43
Common cold
Highly contagious, respiratory droplets
spread by
sneezing, coughing,
or hand contact with the nose, eyes, or face
75% of patients infected with rhinovirus
will have symptoms
-
8/3/2019 Respiratory Tract Infections 12
16/43
Common cold: clinical
presentations Has an incubation period of 2 4 days Sneezing
Coughing
hoarseness Malaise
Headache
nasal congestion
scratchy throat
clear, watery rhinorrhea
+ or - mild fever
-
8/3/2019 Respiratory Tract Infections 12
17/43
Common cold: diagnosis
Made on clinical grounds pt symptoms,
nasal exam showing reddened,
edematous mucosa, narrowed nasal
passages, and watery discharge
Viral isolation/culture is not practical
-
8/3/2019 Respiratory Tract Infections 12
18/43
Common Cold: Treatment
No curative treatment
Supportive therapy 10 treatment Fluids,
rest, humidification, and decongestants Analgesics,
antihistamines are also helpful
Antibiotics not indicated
-
8/3/2019 Respiratory Tract Infections 12
19/43
-
8/3/2019 Respiratory Tract Infections 12
20/43
Influenza: clinical presentations
Often necessary to differentiate influenza
from the common cold
Symptoms include high fever, exhaustion,generalized aches, and
cough
Patients occasionally report headache,
nasal congestion, sneezing, and sore
throat
-
8/3/2019 Respiratory Tract Infections 12
21/43
Influenza : Diagnosis
Diagnosis is based on clinical signs and
symptoms
Nasopharyngeal swab or aspirate can beobtained for a rapid
antigen test
Chest x-ray usually normal
-
8/3/2019 Respiratory Tract Infections 12
22/43
Influenza: Treatment
Analgesics and a cough suppressants for
supportive therapy
Amantadine and rimantadine (both atdoses of 200 mg/day) have
been effective
at treating Influenza A.
Zanamivir and Tamiflu are effective for
patients with Influenza A and B, but with
less side effect
-
8/3/2019 Respiratory Tract Infections 12
23/43
Pharyngitis
90% viruses Epstein-Barr virus
Adenovirus
Influenza A, B Coxsackie A
Parainfluenzae
important bacteria includes
S. pyogenes C. diphtheriae
N. gonorrhoeae
-
8/3/2019 Respiratory Tract Infections 12
24/43
Pharyngitis: clinical presentations
Sore throat
Fever > 38 rC
Difficulty in swallowing Headache, fatigue
Muscle pain
pharyngotonsillar hyperemia / exudates
Soft palate petechia
Anterior cervical LAP
-
8/3/2019 Respiratory Tract Infections 12
25/43
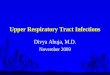
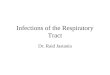
Pharyngotonsilitis
-
8/3/2019 Respiratory Tract Infections 12
26/43
Cont..
-
8/3/2019 Respiratory Tract Infections 12
27/43
Pharyngitis: diagnosis
On PE: observe throat for tonsillar
exudates; obtain throat swab
Rapid streptococcal identification tests aremost commonly used;
there is a sensitivity
of 80% and a specificity of 95%
Throat cultures may be collected if rapid
strep screen is negative
-
8/3/2019 Respiratory Tract Infections 12
28/43
Pharyngitis: Treatment
Symptomatic treatment includes saltwater gargles, PCM,
cool-misthumidification, and throat lozenges
Antibiotics treatment is necessary to treatproven strep
infections
Benzathine penicillin G 1.2 million units as asingle dose, is
optimal therapy
For pen allergic pts, erythromycin 500mg poQID x 10 days or
Azithromycin 500mg oncedaily x 3 days.
-
8/3/2019 Respiratory Tract Infections 12
29/43
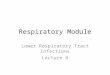
Sinusitis
More common in adult than in children
Organisms
Viral Rhinovirus
Parainfluenzae
Bacterial
S. pneumoniae H. influenzae
fungal
-
8/3/2019 Respiratory Tract Infections 12
30/43
Sinusitis: clinical presentations
feeling of fullness and pressure over the
involved sinuses, nasal congestion, and
purulent nasal discharge
Postnasal drip
Headache
Tenderness on palpation over sinuses,
-
8/3/2019 Respiratory Tract Infections 12
31/43
Cont..
-
8/3/2019 Respiratory Tract Infections 12
32/43
Sinusitis: Diagnosis
Based on clinical signs and symptoms
Sinus radiographs may reveal cloudinessand air fluid levels
-
8/3/2019 Respiratory Tract Infections 12
33/43
Sinusitis: Treatment
Supportive
antibiotics
-
8/3/2019 Respiratory Tract Infections 12
34/43
Acute laryngotracheobronchitis
(croup)
Croup or laryngotracheobronchitis is a
clinical syndrome
COMMON cause of upper airwayobstruction usually mild & self
limiting
BUT is also the commonest cause of
potentially life threatening airway
obstruction in childhood
-
8/3/2019 Respiratory Tract Infections 12
35/43
ALTB: Causes
Commonest cause is viral
parainfluenza, RSV
Influenza virus A and B
-
8/3/2019 Respiratory Tract Infections 12
36/43
ALTB: clinical presentations
Airway obstruction(insp stridor)
Fever
Barking cough Hoarseness of voice
-
8/3/2019 Respiratory Tract Infections 12
37/43
ALTB: Treatment
mild
Reassure parents
Counsel parents re: warning signs
No medication required
Severe
Secure airway
Oxygen
Steroids
epinephrine
-
8/3/2019 Respiratory Tract Infections 12
38/43
Epiglottitis
Serious, life-threatening deep tissue
infection of upper airway
Rapid diagnosis and treatment necessary 2 - 8 year olds most
commonly affected
organisms
H. inftuenzae type B Strep. Pneumoniae
Staph. aureus
-
8/3/2019 Respiratory Tract Infections 12
39/43
Epiglottitis: Clinical Presentation
Sudden onset respiratory distress over 12 - 24 hrs
Fever
Drooling
Dysphagia Dyspnea
Dysphonia
Little or no cough
Anxious, irritable, toxic-appearing
Voice thick, muffled or hoarse
Some inspiratory stridor
-
8/3/2019 Respiratory Tract Infections 12
40/43
Epiglottitis: Diagnosis
Clinical impression important
Direct visualization of the epiglottis risky
Manipulation of oropharynx or examinationwith tongue depressor
may lead to airway
obstruction
Only if patient cooperative and if immediate
intubation possible
-
8/3/2019 Respiratory Tract Infections 12
41/43
Epiglottitis: Treatment
Most important: obtain and maintain an
adequate airway
Broad-spectrum antibiotics coveringH.Influenzae until culture
results available
Second or third generation cephalosporins
Ampicillin
-
8/3/2019 Respiratory Tract Infections 12
42/43
Key points
URTIs are common and self limiting
Most URTIs are viral in origin
Air way transmission Common Sx are cough, sore throat, runny
nose nasal congestion, sneezing, muscle
ache, malaise
Antibiotics only target bacteria
-
8/3/2019 Respiratory Tract Infections 12
43/43
Thank you