-
8/19/2019 Infancy and Childhood - D. Padla
1/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
1 o
Pathology 3.6
Diseases of Infancy and ChildhoodDr. Padla
October 1, 2013
UTLINE
Causes of death related with age
Congenital anomalies
. Disorders of prematurity
.
Perinatal infections
Fetal Hydrops
.
Inborn Errors of Metabolism and other Genetic Disorders
I.
SIDS
II. Tumors
I.CAUSE OF DEATH RELATED WITH AGE
ble 1. Most Common Causes of Death in US
Under 1 year (Infancy) Rate /100,000
1. Congenital malformations, deformations,
chromosomal abnormalities
685.2
2. Disorders related to short gestation & low
birth weight
3. Sudden infant death syndrome
4. Newborns affected by maternal
complications of pregnancy
5.
Respiratory distress of newborn6. Accidents (unintentional
injuries)
7.
Bacterial sepsis of newborn
8.
Intrauterine hypoxia and birth asphyxia
9. Diseases of the circulatory system
Under 1-4 year
29.9
1. Accidents and adverse effects
2. Congenital malformations, deformations,
chromosomal abnormalities
3.
Malignant neoplasms
4.
Homicide and legal intervention
5. Diseases of the heart
6.
Influenza and pneumonia
Under 5-14 year
16.8
1. Accidents and adverse effects
2. Malignant neoplasms
3.
Homicide and legal intervention
4.
Congenital malformations, deformations,
chromosomal abnormalities
5. Suicide
6. Diseases of the heart
Under 15-24 year
80.1
1. Accidents and adverse effects
2. Homicide
3.
Suicide4. Congenital malformations, deformations,
chromosomal abnormalities
5.
Malignant neoplasms
6.
Diseases of the heart
Source: (Minimo et al. National Vital Statistics 55:19,2007)
ote: Accidents and adverse effects are not so much common
in infancy
t it becomes the most common cause of death in the succeeding
age
oups.
II.CONGENITAL ANOMALIES
Congenital anomalies are morphologic defects that are present
at
Malformations
o Disorder of morphogenesis that are intrinsic to the
infant/fe
o It is “within” the fetus (Genetically
determined)
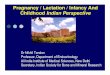
Figure 1.(L) syndactyly; (R) polydactyly
Syndactyly : two or more digits are fused together .
Polydactyly : prese
supernumerary digits on hand
Disruptions
o Results from secondary destruction of an organ or
body
that was previously normal in development.
o Arise from an extrinsic disturbance in
morphogenesis
Figure 2. Disruption of morphogenesis by amniotic band
Note: Disruption and deformation are extrinsic to the
fetus
Deformations
o
Localized or generalized compression of the growing fetabnormal
biochemical factors
o Maternal
includes pregnancy, small uterus, malformed uterus
leiomyomas.
o Fetal (placental)
multiple fetuses and abnormal placental presentation
Figure 3. Malformation brought by homeobox gene.
Left: Cleft palate. Right: Cyclops eye
Sequence
o Effects of initial pathology; follows previous defec
development(e.g. oligohydramnios)
o Cascade of anomalies triggered by one initiating
aberration.
o Manifestations are related to each other
o “Domino effect”
-
8/19/2019 Infancy and Childhood - D. Padla
2/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
2 of
PATHOLOGY 3.6
Figure 4. Oligohydramnios due to a very small amount
of amniotic fluid
It is characterized by inward and downward turning of the
foot(Talipesequinovarus) and a flattened brain. This is termed as
Potter sequence or
Oligohydramnios sequence. Note flattened facial features and
deformed
right foot
Figure 5. Pathogenesis of oligohydramnios
The causes of hydramnios are Amniotic leak, Renal Agenesis (Baby
doesn’t
ave kidneys) and others. In renal agenesis, baby has no kidneys,
therefore
the fetus doesn’t produce urine. The urine of the fetus
contributes to the
amniotic fluid inside the uterus that is why renal agenesis can
be a factor
causing oligohydramnios.
Syndrome: involvement of many organ that are not related
sequentially (Rubella syndrome: congenital heart disease,
cataract,
mental retardation).
o Manifestations are unrelated to each other
Agenesis: absence of primordium (organ) usually due to infection
and
environmental factor during organogenesis
Aplasia: primordium(organ) that fails to develop
Atresia: absence of an opening usually of a hollow visceral
organ
Hypoplasia/Hyperplasia: lesser/greater number of cell
Hypotrophy/Hypertrophy: lesser/greater size of cell
Dysplasia: there is increase in the number of cells but
the structural
arrangement do not follow the normal configuration.
Examples are
adenoma of the liver, cyst of the kidney, hemangioma, fibroma
and
terratoma. Disorganization of cell that causes congenital
anomaly
ble 2. Causes of Congenital Anomalies. Chromosomal
aberration and
endelian inheritance is an example of congenital malformation.
GENETIC Frequency (%)
Chromosomal aberrations 10-15
Mendelian inheritance 2-10
ENVIRONMENTAL
2-3
Maternal/placental Infections
(rubella, toxoplasmosis, syphilis, CMV, Herpes*)
Maternal Disease States
(diabetes, phenylketonuria, endocrinopathies)
6-8
Drugs and Chemicals
(alcohol, folic acid antagonists, androgens,
phenytoin, thalidomide, warfarinj, 13-cis-retinoic
acid, etc)
1
Irradiations 1
MULTIFACTORIAL 20-25
UNKNOWN 40-60
Note: Thalidomide – drug used to treat anxiety
disorders as tranqu
They were given to pregnant mothers decades ago. It is found
teratogenic that is why we do not give this to pregnant mothers
now
Babies who were born to mothers who were taking this drug
phocomelia (loss of extremeties). This occurs because of
the disrup
the signaling pathway of developmental genes (Wingless Sig
Pathway). It is also given as an anti-neoplastic drug.
Pathogenesis of Congenital Anomalies
Timing o Early embryonic period
1st
3 weeks after fertilization: Injurious agent damages
enough cells to cause death and abortion or only few
presumably allowing the embryo to recover.
There will be no congenital anomaly but abortio
happen. If the fetus survives, since it is still too ear
fetus can progress to develop completely.
3rd
week- 9th
week: embryo is extremely suscepti
teratogenesis. During this period, organs are being c
out of the germ cell layers.
o Fetal Period
Futher growth and maturation of the organs
Critical period: Reduced susceptibility to teratogens
but
fetus is susceptible to growth retardation and injuryComplex
interplay
o Environment and genetic make-up
III.DISORDERS OF PREMATURITY
A. Causes of Prematurity and Fetal growth restriction
Premature birth – occurs when the baby is
delivered early than t
term age of 9 months or 37 to 42 weeks
PROM – Premature Rupture of Membrane
o Occurs when the bag of water ruptures after 37 wee
gestation but before 42 weeks
o What happens during PROM?
Amniotic sac contains amniotic fluid where baby floats insid
uterus. Normally, during the full term, when the mother g
labor, the bag of water spontaneously ruptures during labo
the baby comes out. During PROM, the bag of water ru
without labor or contraction of the uterus. This is very
dang
before it will predispose to ascending infection and can
compression of the fetus. The most concern is infection.
o PPROM- Preterm Premature Rupture of Membrane
Occurs when the bag of water ruptures before the 37
of gestation.
This will also lead to ascending infection
Fetal Growth Restrictions
o There are various causes why the baby will be smaller
than n
o Causes can be fetal, placental and maternal. May
include:
Lack of proper nutrition- a complex cause of sma
gestational age-fetus.
Maternal smoking
Inability of the placenta to provide sufficient bloo
nutrient
Fetus can also be larger than normal such as in cases
when the m
has diabetes.
B. Neonatal Respiratory Distress Syndrome
Characterized by prematurity of the lungs
Also called Hyaline Membrane Disease
The Alveolar Type 2 pneumocytes are immature and are not
pro
surfactant needed to reduce surface tension of lung fluid. W
surfactant, the lung collapses, causing distress.
-
8/19/2019 Infancy and Childhood - D. Padla
3/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
3 of
PATHOLOGY 3.6
Classical manifestation of the disease:
o A Premature infant manifests with distress immediately
after birth.
The APGAR score, which describes how live or sick the baby is,
is
very low. The baby requires resuscitation and initially
responds,
but returns to distress after a while. The lungs become
collapsed
and atelectiatic, solid instead of spongy.
o This usually happens for three days. If the baby
survives the critical
3-day period, the pneumocytes will recover and be able to
produce surfactant. If the baby does not survive, the autopsy
will
show collapsed lung with hyaline membrane. This is why
NeonatalRespiratory Distress Syndrome is also called Hyaline
Membrane
Disease.
Other causes of respiratory distress in newborn:
a) Excessive sedation of the mother
b) Fetal head injury during the delivery
c) Aspiration of blood of amniotic fluid
d) Intrauterine hypoxia
Figure 6. Pathophysiology of RDS.
his shows how the hyaline membrane develops in the respiratory
passages,
alveolar ducts and alveolar sacs.
Figure 7. Hyaline Membrane Disease.
This shows atelectiasis and dilation in the alveoli. The
alveolar sacs
sappear and are replaced by cells. The hyaline membrane lines
the alveolar
sacs. Those alveolar sacs which remain are hyperinflated or
overdilated
(compensatory emphysema) because the baby is struggling to
inhale.
ecause of the hyaline membrane, there is still no exchange of
CO2 and O2.
the baby survives the critical 3-day period, the hyaline resorbs
and normal
reathing ensues. There are also other forms of management such
as giving
of surfactant or oxygen therapy.
C. Necrotizing Enterocolitis
o The premature baby is given enteral feeding (tube
feeding) in
bacteria or infection is introduced.
Figure 8. Necrotizing enterocolitis
Manifestations of the infection:
o Presence of blebs or air sacs within the mucosa of the
intest
o On Xray, it has a characterized appearance called
Pneum
Intestinalis.
o Increase in the chemical mediators of inflammation
parti
Platelet Activating Factor (PAF). The PAF increases permeab
the tight junctions between the epithelial cells, leading to
en
bacteria and possible progression to gangrene.
IV. PERINATAL INFECTIONS
Figure 6. Transplacental/Hematologic Spread of Infection
Two(2) ways by which the root of infection may infect the
fetus
perinatal infections:
1.
Transplacental (hematologic)
o The infection crosses the placental barrier from the
mother
fetus.
o The infecting agent (e.g., bacteria, virus) enters
throug
chorionic vili to the fetus.
o PATHWAY of INFECTION:
The mother has infectionThe maternal blood ente
placenta through openings in the endometrium of the
surrounding the fetus At the placental implantation
endometrium, the maternal blood enters the placenta
The fetal blood also enters the placenta and circulates a
the chorionic vili. (Note: Chorionic villi are blood capil
vessels of the fetus in the placenta. They are us
pathologists as histologic markers of placental tissue
cases such as abortion.)
The mother’s blood is also inside the placenta, aroun
chorionic vili. So, the exchange of gas and nutrient ha
between the maternal blood circulating the placenta a
chorionic vili which contains the fetal blood. (Note tha
is no direct between fetal and maternal circulation.)
In summary:
MotherPlacentaChorionic ViliUmbilicusB
-
8/19/2019 Infancy and Childhood - D. Padla
4/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
4 of
PATHOLOGY 3.6
Transcervical (Ascending)
o PATHWAY of INFECTION
The infection goes through the cervix and then ultimately
to
the amniotic sac The amniotic sac becomes infected,
creating amnionitis The infection contaminates the
amniotic fluid The baby inhales the infection into the
lungs
TYPES OF SEPSIS BASED ON ONSET OF DISEASE
o Early Onset – When the baby manifests the
disease within 7 days
of life
Group B Streptococcus is the most common infective
agent
causing meningitis, pneumonia and sepsis
o Late Onset – When the baby manifest the
disease after 7 days of
life
Listeria and Monilla fungal infections are more
common
Characterized by long latent period
V. FETAL HYDROPS
Fetal hydrops refers to the accumulation of edema fluid in the
fetus
during intrauterine growth.
NON IMMUNE HYDROPS (Parvovirus B19)
o Suprresion of RBC proliferation Anemia
Compensatory
increase in rate of pumping by heart Increase blood
volume
Increase Hydrostatic pressure Edema Fetal
Hydrops
Figure 7. Bone marrow from infant with parvovirus
B19. e (arrows) indicate 2 large erythroid precursors with
large nucleus, due to
viral intranuclear inclusions, and a peripheral rim of residual
chromatin.
IMMUNE HYDROPS
o Destruction of RBC
o Hemolytic disease caused by blood group incompatibility
between
mother and fetus.
o For example: Rh incompatibility (Mother: Rh- and Fetus:
Rh+)
Mother is sensitized by fetal Rh+ antigen during 1st
pregnancy
producing IgM Antibodies that does not pass placental
barrier.
Hence, no hemolytic destruction of RBC.
During 2nd
pregnancy, re-exposure to same antigen produces
IgG Antibodies that cross placental barrier, causing
hemolytic
destruction of fetal RBC. o 2 Mechanisms:
1. Anemia: Direct result of red cell loss.
Hemolytic Anemia Compensatory increase in rate of
pumping by heart Increase blood volume Increase
Hydrostatic pressureEdema Fetal Hydrops
2. Jaundice: Develops because hemolysis produces
unconjugated bilirubin.
Can produce Kernicterus if bilirubin passes
blood-brain
barrier Hypoalbuminemia Decrease in Oncotic
pressure Extravasation of fluid Edema Fetal
Hydrops
Figure 8. Pathogenesis of immune hydrops fetalis
Note: On the subsequent pregnancy, the IgG crosses the placenta
atta
to the Rh+ erythrocyte causing hemolysis. Unconjugate bilirubin,
whi
lypophilic, crosses the blood brain barrier and causes
kernicterus causin
manifestation.
Figure 9. (A) hydrops fetalis (B) cystic
hygroma – fluid
accumulation is particularly prominent in the soft tissues of
the neck,
because of non-development of lymphatic channels.
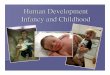
Figure 10. Kernicterus.
This is the a picture of midbrain that controls the vegetative,
respirato
cardiocvascular function. Destruction of this region will lead
to fet
consequences in the baby
Figure 11. Islands of extramedullary hematopoeisis. Liver.
This is due to the compensation to restore the normal amount of
bloo
to hemolysis.
-
8/19/2019 Infancy and Childhood - D. Padla
5/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
5 of
PATHOLOGY 3.6
ble 3. Immune Hydrops and Non-immune hydrops
Reason CharacteristicHematopoeitic
Response
Immune
Hydrops
Rh Incompatibility Destruction of RBC Bone Marrow
Hypercellularity/
Hyperplasia
With Extramedullary
hematopoesis
Non-
Immune
Hydrops
Parvovirus B19 Suppression of RBC
proliferation
Bone Marrow
Aplasia/ Hypoplasia
Without Extramedullary
hematopoeisis
VI.INBORN ERRORS OF METABOLISM AND OTHER GENETIC DIISORDERS
Phenylketonuria: Abnormalities of phenylalanine
metabolism
o Phenylalanine hydroxylase deficient (nausea, vomiting,
mental
retardation) – error in metabolizing phenylalanine
protein leading
to its accumulation in the system. Metabolites are produced
from
this which causes symptoms such as mental retardation (due
to
metabolic derangement)
o Phenyl acetic acid accumulation –
excreted in urine and sweat
which gives the infant a mousy odor which is distributed
throughout the body
o
Screening fos this condition is important – early
diagnosis canprevent the occurrence and further complications of
the disease
by not giving phenyalanine rich food to the baby
Figure 12. Phenylalanine hydroxylase system
Galactosemia: autosomal recessive disorder of galactose
metabolism.
o Most common and severe: Reaction 2 will not take
place
o Lacks the enzyme that digest galactose present in
themilk leading
to Galactose 1- phosphate accumulation
o Manifestations:
Mental retardation (brain) - yhis is due to the accumulation
of
the metabolites produced
Cataract (eye)
Hepatomegaly (liver)
o Don’t give galactose in the diet in the first 2 years of
life.
o Milk of the mother contains lactose that will be broken
down by
lactase to become galactose and lactose which will worsen
the
manisfestation. Thus other sources of nutrition should be
considered, at least in the first two years.
Figure 13. Pathway of galactose metabolism
Figure 14. Galactosemia in liver causing fibrosis and fatty
change th
causing hepatomegaly.
Cystic Fibrosis (Mucoviscidosis): Disorder of ion
transport in epi
cells that affects fluid secretion in exocrine glands and the
ep
lining of the respiratory, gastrointestinal, and reproductive
tracts;
o Cystic Fibrosis Gene regulates the chloride and
other ion
pass through the ion channel. It is not so much important
metabolic reaction during brain development thus, it doe
cause mental retardation.
o Caucasian> African Americans, Asians, Hispanics
Figure 15. Chloride channel defect in sweat duct.
This is responsible for the salty taste of the baby.
o Cystic fibrosis associated gene: Normal Structure
The primary defect in cystic fibrosis results from
abnormal function of an epithelial chloride channel p
ecroded by the cystic fibrosis transmembrane condu
regulator (CFTR) gene on chromosome 7q31.2
o CFTR regulates multiple additional ion channels and
c
processes. Interaction of CFTR with epithelial sodium ch
(ENaC) has possibly the most pathophysiologic relevance
infibrosis. ENaC is responsible for sodium uptake from the lu
fluid rendering it hypotonic.
o In cystic fibrosis, ENaC activity increases markedly
augm
sodium uptake across the apical membrane. In human sweat
ENaC activity decreases therefore a hypertonic lumina
containing high sweat chloride and high sodium content is f
(salty sweat).
o Functions of CFTR are tissue specific therefore
mutations ar
tissue specific.
o Respiratory and intestinal epithelium
CFTR is an avenue for active luminal excretion of chlorid
mutations result in loss or reduction of chloride secretio
the lumen.
-
8/19/2019 Infancy and Childhood - D. Padla
6/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
6 of
PATHOLOGY 3.6
increase passive water reabsorption from the lumen,
lowering the water content of the surface fluid layer
coating
mucosal cells.
In the lungs, dehydration leads to defective
mucociliary
action and the accumulation of hyperconcentrated, viscid
secretions.
o Gene: CFTR
Class I – Defective protein synthesis
complete lack of CFTR protein
Class II - Abnormal protein folding, processing, trafficking
defective processing of the protein from the
endoplasmic reticulum to the Golgi apparatus.
Does not become fully folded and glycosylated
Class III - Defective regulation
prevent activation of CFTR by preventing ATP binding
and hydrolysis
Class IV – Decreased conductance
reduced function of CFTR
Class V - Reduced abundance
reduced amount of normal protein
Class VI – Altered regulation of separate ion
channels
affect regulatory role of CFTR
Figure 16. Clinical manifestations of mutations in CFTR
gene.
Two severe mutations are associated with the classic cystic
fibrosis
phenotype while the presence of a mild mutation on one or
both alleles
results in a less severe type.
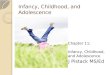
Figure 17. CF changes in pancreas.
Hyperconcentrated fluid will cause the obstruction of the duct
causing
latation of exocrine glands (digestive glands) which contains
acids that are
orrosive. The acid will extravasate in the surrounding gland
causing fibrosis.
This will result to the fibrous thickening in the interspaces of
the dilated
glands. This will result in digestive enzyme insufficiency,
malnutrion,
malabsortion, and hypovitaminosis.
Figure 18. Lungs
The chloride channel and some other electrolyte will lead to the
dehyd
of the lungs thus will increase the lungs susceptibility to
infection
Clinical features of cystic fibrosis.
1. Chronic sinopulmonary disease manifested by
2. Gastrointestinal and nutritional abnormalities,
including
3.
Salt-loss syndromes: acute salt depletion, chronic metabolic
acido
4. Male urogenital abnormalities resulting in obstructive
azoosp
(congenital bilateral absence of vas deferens)
Criteria for diagnosis of cystic fibrosis
One or more characteristic features,o OR, a history of
cystic fibrosis in sibling
o OR, a positive newborn screening test result
AND
An increased sweat chloride concentration on 2 or more
occasion
o or, identification of 2 cf mutations
o or, demonstration of abnormal epithelial nasal ion
transport
Abnormalities suggesting inborn errors of metabolism
GENERAL
o dysmorphic features, deafness, self-mutilation,
abnorma
abnormal body and urine odor, hepatosplenom
cardiomegaly, hydrops
NEUROLOGIC
o
hypotonia or hypertonia, coma, persistent lethargy,
seizuresGASTROINTESTINAL
o poor feeding, recurrent vomiting, jaundice
EYES
o cataract, cherry red macula, dislocated lens,
glaucoma
MUSCLE, JOINTS
o myopathy, abnormnal motility
VII.SUDDEN INFANT DEATH SYNDROME (SIDS)
This is a phenomenon which is known as the killer in the young
in
Autopsy (no clear cause of death)
usually dies while asleep, mostly in the prone or side
position
death or cot death)
Diagnosis of exclusion – you should examine the scene
of death
baby to rule out the possibility of child abuse or no harm was
in
on the baby
Epidemiology
o It is the leading cause of death between age 1 month and
1 y
the USA
o third leading cause of death overall in infancy
o 90% of deaths occur during first 6 months of life
(specifically
mos.)
o Prolonged apnea, marked change in color or muscle
ton
choking or gagging are considered risk factors.
Morphology
o Multiple petechiae on the thymus, visceral and parietal
pleu
epicardium are common
-
8/19/2019 Infancy and Childhood - D. Padla
7/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
7 of
PATHOLOGY 3.6
o Recent infection in the upper respiratory tract
o astrogliosis of the brain stem and cerebellum
o hypoplasia of the arcuate nucleus
Pathogenesis
o Vulnerable infant
delayed development of “arousal” and
cardiorespiratory
control
o Maternal Risk factors
born before term or low birth weight
o
Environment
side sleeping positions, sleeping on sofa surfaces and
thermal
stress
f the cause of death is not clear then it is known as
unclassified infant
ath syndrome and not a condition of sudden infant death
syndrome
SK FACTORS ASSOCIATED WITH SIDS
PARENTAL
o Young maternal age (
-
8/19/2019 Infancy and Childhood - D. Padla
8/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
8 of
PATHOLOGY 3.6
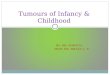
Staging
o Stage 1: Localized tumor with complete gross
excision, with or
without microscopic residual disease
o Stage 2A: Localized tumor with incomplete gross
resection.
Representative ipsilateral nonadherent lymph nodes negative
for
tumor microscopically.
o Stage 2B: Localized tumor with or without complete
gross
excision, ipsilateral nonadherent lymph nodes positive for
tumor.
Enlarged contralateral lymph nodes, which are negative for
tumor
microscopically.o Stage 3: Unresectable unilateral tumor
infiltrating across the
midline with or without regional lymph node involvement; or
localized unilateral tumor with contralateral regional lymph
node
involvement.
o Stage 4: Any primary tumor with dissemination to distant
lymph
nodes, bone, bone marrow, liver, skin, and/or other organs
(except
as defined for stage 4S).
o Stage 4S ("S" = special): Localized primary tumor (as
defined for
Stages 1, 2A, or 2B) with dissemination limited to skin,
liver,
and/or bone marrow; Stage 4S is limited to infants
-
8/19/2019 Infancy and Childhood - D. Padla
9/9
oup # 6 | Manalo, Mangila, Maniego, Manlulu, Maralit Page
9 of
PATHOLOGY 3.6
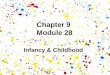
B. WILM’S TUMOR
Pathogenesis & Genetics
o WT1 encodes a DNA-binding transcription factor that is
expressed
within several tissues during embryogenesis. It is critical
for
normal renal and gonadal development
o Children with Beckwith-Wiedemann syndrome
characterized by enlargement of body organs,
macroglossia,
hemihypertrophy, omphalocele, and abnormal large cells in
the adrenal cortex.
Morphologyo Nephrogenic rests- are putative precursor
lesions of Wilms tumors
and seen in the renal parenchyma.
Figure 25. Wilm’s tumor; gross
Clinical Features
o large abdominal mass that may be unilateral or may
extend across
the midline and down into the pelvis.
o Hematuria, abdominal pain
o Anaplastic histology remains a critical determinant of
adverse
prognosis
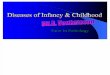
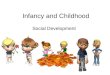
Figure 26. Triphasic Histology of Wilm’s tumor
hase 1: Small blue rounded cells/blastimal cells, Phase 2:
Epithelial cell that
leads to abortive tubules, Phase 3: spindle shaped mesenchymal
cells
…Because your SMILE is my LIFE
Edited by: Rei Israel Manlulu
When God places a burden upon you,
He places His arms underneath you.
“Come to me, all you who are weary and burdened, and I will
give
you rest. Take my yoke upon you and learn from me, for I am
gentle and humble in heart, and you will find rest for your
souls.
For My yoke is easy and My burden is light.”
(Matthew 11:28-30)