Embed Size (px)
Citation preview

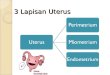
Hysteroscopic Myomectomy
Trans-Cervical Resection of
Myoma (TCRM)
A. Prof. Dr Aisha Mohamed El-Bareg MBBS, DGO, MMedSci (ART), ABOG, (MD), PhD (UK)
Consultant Obstetrician & Gynecologist / subspecialty
in Endoscopic Surgery and Reproductiv medicine
Al-Amal Hospital for Obs&Gyn. Infertility Treatments
and Genetic Research
Faculty of Medicine , Misurata University /Libya

Uterine myomas are benign encapsulated
tumors that originate from the muscle tissue
of the uterus.
Depending upon their location, they can be
classified as :
Subserosal
Intramural
Submucousal.
Cervical, broad ligament myoma
Fibroid, Myoma, Liomyoma


Fibroid, Myoma, Liomyoma
Most frequent benign tumour in gyn practice.
Occurs in 20-30% of women of reproductive
age and frequently increases toward the end of
the reproductive period.
Estrogen increases its growth.
Hysterectomy and laparotomic myomectomy
used to be the tt of choice in women with HMB
and infertility.
Most common reason for hysterectomy.

Burden of Myomas for patients
Pain, Cramping, pressure symptoms
Heavy menstrual bleeding
Anemia
Reproductive complications:
Infertility
Miscarriages
Preterm labor
Malpresentations
Uterine fibroid may be asymptomatic.

Evaluation and classification of
fibroid Submucous fibroids account for 5.5% -16.6% of
all uterine fibroids.
A common structural cause of AUB, pelvis pain,
infertility, and other symptoms.
In women with infertility, an effort should be
made to adequately evaluate and classify
fibroids, particularly those impinging on the
endometrial cavity

Diagnosis -Submucosal Fibroids
Diagnosis:
1. TVS
2. SIS
3. MRI

4. Hysteroscopy
appear as white spherical
masses covered by
network of thin fragile
vessles.

Treatment considerations
Treatment of uterine fibroids can be complex
because:
Fibroids can be located in any part of the uterus
Multiple fibroids can reside in one uterus.
Fibroid can be different sizes.
Fibroid disease varies in severity (some uteri
are replete with tumors).

Fibroids have variable growth rates: some
grow, others are stable, some shrink
spontaneously.
There is no universally accepted classification
system.
Symptoms vary: some studies focused only
on bleeding outcome, other outcomes are
important- pain, fertility, re-intervention.
Treatment considerations

Treatment options
Watchful waiting.
Pain medications.
Hormone therapy.
GnRH agonist/antagoist .
Progesterone-blocking agents (Mefipristone).
Aromatase-blocking agents (Letrozole).
Progestin only pill.
Oral contraceptive pills.

Intrauterine device (Mirena)
Minimally invasive options:
Uterine artery embolization
MRI-guided focused USS
Hysteroscopic/laparoscopic
resection
Treatment options

• In women with otherwise unexplained infertility,
submucosal fibroids should be removed in
order to improve conception and pregnancy
rates.
• There is fair evidence to recommend against
myomectomy in women with intramural fibroids
(hysteroscopically confirmed intact
endometrium) and otherwise unexplained
infertility, regardless of the size of the fibroids.
Surgical Management

Hysteroscopic myomectomy
TransCervical Resection of Myoma
(TCRM)
In the past, a diagnosis of submucous myoma
was usually followed by a recommendation for
hysterectomy.
Dilation and curettage (D&C). a blind
procedure guided by tactile feedback, may be
used as a diagnostic procedure to obtain
tissue for pathologic examination, a
temporizing measure for heavy uterine
bleeding.

Hysteroscopic myomectomy-TCRM
Today, hysteroscopic surgery offers an accurate
diagnostic, assessment and therapeutic
alternatives.
Goal of hysteroscopic myomectomy is
removal of the entire fibroid without
compromising the surrounding myometrium or
endometrium. This will result in alleviation of
the patient’s symptoms without weakening the
myometrium or creating intracavitary
synechia. Removal of the entire myoma will
also decrease the risk of regrowth of the
lesion.

Hysteroscopic Myomectomy- TCRM
Pre-operative assessment:
Fibroid size and location within the uterine
cavity.
Thickness of residual myometrium to the serosa.
Degree of protrusion to the cavity.
A combination of TVS and Hysteroscopy are the
modalities of choice.
Endometrial biopsy is also indicated.

Classification/ European Society Of Hysteroscopy
)0(G0 GRADE
limited to uterine
cavity.
Pedunculated
)1(G1 GRADE
Partial intramural
>50%
endocavitary.
Angle of
protrusion<90o
)2(G2 GRADE
Predominantly
intamural <50%
endocavitary
Angle of protrusion
>90o


Submucosal fibroids are managed hystero-
scopically. The fibroid size should be < 5 cm,
although larger fibroids have been managed
hysteroscopically, but repeat procedures are
often necessary.
Preferred due to:
Higher efficacy
Reduction in surgical morbidity
Absence of abdominal scar
Hysteroscopic Myomectomy- TCRM

Pre-procedural Preparation
1. Use of suppressive medical therapy:
GnRH agonist is commonly used.
Reduction of myoma volume by 40%
Amenorrhea to built up hemoglobin.
Facilitation of procedure, risk of bleeding.
Reduced systemic absorption of the distending
media
Complete resection of large myomas in one
setting.

Factors For GnRH analogues
Parameters disfavoring Infavour pre-tt
•Anaemia none or mild pronounced
•Type of myoma G0 or GI G2
•Diameter <2cm > 4cm
•Residual distance 10 mm <8 mm
to serosa.
•No. of Myoma Single Multiple
•Location. Anterior, post fundus, close to
or lateral tubal ostium
•Ability of the surgeon highly skilled skilled

Pre-procedural Preparation
Various dosing regimens of GnRH a exist.
Depot Luprolide Acetate 7.5 mg IM 6 weeks
preoperatively.
The second injection is given 4 weeks later
and the surgery is scheduled 2–4 weeks after
the second injection.
Longer treatment for up to 3 months can be
tried to maximize the intracavity portion of a
type II myoma prior to surgery.

Pre-procedural Preparation
2. Cervical preparation
Misoprostol – PGE1 analogue
200-400 mcg PO/PV, 12-24 hrs before surgery
Intracervical vasopressin
4 U in 80ml : use 10 ml to inject at 4:00, 8:00 of
the cervix at the time of hysteroscopy.
Significant reduction in force of cx. Dilation.
Decrease risk for absorption syndrome,
bleeding.

Cutting- using
electrosurgical loop
Vaporization-
electrosurgical vaporizer
ball
Morcellation –
Mechanical mincing
Hysteroscopic Myomectomy- TCRM
A 26 Fr resectoscope with working elements is
inserted :

Cutting electrodes resectoscope
Cutting loop utilizing a radiofrequency energy
which either Monopolar or bipolar energy.
Straight loop for fundus, angled one for wall.
Often leave surgeons battling tissue “chips.”
Thin strips of resected tissue, or chips, are
created and need to be periodically removed
from the uterine cavity to enhance visualization
using forceps or grasper.
Hysteroscopic Myomectomy- TCRM

Vaporizing electrodes resectoscope
Roller ball utilizing a radiofrequency energy
device.
Monopolar or bipolar energy.
Vaporizes the myoma so obviating the need for
frequent chip removal but precluding pathologic
examination of the specimen.
Hysteroscopic Myomectomy- TCRM

.
Morcellation • First generation-TRUCLEAR system.
• Second generation- MyoSure system (2009).
• Use a suction-based, mechanical energy,
rotating tubular cutter system rather than the
HF electrical energy.
• Faster and easier to learn.
• No chips in the uterine cavity.
• Chips are retrieved from suction and can be
sent for H/P.
Hysteroscopic Myomectomy- TCRM

Myosure Truclear

Comparison of Device Characteristics of TRUCLEAR™
Hysteroscopic Morcellator and MyoSure® Tissue Removal
System

The loop is first placed behind the fibroid to be
resected. The foot pedal is then used to
activate the energy and the loop is drawn back
into the resectoscope while shaving.
After initiating the current, the loop must be
kept moving while activated to prevent
extensive thermal necrosis with a subsequent
risk of perforation.
Technique of TCRM
A power setting of 60 W of pure cutting current
is often employed.

Technique of TCRM
The technique for removing a submucous
fibroid depends largely on its location and
protrution within the endometrial cavity.
The type 0
Option of first transecting the base of the stalk
or shaving the fibroid, removing it in pieces
through the cervix.
For larger fibroid, it is often symmetrically
shaved off with the resectoscope loop unitl the
base is reached.

The exposed base can then be
coagulated. The free floating fibroid can
be retrieved blindly with a polyp forceps or
grasped under visualization with the
optical tenaculum.
Technique of TCRM

Type 1 & 2
• The intracavitary portion of the fibroid is first
shaved to the level of the endometrium.
• Small myomas will often fall into the uterine
cavity after this initial unroofing, making their
removal easy.
• Larger myoma. After shaving till the level of
endometrium, with the effect of uteime muscle
contractility, the remainder of the fibroid may
protrude into the cavity permitting its safe
resection again.
Technique of TCRM

• The patient should be aware that more
than one surgical attempt may be
necessary for large myoma.




Technique of myoma
vaporization
For type 0: spring-tip electrode is used to
resect the base which then coagulated; the
free fibroid is then retrieved for HP exam.
For type 1,2: As the electrode is moved over
the protruding fibroid, instantaneous tissue
vaporization and desiccation flushing the
fibroid with the endometrium
Bipolar current of 130 W is used.

Postoperative follow-up
GnRH can be continued for 2-3 months if
myoma was not completely resected.
Intraoperative antibiotics.
Follow-up diagnostic
hysteroscopy is generally
performed 2-3 months after
surgery may show residual
myomas. Review HP result: the risk of liomyosarcoma is
low (<0.5%)

Complications of TCRM
Associated with a higher incidence of
complications
Difficult procedure, takes longer time
Perforation, bleeding, infections
Complications of distension media
Risk of synechia

Conclusion
Hysteroscopic myomectomy is a highly
effective and minimally invasive means of
treating symptomatic submucous leiomyomas.
Unfortunately, this treatment modality is
underutilized by today’s gynecologists.
This is likely due to inadequate exposure to
hysteroscopy during residency training as well
as the misconception that the skills necessary
to perform hysteroscopic procedures are
difficult to acquire.

Endometrial polyp
Localized endometrial hyperplasia:
single/multiple; sessile/ pedunculated
Causes:- AUB/ Infertility/ Endometritis
Diagnosis: USG/SIS/Hysteroscopy.


Hysteroscopic polypectomy
Several hysteroscopic systems to resect
endometrial polyps are currently available
Monopolar loop cautery
Bipolar systems
Microscissors or graspers,
Hysteroscopic morcellators
Of these, the monopolar loop is more
commonly available and of lower cost.

THANK YOU
THANK YOU