-
8/14/2019 Chronic Lower Respiratory Tract Infections
1/32
CHRONIC LOWERCHRONIC LOWER
RESPIRATORY TRACTRESPIRATORY TRACT
INFECTIONSINFECTIONS
-
8/14/2019 Chronic Lower Respiratory Tract Infections
2/32
-
8/14/2019 Chronic Lower Respiratory Tract Infections
3/32
BRONCHIECTASISBRONCHIECTASIS
LUNG ABSCESSLUNG ABSCESS
-
8/14/2019 Chronic Lower Respiratory Tract Infections
4/32
BronchiectasisBronchiectasis
DefinitionDefinition
Dilation of bronchi.Dilation of bronchi.
EpidemiologyEpidemiology
Incidence low(
-
8/14/2019 Chronic Lower Respiratory Tract Infections
5/32
Bronchiectasis contd.Bronchiectasis contd.
PathogenesisPathogenesis
Exact process obscure. Most likelyExact process obscure. Most
likely
multifactorial, with the different factorsmultifactorial, with
the different factorstaking on different degrees of importance
intaking on different degrees of importance in
each patient.each patient.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
6/32
Bronchiectasis contd.Bronchiectasis contd.
Mechanistic TheoriesMechanistic Theories
There are 4:There are 4:
i) Pressure of secretion theoryi) Pressure of secretion
theory
ii) Atelectasis theoryii) Atelectasis theory
iii)Traction theoryiii)Traction theory
iv)Infection theoryiv)Infection theory
-
8/14/2019 Chronic Lower Respiratory Tract Infections
7/32
Pressure of secretion theoryPressure of secretion theory
Thick secretions obstruct, then mechanicallyThick secretions
obstruct, then mechanically
distend the airway and the dilation persistsdistend the airway
and the dilation persistseven after clearance of the
obstruction.even after clearance of the obstruction.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
8/32
Atelectasis theoryAtelectasis theory
Collapse of lung parenchyma leads toCollapse of lung parenchyma
leads to
increasingly negative intrapleural pressureincreasingly negative
intrapleural pressureand later dilation of the bronchus inand later
dilation of the bronchus in
question.question.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
9/32
Traction theoryTraction theory
Fibrosis and scarring from parenchymalFibrosis and scarring from
parenchymal
disease exert traction on the bronchial walls.disease exert
traction on the bronchial walls.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
10/32
Infection theoryInfection theory
Infection and the inflammatory responseInfection and the
inflammatory response
damage the supportive structures of thedamage the supportive
structures of thebronchial wall and subsequentbronchial wall and
subsequent
bronchiectasis.bronchiectasis.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
11/32
SummarySummary
Only the Infection Theory is supported by animal models ofOnly
the Infection Theory is supported by animal models ofthis disease.
Atelectasis and traction play minimal, if anythis disease.
Atelectasis and traction play minimal, if anyroles, in the
pathogenesis of bronchiectasis.roles, in the pathogenesis of
bronchiectasis.
Bronchial obstruction and poor drainage i.e. retention
ofBronchial obstruction and poor drainage i.e. retention
ofsecretions (from such cases as foreign bodies) along
withsecretions (from such cases as foreign bodies) along
withinfection appear to be the major factors in most
cases.infection appear to be the major factors in most cases.
Infection or obstruction occurring alone is unlikely to lead
toInfection or obstruction occurring alone is unlikely to lead
tothe more severe forms of bronchiectasis.the more severe forms of
bronchiectasis.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
12/32
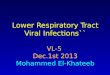
ClassificationClassification
a) Cylindrical bronchiectasis (Group I)a) Cylindrical
bronchiectasis (Group I)
Dilation regular, with the airway continuing to have aDilation
regular, with the airway continuing to have aregular
outline.regular outline.
b) Varicose bronchiectasis (Group II)b) Varicose bronchiectasis
(Group II)
Dilation irregular, with areas of dilation and
constriction.Dilation irregular, with areas of dilation and
constriction.
c) Saccular bronchiectasis (Group III)c) Saccular bronchiectasis
(Group III)
Dilation marked, with destruction of structural
componentsDilation marked, with destruction of structural
componentsof the airway wall.of the airway wall.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
13/32
-
8/14/2019 Chronic Lower Respiratory Tract Infections
14/32
AETIOLOGYAETIOLOGY
a) Infectiona) Infection
The most common:The most common:
i)Tuberculosisi)Tuberculosisii)Histoplasmosisii)Histoplasmosis
iii)Pertussis, measles(complicated by pneumonia)iii)Pertussis,
measles(complicated by pneumonia)
iv)Adenovirus (types 1,3,4,7, and 21) 20 to 64 per
centiv)Adenovirus (types 1,3,4,7, and 21) 20 to 64 per centdevelop
bronchiectasisdevelop bronchiectasis
v) Herpesvirusv) Herpesvirus
vi)vi)Aspergillus fumigatusAspergillus fumigatus
vii)vii) Mycoplasma pneumoniaeMycoplasma pneumoniae
-
8/14/2019 Chronic Lower Respiratory Tract Infections
15/32
b) Congenital and genetic disordersb) Congenital and genetic
disorders
i) Cystic fibrosisi) Cystic fibrosis
ii) Williams-Campbell syndromeii) Williams-Campbell syndrome
iii) Tracheobronchomegalyiii) Tracheobronchomegaly
iv) Marfan syndromeiv) Marfan syndrome
v)Alpha-1-antiproteinase deficiency[v)Alpha-1-antiproteinase
deficiency[-1--1-antitrypsin deficiency]antitrypsin deficiency]
vi) Congenital bronchiectasisvi) Congenital bronchiectasis
-
8/14/2019 Chronic Lower Respiratory Tract Infections
16/32
c) Ciliary Abnormalitiesc) Ciliary Abnormalities
i) Congenital : Kartagener syndrome [triad ofi) Congenital :
Kartagener syndrome [triad of
situs inversus,sinusitis & bronchiectasis].situs
inversus,sinusitis & bronchiectasis].There is an underlying
congenital abnormalThere is an underlying congenital abnormal
ciliary function.ciliary function.
ii)Acquired : occurs as a result of infection.ii)Acquired :
occurs as a result of infection.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
17/32
d) Immunodeficiencyd) Immunodeficiency
e) Foreign body aspiratione) Foreign body aspiration
g) Right middle lobe syndromeg) Right middle lobe syndrome
h) Asthmah) Asthma
i) Others:
-heroin intoxication-heroin intoxication
-intralobar pulmonary sequestration-intralobar pulmonary
sequestration-bronchogenic cyst-bronchogenic cyst
-chronic sinusitis-chronic sinusitis
-
8/14/2019 Chronic Lower Respiratory Tract Infections
18/32
-recurrent aspiration e.g. tracheo--recurrent aspiration e.g.
tracheo-
oesophageal fistula, cerebral palsyoesophageal fistula, cerebral
palsy
-inhaltion of noxious gases-inhaltion of noxious gases -racial
predilections-racial predilections
-
8/14/2019 Chronic Lower Respiratory Tract Infections
19/32
PresentationPresentation
Age: mainly preschool and early school ageAge: mainly preschool
and early school age
years.years. Symptoms: manifestations range fromSymptoms:
manifestations range from
chronic cough with early morning sputumchronic cough with early
morning sputum
production in an overtly healthy child toproduction in an
overtly healthy child torecurrent pneumonia with or
withoutrecurrent pneumonia with or without
haemoptysis in a chronically ill one.haemoptysis in a
chronically ill one.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
20/32
Chronic cough worse in the morning.Chronic cough worse in the
morning.
Purulent , foul smelling sputum. Halithosis.Purulent , foul
smelling sputum. Halithosis.
HaemoptysisHaemoptysis
Others: weight loss, intermittent fever,Others: weight loss,
intermittent fever,
wheezing, dyspnoea, chest pain.wheezing, dyspnoea, chest
pain.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
21/32
Clinical signsClinical signs
Harrisons sulciHarrisons sulci
Finger clubbingFinger clubbingCyanosisCyanosis
-
8/14/2019 Chronic Lower Respiratory Tract Infections
22/32
Dullness to percussion, crepitationsDullness to percussion,
crepitations
(crackles), rhonchi, decreased air entry,(crackles), rhonchi,
decreased air entry,
bronchial breath sounds- usually localizedbronchial breath
sounds- usually localized
over the bronchiectatic area when saccularover the
bronchiectatic area when saccular
changes are present except in diffusechanges are present except
in diffuse
disease.disease.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
23/32
DiagnosisDiagnosis
CXray findings not diagnostic but can beCXray findings not
diagnostic but can be
suggestivesuggestive In mild cases: segmental accentuation,
lossIn mild cases: segmental accentuation, loss
of definition of lung markings.of definition of lung
markings.
In severe cases: honeycomb pattern ofIn severe cases: honeycomb
pattern ofcystic changes.cystic changes.
-
8/14/2019 Chronic Lower Respiratory Tract Infections
24/32
BronchographyBronchography
Flexible fibreoptic bronchoscopyFlexible fibreoptic
bronchoscopy
CT ScanCT Scan Magnetic resonance imagingMagnetic resonance
imaging
Lung scintigraphyLung scintigraphy
-
8/14/2019 Chronic Lower Respiratory Tract Infections
25/32
Differential diagnosesDifferential diagnoses
All underlying causesAll underlying causes
-
8/14/2019 Chronic Lower Respiratory Tract Infections
26/32
Evaluation of patients withEvaluation of patients with
bronchiectasisbronchiectasis
Identify cause and predisposing factorsIdentify cause and
predisposing factors
Infection:Infection: Sputum or BALF for M/C/SSputum or BALF for
M/C/S
Mycobacterial/fungal culturesMycobacterial/fungal culturesViral
cultureViral culture
Skin tests (PPD, fungal)Skin tests (PPD, fungal)
Serological studiesSerological studies
-
8/14/2019 Chronic Lower Respiratory Tract Infections
27/32
ImmunodeficiencyImmunodeficiency
FBCFBC
Quantitative immunoglobulinsQuantitative immunoglobulins
IgG subclassesIgG subclasses
WBC function (nitroblue tetrazolium dyeWBC function (nitroblue
tetrazolium dyetest, chemotactictest, chemotactic
assays,assays,
etc.)etc.)
Total haemolytic complementTotal haemolytic complement
-
8/14/2019 Chronic Lower Respiratory Tract Infections
28/32
AspirationAspiration
Barium swallowBarium swallow
Extended oesophageal pH monitoringExtended oesophageal pH
monitoring
-
8/14/2019 Chronic Lower Respiratory Tract Infections
29/32
Ciliary dysfunctionCiliary dysfunction
Nasal/tracheal epithelium: light and electronNasal/tracheal
epithelium: light and electron
microscopymicroscopy
Cystic fibrosisCystic fibrosis
Sweat testSweat test
-
8/14/2019 Chronic Lower Respiratory Tract Infections
30/32
ComplicationsComplications
Brain and lung abscessBrain and lung abscess
Empyema & pyopneumothoraxEmpyema & pyopneumothorax
Bronchopleural fistulaBronchopleural fistula
Severe atypical pneumoniaSevere atypical pneumonia
HaemoptysisHaemoptysis
AmyloidisisAmyloidisis
Cor pulmonale in advanced diseaseCor pulmonale in advanced
disease
-
8/14/2019 Chronic Lower Respiratory Tract Infections
31/32
TreatmentTreatment
MedicalMedical
Chest physiotherapyChest physiotherapy
AntibioticsAntibiotics BronchodilatorBronchodilator
Good nutritionGood nutrition
Bronchoscopy: to remove foreign body orBronchoscopy: to remove
foreign body orthick secretionthick secretion
-
8/14/2019 Chronic Lower Respiratory Tract Infections
32/32
Treatment (contd.)Treatment (contd.)
SurgicalSurgical
Failure of medical treatment, if disease isFailure of medical
treatment, if disease is
localizedlocalized
PrognosisPrognosis
Depends on causative factorsDepends on causative factors