1. Sequelae1.1. TympanosclerosisTympanosclerosis is thought to
be a complication of otitis media in which hyalin and calcium
deposits accumulate within the tympanic membrane and the submucosa
middle ear. It often occurs as a result of inflammation or trauma
and is therefore commonly seen after recurrent episodes of AOM and
OME and after ventilation tube insertion. In most patients, these
plaques are clinically insignificant and cause little or no hearing
impairment.Tympanosclerotic plaques within the tympanic membrane
appear as a semicircular crescent or horseshoe-shaped white plaque
within the tympanic membrane.If the process is limited to the
tympanic membrane (ie, myringosclerosis), then hearing is usually
unaffected. However, if the middle ear is involved, then the
ossicular chain can become immobilized, resulting in a conductive
hearing loss. Attempts at surgical correction by Tympanoplasty and
ossicular reconstruction can be performed in ears with
tympanosclerosis1.2. AtelectasisAtelectasis is thought to result
mainly from long-standing eustachian tube dysfunction. One of the
main functions of the eustachian tube is ventilation. Opening of
the eustachian tube allows exchanging of gases and equalization
between the environment and middle ear. If the atelectasis
develops, the tympanic membrane becomes retracted. Tympanic
membrane comprises two parts, thepars tensa, which is the main part
of the eardrum, and thepars flaccida, which is a smaller part of
the eardrum located above the pars tensa. Either or both of these
parts may become retracted. The retracted segment of eardrum is
often known as a retraction pocket. In atelectatic ears, the middle
ear space is partially or completely obliterated, but the
Retraction of the tympanic membrane may lead to erosion of the long
process of the incus and the stapes structure.The management of
atelectasis is controversial. If eustachian tube function is still
considered to be present, the insertion of ventilation tubes could
potentially reverse the changes in the tympanic membrane by
normalizing the pressure in the middle ear space. If no improvement
is observed and the location of the retraction raises the concern
of subsequent cholesteatoma formation, then excision and grafting
of the affected portion of the tympanic membrane are recommended.
The recurrence of tympanic membrane retraction after this procedure
is not uncommon; therefore, prolonged observation is advised.
2. Intratemporal complications2.1. MastoiditisMastoiditis is an
inflammation or infection of the mastoid bone, which is a portion
of the temporal bone. Inflammation in the mastoid itself is quite
rare. It is almost always a result of inflammation or infection in
the middle ear space. Since there is a direct communication between
the mastoid and the middle ear space, any inflammatory process
occurring in the middle ear space is directly transmitted into the
mastoid. Infection can spread into the lateral sinus, causing an
infected clot to form within it (lateral sinus thrombosis). The
infection can also extend directly inferiorly, presenting as an
abscess deep to a muscle that is attached to the mastoid
(sternocleidomastoid muscle). These abscesses are termed Bezolds
abscesses. Acute mastoiditis was also associated with high
incidence of meningitis, which is an extension of the bacterial
infection from the mastoid into the lining surrounding the brain.
Untreated meningitis has a very high mortality rate; and those
individuals who do survive are often left with significant
neurologic dysfunction. Lastly, acute mastoid infections can also
create a cerebellar abscess. Since the cerebellum is involved in
fine motor coordination and control of the central part of the
body, especially during walking, these individuals often would lose
coordination or have significant difficulties walking.Mastoid
infections can assume two different patterns. Chronic mastoiditis
is a disease process that is occurring more than three months and
acute mastoiditis is occurring less than three weeks.a. Acute
mastoiditisAcute mastoiditisis almost always a consequence of an
acute ear infection that is not treated or is incompletely treated.
In acute mastoiditis there is a direct bacterial infection in the
mastoid. Often the skin overlying the mastoid directly behind the
outer ear becomes inflamed and as a consequence is red and swollen.
If the infection continues for more than 10 to 14 days, the small,
bony walls that form the air-filled honeycomb begin to be
destroyed. This bone destruction is termed coalescent mastoiditis.
If the infection continues, then there can be direct pus
accumulation under the skin behind the ear, with a resultant
abscess. b. Chronic mastoiditisChronic mastoiditis occurs whenever
there is a chronic inflammatory process that affects the mastoid.
This is usually termed chronic otitis media, where there is a
perforation in the eardrum, with intermittent infected material
draining through the hole in the eardrum. In chronic mastoiditis
there is no bone destruction as is seen in coalescent mastoiditis.
Instead the lining inside the mastoid often becomes thickened and
inflamed.
2.2. PetrositisThis rare complication of OM occurs in both acute
and chronic forms. In the acute form, there is extension of acute
mastoiditis into a pneumatized petrous apex. The chronic form of
petrositis usually occurs as a result of mucosal or
cholesteatomatous CSOM; pneumatization of the petrous apex is not a
prerequisite as the infection spreads by thrombophlebitis,
hematogenous dissemination, or direct extension. Because of the
close relationship of the ophthalmic division of the trigeminal
nerve and the abducens nerve to the petrous apex, the classic
features of petrositis are otorrhea associated with retroorbital
pain and lateral rectus palsy (Gradenigo syndrome). Because of the
high incidence of an intracranial extension of infection from
petrositis, a combination of antibiotics and surgical drainage of
the petrous apex is the management of choice.
2.3. Facial Nerve ParalysisFacial nerve palsy can occur as a
result of either acute or chronic OM. There are two mechanisms by
which OM can result in facial nerve paralysis: 1. as a result of
the locally produced bacterial toxins2. from direct pressure
applied to the nerve by cholesteatoma or granulation tissue. An
episode of AOM can lead to inflammatory edema of the nerve and a
subsequent paresis. This situation should be managed by myringotomy
with aspiration of pus from the middle ear along with antibiotic
therapy, which will mostly result in the rapid resolution of
paralysis. Further surgical exploration of the facial nerve is not
indicated unless the paralysis fails to resolve. If facial nerve
paralysis occurs as a result CSOM, urgent surgical exploration,
with decompression of the facial nerve, is indicated.Facial
paralysis associated with chronic otitis media suggests a high
probability of cholesteatoma, and surgical intervention is
appropriate. The mechanism of facial paralysis associated with
cholesteatoma could be compression or inflammation. Djeric studied
autopsy specimens from patients who had chronic otitis media but no
antemortem evidence of facial paralysis. Two of 20 facial nerves
had focal areas of demyelination, suggesting that adjacent
inflammation may be more important than pressure.2.4.
LabyrinthitisLabyrinthinitis is an uncommon complication of acute
otitis media and mastoiditis. there are serous labyrinthitis,
suppurative labyrinthitis, and labyrinthine fistula.Suppurative
labyrinthitis results from bacterial invasion of the inner ear from
contiguous areas of the temporal bone or meninges. Serous
labyrinthitisis an irritation of the labyrinth caused by otitic or
meningitic infection without bacterial invasion of the inner ear.
Fistulization of the labyrinth occurs most commonly as a result of
erosion of the bony covering of the lateral semicircular canal by
cholesteatomaa. Serous labyrinthitisSerous (or toxic) labyrinthitis
results from irritation of the labyrinth by the by-products of
infection and inflammation. Toxins are thought toenter the inner
ear via the oval and round windows or through a fistula in the bony
labyrinth. Serous labyrinthitis may be a complication of acute
orchronic otitis media; meningitis, in which case the condition may
be masked by the more severe meningeal symptoms.The patient
presents with vertigo, which may be transient and recurrent over
months or years; sensorineural hearing loss may fluctuate and is
less severe than that seen in purulent labyrinthitis. It may not be
distinguishable from purulent labyrinthitis, except for retention
of some audiovestibular function. The signs and symptoms are less
dramatic than those of purulent labyrinthitis, and the pathologic
consequences in the inner ear are less destructive. Management is
directed toward the infectious source. If the labyrinthitis results
from acute otitis media, myringotomy and antibiotic therapy are
sufficient. If coalescent mastoiditis or chronic otitis media with
possible cholesteatoma is present, labyrinthine fistula should be
suspected and mastoidectomy should be performed.b. Suppurative
labyrinthitisSuppurative labyrinthitis can develop as a
complication of acute and chronic otitis media from migration of
the bacteria through the preformed pathways of the oval window,
round window, and preexisting fractures of the temporal bone and
from direct invasion by erosion of the labyrinthine bone by
cholesteatoma. Bacteria may traverse the cochlear aqueduct in
bacterial meningitis. Bacterial invasion of the inner ear produces
irreversible damage to the neuroepithelium, atrophy of the stria
vascularis, collapse of Reissners membrane, and endolymphatic
hydrops. If the patient survives without surgery, healing occurs
with fibrosis and obliterative osteitis of the labyrinth and
cochlea. No audiovestibular function isretained.The symptoms are
most severe during the acute bacterial invasion of the labyrinth.
The vertigo and nystagmus result from sudden loss of the
healthytonic neural impulses from the involved labyrinth, without
any change in the input from the healthy side. Recovery from a
unilateral peripheralvestibular lesion is attributed to the brains
ability to compensate for the sensory mismatch by adapting to the
asymmetric sensory input. This occursgradually as the cerebellum
and brainstem integrate the conflicting information and adapt over
time to a stable lesion. The severity of the symptomsgradually
lessens over the next few days, but central compensation occurs
over several weeks with complete resolution of nystagmus and
vertigo.c. Labyrinthine fistulaFistulization of the labyrinth
occurs most commonly as a result of erosion of the bony covering of
the lateral semicircular canal by cholesteatoma. The patient will
have active or inactive chronic otitis media for many years. The
mainstay of the diagnosis, the fistula test, is performed by
application of positive and negative pressure to the middle ear
with a pneumatic otoscope. A positive fistula test produces
nystagmus with the fast component toward the tested ear with
application of positive pressure, and away from the tested ear with
application of negative pressure. The nystagmus results from motion
of the soft tissue over the fistula; positive pressure causes
ampullofugal movement of endolymph (away from the ampulla), and
negative pressure causes ampullopetal movement of the endolymph
(toward the ampulla. Management is mastoidectomy with eradication
of cholesteatoma
3. Intracranial ComplicationsThe most common early symptoms of
intracranial extension of infection are persistent headache and
fever. Other features include lethargy, irritability, and neck
stiffness. A decreasing level of consciousness and seizures are
late signs associated with a poor prognosis. The incidence of
intracranial complications has been considerably reduced since the
introduction of antibiotics. Despite this fact, once an
intracranial complication develops, it carries a significant risk
to life. Therefore, early recognition and treatment are vital to
improve the prognosis. It is not uncommon for more than one
intracranial complication to occur simultaneously. 3.1.
MeningitisAcute otitis media is the most common cause of bacterial
meningitis. It can occur as a result of hematogenous spread, of
direct extension from the middle ear through a bony dehiscence, or
through the cochlear aqueduct via the inner ear. The most common
organisms responsible for otic meningitis are S pneumoniae and H
influenzae type B. The classic presentation is with
headaches,photophobia, neck stiffness, and fluctuating levels of
consciousness. The evaluation should include an MRI of the brain to
rule out other intracranial complications as well as a lumbar
puncture. If meningitis is secondary to AOM, then a myringotomy
should be performed once antibiotic therapy has been initiated. In
the case of CSOM resulting in meningitis, the patient should be
fully stabilized before considering surgical management of the
chronic ear disease.
3.2. Intracranial Abscess Brain, subdural, and extradural
abscesses can all arise as a complication of middle ear infections
(commonly associated with chronic disease). Intracranial abscesses
are usually caused by multiple aerobic and anaerobic bacteria.
Commonly cultured organisms include streptococci, S aureus, S
pneumoniae, H influenzae, P aeruginosa, Bacteroides fragilis, and
Proteus species.a. Brain abscessMost otogenic brain abscesses
develop within the temporal lobe or cerebellum. The progression of
symptoms from a brain abscess can be gradual, occurring over days
or even weeks. In addition to the generalized symptoms, focal
neurologic signs can develop depending on the anatomic location of
the abscess within the brain. As the abscess enlarges, features
typical of raised intracranial pressure develop. Once a brain
abscess has been diagnosed, urgent neurosurgical intervention is
indicated to drain the abscess. Surgery for the associated ear
disease is less urgent and should be planned when the patients
condition is more stable.b. Subdural abscessA subdural abscess
forms between the dura mater and the arachnoid mater. Symptoms and
signs tend to progress much more rapidly than those seen with a
brain abscess. Drainage of the abscess is the mainstay of
treatment.c. Extradural abscessExtradural abscesses are typically
formed in the middle fossa between the dura mater and the thin bony
plate of the tegmen. They can also occur in the posterior fossa,
where they are commonly associated with lateral sinus thrombosis.
The clinical features are often nonspecific and may fluctuate if a
dehiscence in the tegmen is present, allowing the abscess to
partially drain into the mastoid cavity. As with other intracranial
complications, headache and fever are the most common features.
Because of its location, an extradural abscess can usually be
drained through a mastoidectomy approach while treating the
underlying middle ear disease.
3.3. Lateral Sinus ThrombosisBecause of its close proximity to
the mastoid air cells, the lateral, or sigmoid, sinus is prone to
involvement in middle ear infections, which may lead to thrombosis.
Once an infected thrombus has formed in the lateral sinus, it may
propagate both distally and proximally and may give rise to
infected emboli. Typically, there are intermittent episodes of high
pyrexia associated with rigors. If the thrombus propagates into the
neck, there will be neck tenderness along the internal jugular vein
and neck stiffness or torticollis. Proximal extension of the
thrombus to the sagittal sinus can result in symptoms and signs of
raised intracranial pressure. MRI most reliably makes the diagnosis
of lateral sinus thrombosis. The management of lateral sinus
thrombosis requires broad-spectrum antibiotics and surgery. A
complete mastoidectomy should be performed, with exposure of the
lateral sinus. Once the diagnosis has been confirmed by needle
aspiration, the sinus is opened and the infected thrombus
evacuated. If symptoms persist after this procedure, consideration
should be given to ligation of the ipsilateral internal jugular
vein, once the possibility of other intracranial complications has
been excluded.
3.4. Otic HydrocephalusOtic hydrocephalus is a rare complication
in which raised intracranial pressure develops as a result of a
middle ear infection, but its pathophysiology is poorly understood.
The usual features are headache, vomiting, disturbed mental state,
visual disturbance, and papilledema associated with a middle ear
infection. Imaging of the brain reveals the ventricular size to be
normal, but lumbar puncture confirms raised cerebrospinal fluid
pressure. Management is aimed at resolving the middle ear infection
while normalizing intracranial pressure with the use of steroids,
diuretics (eg, mannitol), and, if required, intermittent drainage
of cerebrospinal fluid.
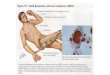
Facial Nerve
Motor Component of Facial NerveThe nucleus of the motor
component of the facial nerve is located in the ventrolateral
portion of the pontine tegmentum. The neurons of this motor nucleus
are analogous to the anterior horn cells of the spinal cord, but
are embryologically derived from the second branchial arch. The
root fibers of this nucleus take a complicated course.Within the
brainstem, they wind around the abducens nucleus (forming the
so-called internal genu of the facial nerve), thereby creating a
small bump on the floor of the fourth ventricle (facial
colliculus). They then form a compact bundle, which travels
ventrolaterally to the caudal end of the pons and then exits the
brainstem, crosses the subarachnoid space in the cerebellopontine
angle, and enters the internal acoustic meatus together with the
nervus intermedius and the eighth cranial nerve (the
vestibulocochlear nerve).Within the meatus, the facial nerve and
nervus intermedius separate from the eighth nerve and travel
laterally in the facial canal toward the geniculate ganglion. At
the level of the ganglion, th e facial canal takes a sharp downward
turn (external genu of the facial nerve). At the lower end of the
canal, the facial nerve exits the skull through the stylomastoid
foramen. Its individual motor fibers are then distributed to all
regions of the face (some of them first traveling through the
parotid gland). They innervate all of the muscles of facial
expression that are derived fromthe second branchial arch, i.e.,
the orbicularis oris and oculi, buccinator, occipitalis, and
frontalis muscles and the smaller muscles in these areas, as well
as the stapedius, platysma, stylohyoid muscle, and posterior belly
of the digastric muscle.
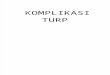
Motor lesions involving the distribution of the facial nerve.The
muscles of the forehead derive their supranuclear innervation from
both cerebral hemispheres, but the remaining muscles of facial
expression are innervated only unilaterally, i.e., by the
contralateral precentral cortex. If the descending supranuclear
pathways are interrupted on one side only, e. g., by a cerebral
infarct, the resulting facial palsy spares the forehead muscles:
the patient can still raise his or her eyebrows and close the eyes
forcefully. This type of facial palsy is called central facial
palsy.In a nuclear or peripheral lesion, however, all of the
muscles of facial expression on the side of the lesion are weak.
One can thus distinguish central from nuclear or peripheral facial
palsy by their different clinical appearances. The motor nuclei of
the facial nerve are innervated not only by the facial cortex but
also by the diencephalon, which plays a major role in
emotion-related facial expressions. Further input is derived from
the basal ganglia; in basal ganglia disorders (e. g., Parkinson
disease), hypomimia or amimia can be seen. There are also various
dyskinetic syndromes affecting the muscles of facial expression
with different types of abnormal movement: hemifacial spasm, facial
dyskinesias, and blepharospasm, among others. The site of the
causative lesion in these syndromes remains unknown.
Differetial Diagnosis of Facial Paralysis
RESOURCES: Lalwani AK, editor. Current Diagnosis & Treatment
in Otolaryngology - Head & Neck Surgery. USA: McGraw-Hill;
2008. Cummings et al, editor. Otolaryngology - Head and Neck
Surgery. Ed ke-3. USA: Mosby-Year Book; 1998. Baehr M, Frotscher M.
Duus Topical Diagnosis in Neurology. Ed ke-4. Germany: Georg Thieme
Verlag; 2005. Putz R, Pabst R. Sobotta: Atlas Anatomi Manusia. Ed
ke-22. Jilid 1. Jakarta: Penerbit Buku Kedokteran EGC; 2006.
Effendi H, editor. Boies: Buku Ajar Penyakit THT. Ed ke-6. Jakarta:
Penerbit Buku Kedokteran EGC; 1997.