Embed Size (px)
Citation preview
Update on spinocerebellar ataxias (SCAs)
Thomas Klockgether
EuroAtaxia Conference 2018 Frankfurt, 09.11.2018
• The spinocerebellar ataxias (SCAs) are a group of more than 40 autosomal dominantly inherited progressive ataxia disorders.
• SCAs are rare diseases with an estimated prevalence of 5 : 100,000.
• The clinical hallmark of SCAs is progressive loss of balance and coordination accompanied by slurred speech with an onset in adult life.
• People affected by SCAs suffer substantial restrictions of mobility and communicative skills resulting in impaired quality of life.
• Many SCAs lead to premature death.
Spinocerebellar ataxias (SCA)
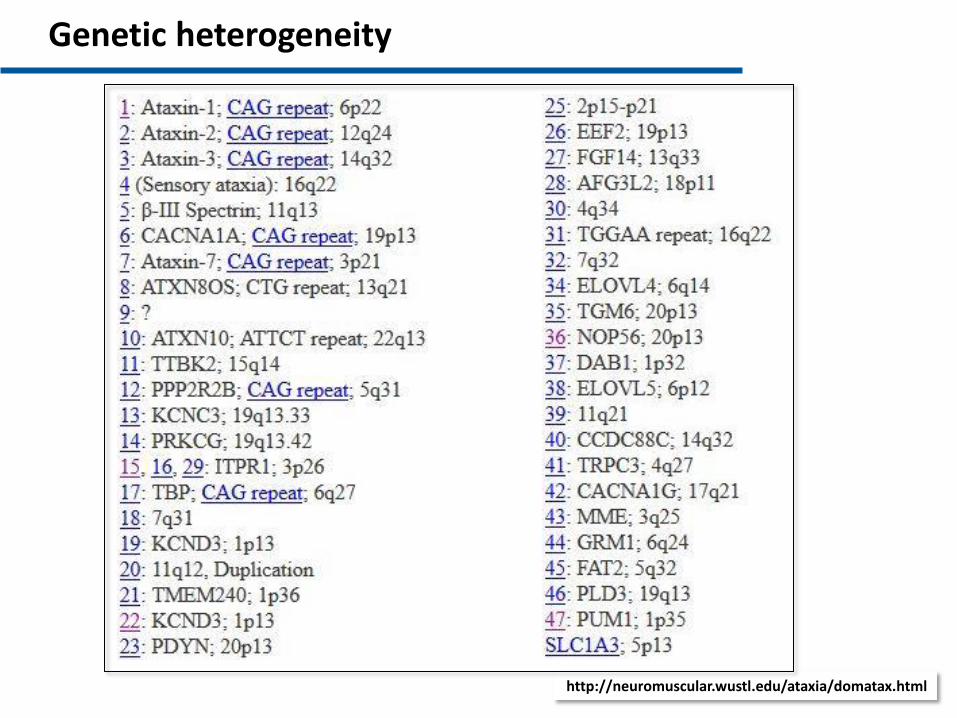
Genetic heterogeneity
http://neuromuscular.wustl.edu/ataxia/domatax.html
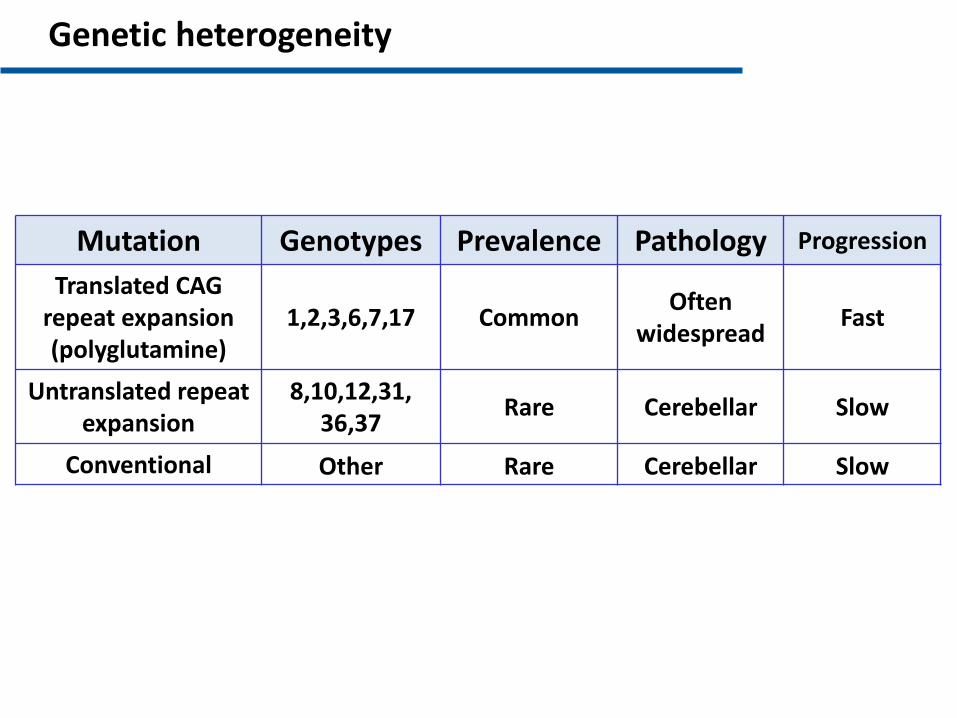
Genetic heterogeneity
Mutation Genotypes Prevalence Pathology Progression
Translated CAG repeat expansion (polyglutamine)
1,2,3,6,7,17 Common Often
widespread Fast
Untranslated repeat expansion
8,10,12,31, 36,37
Rare Cerebellar Slow
Conventional Other Rare Cerebellar Slow
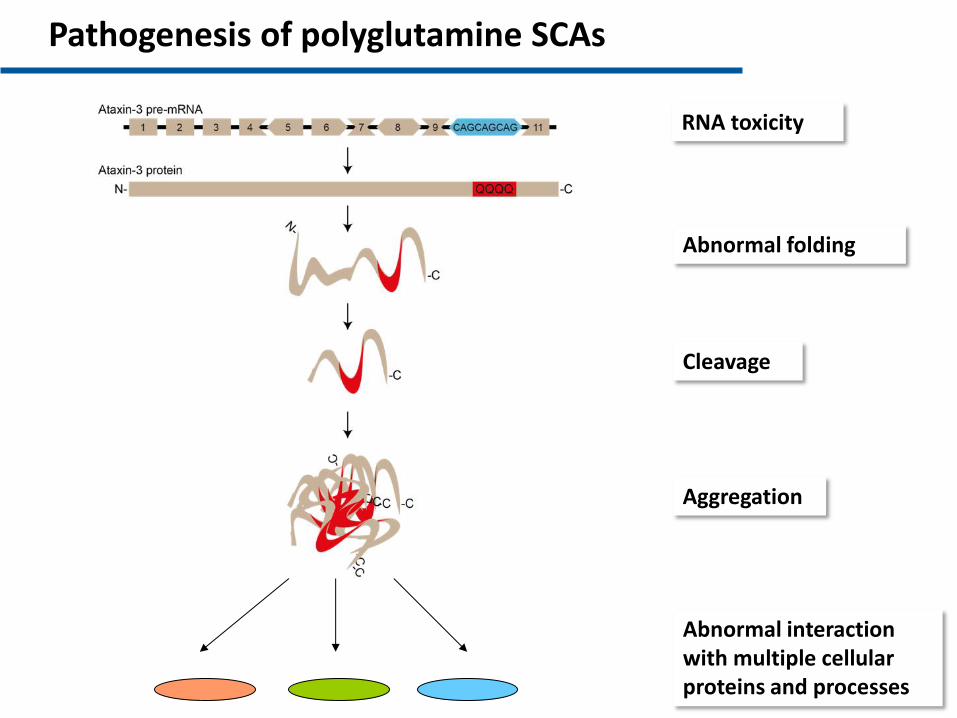
RNA toxicity
Abnormal folding
Cleavage
Aggregation
Pathogenesis of polyglutamine SCAs
Abnormal interaction with multiple cellular proteins and processes
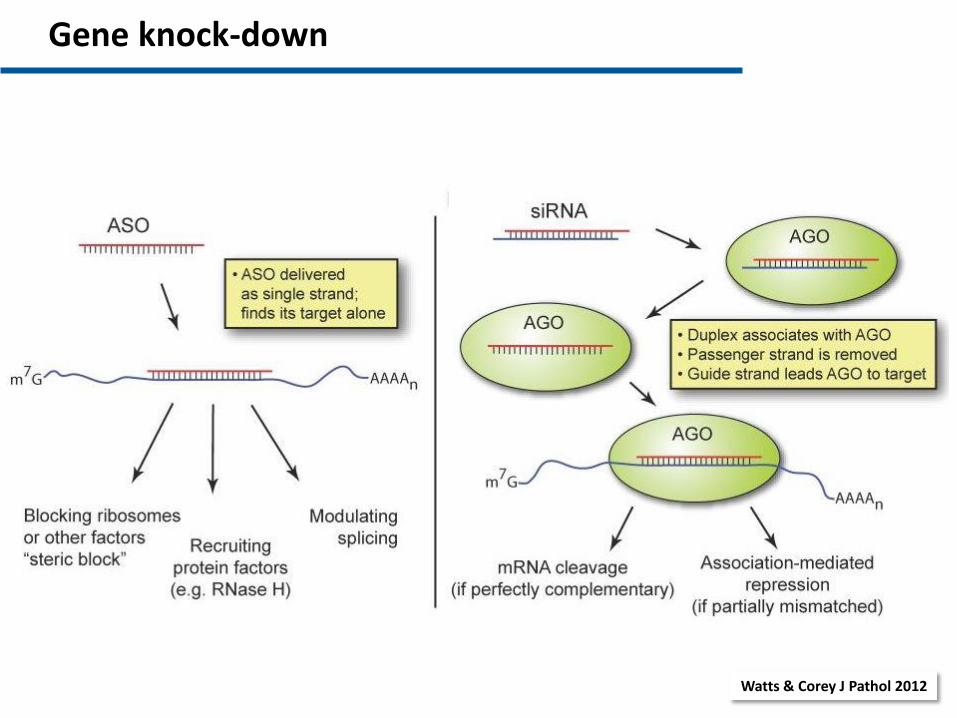
Gene knock-down
Watts & Corey J Pathol 2012
McLoughlin et al. Ann Neurol 2018
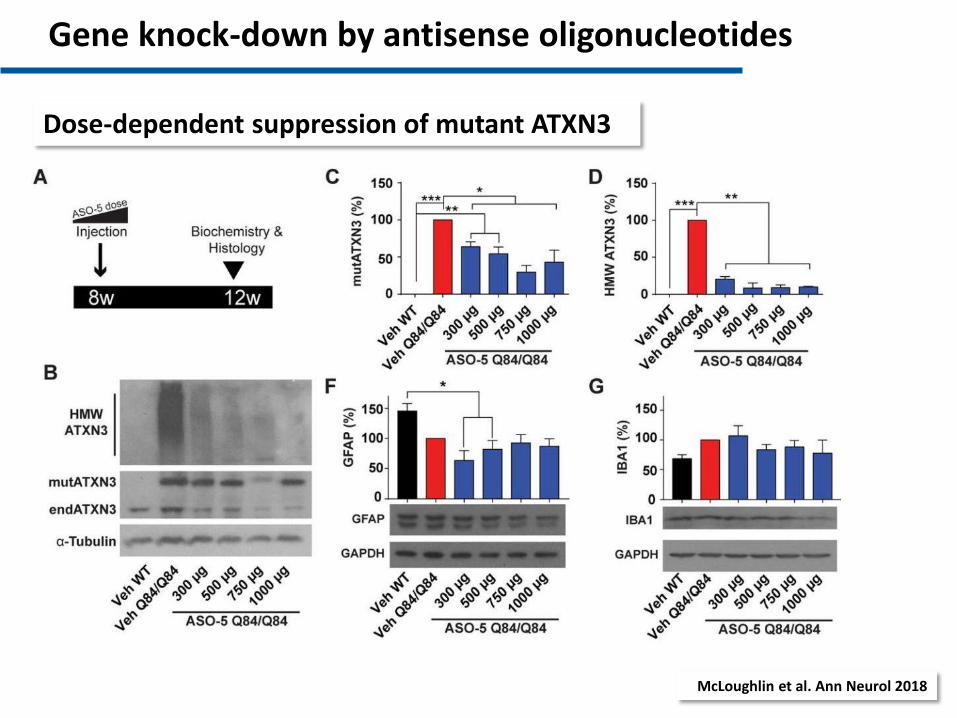
Dose-dependent suppression of mutant ATXN3
Gene knock-down by antisense oligonucleotides
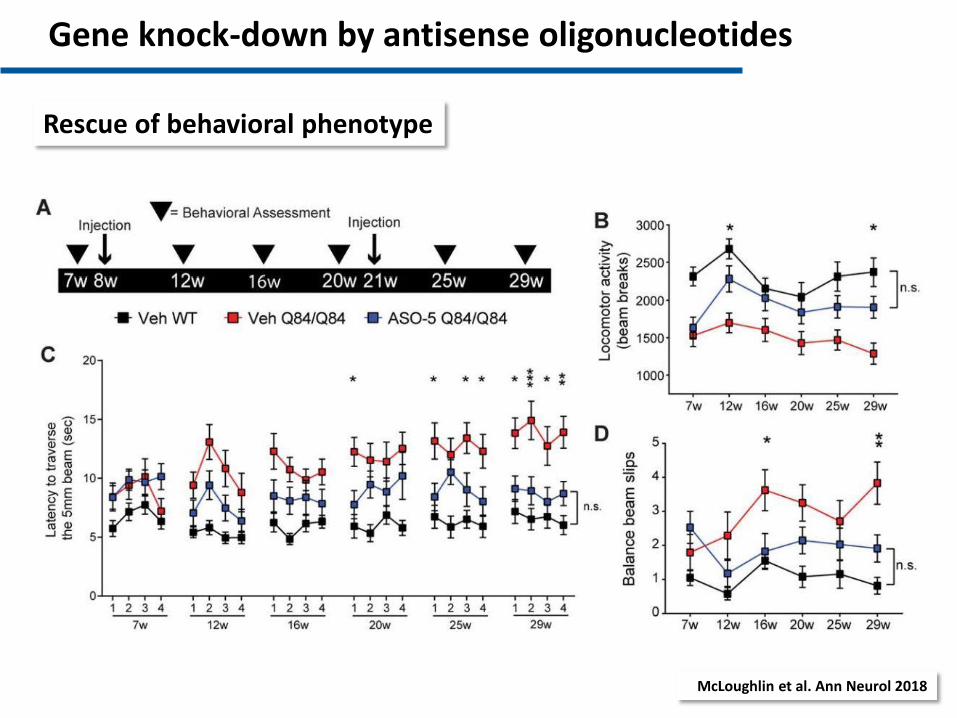
McLoughlin et al. Ann Neurol 2018
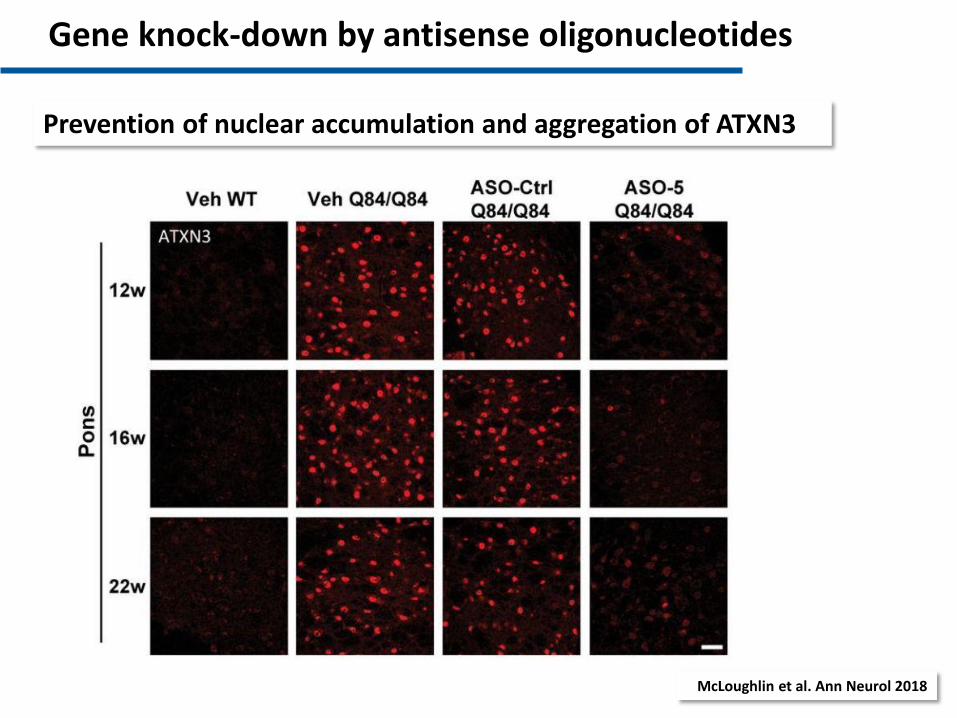
Prevention of nuclear accumulation and aggregation of ATXN3
Gene knock-down by antisense oligonucleotides
McLoughlin et al. Ann Neurol 2018
Rescue of behavioral phenotype
Gene knock-down by antisense oligonucleotides
• ASOs need to be repeatedly administered intrathecally at intervals of several months
• ASO treatment approved for SMA, positive trial in HD
• Active development programs by (big) pharmaceutical companies
Gene knock-down by antisense oligonucleotides
SARA
0 2 5 5 0 7 5 1 0 0
0
2 5
5 0
7 5
1 0 0
S A R A
VA
S
2 0 4 0 6 0 8 0 1 0 0
- 6 0
- 4 0
- 2 0
0
2 0
4 0
6 0
8 0
1 0 0
S A R A
VA
S
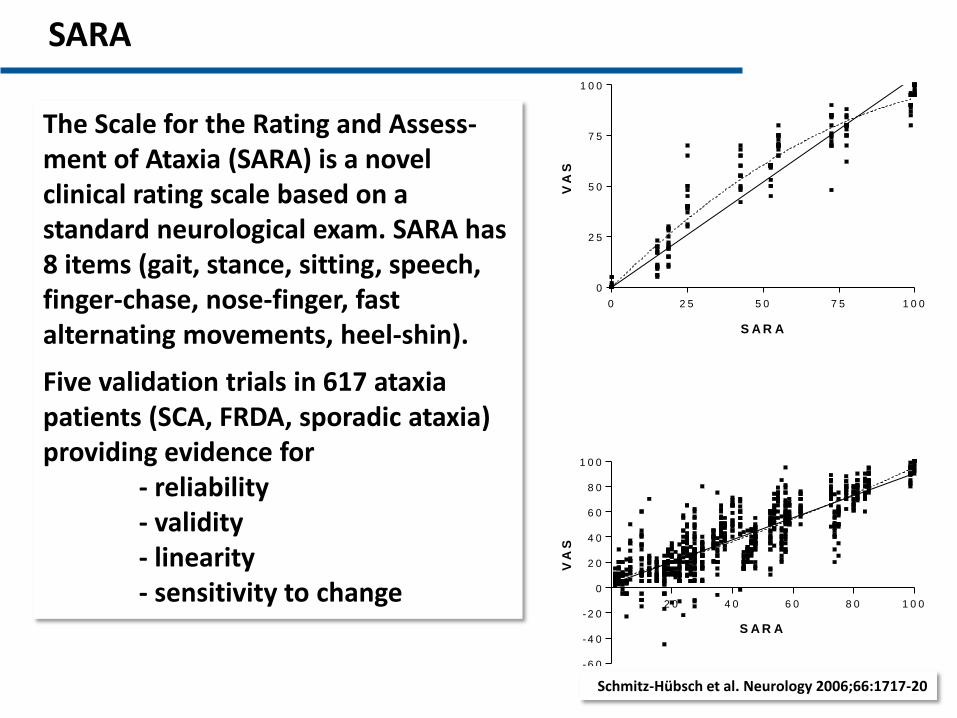
Schmitz-Hübsch et al. Neurology 2006;66:1717-20
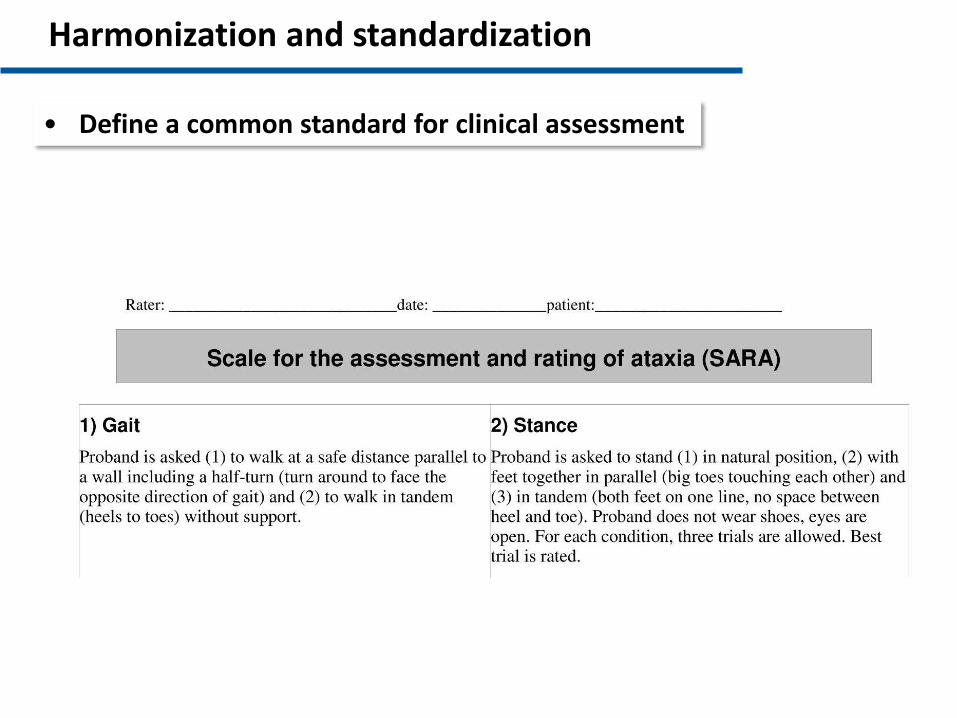
The Scale for the Rating and Assess-ment of Ataxia (SARA) is a novel clinical rating scale based on a standard neurological exam. SARA has 8 items (gait, stance, sitting, speech, finger-chase, nose-finger, fast alternating movements, heel-shin).
Five validation trials in 617 ataxia patients (SCA, FRDA, sporadic ataxia) providing evidence for - reliability - validity - linearity - sensitivity to change
Training and education
• SARA training tool
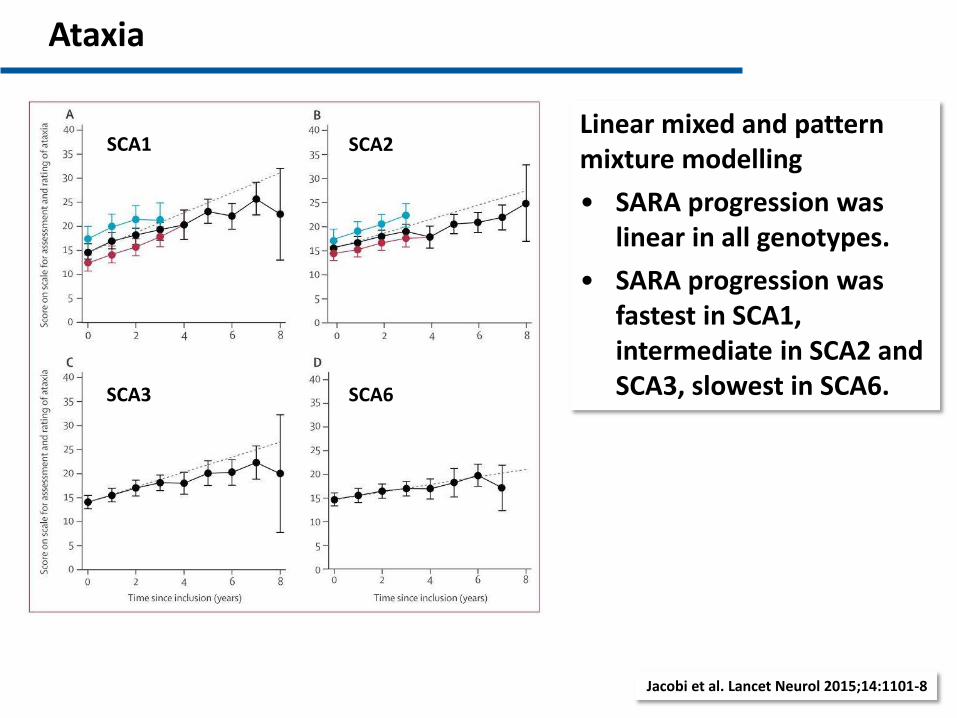
Jacobi et al. Lancet Neurol 2015;14:1101-8
Linear mixed and pattern mixture modelling
• SARA progression was linear in all genotypes.
• SARA progression was fastest in SCA1, intermediate in SCA2 and SCA3, slowest in SCA6.
Ataxia
SCA1 SCA2
SCA3 SCA6
Jacobi et al. Lancet Neurol 2013
Pre-ataxia stage
• RISCA is a longitudinal observational study of 300 non-ataxic first-degree relatives of SCA1, SCA2, SCA3 or SCA6 patients.
• Genetic testing was done anonymously so that study participants and investigators were not aware of the individual genetic status.
• SCA1, SCA2, SCA3 mutation carriers were enrolled on average 10 years before the expected ataxia onset, SCA6 carriers 20 years.
Jacobi et al. Lancet Neurol 2013
non-carrier
carrier
SCA1 SCA2 SCA3 SCA6
0 .0 0
0 .2 5
0 .5 0
0 .7 5
1 .0 0
CC
FS
.
- 0 .5 0
- 0 .2 5
0 .0 0
0 .2 5
0 .5 0
S C A 1 S C A 2 S C A 3 S C A 6
SC
AF
I
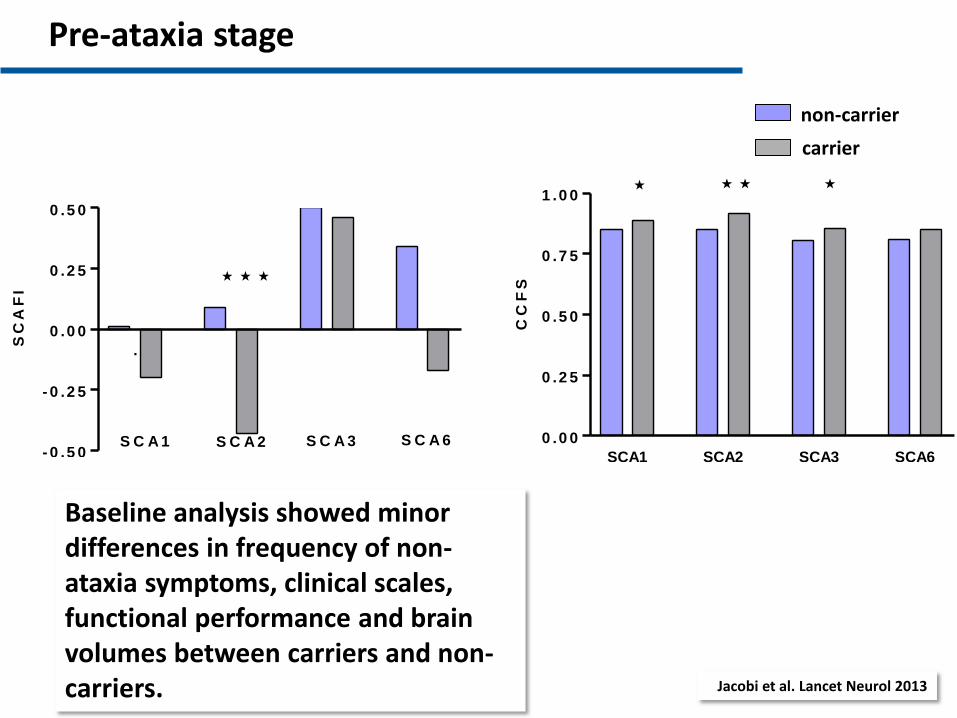
Baseline analysis showed minor differences in frequency of non-ataxia symptoms, clinical scales, functional performance and brain volumes between carriers and non-carriers.
Pre-ataxia stage
• Within the observation period, 52% of SCA1 mutation carriers converted to manifest ataxia.
• Clinical scales and test performance deteriorated in mutation carriers, but not non-carriers.
Pre-ataxia stage
Regions with significant volume loss in non-ataxic SCA3 mutation carriers (compared to controls): 4th ventricle, pallidum, medulla oblongata, pons, mesencephalon)
MRI marker
Regions with significant volume loss in ataxic SCA3 mutation carriers (compared to non-ataxic carriers): Cerebellar lobules
MRI marker
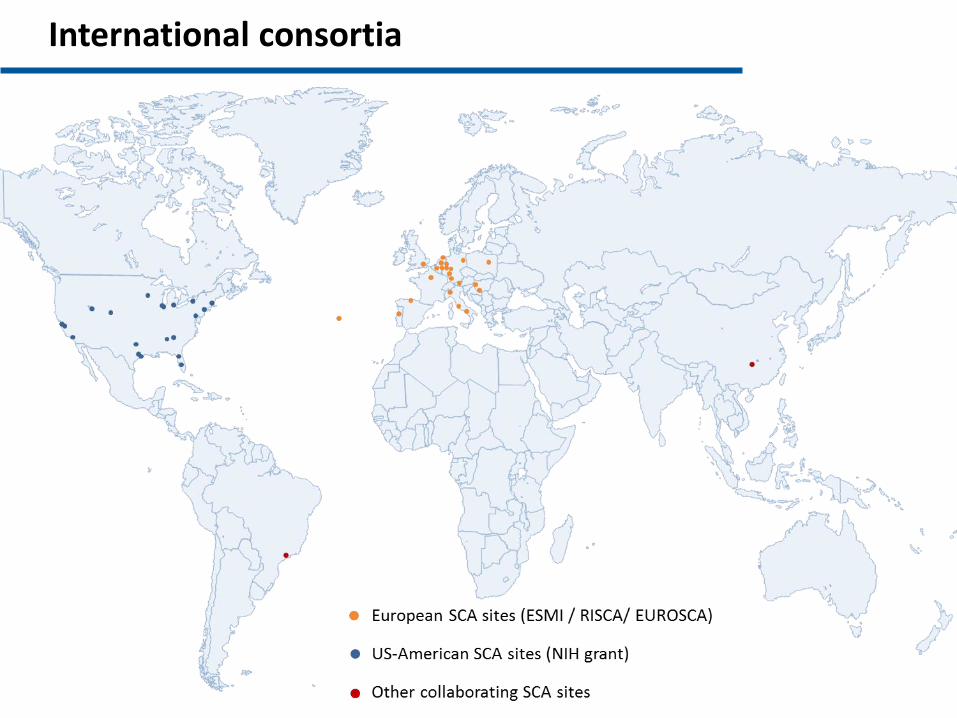
International consortia
Despite extensive knowledge of clinical features and natural history of the common polyQ-SCAs, there remain major knowledge gaps and hurdles that preclude further progress towards effective therapies. Specifically,
• it is not known how clinical features of SCA patients from different world regions compare to each other,
• there is no detailed knowledge of the disease evolution in non-polyQ-SCAs,
• imaging biomarkers have not yet been extensively validated,
• biochemical markers are almost completely lacking, and
• access to potential and well characterized study participants is limited.
Clinical SCA Research - Challenges
SCA Global is conceived as a flexible and open research platform, with which we wish to pursue the following goals:
• To better understand the manifestation, evolution and impact of the various SCAs
• To develop and validate biomarkers which can be used in future interventional trials
• To facilitate access to people with SCAs who are willing to participate in clinical trials
SCA Global
SCA Global has been launched during the NAF meeting in April 2018 in Philadelphia
Harmonization and standardization
• Define a common standard for clinical assessment
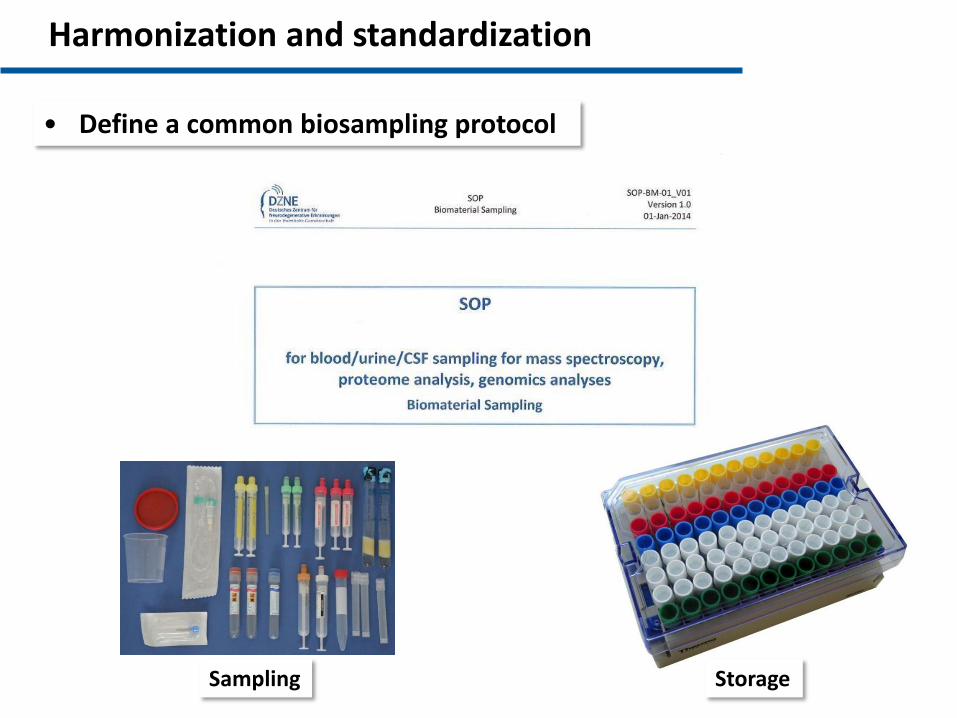
Sampling Storage
Harmonization and standardization
• Define a common biosampling protocol
Harmonization and standardization
• Define a common MRI protocol
• Liaise with ENIGMA Ataxia (Ian Harding)
Harmonization and standardization
• Define a common standard for consent forms
• Create templates for data and material transfers agreements
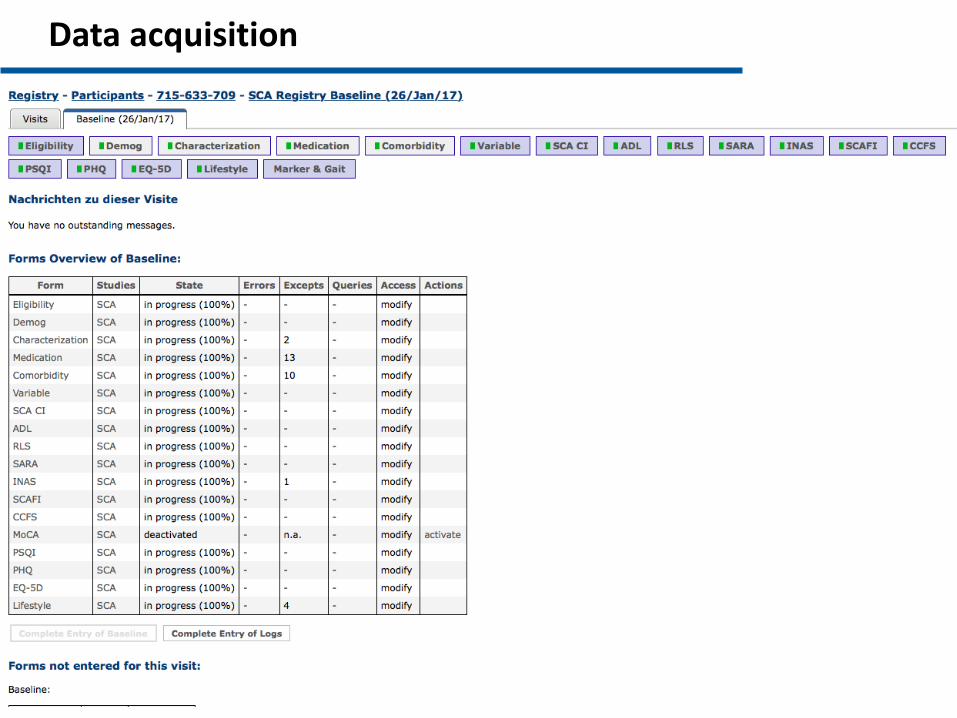
Data acquisition
• SCA Registry uses the same software as the Enroll-HD database (2mt Software (Ulm, Germany)
Data acquisition
• Transparent and democratic governance with participation of patient representatives
• Accordance with high standards of data protection
• Full and unlimited access of each investigator to own data and materials
• Fair access of investigators to data and materials
Basic principles
Governance
• Coordinator
• Steering committee NAF, EuroAtaxia, other lay organizations Clinical investigators (Europe, USA, South America, East Asia, Australia)
• Business office

Agenda
• Steering committee established
• Website launched
• Registration process in preparation
• Organize 1st SCA Global Meeting, 27-29 Mar 2019, Las Vegas
• Define standards (working groups)
• Start data merging/acquisition
Website





























