Embed Size (px)
Citation preview

THYROID DISORDERS
& PARATHYROID DISORDERS
PHARMACOTHERAPY 2
•ONANONG WALEEKHACHONLOET
•THANANAN RATTANACHOTPHANIT


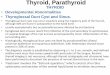
ต ำแหนง Thyroid gland & Parathyroid glands
Larynx
Trachea
Superior parathyroid gland
Inferior parathyroid gland

Thyroid hormone function
• Thyroid hormones are critical determinants of brain and somatic
development in infants and of metabolic activity in adults.
• Thyroid hormones also affect the function of virtually every organ
system.
•Major targets of thyroid hormone: skeleton, heart, and
metabolic regulation
• Thyroid hormones must be constantly available to perform these
functions, there are large stores of thyroid hormone in the thyroid
gland to maintain their availability.

Thyroid disorderI. ควำมผดปกตของกำรท ำงำนของตอม thyroid
- Thyrotoxicosis / Hyperthyroidism
- Hypothyroidism
II. ตอมธยรอยด thyroid ท ำงำนปกต แตมขนำดโตขน
- Diffuse euthyroid goiter
- Solitary thyroid nodule
- Multinodular goiter
III. ควำมผดปกตของ thyroid function test โดยทตอม thyroid
ท ำงำนปกต
- Euthyroid hyperthyroxinemia
- Euthyroid sick syndrome
- Euthyroid hypothyroxinemia
IV. ควำมผดปกตของตอมธยรอยดแบบ subclinical- Subclinical hypothyroidism- Subclinical hyperthyroidism

Thyroid gland
• Biggest endocrine gland
สงเคราะห “Thyroid hormone”
- Triiodothyronine (T3)
- Tetraiodothyronine (Thyroxine) (T4)
สงเคราะห “Calcitonin”
• Synthesis and Release is achieved by an intricate
negative feedback mechanism involving gland
and hypothalamic-pituitary axis
• Autoregulation depend on iodine: Wolff-Chaioff
effect
Wolff-Chaioff effect: A reduction in thyroid hormone levels/production caused
by ingestion of a large amount of iodine
• กลไกการปรบตวของตอมไธรอยดขณะทรางกายมระดบ iodine ในเลอดสงโดยเกดการ
ยบยงการสราง thyroid hormone ชวคราว

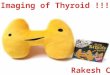
Iodine & Thyroid hormones synthesis
• iodine ในอาหารถกเปลยนเปน inorganic iodide และถกดดซมในล าไสเลก เพอน าไปใชในการสราง thyroid hormone
ผำน 3 ข นตอนใหญๆ คอ
1. Iodide transport
2. Oxidation ของ iodine
และ organic iodination
3. การสราง iodothyronine
TG= thyroglobulin, a large glycoprotein
synthesized in the thyroid cell

• Thyroxine (T4) and triiodothyronine (T3) are formed within thyroglobulin
• The unique tertiary structure of this glycoprotein (iodinated tyrosine residues
present in TG) are able to bind together to form active thyroid hormones

Thyroid hormones synthesis
คณสมบต Thyroid hormones: • "double" tyrosine with the critical incorporation of 3 or 4 iodine
atoms• lipid soluble

• T4 and T3 are transported in the bloodstream primarily by three proteins
: thyroxine-binding globulin (TBG), transthyretin (TTR), and albumin
(มากกวารอยละ 99 จบกบโปรตน)
• Circulating T3 : 80 % is derived from extrathyroidal conversion of T4 to
T3, 20% from direct thyroidal secretion
• Only the free thyroid hormone is able to diffuse into the cell and
some tissues, such as the brain, by active transport.

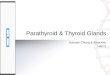
การควบคมการสราง thyroid hormone
Pathway I: ควบคมโดย TSH ซงหล ง
จำก anterior pituitary gland
• The secretion of TSH is itself under
negative feedback control by the
circulating level of free thyroid
hormone and positive influence of
hypothalamic thyrotropin-releasing
hormone (TRH).
Pathway II:
• Extrathyroidal deiodination of T4 to T3
is regulated by a variety of factors
including nutrition, nonthyroidal
hormones, ambient temperatures,
drugs, and illness.TRH= thyrotropin releasing hormone
TSH= thyroid stimulating hormone

Hypothalamus & Pituitary
•Thyroid hormone biosynthesis and secretion are maintained within narrow
limits by a regulatory mechanism that is very sensitive to small changes
in circulating hormone concentrations.
TRH= thyrotropin releasing hormone
TSH= thyroid stimulating hormone
Negative feedback
ถารางกายมระดบธยรอยด
ฮอรโมนในกระแสเลอดสงจะกด
การสรางและหลง TSH ท าให
ระดบ TSH ในกระแสเลอดต าลง
ตรงกนขาม
ถารางกายมระดบธยรอยด
ฮอรโมนในกระแสเลอดลดลงจะ
กระตนการสรางและหลง TSH ให
มระดบสงขน

THYROID FUNCTION TEST: Normal value
Current units SI units
Total T4 4.5-12.0 G/dl 58-155 nmol/L
Free T4 0.8-2.7 ng/dl 10.3-34.8 pmol/L
Free T3 0.2-0.5 ng/dl 3.5-7.7 pmol/L
Total T3 80-200 ng/dl 1.2-3.1 nmol/L
T4 index 1.2-3.6 1.2-3.6
TSH 0.35-6.20 U/ml 0.35-6.20 mU/L

Metabolism of thyroid hormones• Primary metabolism of thyroxine is deiodination.
• Deiodination of T4 may occur by monodeiodination of “outer ring”
producing 3,5,3’- triiodothyronine - T3 by 5’-monodeiodinase.
(T3 is 4 times more potent than T4)
• Deiodination of “inner ring” produce 3,3’,5’ – reverse
triiodothyronine – rT3 (inactive) by 5-monodeiodinase.
• In extrathyroidal tissue: T4 change to T3 by using 5-deiodinases in
liver.

Outer ring Inner ring
5’-monodeiodinase. 5-monodeiodinase.
Metabolism of thyroid hormones
•Beta blockers•High dose propylthiouracil•Steroid
•low T3 & high
of rT3

การสราง Thyroid Hormone
T4 (prohormone) T3 (active hormone)
Thiocyanate
Hypochlorite

17
Thyroid Hormone Synthesis and Secretion Inhibitors
• Blocks iodide transport into the thyroid :
– Bromine, Fluorine, Lithium
• Impairs organification and coupling of thyroid hormones:
– Thionamides, Sulfonylureas, Sulfonamide (?), Salicylamide (?),Antipyrine (?)
• Inhibits thyroid hormone secretion:
– Iodide (large doses), Lithium

MEDICATION &THYROID FUNCTION
Drugs affecting the secretion of TSH
• Dopamine: 1 microgram/kg/min
• Glucocorticoids: dexamethasone at least 0.5 mg/day
hydrocortione at least 100 mg/day
• Octreotide: 100 microgram/day
Drugs affecting the secretion of thyroid hormone
• Lithium: interfere synthesis and decrease secretion (occur in long term
treatment ~ 50%)
• Iodine containing medications: iodide, amiodarone, aminoglutethimide
Drugs affecting T4 absorption
• Colestipol, Cholestyramine, Aluminium hydroxide, Ferrous sulfate,
Sucralfate

MEDICATION AND THYROID FUNCTION
Drugs affecting transportation
• Increased TBG concentration: estrogen, tamoxifen, heroin, methadone,
mitotane, fluorouracil
• Decreased TBG concentration: androgen, anabolic steroids, slow release
nicotinic acid, glucocorticoids
• Displacement from protein-binding site: furosemide, fenclofenac,
mefenamic acid, salicylates
Drugs that alter T4 and T3 metabolism
• Increased hepatic metabolism: phenobarbital, rifampin, phenytoin,
carbamazepine
• Decreased 5-deiodinase activity: PTU, amiodarone, beta antagonist,
glucocorticoids
• Cytokines: interferon alfa, interleukin-2

Hyperthyroidism & Hypothyroidism

Thyroid evaluation
Symptoms of thyroid excess or deficiency
History of familial thyroid abnormality
Examination of thyroid for enlargement, consistency,
nodularity
Medication history
Thyroid function test (TSH, T3, T4)
ผปวยสวนใหญมกจะมาดวยภาวะ
• abnormal thyroid hormone levels
• diffuse or nodular thyroid enlargement
MNG=Multinodular goiter

Physical examination
• Weight
• Blood pressure
• Pulse rate & cardiac rhythm
• Thyroid palpation & auscultation
• Neuromuscular examination
• Eye examination
• Dermatologic examination
• Cardiovascular examination
• Lymphatic examination (nodes and spleen)

23
HyperthyroidismHypothyroidism

Physiological system
Hyperthyroidism(thyrotoxicosis)
Hypothyroidism
Skin --
appendages
warm, moist skin; sweating; fine,
thin hair; Plumber's nails;
pretibial dermopathy (Graves'
disease)
pale, cool, puffy skin; brittle hair
and nails
Eyes, face Upper lid retraction (wide stare);
periorbital edema;
exophthalmos, diplopia (Graves'
disease)
Eyelid drooping; periorbital
edema; puffy, nonpitting facies;
large tongue
Cardiovascular decreased peripheral resistance,
increased cardiac output, stroke
volume, heart rate, pulse
pressure; congestive heart
failure (high-output); increased
contractility,. arrhythmogenic;
angina
increased peripheral resistance,
decreased cardiac output, stroke
volume, heart rate, pulse
pressure; congestive heart
failure (low output); bradycardia
(low voltage ECG with prolonged
PR interval, flat T wave);
pericardial effusion

Physiological
systemHyperthyroidism
(thyrotoxicosis)
Hypothyroidism
Respiratory dyspnea; reduced vital capacity hypoventilation (CO2 retention)
pleural effusions
Gastrointestinal increased appetite; increased
bowel movement frequency;
hypoproteinemia
decreased appetite, decreased
bowel movement frequency;
ascites
CNS Nervousness, hyperkinesia,
variable emotional states
lethargy, neuropathy
Musculoskeletal Weakness; fatigue;
hypercalcemia, osteoporosis,
increased deep tendon reflex
muscle fatigue, reduced deep
tendon reflex, increased
alkaline phosphatase, LDH, AST

Physiological system
Hyperthyroidism (thyrotoxicosis)
Hypothyroidism
Renal Increased renal blood flow;
increased GFR; mild polyuria
Decreased renal blood flow;
decreased GFR; reduced water
excretion
Hematopoietic anemia (increased RBC
turnover); increased
erythropoiesis
anemia (decrease production
rate, decreased iron absorption,
decreased folate acid
absorption, autoimmune
pernicious anemia),decreased
erythropoiesis
Reproductive decreased fertility; menstrual
irregularity; enhanced gonadal
steroid metabolism
infertility;hypermenorrhea,
decreased libido; impotence,
decreased gonadal steroid
metabolism

Physiological system
Hyperthyroidism (thyrotoxicosis)
Hypothyroidism
Metabolic increased basal rate; negative
nitrogen balance,
hyperglycemia; increased free
fatty acids, decreased
cholesterol and triglycerides;
increased hormone
degradation; increased
requirement for fat-and water-
soluble vitamins; enhanced
drug detoxification
decreased basal rate; delayed
insulin degradation, with
increased sensitivity; enhanced
cholesterol and triglyceride
levels; decreased hormone
degradation; decreased
requirements for fat-and
water-soluble vitamins;
decreased drug detoxification.

Thyroid function test
• TSH: the most cost effective
screening test but it is not reliable in
secondary hypothyroidism
• FT4: patients recently treated for
thyroid disorder
• Nonspecific indice: cholesterol and
other lipid profile, SGOT, SGPT, CPK,
Cr
The most common
Lab used:
• TSH,
• total T4
• free T4
• total T3
• free T3
*** Drug or disease state can alter laboratory value

THYROID FUNCTION TEST: Normal value
Current units SI units
Total T4 4.5-12.0 G/dl 58-155 nmol/L
Free T4 0.8-2.7 ng/dl 10.3-34.8 pmol/L
Free T3 0.2-0.5 ng/dl 3.5-7.7 pmol/L
Total T3 80-200 ng/dl 1.2-3.1 nmol/L
T4 index 1.2-3.6 1.2-3.6
TSH 0.35-6.20 U/ml 0.35-6.20 mU/L

CASE 1: 55 yrs Thai female, TSH = 52 U/ml, Free T3 = 0.01 ng/dl
CASE 2: 36 yrs Thai female, TSH = 0.20 U/ml, Free T3 = 0.3 ng/dl

Thyroid binding globulin (TBG) level & Thyroid hormone level
• ความผดปกตของระดบ TBG ในเลอด หรอมปจจยรบกวนการจบกนของธย
รอยดฮอรโมนกบโปรตน จะสงผลใหการวดระดบธยรอยดฮอรโมนรวม (total
T3, total T4) ผดปกตได โดยทระดบ free T3, Free T4 ไมเปลยนแปลงตาม
– รางกายมระดบ IBPs ในเลอดสงขน จะท าให total T3 และ total T4 สง
กวาปกต แต free T3, T4 ปกต เรยกวา Euthyroid hyperthyroxinemia
– รางกายมระดบ IBPs ในเลอดต ำลง จะท าให total T3, total T4 ต ากวา
ปกตแต free T3, T4) ปกต เรยกวา Euthyroid hypothyroxinemia
• มความจ าเปนทตองทราบและประเมนรวมดวยวาผปวยมภาวะใดหรอไมทจะท า
ใหมความผดปกตของโปรตนทจบอยกบธยรอยดฮอรโมน
IBP= iodothyronine binding proteins

ภำวะทท ำใหระดบซร ม TBG ผดปกต
TBG เพมข น TBG ลดลง
ตงครรภ มการเจบปวย (major systemic illness)
ทารกหลงคลอด กลมอาการเนโฟรตค
มภาวะเอสโตรเจนมากเกน ภาวะทพโภชนาการ
ไดรบเอสโตรเจน active acromegaly
ไดรบยาคมก าเนด ไดรบฮอรโมนเพศชาย
ไดรบเฮโรอนไดรบยา tamoxifen ไดรบยากลโคคอรตคอยดในขนาดสง
ไดรบยา perphenazine ไดรบยา L-asparaginase
ตดเชอโรคเอดส พนธกรรม
Chronic active hepatitis
Biliary cirrhosis
Acute intermittent porphyria
พนธกรรม
TBG= thyroid binding globulin

Hyperthyroidism & Thyrotoxicosis
• Thyrotoxicosis (ภาวะธยรอยดฮอรโมนเปนพษ): ภาวะทรางกายม
อาการและอาการแสดงเนองจากเมตะบอลสมของรางกายทสงขน อน
เปนผลมาจากการทระดบธยรอยดฮอรโมนในกระแสเลอดสงกวาปกต
ระดบธยรอยดฮอรโมนทสงขนเกดไดจากหลายสาเหต โดยระดบฮอรโมน
ทสงอาจมการสรางจากอวยวะอนๆ เชน เนองอกของรงไข, ไดรบยาธยรอยด
ฮอรโมนขนาดมากเกนไป หรอ ภาวะธยรอดอกเสบ (Thyroiditis ) ซงมการปลอยธย
รอยดฮอรโมนมากผดปกต
• Tissues are exposed to excessive levels of T4, T3, or both.
• Hyperthyroidism (ภาวะฮยเปอรธยรอยดสซม): ภาวะทตอมธยรอยดท างานมากผดปกตเปนผลใหมการสรางและหลงธยรอยดฮอรโมน
มากกวาปกต
ระดบธยรอยดฮอรโมนในกระแสเลอดทสงขนจะเกดจากความผดปกตจาก
ตอมธยรอยดเอง

Thyorotoxicosis ทม
Hyperthyroidism
•Graves' disease
•Toxic multinodular goiter
•Toxic adenoma
•Hashimoto’s thyroiditis
(Hashitoxicosis )
•Jod-Basedow (Iodine induced)
•TSH- producing pituitary tumor
•Hydratidiform mole
Thyorotoxicosis ทไมม
Hyperthyroidism
•Subacute thyroiditis
•Transient painless thyroiditis
(Postpartum thyroiditis )
•Lymphocyte (silent) thyroiditis
•Thyrotoxic factitia
•Ectopic thyroid: Struma ovarii
Metastatic follicular carcinoma
•Drug associated thyroiditis
(amiodarone, lithium )
•Cytokine associated thyroiditis
(Interferon, Interleukin-2 )

HYPERTHYROIDISM
Most common causes:
• Graves’ disease: an autoimmune disorder in which thyrotropin
receptor antibodies (TRAbs) stimulate the TSH receptor,
increasing thyroid hormone production. (60-90%)
• Toxic multinodular goiters (TMNG, 10-20%)
• Toxic adenoma: autonomous hormone production can be
caused by somatic activating mutations of genes regulating
thyroid hormone synthesis (5-10%)
Epidemiology
• Women > Men (2% : 0.2%) (~ 10 times)
• Peak incidence in children: 10-12 year old

CASE FINDING FOR THYROID DYSFUNCTION
• Previous thyroid dysfunction
• Goiter
• Surgery or radiotherapy affecting the thyroid gland
• DM
• Vitiligo (depigmentation of parts of the skin)
• Pernicious anemia
• Premature gray hair
• Medications: lithium, amiodarone, radiocontrast, potassium
iodide
Goiter: a swelling of the neck or larynx resulting from enlargement of the
thyroid gland (thyromegaly), associated with a thyroid gland that is not
functioning properly.

Signs & Symptoms of Hyperthyroidism
• ผปวยบางรายอาจไมมอาการหรอ
อาการแสดงทเปนลกษณะจ าเพาะ
ของภาวะธยรอยดฮอรโมนเปนพษ
โดยเฉพาะในผปวยสงอาย
• บางรายอาจมอาการและอาการแสดง
ทางระบบใดระบบหนง
• บางรายมอาการตรงกนขามกบอาการ
และอาการแสดงทควรจะเปน
COMPLICATIONS
• Atrial fibrillation
• CHF
• Osteoporosis

Laboratory test: Hyperthyroidism• Hormone:
– Low TSH, Elevated free and total T3 and T4 serum concentrations,
particularly in more severe disease.
• 90%: T4 และ T3 สงขน
• 5-30%: T3 สง แต T4 ปกต (T3 toxicosis)
• พบนอยมาก: T4 สง แต T3 ปกต (T4 toxicosis)

• Radioactive iodine uptake (RAIU): การตรวจความสามารถใน
กระบวนการจบสารไอโอดนของตอมธยรอยด บงชสภำวะกำรท ำงำนของ
ตอมธยรอยด
–Normal 24-hour RAIU ranges from 10% to 30%
–Elevated RAIU by the thyroid gland when hormone is being overproduced;
–Suppressed RAIU in thyrotoxicosis due to thyroid inflammation (thyroiditis)
39
Laboratory test: Hyperthyroidism
• วธทดสอบ: ใหผปวยกน Radioactive iodine (ขนาดโดยทวไปประมาณ
5-20 uCi) แลววดปรมาณ Radioactivity ทตอมธยรอยดตามเวลาท
ก าหนดไวหลงกน Radioactive iodine และค านวณเปนคารอยละของ
จ านวน Radioactivity ทไดรบ
• ไมแนะน า ใหท าการตรวจ RAIU ในผปวยทมอาการชดเจนทกราย
• ขอหามส าหรบการตรวจ RAIU ไดแก ภาวะตงครรภ, ขณะใหนมบตร, และผทแพ
สารไอโอดน
• 131-ไอโอดน (I 131) half-life 8 days, 123-ไอโอดน I 123 half- life 13 hours

Differential diagnosis of thyrotoxicosis
hCG= human chorionic gonadotropin; RAIU = radioactive iodine uptake;
TSAb = thyroid-stimulating antibody; TSH = thyroid-stimulating hormone.
a = The RAIU may be decreased if the patient has been recently exposed to excess
iodine.

• Other tests:
– Thyroid-stimulating antibodies (TSAbs)
– Thyroglobulin (TG)
– Thyrotropin receptor antibodies
41
Laboratory test: Hyperthyroidism

HYPERTHYROIDISM (THYROTOXICOSIS)
Treatment goals :
Reverse sign & symptoms of hyperthyroidism, reduce goiter
size,
Normalize thyroid hormone levels,
Prevent thyroid storm,
Improve cardiac function and prevent systemic embolism
Preserve bone density and prevent osteoporosis
Improve overall functional capacity and quality of life

Graves’ disease
• พบไดบอยในชวงอาย 20-50 ป
• ลกษณะทางคลนก: hyperthyrodism, diffuse
goiter, ophthalmopathy, dermopathy “localized
myxedema”
• Autoimmune disease: สามารถตรวจ Autoantibody ตอ Ag หลายชนดท
Thyroid cells ไดแก TSH receptor (TSHR), thyroid peroxidase
(TPO), thyroglobulin (TG) และ thyroidal iodide transporter
• 80-100% ของผปวย ม Ab ชนด IgG ตอ TSHR (TSHRAb)
• TSHRAb ชนดทพบบอยและมปรมาณมากทสด ไดแก Thyroid
Stimulating Immunoglobulin (TSI) หรอ Thyroid Stimualting
Antibody (TSAb)

การรกษา Hyperthyroid ทเกดจากโรค Graves' disease
ม 3 วธ
1. การรกษาดวยสารรงส (Radioactive iodine: I131)
2. Subtotal thyroidectomy
3. Medical treatment
The American Association of Clinical Endocrinologists Guideline (AACE)
Factors need to be considered
• Cause of hyperthyroidism
• Severity
• Patient’s age
• Size of goiter
• Other complications
• Social and economic issues

Method Cost Efficacy Failure Adverse events
Surgery
Thyroidectomy
total or near
total
5,000-
20,000
70-80%
Graves’disease
Toxic adenoma
Toxic multinodular
goiter
20-30% Hypothyroid 20-30%
vocal abnormal 1:500
Hypoparathyroid
1:500
RAI 1,800-
3,000
70-80%
Graves’disease
Toxic multinodular
goiter
Toxic adenoma
no data Hypothyroid 3-6%
Teratogenicity
Medications ?? 30-40%
Graves’disease
60% 5-10% Hypothyroid
S/E, hypersensitivity

Surgery 131I Antithyroid drugs
Substantial comorbidity
- Cardiopulmonary diseases
- End stage cancer
Pregnancy (trimester 1 and 3)
• Pregnancy
• Lactation
• Thyroid cancer
• Unable to comply with
guideline
• Females planing a
pregnancy with in 4-6
mon
Major adverse
reactions
Contraindications of each treatment

https://www.aace.com/publications/guidelines
: update May 24, 2011

การรกษา Hyperthyroid ทเกดจากโรค Graves' disease
Advantages Disadvantages Comment
Rapid, effective
treatment,
especially in patients
with large goiters
•Most invasive
•Least costly in long
term after quality-
of-life adjustment
•Permanent
hypothyroidism
•Pain, scar
•Potential choice in
pregnancy if major side
effect from antithyroid
drugs
•Potential complications
(recurrent laryngeal
nerve damage,
hypoparathyroidism)
•Useful when coexisting
suspicious nodule
present
•Option for patients who
refuse radioiodine
Surgery

SURGERY
• Treatment of choice for extremely large nodule (>80g),
severe ophthalmopathy, not response to antithyroid
medications
• Complication: rate < 4 %
- Recurrent hyperthyroidism
- Hypothyroidism
- Hypoparathyroidism
- Vocal cord abnormalities

SURGERY
• Prepartion of surgery:
- PTU or MMI for 6-8 weeks until euthyroid (having normal thyroid
gland function)
- Iodide 500 mg/day for 10-14 days
- Propranolol for 10-14 days
• Relapse of hyperthyroidism occurs in at least 10%
• Permanent hypothyroidism occurs in 5% of patients within the
first year, and thereafter in one or two patients per year.

การรกษา Hyperthyroid ทเกดจากโรค Graves' disease
Advantages Disadvantages Comment
• Cure of
hyperthyroidism
• Lowest cost,
before adjustment
for quality of life
• Permanent hypothyroidism
almost inevitable
• Might worsen
ophthalmopathy
• Pregnancy must be
deferred for 6–12 months;
no breastfeeding
• Small potential risk of
exacerbation of
hyperthyroidism
• Best treatment for
toxic nodules and
toxic multinodular
goiter
Radioactive iodine (131I)

RADIOACTIVE IODINE (RAI)
• 131I colorless and tasteless liquid that is well absorbed and
concentrates in the thyroid
• Mechanism: 131I disrupt hormone synthesis
• Benefit for debilitated, cardiac, elderly, drug failure or toxic,
relapse after surgery
• Β-blockers are adjunct therapy prior to RAI. 1/+00
• If MMI is given, discontinue MMI 3-5 days before RAI, restart
3-7 days later and taper over 4-6 weeks.
• If hyperthyroidism persists after 6 month of RAIs, retreatment with RAI is suggested. 2/+00

FACTS ABOUT RADIOACTIVE IODINE
• Pregnancy is an absolute contraindication
– After receiving RAI for 4-6 months,
• patient should avoid pregnant.
• It needs 3-4 months in men to allow for turnover of
sperm production.
• Radiation thyroiditis can occur within the first two weeks after
RAI
• Hypothyroidism commonly occur following RAI
– Hypothyroidism after RAI for 6 months may be transient or
permanent
• RAI worsening ophthalmopathy
• Theoretical risk of genetic abnormality: 0.005%

Instructions for patients after RAI
• Do not share food or eating utensil for 5 days
• Avoid close contact with infants, young children (under 8 years),
pregnant women for 5 days
• No breast feeding is allowed for lactation: at least 6 weeks
• Flush the toilet twice after urinating and wash hand throughly
• If note increased nervousness, tremulousness, or palpitations,
call a physician

การรกษา Hyperthyroid ทเกดจากโรค Graves' disease
Advantages Disadvantages Comment
•Noninvasive
•Low initial cost
•Low risk of permanent
hypothyroidism
•Possible remissions due
to immune effects
•Low cure rate (30–
80%; average 40–
50%)
•Adverse drug
reactions
•Drug compliance
•First-line treatment in
children, adolescents,
and pregnancy
•Initial treatment in
severe cases or
preoperative
preparation
Methimazole (PTU only second-line therapy)
บญชยาหลกแหงชาต

carbimazole, a precursor of MMI, 10 mg of carbimazole is metabolized to approximately 6 mg of MMI
THIOUREA DRUGS (Thioamides)

• Mechanism : Methimazole (MMI), Propylthiouracil (PTU)
– inhibit the peroxidase enzyme system (peroxidation) and coupling process
– PTU can also inhibit peripheral conversion from T4 to T3
• Patient characteristics for good outcome : small goiter (<50g), short duration of
disease (< 6 month), no previous history of relapse with antithyroid drugs

Pharmacology Thiourea drugs (Thioamides)
Serum protein binding ~75% noneSerum half-life 75 นาท ~4-6 ชวโมง
Volume of distribution ~20 ลตร ~40 ลตร
Metabolism of drug illnessSevere liver disease ปกต ลดลง
Severe kidney disease ปกต ปกต
PTU MMI
tab 50 mg tab 5, 10, 20 mg
Transplacental passage นอย มากกวา
Levels in breast milk นอย มากกวา
Potency 1 10Inhibition of peripheral ม ไมม
conversion of T4 to T3

All adverse reactions 7.1% 3.3%
Major adverse reactionsAgranulocytosis 0.4% (idiosyncrasy) 0.1%(dose related)
Hepatotoxicity hepatocellular damage cholestasisVasculitis พบบอยกวา พบนอยกวา
PTU MMI

Adverse effectCross sensitivity: 50%
Most common
• Rash
• Itching
• Hives (urticaria)
• Abnormal hair loss
• Skin Pigmentation
• Transient leukopenia
(WBC < 4000/mm3)
Less common
• Swelling
•Nausea
•Vomiting
•Heartburn
•Loss of taste
•Joint or muscle aches
•Numbness and headache

Adverse effect
Rare case but severe (first 2 month of therapy)
• Agranulocytosis: PTU> MMI
• Aplastic anemia
• Lupus-like syndrome: occur after 6 months
• Polymyositis
• Hepatotoxic: occur within the first 3 months
• Hypoprothrombinemia
• Vasculitis
** If these complications occur, antithyroid drugs should
be discontinued (absolute contraindication)

Agranulocytosis: Thiourea drugs
One of serious adverse effects of thiourea drug therapy
An idiosyncratic reaction: mostly occur in the first 3 month
Common among patients over 40 year old
Rare among patients receiving < 30 mg of MMI/day
Symptoms: fever, rash, jaundice, arthralgia, oropharyngitis
Granulocyte count <250 per cubic millimeter
Patients can recover within 2-3 wks after the drug is stopped.
Warning: Agranulocytosis is an absolute contraindication
of antithyroid–drug therapy.

THIOUREA DRUGS
•MMI should be used in virtually every patient who chooses
antithyroid drug therapy for Grave disease,
– except during the first trimester of pregnancy when PTU is
preferred, in the treatment of thyroid storm.1/++0
•Patient should be alerted to stop the medications (PTU and MMI)
immediately and call their physician
• when there are symptoms suggestive of agranulocytosis or
hepatic injury. 1/+00
•Medication should be continued for approximately 12–18 months,
– then tapered or discontinued if the TSH is normal at that time.
1/+++

THIOUREA DRUGS
•If a patient with Grave’s disease becomes hyperthyroid after
completing a course of MMI,
• consideration should be given to treatment with RAI or
thyroidectomy.
• Low-dose MMI treatment for longer than 12–18 months may
be considered in patients not in remission who prefer this
approach. 2/+00
•When MMI is discontinued,
• thyroid function testing should continue to be monitored at 1–
3-month intervals for 6–12 months to diagnose relapse early.

Thiourea drugs
• Usual initial dose
– MMI 10-20 mg OD (single dose), Max dose 120 mg/day
– PTU 100 mg TID (300-600 mg/day), Max dose 1200 mg/day
• Improvement in symptom & lab test should be ensured within 4-8 wks
• Monthly dose titrations as needed (based on symptoms and free T4
concentrations); TSH may remain low months after starting therapy
• Maintenance dose for 12-18 month
– MMI : once euthyroid, may reduce to 5–10 mg/day
– PTU: once euthyroid, may reduce to 50 mg 2-3 times daily
Monitoring: baseline, 2 month, 6 month, course of therapy
• After remission: monitoring every 6-12 month

THIOUREA DRUGS IN PREGNANCY
• PTU should be used when antithyroid drug therapy
is started during the first trimester.
• MMI should be used when antithyroid drug therapy
is started after the first trimester. 1/+00
• Patients taking MMI who decide to become pregnant should be
switched to PTU as soon as possible in the first trimester and
changed back to MMI at the beginning of the second trimester.
2/+00
• GD during pregnancy should be treated with the lowest possible
dose of antithyroid drugs.1/+00

BETA BLOCKER
• CCBs: verapamil and diltizem oral can be used in patients with
contraindications with beta-adrenergic blockade
•Beta-adrenergic blockade should be given to elderly patients with
symptomatic thyrotoxicosis and to other thyrotoxic patients with
resting heart rates in excess of 90 bpm or coexistent cardiovascular
disease. 1/++0
•Beta-adrenergic blockade should be considered in all patients with
symptomatic thyrotoxicosis. 1/+00
•Contraindications of beta-adrenergic blockade: severe asthma,
CHF, cardiomyopathy
• used as adjunctive therapy with antithyroid drugs, RAI, or iodides when
treating Graves’ disease or toxic nodules; in preparation for surgery; or in
thyroid storm.
• used to ameliorate thyrotoxic symptoms such as palpitations, anxiety, tremor,
and heat intolerance,

BETA BLOCKER
From AACE guideline 2011

IODIDES
• Short term therapy before surgical, after radiotherapy, acutely thyroid
storm
– Often used as adjunctive therapy to surgery patient to shrink the
size of the gland.
– Do not use in the days before ablative surgery because it may
reduce uptake of radioactive iodine
• Mechanism: block releasing and inhibit synthesis of thyroid hormone.
• Limited efficacy after 7–14 days of therapy because thyroid hormone
release will resume.
• Symptom improvement occur 2-7 day after treated.
ADR : Hypersensitivity (rash, fever, rhinitis,cough)
Salivary gland swelling
Iodism (Metalic taste, burning mouth, stomach upset)
Gynecomastia

IDODIDES
• Lugol solution: 0.1-0.3 ml three time daily
(5% iodine +10% potassium iodide)
(6.3–8 mg of iodide per drop)
20 drop = 1 ml, 1 drop =0.05 ml
Potassium iodide: 60 mg three time daily
130-mg tablets contain 100 mg of iodide
Saturated solution of potassium iodide,
SSKI (38–50 mg of iodide per drop)
typical starting dose of SSKI is 3 to 10 drops daily (120
to 400 mg) in water or juice.

SUBCLINICAL HYPERTHYROIDISM
• Serum TSH below the lower limit of the reference range combined
with free T4 and T3 concentrations that are normal
• Potentially increase risk to develop cardiac and bone density
abnormality
• Few data are available to guide clinical decision regarding the
treatment of subclinical hyperthyroidism
• These patients could be treated with antithyroid agents, surgery,
radioactive iodine.

From AACE guideline 2011
Most practitioners agree that treatment of older patients (> 65 yrs)
with TSH values below 0.1 milli–international unit/L is reasonable.
SUBCLINICAL HYPERTHYROIDISM

THYROID STORM
Precipitating factor
- Surgical procedures
- RAI treatment
- Infection
- Noncompliance of thioamides
- Illness
- Accident
- Excessive iodine
- Excessive thyroid hormone
Signs and symptoms
- High Fever
- Tachycardia
- Agitation
- Weakness
- Dehydration
- Delirium
- Coma
- Nausea/vomiting
- Diarrhea
A life-threatening medical emergency

Diagnosis of thyroid storm
From AACE guideline 2011

Thyroid storm : Treatment1. Correction for hyperthyroidism: suppression of thyroid hormone,
formation and secretion
- Antithyroid drugs: PTU high dose (1200-1500 mg divide to 4-6
times/day)
- Lugol’s solution
- Dexamethasone (inhibit conversion T4 to T3)
- Antiadrenergic therapy
- Other methods: plasmapheresis to remove excess hormone (and to remove
thyroid-stimulating immunoglobulins in Graves’ disease) when the patient has not
responded to more conservative measures, although these measures do not always
work
Inhibition of thyroid hormone biosynthesis: PTU, MMI
Inhibition release of thyroid hormone from the
thyroid gland:
potassium iodide, lithium,
ipodate
Decreasing of the peripheral effects of thyroid
hormone:
PTU, corticosteroids,
ipodate, iopanic acid

Drugs used in thyroid storm
Drug Regimen
Propylthiouracil 900–1,200 mg/day orally in four or six divided doses
Methimazole 90–120 mg/day orally in four or six divided doses
Sodium iodide Up to 2 g/day IV in single or divided doses
Lugol’s solution 5–10 drops three times a day in water or juice
Saturated solution of
potassium iodide
1–2 drops three times a day in water or juice
Propranolol 40–80 mg every 6 hours
Dexamethasone 5–20 mg/day orally or IV in divided doses
Prednisone 25–100 mg/day orally in divided doses
Methylprednisolone 20–80 mg/day IV in divided doses
Hydrocortisone 100–400 mg/day IV in divided doses

• PTU in large doses may be the preferred thionamide because, in
addition to interfering with the production of thyroid hormones, it also
blocks the peripheral conversion of T4 to T3. However, β-blockers
and corticosteroids will serve the same purpose.
77
Drugs used in thyroid storm
• Iodides, which rapidly block the release of preformed thyroid
hormone, should be administered after thionamide is initiated to
inhibit iodide utilization by the overactive gland.
– If iodide is administered first, it could theoretically provide
substrate to produce even higher levels of thyroid hormone.
• Corticosteroids are generally recommended, although there is no
convincing evidence of adrenocortical insufficiency in thyroid storm,
and the benefits derived from steroids may be caused by their
antipyretic action and their effect of stabilizing blood pressure.

Thyroid storm : Treatment
2. Prevention and correction for complications
- Water and electrolyte imbalance: D5W
- Fever : paracetamol (do not use aspirin or other nonsteroidal
antiinflammatory agents because they may displace bound thyroid
hormone)
- CHF, arrhythmia
3. Correction for precipitating factors

Thyroiditis (Inflammatory Thyroid Disease)
• It should be suspected if patient have
pain and tenderness in the thyroid
region
• Hyperthyroidism from thyroiditis usually
is mild and lasted only a few weeks
• Treatment with antithyroid or RAI is not
work.
• Short term salicylate or glucocorticoid
may be needed to relieve thyroid pain
and tenderness
Thyroiditis: hyperthyroidism results from unregulated, inflammation-
induced release of stored thyroxine and triiodothyronine.

Treatment consideration for specific population
• Pregnancy: use PTU low dose ( 300 mg or less and
tapered to 50 to 150 mg daily after 4 to 6 weeks)
• Neonatal and pediatric: PTU 5 -10 mg/kg/day or MMI 0.5-1
mg/kg/day for 8-12 weeks, Iodides for few days

HYPOTHYROIDISM (ภาวะพรองธยรอยดฮอรโมน)
• Women > men (1.4% : 0.1%)
• Majority of patients have
primary hypothyroidism due to
thyroid gland failure due to
chronic autoimmune thyroiditis.
• Cretinism (Child)
• Myxedema (Adult)
• Hashimoto’s thyroiditis
Special populations with higher risk:
• Postpartum women,
• FH of autoimmune thyroid disorders,
• Patients with previous head and neck or
thyroid irradiation or surgery,
• Other autoimmune endocrine conditions
(e.g., Type 1 DM, adrenal insufficiency,
and ovarian failure),
• Some other non-endocrine autoimmune
disorders (e.g., Celiac disease, vitiligo,
pernicious anemia, sjögren’s syndrome,
and multiple sclerosis),
• Primary pulmonary hypertension,
• Down’s and turner’s syndrome

Causes of Hypothyroidism
Primary hypothyroidism
• Hashimoto’s disease
• Iatrogenic hypothyroidism
• Iodine deficiency
• Enzyme defects
• Thyroid hypoplasia
• Goitrogens
82
Caused by drug induce: amiodarone,
povidone iodine, iodinate contrast
media, lithium, nitroprusside
Secondary hypothyroidism
• Pituitary disease
• Hypothalamic disease
Goitrogens = substances that suppress the function of the thyroid gland
by interfering with iodine uptake, which can, as a result, cause an
enlargement of the thyroid

Causes of Hypothyroidism
1.1) Loss of functional thyroid tissue
• Postoperative and postradiation (I131 or external irradiation)
• Chronic autoimmune thyroiditis (Hashimoto’s thyroiditis)
• Reversible autoimmune hypothyroidism (Silent and postpartum
thyroiditis, cytokine thyroiditis)
• Idiopathic myxedema
1. Primary (Thyroidal hypothyroidism)
1.2) Functional defects in thyroid hormone biosynthesis and
releases
• Congenital defects in thyroid hormone biosynthesis
• Iodine deficiency
• Iodine – induced hypothyroidism
• Drug : antithyroid agents, lithium, natural and synthetic goitrogenic
chemicals

2.1) Loss of functional tissue
• Tumors ( pituitary adenoma, craniopharyngioma, meningioma, dysgerminoma, glioma, metastasis )
• Trauma ( Surgery, irradiation, head injury )
• Vascular ( ischemic necrosis, hemorrhage, stalk interruption, aneurysm of internal carotid a. )
• Infections ( abscess; tuberculosis, syphilis, toxoplasmosis )
• Infiltrative ( sarcoidosis, histiocytosis, hemochromocy tosis )
• Chronic lymphocytic hypophysitis
• Congenital ( pituitary hypoplasia, septo-optic dysplasia, basal encephalocele )
2. Central (hypothalamic/pituitary) hypothyroidism
2.2) Functional defects in TSH biosynthesis and release
• Isolate TSH deficiency, TSH synthesis defect, defect in TSH receptor
• Mutation in genes encoding for TRH receptor, TSH- or Pit-1
• Drugs : dopamine, glucocorticoids, L-thyroxine withdrawal
3. Peripheral (extrathyroid) hypo thyroidism
Thyroid hormone resistance

Sign & SymptomGeneral: Cold intolerance, weight gain,
decrease appetite and sweating,easily
fatigue
Head: Dry, brittle, sparse hair
Face: puffy face, large tongue
Neck: goiter in primary hypothyroidism
Cardiac: Cardiac enlargement, poor heart
sounds, dypsnea, low output failure
GI: Constipation
Genitourinary: Amenorrhea
Extremities: Broad hand and feet, cold
and dry skin, brittle nail, yellowish skin
Neuromuscular: Muscle pain and
weakness, paresthesia, delay deep tendon
reflexes
Emotional: Emotional instability,
depression, lethargy, decrease energy,
increase sleep requirement

Thyroid Function Test
• In 1๐ hypothyroidism, TSH level should be elevated.
• In 2๐ hypothyroidism, TSH levels may be within or below the reference range;
when TSH bioactivity is altered, the levels reported by immunoassay may
even be elevated.
• Free and/or total T4 and T3 serum concentrations should be low.
86

TREATMENT: HYPOTHYROIDISM
TREATMENT GOALS :
• Reverse physical finding , and normalize thyroid hormone level
• Reduce goiter size
• Reduce serum cholesterol level
• Improve quality of life
• In neonate and children : maintain normal growth, physical and
mental development
• There is general agreement that patients with primary hypothyroidism
with TSH levels above 10 mIU/L should be treated, which patients with
TSH levels of 4.5-10 mIU/L will benefit is less certain.

Complications:
• CNS: depression, dementia, psychosis, convulsion
• Neuromuscular: Malaise, increasing of creatine
phosphokinase (CPK)
• CVS: increasing risk of coronary heart disease

TREATMENT
Drug of Choice : Sodium levothyroxine (L-thyroxine)
• Daily dosage of L-thyroxine is dependent on age, sex, body size (need
Ideal body weight for daily requirement)
• Initial dose:
• Existing cardiovascular disease 12.5-25 microgram/day
• Adult: 75-200 microgram/day or 1.7 microgram/kg/day
• Children: 4 microgram/kg/day
• Elderly: < 1microgram/kg/day
• Dose titration based on response (control of symptoms, normalization of
TSH and free T4), Can increase or decrease in 12.5- to 25-mcg/day
increments
Adverse effect: hyperthyroidism, osteoporosis, drug allergy, adrenal
crisis.

Monitoring
Plasma TSH concentrations begin to fall within hours and are
usually normalized within 2 weeks,
but they may take up to 6 weeks for some patients, depending
on the baseline value.
TSH concentration is the most sensitive and specific monitoring
parameter for adjustment of L-thyroxine dose. 90
Therapeutic Monitoring
• Patients should be evaluated q 6-8 weeks initially.
• TSH and T4 concentration should be checked monthly until
euthyroid state is achieved.
• Once TSH is normal: visit q 6-12 months is sufficient, TSH should
be measured at least annually.

Drug/Dosage Form Content Relative Dose Comments/Equivalency
Levothyroxine
Synthroid, Levothroid, Levoxyl,
Thyro-Tabs, Unithroid, and other
generics 25, 50, 75, 88, 100, 112,
125, 137, 150, 175, 200, 300 mcg
tablets; 200 and 500 mcg per vial
injection
Synthetic
T4
100 mcg Stable; predictable potency; generics
may be bioequivalent; when switching
from natural thyroid to L-thyroxine,
lower dose by one half grain; variable
absorption between products; half-life
= 7 days, so daily dosing; considered
to be drug of choice
Thyroid USP
Armour Thyroid, Nature-Throid, and
Westhroid (T4:T3 ratio approximately
4.2:1);
Armour, one grain = 60 mg; Nature-
Throid and
Westhroid, one grain = 65 mg. Doses
include 1/4, 1/2, 1, 2, 3, 4, and 5 grain
tablets
Desiccate
d
pork
thyroid
gland
1 grain
(equivalent
to 74 mcg
[˜60–100]
mcg of T4)
High T3:T4 ratio; inexpensive
Liothyronine
Cytomel 5, 25, and 50 mcg tablets
Synthetic
T3
33 mcg
(˜equivalent
to 100 mcg
T4)
Uniform absorption, rapid onset; half-
life = 1.5 days, rapid
peak and troughs
Liotrix
Thyrolar 1/4-, 1/2-, 1-, 2-, and 3-
strength tablets
Synthetic
T4:T3 in
4:1 ratio
Thyrolar 1
= 50 mcg
T4 and 12.5
mcg T3
Stable; predictable; expensive; lacks
therapeutic rationale
because T4 is converted to T3
peripherally. 91

92
Dosage adjustments: L-thyroxine
• Bioequivalent
–If dosage, type, or brand of thyroid preparation changed, TSH
concentration should be measured after 8-12 weeks.
• Decreases in L-thyroxine requirements occur as patients age and following
significant weight loss.
• Patients older than 50-60 years,
– without evidence of coronary heart disease (CHD) may be started on
doses of 50 μg daily.
– with known CHD, usual starting dose is reduced to 12.5-25 μg/day.
• In pregnancy thyroid hormone requirements are increased, then revert
back to baseline after delivery
• Sodium levothyroxine has narrow therapeutic range
• Excessive dose of thyroid hormone may lead to CHF, angina pectorisand MI

ขอมลยา L-thyroxine
• Drug interactions:
- Decrease absorption: cholestyramine, ferrous sulfate, calcium,
antacid, sucralfate, lovastatin
- Protein binding: anticonvulsants
- Increase metabolism: rifampin, phenytoin, carbamazepine,
phenobarbital
L-thyroxine is better absorbed before a meal, instructing patients to
consistently take it with water between 30 and 60 minutes prior to
eating breakfast or at bedtime 4 hours after last meal;
• L-thyroxine should be protected from light and moisture.

Effects of hypothyroidism on some drugs
• Digitalis (increased sensitivity to the digitalis effect)
• Insulin (Insulin degradation may be delayed)
• Warfarin (delays the catabolism of clotting factors)
• Barbiturate, Phenothiazines, Opioid analgesics (increased
sensitivity may increase carbon dioxide retention and precipitate
myxedema coma)
•Metabolism of drugs can be altered for patients with hypothyroidism.

Drug induced thyroid disorders
Drug Mechanism Results
Nitroprusside inhibit hormone effect hypothyroidism
Lithium inhibit hormone release hypothyroidism
Iodides Wolff-Chaikoff effect hypothyroidism or
or iodine-containg hyperthyroidism
Sertraline increase T4 elimination hypothyroidism
Sulfonylureas, inhibit organic bindiing hypothyroidism
sulfonamides
Immunotherapy Autoimmune process hypothyroidism or
hyperthyroidism

Effect of Thyroid Status on Drug Action
Drug Hyperthyroidism Hypothyroidism
Sympathomimetics increase response Blunted response
Digoxin increase Vd, clearance increase sensitivity
Insulin increase metabolism, Prolong effect
increase clearance
Coumadin decrease need of drugs increase need of drugs
Beta-blocker increase clearance not significant
Theophylline not significant decrease clearance
Cortisol decrease half life increase half life

SUBCLINICAL HYPOTHYROIDISM
• Normal free T4 but elevated TSH
• Therapy is recommended if thyroid autoantibodies are
positive: levothyroxine
• If not treated, the patient should be evaluated at yearly
intervals

MYXEDEMA COMA
Precipitating factors:
• Infections
• Transquilizer, nacrotic analgesic
• Some medications: amiodarone, lithium carbonates, sedatives,
narcotics, anesthesia
• Cold weather
• Other conditions eg. Paralysis, CHF
• An uncommon but life-threatening form of untreated hypothyroidism
with physiological decompensation.
• S&S: hypothermia, advanced stages of hypothyroid symptoms, and
altered sensorium (delirium to coma)

Treatment
99
IV thyroid hormone replacement
T4: 100- to 500-mcg loading dose, followed by 75–100 mcg/day,
until patient can tolerate oral therapy.
Lower the initial dose in frailer patients or in patients with
established cardiovascular disease.
Some advocate the use of T3 over T4, given that T3 is more
biologically active and that T4/T3 conversion may be suppressed in
myxedema coma. Cost and availability limit intravenous T3 use.
Antibiotic therapy: Given common infectious causes, some advocate
empiric therapy with broad-spectrum antibiotics.
Corticosteroid therapy
Hydrocortisone 100 mg q 8 hours (or equivalent steroid)
Can be discontinued if random cortisol concentration not
depressed

Euthyroid goiter
• Goiter without other symptoms and having normal laboratory
value of thyroid hormone, TSH
• Causes:
- Starvation: iodine
- Goitrogenic food, drugs
- Congenital abnormality of thyroid gland
• Treatment:
• Iodine supplement, thyroid hormone
“Goitrogen" is a term used to describe any substance that can cause
enlargement of the thyroid gland


Parathyroid Disorders
• Role of parathyroid glands: control
calcium within the blood
• Four parathyroid glands make more or
less parathyroid hormone (PTH) in
response to the level of calcium in the
blood.
• Increased PTH
• causes body to put more calcium into the blood
• causes the bones to release their calcium into the blood.

Calcium is the most important element for the nervous system,
muscular system, and skeletal system.

Parathyroid• When the calcium in our blood goes too low, the parathyroid
glands make more PTH.

Homeostatic mechanisms to maintain serum calcium concentrations.

Pathology: parathyroid gland
• Hypoparathyroidism
• Pseudohypoparathyroidism
• 1o hyperparathyroidism
• 2o hyperparathyroidism
• 3o hyperparathyroidism

Hypoparathyroidism
• Rare disease
• Most common cause is thyroid gland surgical complication
• other causes are RAI, idiopathic
Signs and Symptoms: Hypocalcemia
- Seizures
- Mental changes: emotional instability
- Parkinson-like movement disorder
- Cardiac conduction abnormalities
- Neuromuscular irritability
- Dry hair, brittle nails, dry & scaly skin
- Calcification: cataract

Diagnosis:
Hypoparathyroidism:
• Hypocalcemia
• Hyperphosphatemia
• Chronic tetany
• Normal alkaline phosphatase
• No CKD, diarrhea
• Increase phosphorous in
urine after PTH is given
Pseudohypoparathyroidism:
• Hypocalcemia
• Hyperphosphatemia
• High level of serum PTH
• Hypoparathyroidism which is
not response to exogenous
PTH

Hypocalcemia

Treatment
• Calcium and vitamin D supplement
Type calcium (mg) Amount (mg) Elemental
Calcium lactate 300 39
Calcium gluconate 500 44.6
Calcium carbonate 250 100
• Initial therapy 1 to 3 g/day of elemental calcium.
• Average maintenance doses range from 2 to 8 g of elemental
calcium per day in divided doses.
• Asymptomatic and chronic hypocalcemia associated with
hypoparathyroidism and vitamin D–deficient states can be managed
by oral calcium and vitamin D supplementation

Hyperparathyroidism• Incidence: In US 100,000 person/year
Female: male =2:1
•Most common age group: 50-70 yrs
• The most common cause is the development of a benign tumor (Familial
endocrine neoplasia type I)
• 95% of patients have one enlarged, overactive gland (single adenoma)
• 1o hyperparathyroidism
– adenoma, hyperplasia, carcinoma – high serum calcium
• 2o hyperparathyroidism
– high PTH from negative feedback mech. in CKD
• 3o hyperparathyroidism
– autonomous parathyroid hyperfunction in secondary
hyperparathyroidism

Sign & Symptoms“MOANS, GROANS, STONES, AND BONES”
• "Psychiatric moans“: effects on CNS including lethargy, fatigue,
depression, memory loss, psychosis, ataxia, delirium, and coma.
• "Abdominal groans“: constipation, indigestion, nausea and vomiting,
GERD (high calcium increase acid production), Pancreatitis
• "Stones" : kidney stones, hypercalciuria, nephrocalcinosis, diabetes
insipidus (polyuria and polydipsia). These can ultimately lead to renal
failure Kidney stone, kidney failure
• "Bones“: Osteoporosis
High BP (75% of patients)
Cardiac symptoms: palpitation, arrhythmia, heart value problem
Headache: recurrent headache
Stroke

Laboratory tests
• Hypercalcemia (>10.5 mg/d)
• Hypophosphatemia
• Hyperchloremia (>102 mEq/L)
• High level of parathyroid
hormone
• Low level of bicarbonate
• High level of cyclic AMP in urine
• X-ray, ultrasound, CT scan
Treatment:
Parathyroidectomy: symptomatic 1๐
hyperparathyroidism
Volume expansion
Furosemide
Pamidronate
Ibandronate
Zoledronate
Calcitonin
Glucocorticoids
Dialysis

Hypercalcemic crisis & acute symptomatic severe hypercalcemia
should be considered medical emergencies and treated immediately

Hypercalcemia: Emergency case
• Hydration: NSS 3-4 L
• Increase excretion: Furosemide IV
• Decrease bone resorption: osteoclast inhibitor:
- Calcitonin 4-8 unit/kg SC q 6-12 hr
- Etidronate 7.5 mg/kg IV
- Plicamycin (cause: cancer): 15-25 mg/kg
• Hydrocortisone 200-300 mg/day
• Dialysis

Drug interactions
• PTU - warfarin, digoxin, theophylline
• MMI - warfarin, digoxin, theophylline
• Levothyroxine – Warfarin, Digoxin
PTU – Warfarin (Moderate): may increase the hypoprothrombinemic response to oral
anticoagulants
PTU- Digoxin (Moderate): clearance of digitalis glycosides may be reduced when a
euthyroid state is achieved after the addition of antithyroid agents.
PTU- Theophylline (Moderate): Clearance of theophylline and related agents
depends upon thyroid function. In the hyperthyroid state, clearance may be
enhanced. In the hypothyroid state, clearance may be reduced.
Levothyroxine – Warfarin (Moderate): Since thyroid hormones may increase the
catabolism of vitamin K-dependent clotting factors, the hypoprothrombinemic
response to oral anticoagulants may be enhanced during the initiation of thyroid
hormone therapy.
Levothyroxine- Digoxin (Moderate): clearance of or sensitivity to digitalis glycosides
may be increased in previously hypothyroid patients when a euthyroid state is
achieved after the addition of thyroid hormones.

Amiodarone and thyroid dysfunction
• Both hypo- and hyperthyroidism are complications of amiodarone therapy
• Meta-analysis of 4 RCTs (n=1465 euthyroid patients):
– prevalence of clinical thyroid disease was higher in patients receiving
amiodarone therapy (150 to 330mg/day for a minimum of one year)
when compared with placebo (3.7% VS 0.4%, respectively) .
• In other reviews and reports,
– Risk of amiodarone-induced thyroid dysfunction ranges from 2 to 30%
depending upon an individual's underlying thyroid status, dietary iodine
intake, and whether cases of subclinical thyroid disorders (eg, slight rise
in thyroid-stimulating hormone [TSH] without symptoms) are included.

Amiodarone and thyroid dysfunction
• Amiodarone contains two iodine atoms.
• Amiodarone metabolism in the liver releases ~ 3 mg of inorganic
iodine into the systemic circulation per 100 mg of amiodarone
ingested.
– Average iodine content in a typical American diet is about 0.3 mg/day.
– Thus, 6 mg of iodine associated with a 200 mg dose of amiodarone
markedly increases the daily iodine load.
• Effects of amiodarone on thyroid function can be divided into
• Effects that are intrinsic properties of the drug
• Effects that are due to iodine

Effects that are intrinsic properties of the drug
• Amiodarone
– inhibits outer ring 5'-monodeiodination of thyroxine (T4),
• thus decreasing triiodothyronine (T3) production; reverse T3
accumulates since it is not metabolized to T2.
• Amiodarone, and particularly the metabolite desethylamiodarone,
– blocks T3-receptor binding to nuclear receptors and decreases
expression of some thyroid hormone-related genes.
• Amiodarone
– may have a direct toxic effect on thyroid follicular cells, which results in
a destructive thyroiditis
Effects due to iodine
• Iodine is a substrate for thyroid hormone synthesis.
• Iodine is actively transported into thyroid follicular cells and organified
onto tyrosyl residues in thyroglobulin.

Management
• Amiodarone-induced hypothyroidism: is essentially the same as for
any patient with hypothyroidism, although higher doses of thyroxine
may be required to normalize the serum TSH level.
• Amiodarone-induced hyperthyroidism (AIT):
–Type I AIT : hyperthyroidism with increased synthesis of thyroid
hormone induced by amiodarone
• Thionamides
–Type II AIT: destructive thyroiditis with loss of TG (thyroglobulin)
and thyroid hormones
• Glucocorticoids