Embed Size (px)
DESCRIPTION
Thyroid nodule. History Physical examination Euthyroid Hypothyroid Hyperthyroid Labs TSH (antibodies). Thyroid nodule. Imaging US Scan if TSH is low. Toxic adenoma. Thyroid nodule. Imaging US Scan if TSH is low CT usually precedes referral FNA US-guided. Thyroid nodule. - PowerPoint PPT Presentation
Citation preview

Thyroid nodule
History Physical examination
– Euthyroid– Hypothyroid– Hyperthyroid
Labs– TSH– (antibodies)

Thyroid nodule
Imaging– US– Scan if TSH is low

Toxic adenoma

Thyroid nodule
Imaging– US– Scan if TSH is low– CT usually precedes referral
FNA– US-guided

Thyroid nodule
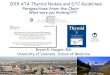
There are 3 ways to diagnose a thyroid nodule:
ultrasound guided FNAultrasound guided FNAultrasound guided FNA

Thyroid nodule
FNA result– Papillary carcinoma– Follicular LESION
Carcinoma Adenoma Adenomatous colloid nodule
– Insufficient for diagnosis

Management Guidelines for Patients withThyroid Nodules and Differentiated Thyroid Cancer
(Cooper, THYROID 2006;16:109-141(

Management Guidelines for Patients withThyroid Nodules and Differentiated Thyroid Cancer
(Cooper, THYROID 2006;16:109-141) FNA Results

Thyroid nodule
FNA result– Papillary carcinoma
–Follicular LESIONCarcinomaAdenomaAdenomatous colloid nodule
– Insufficient for diagnosis

Management Guidelines for Patients withThyroid Nodules and Differentiated Thyroid Cancer
(Cooper, THYROID 2006;16:109-141) FNA Results

Thyroid nodule
conservative approach for most patients with thyroid nodules that are
cytologically indeterminate on fine-needle aspiration and benign according to
gene-expression classifier results.
(Alexander, N Engl J Med. 2012;367:705-15)

Non-mailgnant indications for thyroidectomy
Goiter

Non-mailgnant indications for thyroidectomy
Goiter– Symptomatic

Non-mailgnant indications for thyroidectomy
Goiter– Symptomatic– Esthetic

Non-mailgnant indications for thyroidectomy
Goiter– Symptomatic– Esthetic
Hyperthyroidism

Before and after total thyroidectomy

THYROID CANCERS
CALSSIFICATION:

THYROID CANCERS
CALSSIFICATION:
DIFFERENTIATED THYROID CANCERS

THYROID CANCERS
CALSSIFICATION:
DIFFERENTIATED THYROID CANCERS
OTHER THYROID CANCERS

THYROID CANCERS
CALSSIFICATION:
DIFFERENTIATED THYROID CANCERS
Papillary

THYROID CANCERS
CALSSIFICATION:
DIFFERENTIATED THYROID CANCERS
Papillary Follicular

THYROID CANCERS
CALSSIFICATION:
DIFFERENTIATED THYROID CANCERS
Papillary Follicular
OTHER THYROID CANCERS

THYROID CANCERS
CALSSIFICATION:
DIFFERENTIATED THYROID CANCERS
Papillary Follicular
OTHER THYROID CANCERS Medullary

THYROID CANCERS
CALSSIFICATION:
DIFFERENTIATED THYROID CANCERS Papillary Follicular
OTHER THYROID CANCERS Medullary Anaplastic (?poorly differentiated
papillary carcinoma)

Differentiated thyroid cancer
Follicular Papillary
Age
Gender (Sex)Mode of SpreadMultifocality
Prognosis after surgery(20-y survival)

Differentiated thyroid cancer
Follicular Papillary
35-55 25-45 Age
Gender (Sex)Mode of SpreadMultifocality
Prognosis after surgery(20-y survival)

Differentiated thyroid cancer
Follicular Papillary
35-55 25-45 Age
F F Gender (Sex)Mode of SpreadMultifocality
Prognosis after surgery(20-y survival)

Differentiated thyroid cancer
Follicular Papillary
35-55 25-45 Age
F F Gender (Sex)
Blood borne Lymphatic Mode of SpreadMultifocality
Prognosis after surgery(20-y survival)

Differentiated thyroid cancer
Follicular Papillary
35-55 25-45 Age
F F Gender (Sex)
Blood borne Lymphatic Mode of Spread
No Yes Multifocality
Prognosis after surgery(20-y survival)

Differentiated thyroid cancer
Follicular Papillary
35-55 25-45 Age
F F Gender (Sex)
Blood borne Lymphatic Mode of Spread
No Yes Multifocality
Excellent Excellenter Prognosis after surgery(20-y survival)

Differentiated thyroid cancer
Staging – T1 - Tumor 2 cm or less in greatest dimension
limited to the thyroid.– T2 - Tumor more than 2 cm, but not more than 4
cm, in greatest dimension limited to the thyroid.– T3 - Tumor more than 4 cm in greatest dimension
limited to the thyroid.– T4a - Tumor of any size extending beyond the
thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve.
– T4b - Tumor invades prevertebral fascia or encases carotid artery or mediastinal vessels.

Differentiated thyroid cancer
Staging– N1a - Metastasis to Level VI (pretracheal,
paratracheal, and prelaryngeal/Delphian lymph nodes).
– N1b - Metastasis to unilateral, bilateral, or contralateral cervical or superior mediastinal lymph nodes.

Prognostic factors
A G E S
Age Sex (Gender) Extension Size

Prognosis (Lahey Clinic)
Age Metastasis Extension Size

Prognosis (Lahey Clinic)
Age Metastasis (NOT lymph node) Extension Size

Prognosis (Lahey Clinic)
Age Metastasis (NOT lymph node) Extension (to neighboring
structures) Size

Prognosis (Mayo Clinic)
MACIS Prognostic score Metastasis, Age, Completeness of resection,
vascular Invasion, Size.
M + 3 if Metastasis is found A = Age (y) x 0.08 C + 1 if resection is inComplete I + 1 if vascular invasion (pathologists
report) S 0.3 x largest diameter in centimeters
(Size)

Prognosis (MSKCC)
Even more complicated scoring Includes
– Tumor grade– Lymph node involvement– multifocality

Complications of thyroid surgery

Thyroid operations
Lobectomy ± isthmus Near total thyroidectomy Total thyroidectomy
– ± modified neck dissection for known involved lymph nodes

Operations for papillary carcinoma
Lobectomy (low risk)– Difficult to justify radical surgery for such a
good prognosis cancer
Total/near total thyroidectomy (high risk) – Treatment with radioactive iodine-131– Detection of distant metastases
Total thyroidectomy + modified neck dissection (known lymph node metastasis)

Extensive spread of papillary carcinoma

Operations for follicular carcinoma
Total thyroidectomy Near total thyroidectomy
– Treatment with radioactive iodine-131
– Detection of distant metastases

Adjuvant treatment
Scan for residual glandular tissue– I131 full body scan– Maximal TSH stimulation
Destruction of thyroid remnant– High dose I131 (Maximal TSH stimulation)
Treatment – High dose I131 (Maximal TSH stimulation)
Suppressive T4 for life
Follow up– Thyroglobulin (Tg) with maximal TSH stimulation– I131 full body scan as indicated by Tg
















![Approach to Thyroid Nodule[1]](https://img.pdfslide.net/doc/110x75/55286aea55034670588b47b5/approach-to-thyroid-nodule1.jpg)