Embed Size (px)
Citation preview
Infections of Respiratory
System
Acute Respiratory Infections in Children
Introduction:
Respiratory tract infections are
described according to the areas of
involvement.
The upper respiratory tract or upper airway
consists of primarily the nose & pharynx.
The lower respiratory tract consists of
bronchi & bronchioles.
Acute Upper Respiratory Tract Infections in Children:
Most URTIs are caused by viruses &
are self-limited.
Acute naso-pharyngitis & pharyngitis
(including tonsillitis) are extremely
common in pediatric age groups.
pharyngitis
Inflammation of throat
Winter or early spring
Can be viral or bacterial
Viral
No fever
Less pain
More severe
Symptoms of common cold
H influenza,adenovirus& rhinoviruses
Bacterial
Mostly group A streptococci (15 to 30%)
Fever & pain
Less severe
No flue like symptoms
Unusual pathogens: N.gonnorrhoeae,C.dephtheriae
Lab Diagnosis
The primary goal of lab diagnosis is to differentiate between bacterial and viral pharyngitis
The secondary goal is to be able to detect the uncommon bacterial causes
Specimen Collection
SWAB
swab vigorously the tonsillar areas and posterior pharynx
Avoid tongue and other oral structures (normal flora)
After collecting the specimen, swab may be placed in transport medium

Culture
Culturing the specimen collected will isolate bacterial pathogens (e.g streptoccocci spp)
For culturing a non selective medium is used such as sheep blood agar
Other Methods
LATEX Agglutination Coagglutination test Enzyme immunoassays Rapid antigen detection test (RAPD)
Sinusitis
Viral infection associated with the common cold
Infection of one or more paranasal sinuses
Caused by:
Viral : influenza & para influenza
Bacterial : H.influenzae & C.pneumoniae
Fungal sinusitis are uncommon in normal people but can be found in immuno compromised individuals
Lab Diagnosis
To make a microbial diagnosis of sinus infection , sinus puncture and aspiration is used
Its an invasive and highly painful procedure and is not appropriate for use in routine practice
Only done when person is severely ill or immunocompromised or if there is a suspicion of cranial extension of the infection

Lab Diagnosis
Direct microscopic examination:
Only useful if specimen drawn directly from sinus puncture, gram staining can be done to find dominant bacterial type
Culture :
Samples are inoculated on media such as SBA ,CHOC, MacConky agar
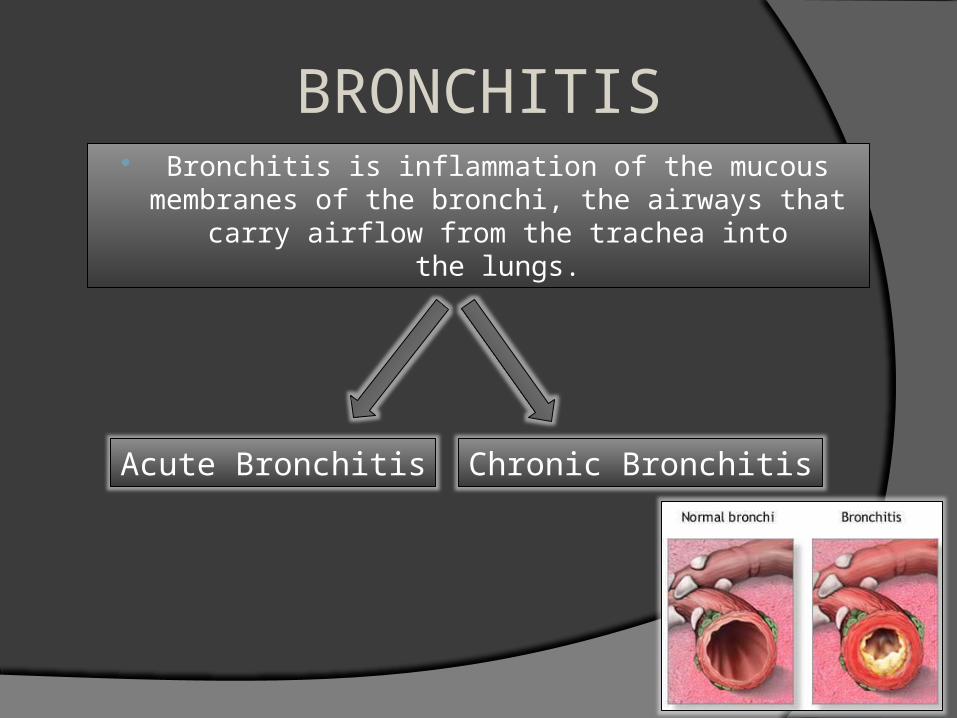
BRONCHITIS Bronchitis is inflammation of the mucous
membranes of the bronchi, the airways that carry airflow from the trachea into the lungs.
Acute Bronchitis Chronic Bronchitis
Acute Bronchitis
Acute bronchitis is an inflammation in the larger branching airways (trachea and bronchi).
Usually arises in connection with a cold or flu.
Chronic Bronchitis A type of chronic obstructive pulmonary disease
Bronchitis is a term that describes inflammation of the bronchial tubes that results in excessive secretions of mucus into the tubes with tissue swelling that may narrow or close off bronchial tubes.
Defined by a productive cough that lasts for 3 months or more per year for at least 2 years
Clinical Manifestations Cough And Fever- Primary Manifestations Sore Throat Runny Nose Nasal Congestion Low-grade Fever Malaise Production of Sputum.
In Case of Chronic Bronchitis Yellow or green colored sputum production Wheezing Shortness of Breath
Acute Bronchiolitis Inflammation of the bronchioles, the smallest air
passages of the lungs.
Infectious disease of infants
Caused by Respiratory Syncytial Virus
Presents coughing, wheezing, and shortness of breath

Laboratory Diagnosis Diagnostic cultures not indicated in
uncomplicated cases In case of secondary bacterial
bronchitis culture data may be useful Collection of sputum minimally
contaminated with oral flora
PneumoniaCommunity Acquired Pneumonia
Nosocomial Pneumonia
Aspiration Pneumonia
Signs and Symptoms
Dyspnea Cough High fever Sweating chills uncontrollable
shaking Sharp or stabbing
chest pain
Rapid, shallow breathing that is often painful
Community Acquired Pneumonia
One of several diseases in which individuals who have not recently been hospitalized develop an infection of the lungs
Occurs because the areas of the lung which absorb oxygen(alveoli) from the atmosphere become filled with fluid and cannot work effectively.
Causes problems like Difficulty breathing Fever Chest pains Cough
Hospital-acquired pneumonia (HAP) or nosocomial pneumonia refers to any pneumonia contracted by a patient in a hospital at least 48–72 hours after being admitted
Usually caused by a bacterial infection, rather than a virus.
Nosocomial Pneumonia
Aspiration pneumonia is bronchopneumonia that develops due to the entrance of foreign materials into the bronchial tree, usually oral or gastric contents (including food, saliva, or nasal secretions)
Aspiration Pneumonia
Laboratory Diagnosis
Involves no risk to patients Care must be taken to avoid
contamination of specimen with oropharengeal flora
Collection of deep sputum in order to get lung secretions not saliva or drainage from nasopharynx
Expectorated sputum examined for its character- preliminary indication
Specimen Collection
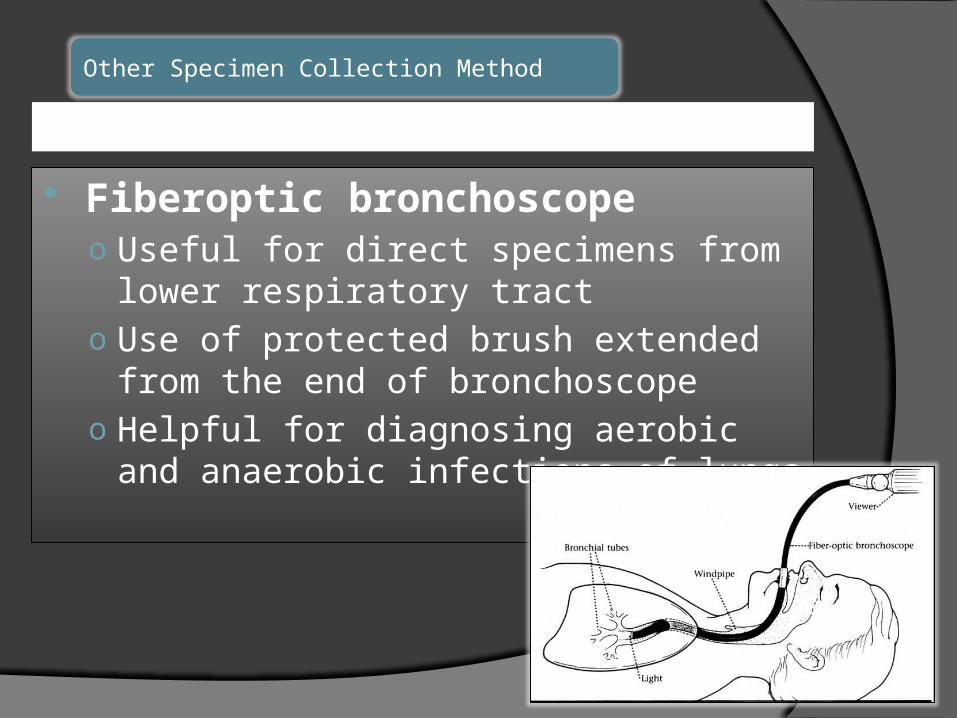
Fiberoptic bronchoscopeo Useful for direct specimens from lower
respiratory tracto Use of protected brush extended from
the end of bronchoscopeo Helpful for diagnosing aerobic and
anaerobic infections of lungs
Other Specimen Collection Method
Quality of specimen determined by a direct Gram- stained smear.
Elimination of contaminants from oropharyngeal region
Determination of neutrophils and epithelial cells under low power magnification
Sample >25 neutrophils and <10 epithelial cells per field- free of contamination
Samples> 25 squamous epithelial cells- should not be cultured
Direct Microscopic Examination
Gastrointestinal Tract Infections
What are GIT infections? It is any infection of the digestive tract caused by
bacteria, viruses or parasites. All may have common clinical features of nausea, vommiting, diarrhoea and anorexia
Causative agents of GIT infections
1. Bacteria (E.coli)2. Virus ( Rotavirus)3. Protozoa ( Entamoeba histolytica)4. Worm ( Ascaris)

Bacterial GIT infections
Symptoms
• Symptoms of dehydration
• Diarrhoea (does not get better in 5 days but get worse)
• Fever• Loss of appetite• Stomach cramping• Pale skin• Blood in stool• Rice water stool
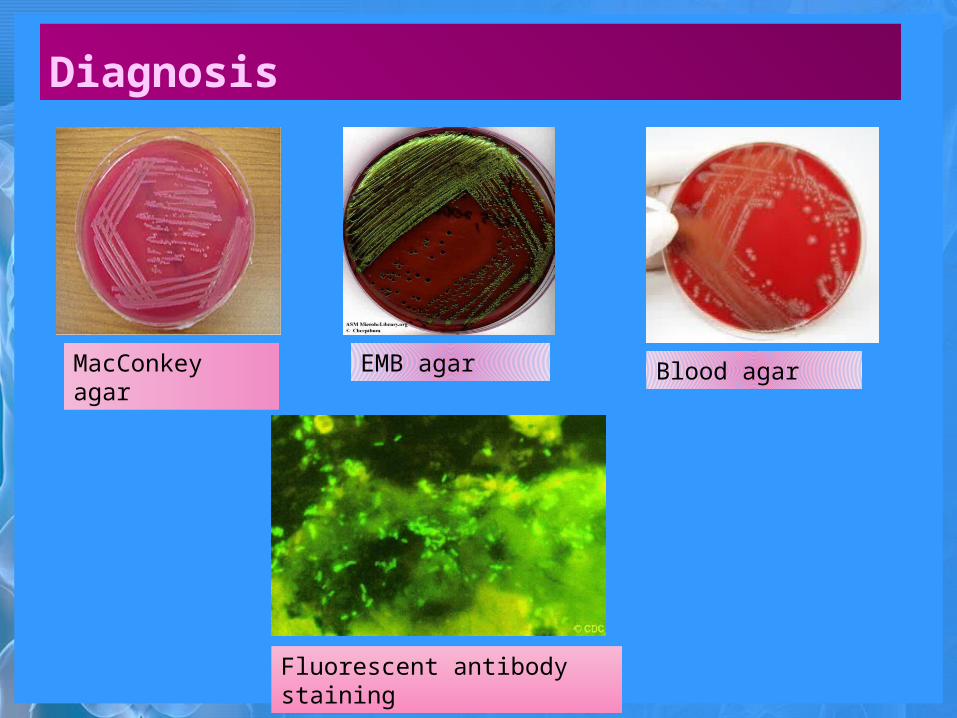
Diagnosis
MacConkey agar
EMB agar Blood agar
Fluorescent antibody staining
Treatment• Antimicrobial agents like trimethoprim-
sulfmethoxazole or an oral penicillin may reduce the symptoms
• Antimotility drugs• Fluid replacement therapy along with oral
rehydration salts• Treatment of HUS (HEMORRHAGIC Uremic
Syndrome) may require dialysis
Viral GIT infections
ROTAVIRUS
• Members of the family Reoviridae• Infect cells of the villi of the small intestine
leading to epithelial atrophy• Decrease the lactase production resulting in milk
intolerance• This decreases the absorptive capacity of bowel
as well as stimulating the enteric nervous system• Viral gastroenteritis is also known as “stomach flu”
Symptoms
Signs of dehydration
• Sunken eyes• Low blood pressure• No tears• Dry or sticky
mouth Abdominal pain Diarrhoea Nausea Chills and fever Joint stiffness Weight loss
Diagnosis
ELISA Latex agglutination assay
Treatment
• Increased fluid intake• Salt replacement (orally or IV)• FDA approved live rotavirus vaccine• No antiviral therapy
AYISHA NASIM***
*FOOD POISONING*
DEFINATION***
• Inflammation of GI tract • Occurs due to consumption of food
containing toxins, which may be due to • microbes secreting toxins (preformed
toxins)• chemicals (Heavy metals)
• Acute onset• Usually < 10 days
IN CASE OF ***
Incubation Period if Short
{Minute to hours}
Chemical toxinsE.g., copper poisoning
Neurotoxins, histamine, allergensE.g. Shellfish toxins

IN CASE OF ***
Incubation Period: Short to medium
{1-12 hours}
Bacterial enterotoxinsE.g., Staphylococcal or
Bacillus cereus
IN CASE OF ***Incubation Period: Long
{6 hours – 10 days}
Bacterial infections
E.g., Salmonella,Shigella

MAIN TYPES OF FOOD POISONING ***Staphylococcal Food Poisoning
Clostridium perfringens
Food Poisoning
BACILLUS CEREUS FOOD
POISONING
Clostridium botulinum
Food Poisoning Shigella
food poisoning
Salmonella food
poisoning
1:STAPHYLOCOCCAL FOOD POISONING***• Scenario – picnic
• Encounter – from skin, nose or wound of infected person
• Entry – bacteria gets in food via contact; toxin gets in person via ingestion
• Spread – toxin spreads
• Multiplication – only in food, not in person
• Avoid Host Immune Response – resistant to stomach acid
• Damage – enterotoxins
2:CLOSTRIDIUM PERFRINGENS FOOD POISONING***• Scenario – cold meat pie
• Encounter – spores contaminate meat, germinate on storage of
cooked stews, etc.• Entry - ingestion
• Spread – toxin may spread, bacteria do not
• Multiplication – bacteria sporulate, don’t replicate; in a food borne infection the bacteria replicate
• Avoid Host Immune Response – bacteria are acid resistant
• Damage – toxin increases capillary permeability resulting in ileal fluid accumulation. It accounts for about 20% of bacterial diarrhoea.
• {done by enterotoxin producing strain type A}• { b-toxin producing type C strain- cause bloody diarrhoea, abdominal pain}
3.CLOSTRIDIUM BOTULINUM FOOD POISONING***
• Encounter - Home canned vegetables, potatoes, fish & preserved sea food• food contaminated with spores • anaerobic conditions
• Entry - Ingestion• Spread – toxin spreads from GI tract to nerve terminals
hematogenously • Multiplication - NONE• Avoid Host Immune Response
• Toxin: Resistant to proteolysis in stomach due to accessory proteins
• Absorption: Alkaline pH of intestine dissociates toxin from proteins, allows absorption into circulation
• Damage – exotoxin produces flaccid paralysis

DIAGNOSIS***
• Gross & microscopic stool examination
• Stool culture• Identification tests• Endoscopy if noninfectious
etiology suspected (inflammatory bowel disease)


TREATMENT***
ELMO
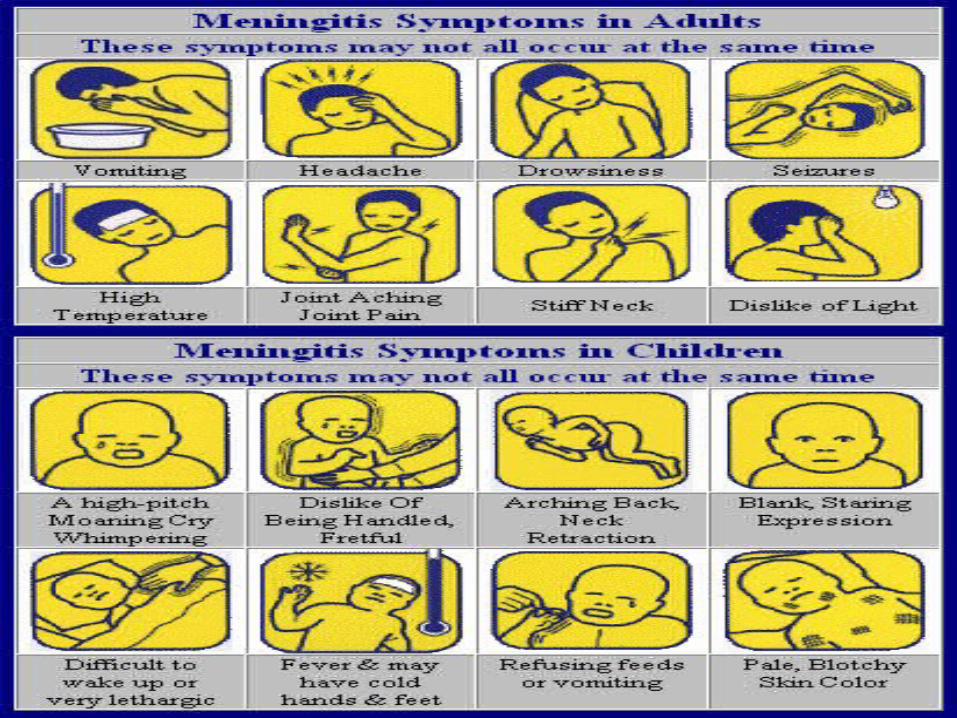
WHAT IS MENINGITIS..??
• an inflammation of the meninges; the membranes that cover the brain and spinal cord
• Condition is classified as medical emergency
BACTERIA
VIRUSFUNGU
S
CERTAIN
DRUGS
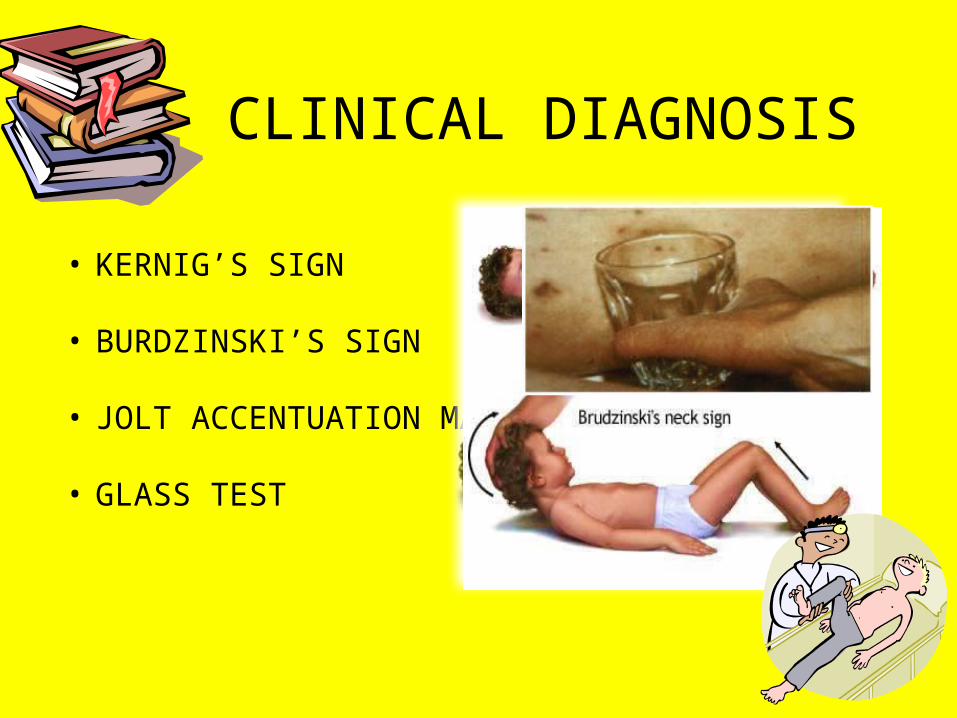
CLINICAL DIAGNOSIS
• KERNIG’S SIGN
• BURDZINSKI’S SIGN
• JOLT ACCENTUATION MANEUVER
• GLASS TEST
• Blood test (complete blood count) LeukocytopeniaPossible thrombocytopenia
• Blood cultures (40-70% positive)• PCR• CSF analysis (Lumbar puncture; ICP
level)• CT and MRI scan
LABORATORY DIAGNOSIS
TREATMENT Antibiotics are given depending upon the
type of infectious agent and clinical manifestations
Usually broad spectrum antibiotics are given initially
ENCEPHALITIS
RABBIYA TAHIR
Encephalitis is an acute inflammation Of the brain mostly due to the infections. Encephalitis with meningitis is known as meningoencephalitis.
DIAGNOSISBRAIN IMAGING
CEREBROSPINAL FLUID TESTS
BLOOD TESTS
BRAIN BIOPSY
Flu like symptoms
Severe symptoms
confusion
drowsiness
Visual sensitivity to light
Irratibility
Stiff neck
Muscle weakness
Sudden impaired judgement
seizures
paralysis
SYMPTOMS
headache
Memory loss
Poor responsivene
ss
TREATMENT
Zovirax Foscavir
Phenytoin Acetaminophen
Dexamethasone

INTRODUCTION
Rabies (From Latin: rabies, "madness") is a viral disease that causes acute encephalitis (inflammation of the brain) in warm-blooded animals.
Rabies, or 'hydrophobia', is known as a disease that makes dogs sick and mad.
When an animal gets sick, it may start to bite. People are most often infected by the bite of a dog, bat or monkey. In Europe the virus is mainly carried by the fox.
CAUSATIVE AGENTThe virus that causes rabies is a
lyssa virus. Lyssavirus is a genus of viruses belonging to the family Rhabdoviridae, in the order Mononegavirales.
SIGNS AND SYMPTOMSSymptoms may include: Anxiety, stress, and tension Drooling Convulsions, Excitability Exaggerated sensation at the bite site Low-grade fever Muscle spasms Numbness and tingling Pain at the site of the bite Restlessness Swallowing difficulty
MODE OF TRANSMISSION The commonest mode of transmission in man is by the bite of
a rabid animal or the contamination of scratch wounds by virus- infected saliva.
Other routes have been implicated in the past, such as through mucous membranes
Infection by aerosol Man to man transmission

DIAGNOSISRabies diagnosis in humans: Several tests are necessary to confirm or rule out rabies in a human.
No single test can be used to rule out rabies in humans with certainty.
Cerebral inclusion bodies called Negri bodies are 100% diagnostic for rabies infection.
Diagnosis can be made from saliva, serum, urine, and cerebrospinal fluid samples, but this is not as sensitive.
The skin biopsy specimen is examined by dFA for the presence of rabies antigen in cutaneous nerves at the base of hair follicles.
Saliva may be tested by virus isolation or nested reverse transcription polymerase chain reaction (RT-PCR) methods.
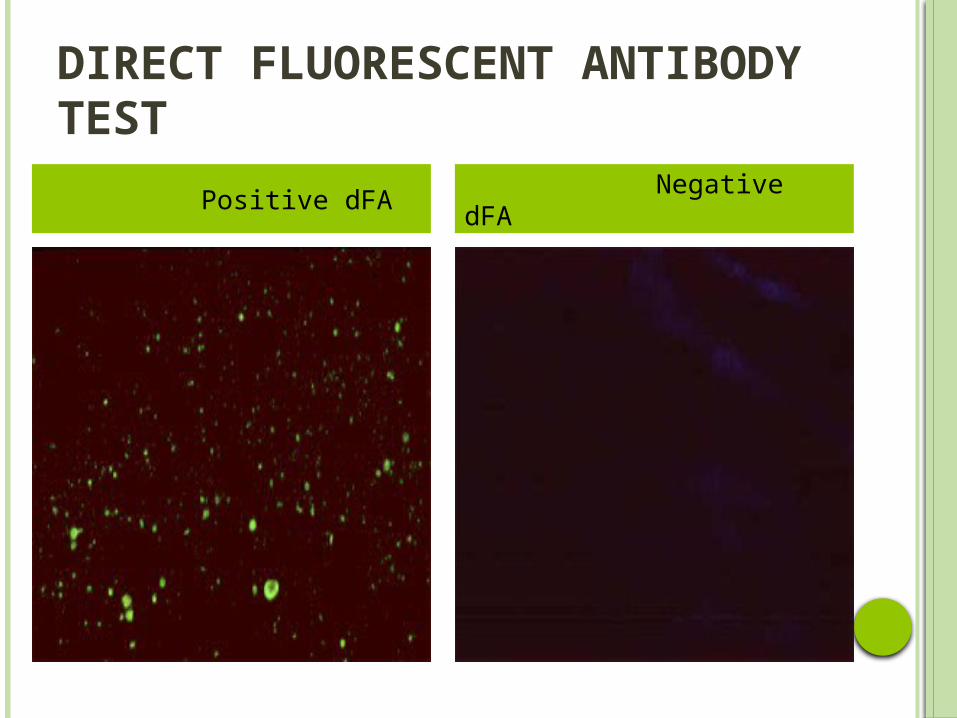
DIRECT FLUORESCENT ANTIBODY TEST
Positive dFA Negative dFA
DIAGNOSIS
Rabies diagnosis in animals:The direct fluorescent antibody test (dFA) is most frequently used to diagnose rabies. This test can be performed on brain tissue of animals suspected of being rabid.
MANAGEMENT AND PREVENTION Once rabies is established, there is nothing much that could be done except intensive supportive care.
However, two decades ago, research scientists developed an extremely effective new rabies treatment regimen that provides protection from the disease.
When administered after an exposure (post-exposure prophylaxis).
The treatment can also be used for protection before an exposure occurs (pre-exposure prophylaxis).
BACTEREMIA…AN INTRO
• Presence of viable bacteria in the bloodstream
• It can be:Sustained/transient Metastatic /systemic leading to meningitis, pericarditis, endocarditis, osteomyelitis and infectious arthritis.
• Development of sepsis (a consequence of bacteremia)
pneumonia
cathetherization
Indewelling devices
Surgical treatment
abscess
Brushing
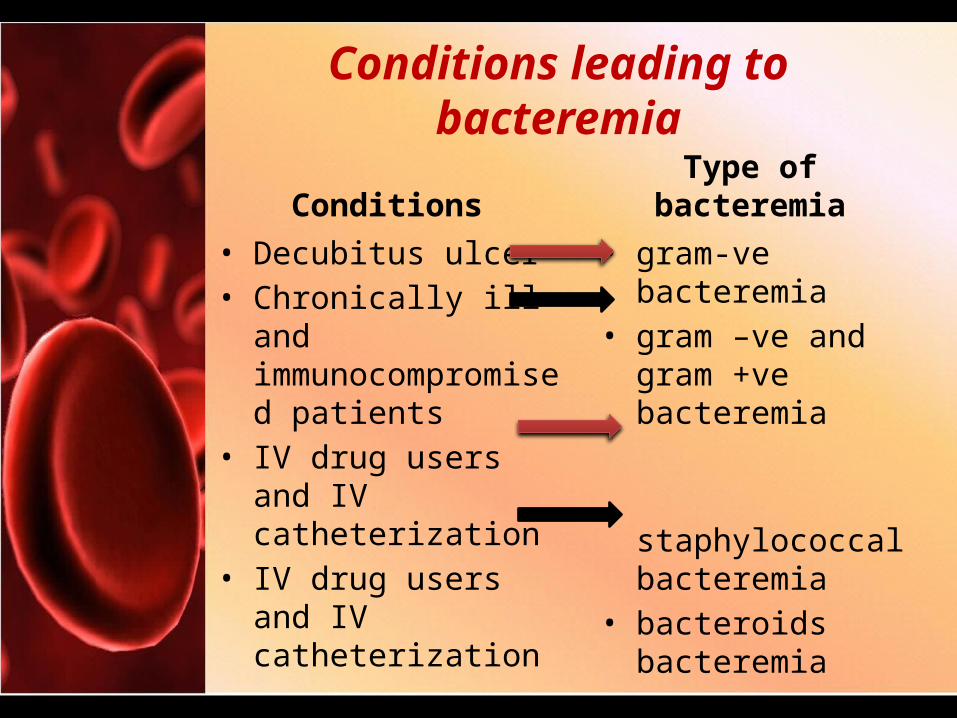
Conditions leading to bacteremia
Conditions• Decubitus ulcer• Chronically ill and immunocompromised patients
• IV drug users and IV catheterization
• IV drug users and IV catheterization
Type of bacteremia• gram-ve bacteremia• gram –ve and gram +ve bacteremia
staphylococcal bacteremia
• bacteroids bacteremia
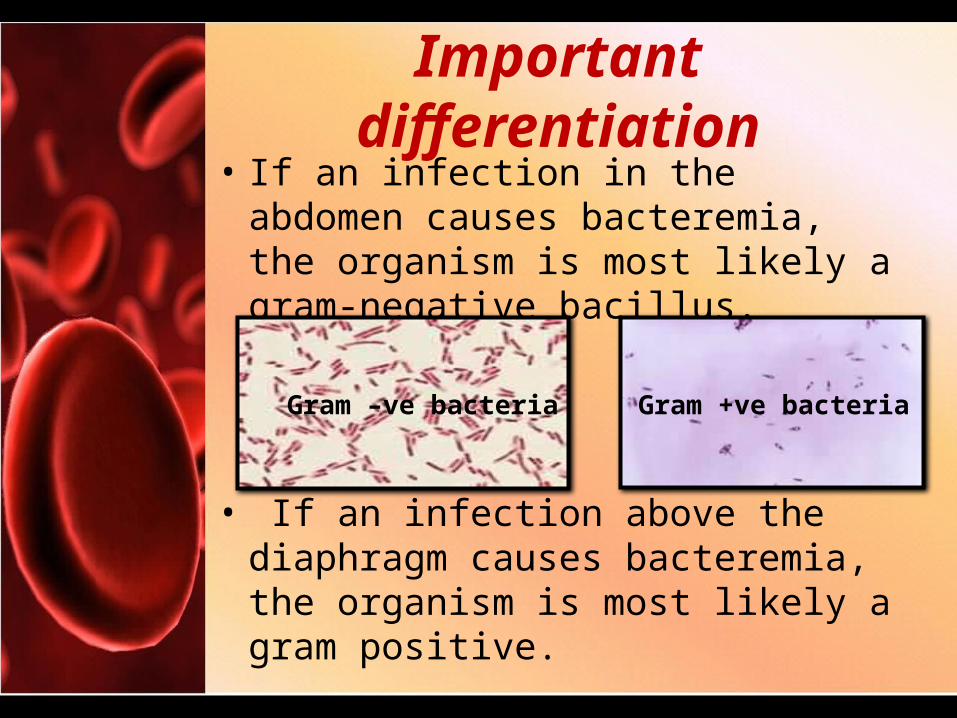
Important differentiation• If an infection in the abdomen causes bacteremia, the organism is most likely a gram-negative bacillus.
• If an infection above the diaphragm causes bacteremia, the organism is most likely a gram positive.
Gram –ve bacteria Gram +ve bacteria
Symptoms
• Asymptomatic patients• Mild fever• tachypnea, shaking chills, persistent fever, altered sensorium, hypotension, and GI symptoms (abdominal pain, nausea, vomiting, diarrhea) suggests septic shock.
• Septic shocks develop in 25-40% of patients with significant bacteremia.

Diagnosis and treatment
• Blood tests • Blood culture• PCR amplification of microbial genes followed by gel electrophoresis.
• Some of the different medications used in the treatment of Bacteremia include:
• Daptomycin • Cubicin• High risk people are given antibiotics before procedures that can cause bacteremia.
Sepsis: Blood poisoning
Excessive systemic inflammatory response to infection leading to life-threatning complications.
Elevated plasma concentration of cytokines
More common and dangerous in Elderly people Weakened immune system Infants under 3 months Chronic infections
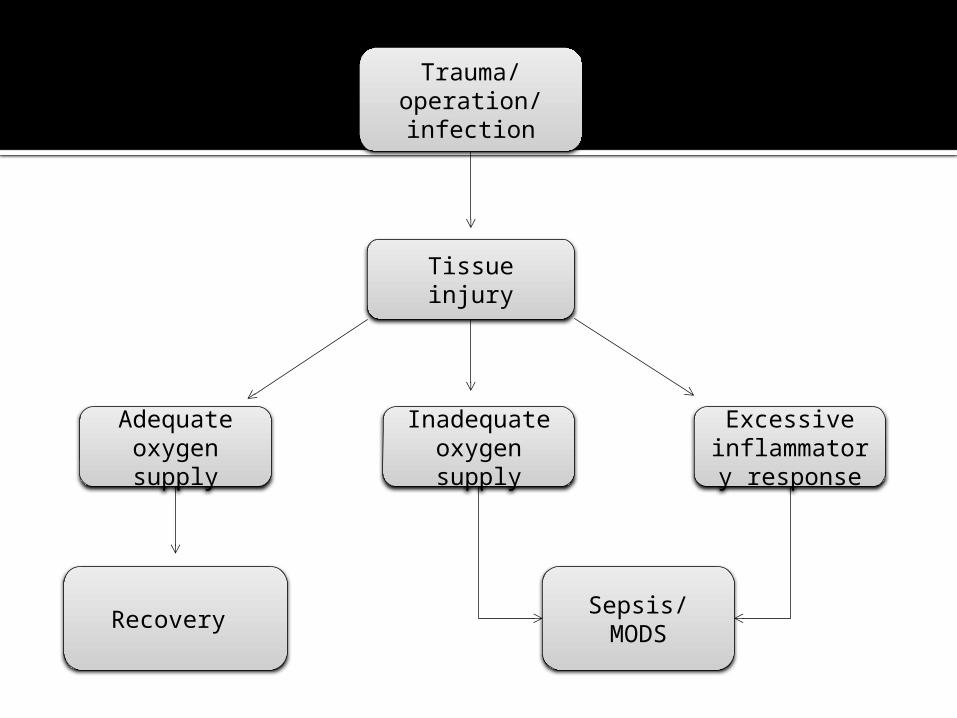
Trauma/ operation/ infection
Sepsis/ MODS
Excessive inflammatory
response
Inadequate oxygen supply
Tissue injury
Recovery
Adequate oxygen supply
Signs & symptoms
Fever Chills and severe shaking Increased heart rate Low blood pressure Rapid breathing Confusion, disorientation & dizziness Decreased urination Rash throughout the body Pain in joints
Diagnosis
Blood test: white blood cell count Evidence of infection Clotting problems Impaired oxygen availability
Blood culture before antibiotic treatment Other samples include
Sputum Urine Abscess contents
imaging tests include X-rays CT scan Ultrasound MRI
Cardiac monitor
Treatment
Hospitalization (ICU) Life saving measures
Medication: Antibiotics Vasopressors Others: costicosteroids, insulin
painkillers or sedatives Therapy Surgery
What is a UTI ?What is a UTI ?
An infection of urinary tract caused by germs, that
enter the urethra and then the bladder. This can lead to infection in the bladder itself, which can spread to
the kidneys
Type of urinary tract infected:Type of urinary tract infected:
• Cystitis Bladder• PyelonephritisKidney• Rarely the site of infectionUreter• UrethritisUrethra

E.Coli
80-85%Candida Staphylococcus
Saprophyticus
ChlamydiaCAUS
ESKlebsiella Species
Proteus Mirabilis Mycoplasma Enterococci
Who is at risk for a UTI?Who is at risk for a UTI?
People with spinal cord injuries• Difficulty emptying the bladder• Bacterial growth in the urine
Abnormality of the urinary tract
Diabetics
Patients using catheters
Types of UTITypes of UTI
• Upper urinary tract Infections:–Pyelonephritis
• Lower urinary tract infections–Cystitis (“traditional” UTI)–Urethritis (often sexually-
transmitted)–Prostatitis
Pathogenesis of UTIPathogenesis of UTI
Urethra colonised by bacteria
Bacteria enters bladder
Pathogens colonise bladder due to adherence properties
Pathogens attach to uroepithelial mucosa
Secretion of cytokines causing inflammation
PyelonephritisPyelonephritis
Pyelonephritis is a bacterial infection that most often occurs
when there is a persistent backflow of urine from the
bladder into the ureters or the kidney pelvis. It can be acute or
chronic
SymptomsSymptoms
• Flank Pain• Fever
Higher than 102 degrees Fahrenheit
Persists for more than 2 days
• Skin changes Flushed or
reddened Moist and Warm
• Severe abdominal pain Occurs
occasionally
• Urination Problems Blood in the urine Cloudy or
abnormal Urine color
Strong urine odor Nocturia Painful Urination Increased
Frequency
• Muscle Tenderness• Chills with shaking• Nausea and
Vomiting
DiagnosisDiagnosis
• Wide variation • exists in the clinical presentation, • severity, • options, and • disposition of the disease. • The triad of flank pain, fever, and nausea
and vomiting prompts examination and investigation.
Physical Examination
• Temp > 38.0ºC
• Tachycardia• Abdominal
Tenderness• Renal
Scarring• Odor• Appearance
Laboratory Tests
• Urinalysis • Pyuria• Bacteriuria• Haematuria• Urine Culture• Blood
Cultures - infection
• WBC Casts
Imaging Studies
• 99m-Tc-DMSA
• Ultrasound• shows
abnormalities in the kidney & bladder
• CT scan of abdomen
• MRI• Voiding
cystourethrogram• urethra & bladder
abnormalities• IVP
TREATMENTTREATMENT• The goals of treatment are to:
Control the infectionRelieve symptoms
• Symptoms go away within 48 to 72 hours • Antibiotics: are given after a urine culture
identifies the bacteria. A 10- to 14-day course of antibiotics.Mild infections: treated orally.
fluoroquinolones,Moderate - severe infections – parenteral aminoglycosides,
Interstitial cystitisInterstitial cystitis
• Inflammation of bladder• Age and Sex• Women : E.Coli• Men:S
Sign and SymptomsSign and Symptoms
• Decreased bladder capacity• Urinary urgency• Urinary frequency (60%)• Urinary discomfort• Pelvic pain• Low grade fever
• Bladder biopsy• Urinalysis• Urine culture• Urine cytology• Cystoscopy• Video urinodynamics• Imaging test• Potassium sensitivity test
DiagnosticsDiagnostics
UrinalysisUrinalysis
• Color• Clarity• Odor• Specific gravity• pH• Protein• Glucose• Ketones• Microscopic analysis
Urine culture testUrine culture test
• Detection and identification of bacteria and fungi
• Agar plate at room temp.• Size ,shape• Gram test• Escherichia coli gives pink color• Lactobacillus gives purplish color
CystoscopyCystoscopy
• Cystoscope• Examination of urethra and
bladder
UreteroscopyUreteroscopy
• Ureterscope• Laser beam• Examination of ureter
Cont…Cont…
• Local anesthetic• Saline• 15-30 mins• Avoid urination • Drink two 8-ounce glasses of
water each hour for 2 hours