Embed Size (px)
Citation preview

Management Approach to Thyroid NoduleAmerican Thyroid Association Guideline, January, 2016
Dr. S G Mogni MowlaAsst. Professor of MedicineDhaka Medical CollegeDhaka, Bangladesh

2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer
Published in Thyroid. Volume: 26 Issue 1: January 12, 2016 2016 Jan;26(1):1-133.
Source

Thyroid nodules are common Prevalence of palpable thyroid nodules is
approximately 5% in women and 1% in menHigh-resolution ultrasound (US) can detect
thyroid nodules in 19–68% of randomly selected individuals
The clinical importance rests in excluding thyroid cancer, which occurs in 7–15%
By 2019, one study predicts that papillary thyroid cancer will become the third most common cancer in women at a cost of 19-21 billion dollars in the U.S.
Introduction

The aim of these guidelines is to inform clinicians, patients, researchers, and health policy makers on published evidence relating to the diagnosis and management of thyroid nodules and differentiated thyroid cancer.
We will focus on management approach of thyroid nodules only
Aims & Objectives

Thyroid nodule is a discrete lesion within the thyroid gland that is radiologically distinct from the surrounding parenchyma.
Some palpable lesions may not correspond to distinct radiologic abnormalities. They do not meet the strict definition for thyroid nodules.
Non-palpable nodules detected on US or other anatomic imaging studies are termed incidentally discovered nodules or “incidentalomas”
Nodules

Generally, only nodules >1 cm should be evaluated, since they have a greater potential to be clinically significant cancers.
Occasionally, there may be nodules <1 cm that require evaluation because ofsuspicious sonographic findings, associated lymphadenopathy, orother high-risk clinical factors such as
a history of childhood head and neck irradiation or
a history of thyroid cancer in one or more first degree relatives.
Nodules…

With the discovery of a thyroid nodule, a complete history and physical examination focusing on the thyroid gland and adjacent cervical lymph nodes should be performed.
Clinics

Pertinent historical factors predicting malignancy include:a history of childhood head and neck
irradiation, total body irradiation for bone marrow
transplantation exposure to ionizing radiation from fallout
in childhood or adolescence familial thyroid carcinoma, or thyroid
cancer syndrome in a first-degree relative, rapid nodule growth and/or hoarseness.
History

Pertinent physical findings suggesting possible malignancy includevocal cord paralysis, cervical lymphadenopathy, and fixation of the nodule to surrounding
tissues.
Examination

What is the appropriate laboratory and imaging evaluation for patients with clinically or incidentally discovered thyroid nodules?
Recommendations

A serum TSH levelIf the serum TSH is subnormal, a
radionuclide thyroid scan should be obtained If the serum TSH is normal or elevated, a
radionuclide scan should not be performed as the initial imaging evaluation
Ultrasound of neckThyroidal uptake on F18-flurodeoxyglucose
positron emission tomography (18FDG-PET) scan
FNAC
Investigations

A higher serum TSH level, even within the upper part of the reference range, is associated with increased risk of malignancy in a thyroid nodule, as well as more advanced stage thyroid cancer
If TSH low, risk of malignancy depends on radio uptake scan: Tracer uptake : hyperfunctioning “hot” nodule-
rarely harbor malignancy, no cytologic evaluation is necessary.
Tracer uptake is equal to the surrounding thyroid isofunctioning “warm” nodule
Uptake : nonfunctioning “cold”nodule
TSH & Scan

Thyroid sonography with survey of the cervical lymph nodes should be performed in all patients with known or suspected thyroid nodules.
Thyroid US can answer the following: Is there truly a nodule? How large is the nodule? What is the nodule’s pattern of ultrasound imaging
characteristics? Is suspicious cervical lymphadenopathy present? Is the nodule greater than 50% cystic? Is the nodule located posteriorly in the thyroid
gland?
Sonography

Sonography features that are associated with thyroid cancer include: microcalcifications, nodule hypoechogenicity compared with the
surrounding thyroid or strap muscles, irregular margins (defined as either infiltrative,
microlobulated or spiculated), and A shape taller than wide measured on a transverse
view. Features with the highest specificities (median
>90%) for thyroid cancer are microcalcifications, irregular margins, and tall shape,
Sonography

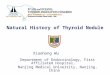
Fig: Sonographic Patterns & Risk of Malignancy

High suspicion [malignancy risk >70-90%]: Solid hypoechoic nodule or a solid hypoechoic component in a partially
cystic nodule with one or more of the following features: irregular margins (specifically defined as
infiltrative, microlobulated, or spiculated), microcalcifications, taller than wide shape, disrupted rim calcifications, or evidence of extrathyroidal extension
US-characteristics

Intermediate suspicion [malignancy risk 10-20%]: Hypoechoic solid nodule with asmooth regular margin, without -
microcalcifications, extrathyroidal extension, or taller than wide shape
US-Characteristics

Low suspicion [malignancy risk 5-10%]: Isoechoic or hyperechoic solid
nodule, orpartially cystic nodule with eccentric
uniformly solid areas without –
microcalcifications, Irregular margin extrathyroidal extension, or taller than wide shape
US-Characteristics

Very low suspicion [<3%]: Spongiform or partially cystic nodules
without any of the sonographic features described in the low, intermediate or high suspicion patterns have a low risk of malignancy (<3%).
US-Characteristics



Thyroid nodule diagnostic FNA is recommended for:
A) Nodules > 1cm in greatest dimension with high suspicion sonographic pattern
B) Nodules > 1 cm in greatest dimension with intermediate suspicion sonographic
C) Nodules > 1.5cm in greatest dimension with low suspicion sonographic pattern (Weak recommendation, Low-quality evidence)
FNAC

Thyroid nodule diagnostic FNA may be considered for:D) Nodules > 2cm in greatest dimension with very low suspicion sonographic pattern (e.g. – spongiform). Observation without FNA is also a reasonable option
Thyroid nodule diagnostic FNA is not required for:E) Nodules that do not meet the above criteria. F) Nodules that are purely cystic
FNAC

Thyroid nodule FNA cytology should be reported using diagnostic groups outlined in the:Bethesda System for Reporting Thyroid Cytopathology
FNAC: Interpretation

(i) nondiagnostic/unsatisfactory; (ii) benign; (iii) atypia of undetermined significance/
follicular lesion of undetermined significance (AUS/FLUS)
(iv) follicular neoplasm/suspicious for follicular neoplasm (FN), a category that also encompasses the diagnosis of Hürthle cell neoplasm/suspicious for Hürthle cell neoplasm;
(v) suspicious for malignancy (SUSP), and (vi) malignant.
Categories


Nondiagnostic cytologyA) FNA should be repeated with US guidance
and, if available, on-site cytologic evaluation B) Repeatedly nondiagnostic nodules without a
high suspicion sonographic pattern require close observation or surgical excision for histopathologic diagnosis
C) Surgery should be considered for histopathologic diagnosis if the cytologically nondiagnostic nodule has a high suspicion sonographic pattern, high growth rate or clinical risk factors for malignancy are present
Recommendations

Benign cytologyIf the nodule is benign on cytology, further immediate diagnostic studies or treatment are not required
Recommendations

AUS/FLUS CytologyIf repeat FNA cytology and/or molecular
testing are not performed or inconclusive, either surveillance or diagnostic surgical
excision may be performed for an AUS/FLUS thyroid nodule,
depending on clinical risk factors, sonographic pattern, and patient preference.

Follicular Neoplasm/Suspicious for Follicular Neoplasm (FN/SFN) CytologyIf molecular testing is either not performed or inconclusive, surgical excision may be considered for removal and definitive diagnosis of an FN/SFN thyroid nodule.

Suspicious for Malignancy (SUSP) CytologySurgical management should be similar to that of malignant cytology, depending on clinical risk factors, sonographic features, patient preferenceWhen surgery is considered for patients with a solitary, cytologically indeterminate nodule, thyroid lobectomy is the recommended initial surgical approach. This approach may be modified based on clinical or sonographic characteristics, patient preference

Malignant CytologyIf a cytology result is diagnostic for primary thyroid malignancy, surgery is generally recommended.
An alternative active surveillance management approach can be considered in:
A) patients with very low risk tumorsB) patients at high surgical risk because of co-
morbid conditions,C) patients expected to have a relatively short
remaining life span

A) 18FDG-PET imaging is not recommended for the evaluation of patients with newly detected thyroid nodules or thyroidal illness, the incidental detection of abnormal thyroid uptake may be encountered
B) Focal 18FDG-PET uptake within a sonographically confirmed thyroid nodule conveys an increased risk of thyroid cancer, and fine needle aspiration is recommended for those nodules > 1 cm.
C) Diffuse 18FDG-PET uptake, in conjunction with sonographic and clinical evidence of chronic lymphocytic thyroiditis, does not require further imaging or fine needle aspiration
18FDG-PET scan

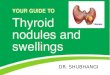
Algorithm for evaluation and management of patients with thyroid nodules

How should multinodular thyroid glands (i.e. 2 or more clinically relevant nodules) be evaluated for malignancy?

A) Patients with multiple thyroid nodules >1 cm should be evaluated in the same fashion as patients with a solitary nodule >1 cm, excepting that each nodule >1 cm carries an independent risk of malignancy and therefore multiple nodules may require FNA.
B) When multiple nodules >1 cm are present, those with a suspicious sonographic patern should be aspirated preferentially. FNA should be performed preferentially based upon nodule sonographic pattern and respective size cut-off.

A low or low-normal serum TSH concentration in patients with multiple nodules may suggest that some nodule(s) may be autonomous.
In such cases, a radionuclide thyroid scan should be considered and directly compared to the US images to determine functionality of each nodule >1 cm.
FNA should then be considered only for those isofunctioning or nonfunctioning nodules with high suspicion

What are the best methods for long-term follow-up of patients with thyroid nodules?

Recommendations for initial follow-up of nodules with benign FNA cytology

A) Nodules with high suspicion US pattern: repeat US and US-guided FNA within 12 months
B) Nodules with low to intermediate suspicion US pattern: repeat US at 12-24 months. If sonographic evidence of growth is rapid or development of new suspicious sonographic features, the FNA could be repeated or observation continued with repeat US

C. Nodules with very low suspicion US pattern (including spongiform nodules): the utility of surveillance is not known
D. If a nodule has undergone repeat US-guided FNA with a second benign cytology result, ultrasound surveillance for this nodule for continued risk of malignancy is no longer indicated

Follow-up for nodules that do not meet FNA criteria

A) Nodules with high suspicion US pattern: repeat US in 6-12 months
B) Nodules with sonographic features of low to intermediate suspicion US pattern: consider repeat US at 12-24 months.
C) Nodules > 1 cm with very low suspicion US pattern (including spongiform nodules) and pure cyst: risk not known. If US is repeated, it should be at > 24 months
D) Nodules < 1 cm with very low suspicion US pattern (including spongiform nodules) and pure cysts do not require routine sonographic follow-up

What is the role of medical or surgical therapy for benign thyroid nodules?

Routine TSH suppression therapy for benign thyroid nodules in iodine sufficient populations is not recommended. Though modest responses to therapy can be detected, the potential harm outweighs benefit for most patients.
Individual patients with benign, solid or mostly solid nodules should have adequate iodine intake. If inadequate, a daily supplement (containing 150 mcg iodine) is recommended.
Surgery may be considered for growing nodules that are benign after repeat FNA if they are large (>4 cm), causing compressive or structural symptoms, or based upon clinical concern.

Patients with growing nodules that are benign after FNA should be regularly monitored. Most asymptomatic nodules demonstrating modest growth should be followed without intervention.
Recurrent cystic thyroid nodules with benign cytology should be considered for surgical removal or percutaneous ethanol injection (PEI) based on compressive symptoms and cosmetic concerns. Asymptomatic cystic nodules may be followed conservatively
There are no data to guide recommendations on the use of thyroid hormone therapy in patients with growing nodules that are benign on cytology

How should thyroid nodules in pregnant women be managed?

FNA for thyroid nodules discovered during pregnancyA) FNA of clinically relevant thyroid nodules
(refer to section [A10]) should be performed in euthyroid and hypothyroid pregnant women
B) For women with suppressed serum TSH levels that persist beyond 16 weeks gestation, FNA may be deferred until after pregnancy and cessation of lactation. At that time, a radionuclide scan can be performed to evaluate nodule function if the serum TSH remains suppressed.

Approaches to pregnant patients with malignant or indeterminate cytologyA) PTC discovered by cytology in early pregnancy should
be monitored sonographically. B) If it grows substantially before 24-26 weeks gestation,
or if US reveals cervical lymph nodes that are suspicious for metastatic disease, surgery should be considered during pregnancy.
C) However, if the disease remains stable by mid-gestation,or if it is diagnosed in the second half of pregnancy, surgery may be deferred until delivery
D) In pregnant women with FNA that is suspicious for or diagnostic of PTC, thyroid hormone therapy to keep the serum TSH 0.1-1.0mU/L is recommended.

Thank You