Embed Size (px)
Citation preview

Central Journal of Neurological Disorders & Stroke
Cite this article: Kim Y, Kondo M, Sunami Y, Kawata A1, Komori T, et al. (2014) MRI Findings in Spinocerebellar Ataxias. J Neurol Disord Stroke 2(3): 1072.
*Corresponding authorReiji Koide, Department of Neurology, Tokyo Metropolitan Neurological Hospital, 2-6-1 Musashidai, Fuchu, Tokyo 183-0042, Japan, Tel: 81+42-323-5110; Fax: 81+42-322-6219; Email:
Submitted: 02 January 2014
Accepted: 07 February 2014
Published: 21 February 2014
Copyright© 2014 Koide et al.
OPEN ACCESS
Keywords•Magnetic resonance imaging•Spinocerebellar ataxia•Radiologic-pathologic correlation•“Hot cross bun” sign
Review Article
MRI Findings in Spinocerebellar AtaxiasYounhee Kim1, Madoka Kondo1, Yoko Sunami1, Akihiro Kawata1, Takashi Komori2, Kiyomitsu Oyanagi3, Imaharu Nakano1 and Reiji Koide1*1Department of Neurology, Tokyo Metropolitan Neurological Hospital, Japan2Department of Pathology, Tokyo Metropolitan Neurological Hospital, Japan3Department of Brain Disease Research, Division of Neuropathology, Shinshu University School of Medicine, Japan
Abstract
The recent advances in genetic analysis have facilitated the classification of autosomal dominant or recessive spinocerebellar ataxia. Although differential diagnosis of spinocerebellar ataxia is clinically very complicated, MRI characteristics may be an important tool for diagnosis. In the present review article, we summarize the skills of neuroradiology for a diagnosis of various types of spinocerebellar ataxia.
AbbreviAtionsMSA: Multiple System Atrophy; SCA: Spinocerebellar Ataxia;
DRPLA: Dentatorubral Pallidoluysian Atrophy; AOA: Ataxia with Oculomotor Apraxia; ALD: Adrenoleukodystrophy; AMN: Adrenomyeloneuropathy; PSP: Progressive Supranuclear Palsy; MRI: Magnetic Resonance Imaging; KB staining: Klüver-Barrera (KB) staining
introductionSpinocerebellar Ataxia (SCA) is one of a group of
neurodegenerative disorders characterized by slowly progressive dis-coordination of limbs and gait. The recent advances in genetic analysis have facilitated the classification of autosomal dominant or recessive SCA. The differential diagnosis of SCA is considered one of the most important skills in neurology. The article aims to review research findings on the value of Magnetic Resonance Imaging (MRI) in the differential diagnosis of various types of SCA.
discussion And conclusion
Multiple system Atrophy (MsA)
Multiple System Atrophy (MSA) is a neurodegenerative disorder that affects cerebellar, extrapyramidal, and autonomic systems. The most frequent symptoms include cerebellar ataxia, parkinsonism, and autonomic failures (such as postural hypotension and urinary dysfunction). This condition progresses slowly over several years, and will become being a bedridden state. Physicians often classify MSA as either MSA-C (with predominant cerebellar ataxia) or MSA-P (with predominant parkinsonism). We discuss here MSA-C. Characteristic MRI findings in MSA-C are cerebellar atrophy accompanied by dilatation of fourth ventricle,
atrophy of the brainstem (predominantly in pontine base), and “hot cross bun” sign (Figure 1) [1,2]. In MSA-C, high-signal-intensity lesions are observed in the pons and middle cerebellar peduncles on T2-weighted MR images. Cruciform hyperintensity in the pons is known as “hot cross bun” sign, which may reflect loss of myelinated transverse pontocerebellar fibers (Figure 3A, D).
spinocerebellar ataxia type 3 (scA3)
SCA3, also known as Machado-Joseph disease, is the most common hereditary SCA in worldwide, and is caused by the expansion of a CAG repeat in the ataxin-3 gene [3]. The clinical features of younger-onset SCA3 patients are cerebellar ataxia, spasticity, and dystonia, whereas those of older-onset SCA3 patients are cerebellar ataxia, polyneuropathy, and ophthalmoplegia. Although atrophy of the brainstem and cerebellum is common features on MRI, it should be noted that the MRI abnormalities are difficult to detect in the early stage of SCA3. We should carefully evaluate the atrophy in the pontine tegmentum (Figure 2A,B) [4]. In the later stage, brainstem and cerebellar atrophy will be clear, and we can often observe linear high-intensity-signal lesion in the midline of pons coursing an anteroposterior direction (Figure 3B). This finding is considered to be early change of “hot cross bun” sign. In SCA3, neurons of the pontine nuclei are slightly shrunken, but the cell architecture is well preserved. Therefore, the myelinated transverse pontocerebellar fibers are preserved as compared to MSA-C, and loss of these fibers can be observed only in the midline of pons where the fibers coming from the left and right pontine nuclei cross (Figure 3B, E).
spinocerebellar ataxia type 1 (scA1)
Spinocerebellar ataxia type 1 (SCA1) is an autosomal dominant

Central
Koide et al. (2014)Email:
J Neurol Disord Stroke 2(3): 1072 (2014) 2/5
SCA characterized by cerebellar ataxia, spasticity, increased tendon reflexes, cognitive impairment, and ophthalmoplegia. SCA1 is caused by the expansion of a CAG repeat in the ataxin-1 gene [5]. Characteristic MRI findings are atrophy of the brainstem and cerebellum (Figure 4), which resemble those of SCA3 [6]. Similarly to SCA3, linear high-intensity-signal lesion in the midline of pons coursing an anteroposterior direction is also observed (“hot cross bun” sign).
spinocerebellar ataxia type 2 (scA2)
The clinical features of SCA2 include cerebellar ataxia, slow saccadic eye movement, involuntary movement (such as myoclonus, dystonia), dementia, and polyneuropathy. SCA2 is caused by the expansion of a CAG repeat in the ataxin-2 gene [7-9]. Brain MRI show prominent atrophy of the brainstem and
cerebellum. Atrophy of the pons is more prominent in the pontine base than in the pontine tegmentum, and “hot cross bun” sign is observed in the pons on axial T2-weighted MR images (Figure 5) [10,11]. MRI findings of SCA2 are quite similar to those of MSA-C. When a young patient shows on MRI findings resembling to MSA-C, we should consider a possibility of SCA2.
spinocerebellar ataxia type 6 (scA6), spinocerebellar ataxia type 31 (scA31)
Both spinocerebellar ataxia type 6 (SCA6) and spinocerebellar ataxia type 31 (SCA31) are autosomal dominant SCA, and exhibit late-onset pure cerebellar phenotype. In SCA6 and SCA31, cardinal symptom is cerebellar ataxia, although mild dystonia in the limbs is occasionally observed. SCA 6 is caused by the small expansion of a CAG repeat in the alpha1A-voltage-dependent
Figure 1 MR images of a patient with MSA-C.A 55-year-old Japanese male presented with 2-year history of dysarthria. The MR images obtained at 55 years of age show atrophy of the cerebellum and brainstem associated with dilatation of the fourth ventricle. (A) In the sagittal T1-weighted MR image, atrophy of the pons is more prominent in the pontine base than in the pontine tegmentum. (B) Axial T2-weighted MR image shows cruciform hyperintensity (“hot cross bun” sign) in the pons. Middle cerebellar peduncles are also atrophied, with high-signal-intensity lesions.
Figure 2 MR images of a patient with SCA3A 42-year-old Japanese female presented with slowly progressive gait disturbance since 36 years of age. At 42 years of age, she was unable to walk without assistance, and neurological examinations showed limb and truncal ataxia, increased tendon reflexes, and extensor plantar responses. The MR images were obtained at 42 years of age. (A) Sagittal T1-weighted MR image shows mild atrophy of the pons (particularly in the pontine tegmentum) and cerebellum. (B) The pontine tegmentum is defined as the dorsal area of the pons between the medial lemniscus and the base of the fourth ventricle (between the arrows).(C) Axial T2-weighted MR image shows mild atrophy of the pons and cerebellum.

Central
Koide et al. (2014)Email:
J Neurol Disord Stroke 2(3): 1072 (2014) 3/5
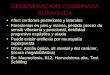
Figure 3 Radiologic-pathologic correlation of MSA-C and SCA3(A) Axial T2-weighted MR image in a patient with MSA-C shows atrophy of the pons with cruciform hyperintensity (“hot cross bun” sign).(B) Axial T2-weighted MR image in a patient with SCA3 shows atrophy of the pons with linear high-intensity-signal lesion in the midline of pons coursing an anteroposterior direction.(C) Klüver-Barrera (KB) staining section of the pons from normal control.(D) KB staining section of the pons from a patient with MSA-C (the same case as Panel B) shows atrophy of the pons and marked reduction of the myelinated fibers including transverse pontocerebellar fibers. (E) KB staining section of the pons from a patient with SCA3 (the same case as Panel C) shows marked atrophy of the pons. Although loss of myelinated fiber is very mild compared with the MSA-C, it is also observed in the midline of pontine base (arrow).
Figure 4 MR images of a patient with SCA1The patient is a 44-year-old Japanese female. Her first symptom was gait instability, which began when she was 35 years old. At 44 years of age, neurological examinations showed obvious limb and truncal ataxia, increased tendon reflexes, and moderate dementia. The MR images were obtained at 44 years of age. (A) Sagittal T1-weighted MR image shows atrophy of the cerebellum and brainstem. (B) Axial T2-weighted MR image shows atrophy of the cerebellum, brainstem, and middle cerebellar peduncles. In the pons, linear high-intensity-signal lesion in the midline of pons is slightly observed (arrow).
calcium channel gene [12], and SCA31 is caused by 2.5- to 3.8-kb insertion containing pentanucleotide repeats within an intron of the BEAN gene [13]. MRI findings of SCA6 or SCA31 show isolated cerebellar atrophy without brainstem and cerebral involvement (Figure 6 and 7) [14,15]. We are not able to distinguish between SCA6 and SCA31 clinically or radiologically.
dentatorubral pallidoluysian atrophy (drPlA)
DRPLA is an autosomal dominant spinocerebellar ataxia caused by the expansion of a CAG repeat in the atrophin-1 gene [16,17]. On interpretation of the MRI of DRPLA, we should divide the patients into a juvenile-onset group and an adult-onset group.

Central
Koide et al. (2014)Email:
J Neurol Disord Stroke 2(3): 1072 (2014) 4/5
Figure 5 MR images of a patient with SCA2The patient, a 28-year-old Japanese male, presented with gait instability and tremor of the head. His initial symptoms of head tremor developed in his 20s. At 28 years of age, neurological examinations demonstrated tremor of the head, slow saccadic eye movement, limb and truncal ataxia, dysarthria, and neck dystonia. The MR images were obtained at 28 years of age.(A) Sagittal T1-weighted MR image shows atrophy of the cerebellum and brainstem associated with dilatation of the fourth ventricle. Similar to MSA-C, atrophy of the pons is more prominent in the pontine base than in the pontine tegmentum.(B) Axial T2-weighted MR image show atrophy of the cerebellum and brainstem, and “hot cross bun” sign. High-intensity-signal lesions are slightly showed in the middle cerebellar peduncles.
Figure 7 MR images of a patient with SCA31.A 63-year-old Japanese male presented with a 5-year history of unsteady gait. At 63 years of age, neurological examinations showed dysarthria, limb and truncal ataxia. The MR images were obtained at 63 years of age.(A) Sagittal T1-weighted MR image shows atrophy of the cerebellar vermis.(B) Axial T2-weighted MR image shows atrophy of the cerebellum without brainstem and cerebral involvement.
Figure 6 MR images of a patient with SCA6.A 60-year-old Japanese female presented with slowly progressive gait disturbance since 45 years of age. At 60 year of age, neurological examinations showed limb and truncal ataxia, and she was unable to walk without assistance. The MR images were obtained at 60 years of age.(A) Sagittal T1-weighted MR image shows atrophy of the cerebellar hemispheres and vermis. (B) (C) Axial T2-weighted MR images show atrophy of the cerebellum without brainstem and cerebral involvement.

Central
Koide et al. (2014)Email:
J Neurol Disord Stroke 2(3): 1072 (2014) 5/5
Figure 8 MR images of a patient with DRPLA (adult-onset group). The patient is a 63-year-old Japanese male. He presented with unsteady gait at 60 years of age. At 63, he presented limb and truncal ataxia. The MR images were obtained at 63. (A) Sagittal T1-weighted MR image shows atrophy of the cerebellum and brainstem. (B) (C) (D) Axial T2-weighted MR images show high-signal-intensity lesion in the cerebral white matter and pons, in addition to atrophy of the cerebellum.
Figure 9 MR images of a patient with DRPLA (juvenile-onset group).The patient is a 40-year-old Japanese male. His symptoms began at 25 years of age with generalized seizure. His intellectual function deteriorated gradually, and the epilepsy remained resistant to drug therapy. At 40 years of age, he was bedridden, and was unable to communicate. The MR images were obtained at 40 years of age. (A) Sagittal T1-weighted MR image shows atrophy of the cerebellum, brainstem, cerebral hemisphere, and corpus callosum. (B) (C) (D) Axial T2-weighted MR images show prominent atrophy of the cerebral hemispheres, in addition to atrophy of the cerebellum. Involvement of the cerebral white matter is not clear.

Central
Koide et al. (2014)Email:
J Neurol Disord Stroke 2(3): 1072 (2014) 6/5
The former exhibits myoclonus epilepsy, and the latter cerebellar ataxia with chorea. On MR imaging, atrophy of the brainstem and cerebellum are common findings. In contrast to those of MSA, atrophy of the pons is more prominent in the pontine tegmentum than in the pontine base. In adult-onset group, high-signal-intensity lesions are observed in the cerebral white matter, brainstem, and thalamus on T2-weighted MR images (Figure 8) [18]. On the other hand, in juvenile-onset group, signal abnormalities in the cerebral white matter are usually absent (or periventricular white matter changes appear in the most advanced stage). Severe cerebral atrophy is a characteristic finding in juvenile-onset group (Figure 9) [18]. Cerebral atrophy in juvenile-onset group may correlate to the severe dementia and epilepsy [19].
Ataxia with oculomotor apraxia type 1 (AoA1)
AOA1 is an autosomal recessive neurodegenerative disorder characterized by cerebellar ataxia, oculomotor apraxia, and peripheral neuropathy, and results from a mutation in the aprataxin gene [20]. The key clue that should alert physicians to consider the possibility of AOA1 is the presence of oculomotor apraxia (86%) [21]. MRI of AOA1 show cerebellar atrophy, mild
brainstem atrophy, and, in advanced cases, cortical atrophy (Figure 10) [21].
Ataxia with oculomotor apraxia type 2 (AoA2)
AOA2 is an autosomal recessive neurodegenerative disorder characterized by cerebellar ataxia, saccadic ocular pursuit, oculomotor apraxia (less than 50%), and peripheral neuropathy, and is caused by mutation in the senataxin gene [22]. The most striking characteristics of AOA2 are the presence of peripheral neuropathy and elevated serum levels of alpha-fetoprotein [23]. MRI finding of AOA2 is cerebellar atrophy (Figure 11).
Miscellaneous diseases masquerading as spinocerebellar ataxia
Superficial siderosis: Superficial siderosis of the central nervous system is a rare disorder that results of choronic subarachnoid hemorrhage and hemosiderin deposition on the leptomeninges of the brain and spinal cord [24]. Clinical features of this condition include sensorineural hearing loss, cerebellar ataxia, and pyramidal signs. By T2-star weighted image, hemosiderin deposition on the leptomeninges can be detected with high sensitivity (Figure 12).
Figure 10 MR images of a patient with AOA1.The patient is a 37-year-old Japanese male. He presented with unsteady gait at 2 years of age. At 8, a pediatrician had pointed out abnormal ocular movement and cerebellar atrophy on the MRI. At 37, he was unable to walk, and neurological examinations showed mild mental retardation, limb and truncal ataxia, absent tendon reflexes, and oculomotor apraxia. The MR images were obtained at 37 years of age. (A) Sagittal T1-weighted MR image shows prominent atrophy of the cerebellum. (B) Axial T2-weighted MR image shows atrophy of the cerebellum, without obvious involvement of the brainstem.
Figure 11 MR image of a patient with AOA2.The patient is a 55-year-old Japanese male with consanguineous parents. He presented with gait disturbance in his teens. Cerebellar ataxia and peripheral neuropathy progressed gradually to a wheelchair-bound state at around 30 years. Ophthalmologic examinations showed saccadic ocular pursuit, but not oculomotor apraxia. The MR image was obtained at 55 years of age. Sagittal T1-weighted MR image shows marked atrophy of the cerebellum.

Central
Koide et al. (2014)Email:
J Neurol Disord Stroke 2(3): 1072 (2014) 7/5
Figure 12 MR image of a patient with superficial siderosis.The patient is a 63-year-old Japanese male presented with a 1-year history of unsteady gait and hearing loss. At 63 years of age, he presented bilateral sensorineural hearing loss, truncal ataxia, and urinary incontinence. The MR image was obtained at 63 years of age. Axial T2-star weighted MR image shows low-signal intensity surrounding the central nervous system surface, indicating hemosiderin deposition.
Figure 13 MR images of a patient with AMN.The patient is a 65-year-old Japanese male. His first symptom was gait difficulty, which began when he was 40 years old. Progression of the spastic gait was very so slow that he was still able to walk with a cane at 65 years of age. The MR images were obtained at 65 years of age [25]. (A) Sagittal T1-weighted MR image shows mild atrophy of the cerebellum. (B) Axial T2-weighted MR image shows no remark
Adrenomyeloneuropathy (AMN): Adrenoleukodystrophy (ALD) is an X-linked metabolic disorder, and has a widely varied disease phanotype. AMN is one of the clinical phenotype of ALD, and has mainly an involvement of spinal cord and peripheral nerves. Patients with ALD usually show diffuse cerebral white matter signal change. On the other hand, half of the patients with AMN exhibit cerebral involvement about 10 years after onset. In such cases, atrophy of the cerebellum or spinal cord may be observed alone (Figure 13) [25]. Key clues that should alert physicians to consider the possibility of ALD include the presence of adrenal insufficiency, cutaneous and mucosal pigmentation, and early baldness. Measurement of plasma very long-chain fatty acids has been widely used as a screening test for ALD.
Progressive supuranuclear palsy (PsP) with cerebellar ataxia: PSP is a parkinsonian disorder characterized by supranuclear vertical gaze palsy, nuchal dystonia, dementia, and frequent falls. In the cases of PSP, there are some cases presenting with cerebellar ataxia as the initial symptoms [26]. On interpretation of MRI findings in the patients with cerebellar ataxia, we should also evaluate atrophy of the midbrain tegmentum.
reFerences1. Savoiardo M, Strada L, Girotti F, Zimmerman RA, Grisoli M, Testa D,
et al. Olivopontocerebellar atrophy: MR diagnosis and relationship to multisystem atrophy. Radiology. 1990; 174: 693-696.
2. Srivastava T, Singh S, Goyal V, Shukla G, Behari M. “Hot cross bun” sign in two patients with multiple system atrophy-cerebellar. Neurology. 2005; 64: 128.
3. Kawaguchi Y, Okamoto T, Taniwaki M, Aizawa M, Inoue M, Katayama S, et al. CAG expansions in a novel gene for Machado-Joseph disease at chromosome 14q32.1. Nat Genet. 1994; 8: 221-228.
4. Onodera O, Idezuka J, Igarashi S, Takiyama Y, Endo K, Takano H, et al. Progressive atrophy of cerebellum and brainstem as a function of age and the size of the expanded CAG repeats in the MJD1 gene in Machado-Joseph disease. Ann Neurol. 1998; 43: 288-296.
5. Orr HT, Chung MY, Banfi S, Kwiatkowski TJ Jr, Servadio A, Beaudet AL, et al. Expansion of an unstable trinucleotide CAG repeat in spinocerebellar ataxia type 1. Nat Genet. 1993; 4: 221-226.
6. Bürk K, Abele M, Fetter M, Dichgans J, Skalej M, Laccone F, et al. Autosomal dominant cerebellar ataxia type I clinical features and MRI in families with SCA, SCA2 and SCA3. Brain. 1996; 119 : 1497-1505.
7. Pulst SM, Nechiporuk A, Nechiporuk T, Gispert S, Chen XN, Lopes-

Central
Koide et al. (2014)Email:
J Neurol Disord Stroke 2(3): 1072 (2014) 8/5
Kim Y, Kondo M, Sunami Y, Kawata A1, Komori T, et al. (2014) MRI Findings in Spinocerebellar Ataxias. J Neurol Disord Stroke 2(3): 1072.
Cite this article
Cendes I, et al. Moderate expansion of a normally biallelic trinucleotide repeat in spinocerebellar ataxia type 2. Nature Genet. 1996; 14: 269-276.
8. Sanpei K, Takano H, Igarashi S, Sato T, Oyake M, Sasaki H, et al. Identification of the spinocerebellar ataxia type 2 gene using a direct identification of repeat expansion and cloning technique, DIRECT. Nat Genet. 1996; 14: 277-284.
9. Imbert G, Saudou F, Yvert G, Devys D, Trottier Y, Garnier JM, et al. Cloning of the gene for spinocerebellar ataxia 2 reveals a locus with high sensitivity to expanded CAG/glutamine repeats. Nat Genet. 1996; 14: 285-291.
10. Ying SH, Choi SI, Perlman SL, Baloh RW, Zee DS, Toga AW. Pontine and cerebellar atrophy correlate with clinical disability in SCA2. Neurology. 2006; 66: 424-426.
11. Lee YC, Liu CS, Wu HM, Wang PS, Chang MH, Soong BW. The ‘hot cross bun’ sign in the patients with spinocerebellar ataxia. Eur J Neurol. 2009; 16: 513-516.
12. Zhuchenko O, Bailey J, Bonnen P, Ashizawa T, Stockton DW, Amos C, et al. Autosomal dominant cerebellar ataxia (SCA6) associated with small polyglutamine expansions in the alpha 1A-voltage-dependent calsium channel. Nature Genet. 1997; 15: 62-69.
13. Sato N, Amino T, Kobayashi K, Asakawa S, Ishiguro T, Tsunemi T, et al. Spinocerebellar ataxia type 31 is associated with “inserted” penta-nucleotide repeats containing (TGGAA)n. Am J Hum Genet. 2009; 85: 544-557.
14. Ikeuchi T, Takano H, Koide R, Horikawa Y, Honma Y, Onishi Y, et al. Spinocerebellar ataxia type 6: CAG repeat expansion in alpha1A voltage-dependent calcium channel gene and clinical variations in Japanese population. Ann Neurol. 1997; 42: 879-884.
15. Nozaki H, Ikeuchi T, Kawakami A, Kimura A, Koide R, Tsuchiya M, et al. Clinical and genetic characterizations of 16q-linked autosomal dominant spinocerebellar ataxia (AD-SCA) and frequency analysis of AD-SCA in the Japanese population. Mov Disord. 2007; 22: 857-862.
16. Koide R, Ikeuchi T, Onodera O, Tanaka H, Igarashi S, Endo K, et al. Unstable expansion of CAG repeat in hereditary dentatorubral-pallidoluysian atrophy (DRPLA). Nat Genet. 1994; 6: 9-13.
17. Nagafuchi S, Yanagisawa H, Sato K, Shirayama T, Ohsaki E, Bundo M, et al. Dentatorubral and pallidoluysian atrophy expansion of an unstable CAG trinucleotide on chromosome 12p. Nat Genet. 1994; 6: 14-18.
18. Koide R, Onodera O, Ikeuchi T, Kondo R, Tanaka H, Tokiguchi S, et al. Atrophy of the cerebellum and brainstem in dentatorubral pallidoluysian atrophy. Influence of CAG repeat size on MRI findings. Neurology. 1997; 49: 1605-1612.
19. Sunami Y, Koide R, Arai N, Yamada M, Mizutani T, Oyanagi K. Radiologic and neuropathologic findings in patients in a family with dentatorubral-pallidoluysian atrophy. AJNR Am J Neuroradiol. 2011; 32: 109-114.
20. Date H, Onodera O, Tanaka H, Iwabuchi K, Uekawa K, Igarashi S, et al. Early-onset ataxia with ocular motor apraxia and hypoalbuminemia is caused by mutations in a new HIT superfamily gene. Nat Genet. 2001; 29: 184-188.
21. Le Ber I, Moreira MC, Rivaud-Péchoux S, Chamayou C, Ochsner F, Kuntzer T, et al. Cerebellar ataxia with oculomotor apraxia type 1: clinical and genetic studies. Brain. 2003; 126: 2761-2772.
22. Moreira MC, Klur S, Watanabe M, Németh AH, Le Ber I, Moniz JC, et al Senataxin, the ortholog of a yeast RNA helicase, is mutant in ataxia-ocular apraxia 2. Nat Genet. 2004; 36: 225-227.
23. Anheim M, Monga B, Fleury M, Charles P, Barbot C, Salih M, et al. Ataxia with oculomotor apraxia type 2: clinical, biological and genotype/phenotype correlation study of a cohort of 90 patients. Brain. 2009; 132: 2688-2698.
24. Bracchi M, Savoiardo M, Triulzi F, Daniele D, Grisoli M, Bradac GB, et al. Superficial siderosis of the CNS: MR diagnosis and clinical findings. AJNR Am J Neuroradiol. 1993; 14: 227-236.
25. Morita M, Kobayashi J, Yamazaki K, Kawaguchi K, Honda A, Sugai K, et al. A Novel Double Mutation in the ABCD1 Gene in a Patient with X-linked Adrenoleukodystrophy: Analysis of the Stability and Function of the Mutant ABCD1 Protein. JIMD Rep. 2013; 10: 95-102.
26. Kanazawa M, Shimohata T, Toyoshima Y, Tada M, Kakita A, Morita T, et al. Cerebellar involvement in progressive supranuclear palsy: A clinicopathological study. Mov Disord. 2009; 24: 1312-1318.