Embed Size (px)
Citation preview

J. clin. Path. (1954), 7, 275.
THE APPEARANCE AND SIGNIFICANCE OF TISSUEMAST CELLS IN HUMAN BONE MARROW
BY
J. M. JOHNSTONE095 From the Department of Pathology, the University and Western Infirmary, Glasgow
(RECEIVED FOR PUBLICATION MARCH 4, 1954)
Despite an increasingly vast literature concerningthe examination of bone marrow, scant attentionhas been paid to the occurrence of tissue mast cellsin human marrow or to their significance whenpresent. Only recently have mast cells beendescribed in the marrow of a small number ofcases by Rohr (1949), Leitner (1948, 1949), Bremy(1950), Tischendorf and Hartmann (1950), Fadem(1951), Koszewski (1952), and Hayhoe (1953).Generally the patients had a severe marrow dis-turbance, which was frequently of the hypo- oraplastic variety, and, in the opinion of both Undritz(1946a and b) and Bremy (1950), the appearanceof mast cells in the marrow indicates severemarrow depression and is of diagnostic and prog-nostic significance. However, Williams (1952),using marrow biopsy particle smears, was able todemonstrate mast cells in as many as 56 (17 %)of 325 marrows.
Fixed tissue sections of routine marrow aspirateswere used in the present work, the object of whichwas to observe the frequency with which tissuemast cells occur in human marrow and to try toassess their significance.
Methods and MaterialsThe material for this investigation was taken from
consecutive marrow aspirates submitted routinely tothis laboratory for examination, the marrow samplesbeing aspirated by standard methods, in most instancesfrom the sternum. While sections of some of theearlier material were prepared according to the methoddescribed by Cappell, Hutchison, and Smith (1947),for the majority the modification detailed by Hutchi-son (1953) was used. The sections were stained with0.001% aqueous toluidine blue, and while no differencewas found to exist between the staining properties ofmast cells in sections prepared by either method, theadvantage of the latter lies in the fact that the blood,which always contaminates and dilutes aspirates, isremoved in the processing and consequently a frag-ment of pure marrow concentrate is obtained.
Tissue mast cells and basophil leucocytes (bloodmast cells) differ morphologically, having in commononly the metachromatic staining property of their
granules. As the granules of these latter cells havebeen found to be extremely soluble in water andalcohol they are not seen in fixed tissue sectionswhen an aqueous or alcoholic fixative has been used,and the basophil leucocytes therefore cannot beidentified.
Sections have been compared by enumerating themast cells in microscopic fields at a constant magnifi-cation (x 320), and the marrows placed in one orother of the following groups. Those marrows inwhich no mast cells were seen form Group 1:Group 2 contains marrows with an average of upto five mast cells per microscopic field, while inGroup 3 an average of more than five mast cells wasseen in each field. Only occasionally was it founddifficult to decide into which group a marrow shouldbe placed.
IncidenceApart from necropsy material, which wi!l be
mentioned later, 269 marrow aspirates from 230patients were examined. No mast cells were seenin 68 (30%) patients (Group 1). Group 2 con-tained the largest number with 139 (60%) cases,while the remaining 23 (10%) fell into Group 3.The pathological diagnoses of the patients in eachgroup are detailed in Table I.Twenty-seven patients had more than one
marrow aspiration. In 21 the marrows wereclassified under the same group each time, in onecase the proportion of mast cells remaining con-stant over 10 marrow examinations. In the re-maining six patients the number of mast cellsvaried only slightly.The advantage of sections over smears in the
demonstration of tissue mast cells was striking.No quantitative comparison was made, but examin-ing smears for their presence was time consum-ing and generally unrewarding. Even when shownto be abundant in the sections they were usuallyabsent or scanty in the smears.
MorphologyThe morphological characteristics of mast cells
seen in marrow have been described elsewhere
copyright. on A
ugust 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.7.4.275 on 1 N
ovember 1954. D
ownloaded from

J. M. JOHNSTONE
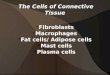
FIG. 1.-Details oftwo mast cells,one (b) showingan elongatedcytoplasmicprocess x 1,900(toluidine blue).
FIG. la
FIG. 1b
(Brerny, 1950; Fadem, 1951). While the majorityof the cells are rounded or ovoid (Fig. 1) bizarreforms are frequently seen. Some show pseudo-
podia-like extensions, many are elongated andspindle-shaped, while others have a blunted headcontaining the nucleus with the remainder of thecytoplasm drawn out into a long filamentous pro-cess, occasionally seen to be bifid. Cytoplasmicgranulations frequently overlaid the nucleus andoften completely obscured it. Mitotic division andbinucleated forms were not seen.
DistributionMast cells are known to occur throughout the
body and particularly in relation to the adventitiaof small blood vessels. This has certainly beenobserved in the marrow, but for the most part theyare by no means confined to this situation. Theyoccur somewhat irregularly ; in the reticular frame-work of the marrow, among the haemopoieticelements, and even stretched over the surface offat cells. The irregularity of distribution isoccasionally pronounced and a small area withabundant mast cells may be observed in a marrowwhich otherwise contains but few mast cells.
In sections of the whole thickness of boneobtained at necropsy-the mast cells are often seento be most numerous in and about the endosteumbut scanty towards the centre of the medullarycavity. This was also noted by Ellis (1949) at thenecropsy of a 12-month-old infant with urticariapigmentosa.
AgeVery few children were included in this material,
the majority of the patients being in the fifth toseventh decades, the ages ranging from 11 to 81years.
TABLE ITYPES OF CASES COMPRISING EACH GROUP
Type of Case
Pernicious anaemia 20Iron-deficiency anaemia 12Haemolytic anaemiaReticulosis 4Carcinoma 3ChrQnic infection 2Myelomatosis 3Leukaemia 8
Miscellaneous .. .. 16
Group I: No Mast Cells Group 2: Up to 5 Mast Cells per Field
Polycythaemia, myxoedema (2each); aregenerative anaemia,cerebro-vascular degeneration,red cell aplasia, osteoporosis,scurvy, anxiety state, nephritis,mitral stenosis, histoplasmosis,malabsorption syndrome, gastro-enteritis, myeloid metaplasia (1each)
Group 3: More than 5 MastCells per Field
38 643 536 110 252I I
I~-
31Vascular disease (4), cirrhosis, Bantisyndrome, B.T. malaria, nephritis,treated breast carcinoma (2 each);aplastic anaemia, essential thrombo-cytopenic purpura, normal, sprue,pneumonia, splenic neutropenia,sarcoidosis, ulcerative colitis, stea-torrhoea, peripheral neuritis, dis-seminated sclerosis, infectiousmononucleosis, haemachromatosis,rheumatoid arthritis, renal cyst,peptic ulcer, cardiac failure (1 each)
8Aregenerative anaemia, unexplainedcontinued pyrexia, uraemia, Bantisyndrome, aplastic anaemia, osteo-porosis, oesophageal stricture,cachexia (I each)
Total .. 68 139 23
276
copyright. on A
ugust 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.7.4.275 on 1 N
ovember 1954. D
ownloaded from

TISSUE MAST CELLS IN HUMAN BONE MARROW
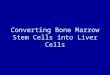
(a) (b)FIG. 2.-(a) Large numbers of tissue mast cells in a marrow of normal ervthropoiesis x 750 (toluidine blue). (b) Many tissue mast
cells in a hyperplastic marrow (pernicious anaemia) x 650 (toluidine blue).
Marrow was obtained at necropsy from varioussites from 31 infants and children dying from awide variety of pathological conditions. Mastcells were seen in only six cases and were alwaysscanty.
IronIron is stored in stainable form in the reticulo-
endothelial cells of the marrow in varying amountsdependent on the existing pathological conditions.Marrow sections from 185 of the aspirates hadbeen stained for iron (Hutchison, 1953), but nocorrelation could be found between the iron con-tent of the marrow and the number of mast cellsseen.
HaemopoiesisAt an early stage in this investigation it seemed
that the numbers of mast cells in the marrow mightdepend on a purely mechanical factor and be regu-
TABLE I1NUMBER OF CASES IN EACH GROUP COMPARED WITH
THE DEGREE OF HAEMOPOIESIS
Degree of HaemopoiesisGroup Moderate Marked
Hypocellular Normal Hyperplasia HyperplasiaOne .. 1 18 18 31Two .. 3 50 44 33Three. 26 8
lated simply by the degree of marrow cellularity,i.e., extreme marrow hyperplasia might crowd outmast cells from the marrow and hypoplasia allowtheir free multiplication. That this is not the caseis readily seen in Table II, where it is obvious thatthere is no association between the numbers ofmast cells and the extent of haemopoiesis (Fig. 2).
Lymph FolliclesIn sections from 21 (9%) of the cases lymphoid
follicles were observed in the marrow. Thesefollicles are minute foci or aggregates of smalllymphocytes with no germinal centre. Mast cellsappear constantly in the periphery of these fol-licles, but are never obserxed in the centre (Fig. 3).The number of mast cells varied considerably;occasionally they were scanty, generally plentiful,and sometimes abundant. While constantly pre-sent in these lymphoid follicles, transitional formsbetween mast cells and lymphocytes were notobserved, and the lymphocyte and plasma cellorigin of mast cells expounded by Downey (1913)cannot be refuted or confirmed.
DiscussionIt is our belief that tissue mast cells form a
normal constituent of human bone marrow. Bymaking use of fixed tissue sections, mast cells have
277
41 Aw.
tv
JO
copyright. on A
ugust 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.7.4.275 on 1 N
ovember 1954. D
ownloaded from

278I~~~~~.M. JOHNSTONE
been observed in as many as 70 % of the marrowsexamined. The pathological state of the patientsfrom which these marrows were aspirated repre-sent a wide variety of conditions, but some of themarrows themselves show no qualitative abnor-mality. Further, mast cells have been demonstratedin marrow obtained at necropsy from a few normalhealthy individuals who have died from injuriessustained in various forms of accidents.Mast cells were not observed in 30% of the
marrows, but it is probable that when scanty theirpresence or absence in any given marrow sectionmay well be governed by the selection inevitablein a small sample.
In a small proportion of the present cases thenumbers of observed mast cells must be consideredabnormally high in relation to the numbers seenin the great majority of the marrows. The causeof this increase is not immediately apparent al-though several suggestions have been put forward.Mast cell granules are generally believed to con-tain heparin (Jorpes' Holmgren, and Wilander,1937 ; Jorpes, 1946 ; Oliver, Bloom and Mangieri,1947; Kojksal, 1953), and Paff, Bloom, and Reilly(1947) thought that the inhibitory effect of heparinon growth (Goerner, 1931) explained the failureof all cells but mast cells to grow when tissue fromdog mastocytoma was cultured, but Macdougalland Riley (1954) attribute this simply to the greatpreponderance of mast cells present in the originaltissue. Fadem (1951) considered it possible thata similar relationship might *2xist between mast
4444'~~~44~~~~4~~4~~~ 4A
4OV.~ ~ ~ ~ 4 4~4 4
44~~ 4444 A
Vl~~~ ~ ~ ~ ~ ~ ~ ~ ~ 44
..4: 44
.444 444
4.
4 4
444
4'4:'
94* 4.,4
444
44$
4.
cell accumulation and hypoplasia of the marrowin some cases, the marrow growth being inhibitedby the excessive amount of heparin elaborated bythe increased numbers of mast cells in the marrow.However, if this be the case, the marrow depressionis but secondary to the increase of mast cells andthe explanation of this increase remains unsolved.
In the present series marrow hypoplasia was.observed in only two of the aspirates showing mastcell accumulation, erythropoiesis in the remainderbeing either normal or hyperplastic. Further, inaddition to the six cases of severe marrow depres-sion included in Table I, material from marrowdepressive states from eight necropsies and twobone marrow trephines was examined, mast cellaccumulation being observed. in only five of these16 cases. From this it is clear that hypoplasia ofthe marrow per se is neither a prerequisite formast cell accumulation nor an inevitable con-sequence of it, although the presence of mast cellsis frequently associated with some form of marrowdepression in the cases recorded in the literature(Bremy, 1950; Leitner, 1949 ; Rohr, 1949 ; Fadem,1951 ; Hayhoe, 1953).
Describing " myelitis chronica interstitialisRolbr (1948) suggested that in the early stages ofthe more serious form there is an irreversible pro-liferation of the marrow stromal fibrocytes andreticulum cells together with plasma cells and mastcells, sometimes leading to a resistant- secondarymarrow depression, and later to the final extremepicture of myelofibrosis. The marrow stromal
change was thought to be the local mani-festation of a systemic reaction, possiblyof an allergic nature, to some infection ornoxious agent. Certainly mast cells areknown to accumulate in other sites in re-lation to areas of chronic inflammation,and it is interesting to note that recentwork affords strong presumptive evidencethat the granules of mast cells containhistamine in addition to hep-arin (Rileyand West, 1952 ; -Riley, 1953). Thustheir association with anaphylactic-allergicstates would not be unexpected.
Brief details of all the present casesshowing mast cell accumulation are givenin the table in the appendix. While thistable contains a few cases of marrow
4 depressiv~e states similar to those describedAs- by Rohr- (1948, 1949) and Bremy (1950),
on the whole it affords little evidence to* support their view that the appearance of
4 *4..*
L%44 44.
#4
1V7'U4444
4 4*444 4
94 *
FIG. 3.-Lymphoid follicle in marrow with many tissuemast cells towards the periphery x 225 (tohiidineblue).
278
copyright. on A
ugust 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.7.4.275 on 1 N
ovember 1954. D
ownloaded from

TISSUE MAST CELLS IN HUMAN BONE MARROW
mast cells in the marrow is part of a reaction toan allergic process. There is little in the caseswhich might suggest any infective agent, either pastor present, and the majority of the marrows arehyperplastic with no increase in the amount ofstromal elements or plasma cells.Anaemia of moderate to severe degree is the
only factor common to all the cases although manydo also show some degree of splenomegaly. Butneither anaemia nor splenomegaly, alone or incombination, are essential for, or invariablyaccompanied by, mast cell proliferation.Adrenal cortical hypofunction or adrenalectomy
is said to result in marrow hypoplasia (Gordonand Charipper, 1947; Feldman, Rachmilewitz,Stein, and Stein, 1953), and the number of mastcells in the skin, muscle, and heart of intact ratswas observed by Cavallero and Braccini (1951) tobe markedly reduced following the injection ofcortisone, but the effect of adrenalectomy on thesecells is not known. It seems therefore theoreti-cally possible that adrenal cortical hypofunctionmay be at least partly responsible for the increaseof mast cells in the marrow of some cases exhibitingmarrow depression, but the response to A.C.T.H.and cortisone in such patients is as yet most dis-appointing (Wintrobe, 1951 ; Spaet, Rosenthal,and Dameshek, 1951 ; Davidson, Girdwood, andSwan, 1952; Medical Research Council Report,1953), and no change was observed in the numberof mast cells in the marrow of two cases receivingtreatment with A.C.T.H. (Williams, 1952).
Summary and ConclusionsTwo hundred and sixty-nine marrow aspirates
from 230 patients have been specifically examinedfor mast cells and they have been classified inthree grades according to the numbers present.The advantage of section over smears for this pur-pose is stressed.No mast cells were seen in 68 (30%) of the
patients, a few were present in 139 (60%), and in23 (10%) they were abundant.The presence and numbers of mast cells in the
marrow bore no relation to the iron content of themarrow or to the degree of erythropoiesis.Lymph follicles were seen in 21 (9 %) of the
marrows and mast cells were then constantlyobserved in their periphery; they were, however,
not confined to this situation. The morphologyand distribution of the mast cells have beendescribed.Mast cells are believed to form one of the
normal constituents of human bone marrow andthey have been observed to accumulate abnor-mally in a small proportion of cases. The causeof this increase is not clear and no single factorcan as yet be held responsible. While these casesshow a varying degree of anaemia associatedgenerally with a moderate to severe marrow dis-turbance, the earlier explanations offered and thegloomy prognosis previously associated with theappearance of mast cells in the marrow cannot besubstantiated.
I should like to thank the physicians and surgeonsin charge of wards at the Western Infirmary for theclinical details, Mr. M. Fitch, F.I.M.L.T., for tech-nical assistance, and Mr. G. Kerr for the photomicro-graphs.
REFERENCES
Bremy, P. (1950). Die Gewebsmas!zellen im menschlichen Knochen-mark. Thieme, Stuttgart.
Cappell, D. F., Hutchison, H. E., and Smith, G. H. (1947). Brit.med. J., 1, 403.
Cavallero, C., and Braccini, C. (1951). Proc. Soc. exp. Biol., N.Y.,78, 141.
Davidson, L. S. P., Girdwood, R. H., and Swan, H. T. (1952).Brit. med. J., 2, 1059.
Downey, H. (1913). Folia haemat., Lpz. (Arch.), 16, 49.Ellis, J. M. (1949). Archt. Path., Chicago, 48, 426.Fadem, R. S. (1951). Blood, 6, 614.Feldman, J. D., Rachmilewitz, M., Stein, O., and Stein, Y. (1953).
Ibid., 8, 342.Goerner, A. (1931). J. Lab. clin. Med., 16, 369.Gordon, A. S., and Charipper, H. A. (1947). Ann. N.Y. Acad. Sci.,
48, 615.Hayhoe, F. G. J. (1953). Brit. med. J., 1, 1143.Hutchison, H. E. (1953). Blood, 8, 236.Jorpes, E., Holmgren, H., and Wilander, 0. (1937). Z. mikr.-anat.
Forsch., 42, 279.Jorpes, J. F. (1946). Heparin in the Treatment of Thromnbosis, 2nd ed.
Oxford Medical Publications, London.Koksal, M. (1953). Nature, Lond., 172, 733.Koszewski, B. J. (1952). Blood, 7, 1182.Leitner, S. J. (1948). Acta med. scand., 130, 66.- (1949). Bone Marrow Biopsy. Churchill, London.Macdougall, J. D. B., and Riley, J. F. (1954). Proceedings of the
Scottish Society for Experimental Medicine, Glasgow, 6 February,1954.
Medical Research Council Haematology Panel's Second Report(1953). Brit. med. J., 2, 1400.
Oliver, J., Bloom, F., and Mangieri, C. (1947). J. exp. Med., 86, 107.Paff, G. H., Bloom, F., and Reilly, C. (1947). Ibid., 86, 117.Riley, J. F. (1953). J. Path. Bact., 65, 471.- and West, G. B. (1952). J. Physiol.,Lond., 117, 72P.Rohr, K. (1948). Sang, 19, 521.- (1949). Blood, 4, 130.Spaet, T. H., Rosenthal, M. C., and Dameshek, W. (1951), Bull.
New Engl. med. Cettt., 13, 252.Tischendorf, W., and Hartmann, F. (1950). Acta haemat., Basel,
4, 374.Undritz, E. (1946a). Schweiz. med. Wschr., 76, 88 and 115.-- (1946b). Ibid.. 76, 333.Williams, G. T. (1952). Amer. J. cdin. Path., 22, 1039.Wintrobe, M. M. (1951). Clinical Haematologv. 3rd ed. Kimpton,
London.
279
copyright. on A
ugust 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.7.4.275 on 1 N
ovember 1954. D
ownloaded from

J. M. JOHNSTONE
APPENDIXBRIEF DETAILS OF ALL CASES SHOWING MAST CELL PROLIFERATION
Case Age Sex Hb R.B.C.No_ g,. (MIcm )
2
34
5
6
7
8
910
11
1213
50
72486950
62
56
564666
53
5344
M
M
FFM
F
FFF
M
M
M
F
10-5 3 35
5-7 1608-3 1-953-0 0-994-0 1-05
9-7 3-12
6-0 I1-407-0 1-416-0 3-556 0 1-98
10-0 39c10
5 96 1
14 65 F )-0
15 56 F
16 50 M 9 7
17 52 F 8-0
18 46 F 5-619 62 M 4-520 81 M 9-0
21 26 F 5 322 64 F 10-3
23 62 F 10.5Marrow trephine material
24 71 M 5.7
Necropsy mwaerial25 44 M
26 67 F
27 56 M
1-031-72
2-4
3.3
4-?
3-22-93-0
3-1
4-35
5-1
1.9
Erythropoiesis Diagnosis Remarks
Hyperplasia + Bronchial carcinoma; Wassermann reaction positiveskeletal metastases;specific aortitis
+ + + Pernicious anaemia Megaloblastic marrow,, +++ , ,.
Severe hypoplasia Aplastic Death in 4,12 from first symptom: no causeidentified: few cells, other than lymphocytes,in marrow
Normal Atypical rheumatoid Mild pyrexia; joint pains; W.B.C. 8,000; labora-arthritis tory tests negative; responded eventually to
ButazolidinHyperplasia + + + Pernicious anaemia Megaloblastic marrow
,, +++ ., , . .+ + Iron-deficiency anaemia
Normal Carcinomatosis Carcinomatosis; hepatic secondaries proven alaparatomy?Bronchial primary. No necropsy
Cachexia 6/12 weakness and weight loss: E.S.R. 108121;hepatomegaly; achlorhydria; skeletonnormal; plasma proteins normal; G.I. tractnormal; pyrexia responded to antibiotics
Hyperplasia + + + Pernicious anaemia Megaloblastic marrow+ + +- Aregenerative anaemia W.B.C. 2,900'c.mm.; marrow-megakaryocvtes
+ +; scanty erythroid series; maturationfailure of both erythroid and myeloid series;no stromal or plasma cell increase. Requiredblood transfusions every 6152
+ + Oesophageal stricture Simple oesophageal ulceration. W.R. nee.Normal Osteoporosis Epileptic. Long-standing generalized osteo-
porosis with multiple fractures and collapse ofseveral lumbar vertebrae
Hynerplasia - Aleukaemic lymphatic Confirmed at necropsyleukaemia
. ++ Banti's syndrome Iron deficient; W.B.C. 2,600: splenomegaly;thymol turbidity 6 units; plasma proteinsnormal. Several hundred mast cells/field,, + Iron-deficiency anaemia|
Hypoplasia + Uraemia Hypertensive. Prostatic obstruction; blood tirea174 mg. °'. Plasma proteins normal
Hyperplasia --- -4- Iron-deficiency anaemia --
Normal P.U.O. Unexplained pvrexia for 4 months. Albumin3-1 ; globulin 3-4 g. 100 ml. serum. E.S.R.120 mm. in I houir. W.B.C. 11,0001c.mm.Normal differential. All other clinical andlaboratory findings normal
Normal Iron-deficiencv anaemia
Hyperplasia + +14 Reticulo-sarcoma Bone trephine suggested myelofibrosis with manyreticulum and connective tissue cells.Necropsy, reticulo-sarcoma with ex'ensivemarrow spread
Hyponlasia Myelofibrosis Aplastic anaemia requiring transfusions for 11years; hepatomegaly and splenomegaly; atnecropsy, mvelofibrosis and osteoscleros-s
Agranulocytosis Drug agranulocvtosis: W.B.C. 50,c.mm. Ulcer-ation of fauces and rectum: death trompulmonary embolism
Normal Aregenerative anaemia No details available
280
copyright. on A
ugust 30, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.7.4.275 on 1 N
ovember 1954. D
ownloaded from