Embed Size (px)
Citation preview

Myotonia CongenitaMyotonia Congenita
Shannon L Venance, MD PhDShannon L Venance, MD PhD
ICNDM, Kansas CityICNDM, Kansas City
June 3, 2007June 3, 2007

Disclosure StatementDisclosure Statement
NIH: 8U54 NS059065 funding for NIH: 8U54 NS059065 funding for the Consortium for Clinical the Consortium for Clinical Investigation of Neurological Investigation of Neurological ChannelopathiesChannelopathies
Port Elgin Rotarians for patient-Port Elgin Rotarians for patient-centered Muscular Dystrophy centered Muscular Dystrophy ResearchResearch

Nondystrophic Nondystrophic MyotoniasMyotonias
disorders of muscle membrane excitabilitydisorders of muscle membrane excitabilitypainless muscle stiffnesspainless muscle stiffness
chloride channelopathies (chloride channelopathies (CLCN1CLCN1) ) – myotonia congenita (MC)myotonia congenita (MC)
autosomal dominant (Thomsen) 1876autosomal dominant (Thomsen) 1876 autosomal recessive (Becker) 1977autosomal recessive (Becker) 1977
– myotonic dystrophy type 1 and 2myotonic dystrophy type 1 and 2
sodium channelopathies (sodium channelopathies (SCN4ASCN4A))– paramyotonia congenita (PMC)paramyotonia congenita (PMC)– potassium-aggravated myotonia (PAM)potassium-aggravated myotonia (PAM)
AZM-responsive myotoniaAZM-responsive myotonia myotonia fluctuans and myotonia permanensmyotonia fluctuans and myotonia permanens
– hyperkalemic periodic paralysis (HyperPP)hyperkalemic periodic paralysis (HyperPP)

CaveatsCaveats
marked phenotypic variability within and marked phenotypic variability within and between affected individuals and between affected individuals and kindreds kindreds (e.g. Thomsen pedigree P480L )(e.g. Thomsen pedigree P480L )– dominant mutations with dominant mutations with reduced reduced
penetrancepenetrance– asymptomatic heterozygotes in AD pedigreesasymptomatic heterozygotes in AD pedigrees– identical mutations in dominant and identical mutations in dominant and
recessive pedigreesrecessive pedigrees– kindreds with unusual featureskindreds with unusual features
modifying genes and/or environmental modifying genes and/or environmental factors yet to be determinedfactors yet to be determined
need for prospectively collected, need for prospectively collected, standardized data standardized data

27 yo male with muscle stiffness27 yo male with muscle stiffness went to his family physician at age 12went to his family physician at age 12
– parents and teachers were “hassling” him to “try parents and teachers were “hassling” him to “try harder”harder”
– ““last kid off the mark in gym class”last kid off the mark in gym class” knew he “couldn’t keep up” in ? grade 1 but knew he “couldn’t keep up” in ? grade 1 but
“tried to hide it by constantly moving”“tried to hide it by constantly moving” responds well to mexiletineresponds well to mexiletine 2 sisters also affected, but to a lesser degree2 sisters also affected, but to a lesser degree parents clinically and (dad parents clinically and (dad
electrophysiologically) unaffectedelectrophysiologically) unaffected ocular myotonia; lid lag; percussion and grip ocular myotonia; lid lag; percussion and grip
myotonia - improves with repetitionmyotonia - improves with repetition hypertrophy of thoracolumbar paraspinals, hypertrophy of thoracolumbar paraspinals,
thigh and leg; mild restriction of ankle thigh and leg; mild restriction of ankle dorsiflexiondorsiflexion

37 yo male with lifelong muscle stiffness 37 yo male with lifelong muscle stiffness (father similarly affected)(father similarly affected)
onset in infancy: stiffness noted with rolling onset in infancy: stiffness noted with rolling over and crawling; frequent falls when over and crawling; frequent falls when learning to walk learning to walk
stiffness is painless and improves with stiffness is painless and improves with activityactivity– stopped playing hockey as a teenager – fell on the stopped playing hockey as a teenager – fell on the
ice, unable to “jump over the boards”ice, unable to “jump over the boards”– continues to golf and play tennis – uses continual continues to golf and play tennis – uses continual
motion to stay loosemotion to stay loose ““worse in the cold”worse in the cold” flecainide 100 mg bid helpful (tocainide was flecainide 100 mg bid helpful (tocainide was
better)better) delayed eye opening with forced eye closure, delayed eye opening with forced eye closure,
better with repetition; lid lag; mild percussion, better with repetition; lid lag; mild percussion, grip (and widespread electrical) myotoniagrip (and widespread electrical) myotonia
well-developed musculature well-developed musculature

MC: AR MC: AR andand AD AD
typically onset in 1typically onset in 1stst decade decade painless muscle stiffness; mild to severepainless muscle stiffness; mild to severe ““warm-up”warm-up”
may not be prominent if severe myotoniamay not be prominent if severe myotonia triggers incl activation after rest, triggers incl activation after rest,
stress/startle, pregnancystress/startle, pregnancyExam……….Exam………. muscle hypertrophy (+/- atrophy)muscle hypertrophy (+/- atrophy) ocular, grip and percussion myotonia w/ ocular, grip and percussion myotonia w/
warmupwarmup lid laglid lag stair test stair test
– 10 stairs ~ 4 seconds if unaffected10 stairs ~ 4 seconds if unaffected
EDX – diffuse electrical myotoniaEDX – diffuse electrical myotonia

AR (AR (vs.vs. AD) AD)
absent family historyabsent family history older onset older onset more severely affected ; 15-20% painfulmore severely affected ; 15-20% painful leg onset (vs. face/hands in AD)leg onset (vs. face/hands in AD) males males ±± more severely affected than females more severely affected than females transient weakness transient weakness ±± progressive into 4 progressive into 4thth decade decade ±± focal atrophy (distal forearms and neck) focal atrophy (distal forearms and neck) a proportion develop fixed weaknessa proportion develop fixed weakness

Lumpers vs. SplittersLumpers vs. Splitters
Big picture gal? Detail guy?
Cl vs Na MC+v, PAM+v, PMC

Myotonia Congenita Myotonia Congenita VariantsVariants
due to due to CLCN1CLCN1; dominant inheritance; dominant inheritance– myotonia levior myotonia levior
milder, later onset, grip stiffness after rest milder, later onset, grip stiffness after rest no hypertrophyno hypertrophy
– fluctuating myotonia congenita fluctuating myotonia congenita (G200R)(G200R) painfulpainful; legs > arms; legs > arms percussion and grip myotoniapercussion and grip myotonia fluctuates with fluctuates with symptom free intervalssymptom free intervals stiffness with activation after rest, pregnancy, stiffness with activation after rest, pregnancy,
fasting, stressfasting, stress

and…Potassium and…Potassium Aggravated Myotonia Aggravated Myotonia
(PAM)(PAM) sodium channelopathies (sodium channelopathies (SCN4A); SCN4A); often ADoften AD
– potassium potassium and and exerciseexercise trigger symptoms trigger symptoms– do not worsen after cold exposuredo not worsen after cold exposure– do not have episodic weaknessdo not have episodic weakness
myotonia fluctuansmyotonia fluctuans– asymptomatic periodsasymptomatic periods; worsening myotonia with delay ; worsening myotonia with delay
after start of exercise; ocular paramyotoniaafter start of exercise; ocular paramyotonia acetazolamide responsive myotoniaacetazolamide responsive myotonia
– painfulpainful; may worsen throughout childhood and ; may worsen throughout childhood and adolescence with dramatic improvement with adolescence with dramatic improvement with ACZACZ
myotonia permanensmyotonia permanens (G1306E) sporadic (G1306E) sporadic– severe, persistent myotonia of face, limbs and severe, persistent myotonia of face, limbs and
intercostals; hypertrophy of neck and shoulder muscles; intercostals; hypertrophy of neck and shoulder muscles; ± ± respiratory compromiserespiratory compromise

inheritanceinheritance Thomsen ADThomsen AD Becker ARBecker AR PAM ADPAM AD PMC ADPMC AD
clinical clinical myotoniamyotonia
mild-mild-moderatemoderate
face; UE > face; UE > LELE
mod-severemod-severe
LE > UELE > UEfluctuating to fluctuating to
severeseveremild-modmild-mod
face, UE, LEface, UE, LE
age of age of onsetonset
11stst decade decade 11stst -2 -2ndnd decadedecade
childhoodchildhood
late 1late 1stst decadedecade
late 1late 1stst decade decade
triggerstriggers restrest restrest exercise, Kexercise, K exercise, coldexercise, cold
warm-upwarm-up improvesimproves improvesimproves ?? worsensworsens
coldcold no effectno effect no effectno effect not reallynot really myotonia myotonia worse; ± worse; ± paralysisparalysis
episodic episodic weaknessweakness
nono ± transient ± transient proximalproximal
nono yesyes
lid laglid lag yesyes yesyes yesyes yesyes
hypertrophhypertroph
yy
mildmild modmod ARM and MPARM and MP ±±
treatmenttreatment mexiletinemexiletine
flecanideflecanidemexiletinemexiletine
flecanideflecanidemexiletinemexiletine
acetazolamidacetazolamidee
mexiletinemexiletine
acetazolamideacetazolamide
genegene CLCN1CLCN1 CLCN1CLCN1 SCN4ASCN4A SCN4ASCN4A

Questions to be Questions to be answeredanswered
Will the differences in clinical Will the differences in clinical phenotype combined with EDX studies phenotype combined with EDX studies accurately predict genotype?accurately predict genotype?
What additional genetic and/or What additional genetic and/or environmental factors are responsible environmental factors are responsible for the intra- and inter-familial for the intra- and inter-familial phenotypic variability?phenotypic variability?
Will treatment prevent the permanent Will treatment prevent the permanent weakness seen in a proportion of NDM weakness seen in a proportion of NDM patients? How do we identify those patients? How do we identify those that will benefit from treatment?that will benefit from treatment?

AcknowledgementsAcknowledgements
London ON CINCH team
Angelika Hahn
Wilma Koopman
Kori LaDonna
Karen Findlater
CINCH
Rochester NY
Robert Griggs
Rabi Tawil
Barbara Herr
Kansas City, KS
Rick Barohn
Laura Herbelin

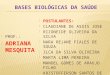
AR myotonia congenitaAR myotonia congenita(Becker)(Becker)
~ 1/50,000 onset late in 1st decade; more severe than AD legs > arms; 15% painful warm-up helpful for most, but not all triggered after rest, stress, worsens during
pregnancy grip, neck > tongue myotonia; lid lag ~50% hypertrophy often of gluteal and leg muscles with
atrophy of forearm muscles transient weakness but % will develop permanent
weakness ± wrist and ankle contractures; toe walking CK normal to 2-3x ↑

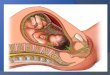
AD myotonia congenitaAD myotonia congenita(Thomsen)(Thomsen)
~1/15,000-25,000~1/15,000-25,000 onset in onset in infancy or early childhoodinfancy or early childhood face, tongue, pharyngeal muscles, handsface, tongue, pharyngeal muscles, hands
and legsand legs triggered by activation after rest, startle, triggered by activation after rest, startle,
stress, increased in pregnancystress, increased in pregnancy ““warm-up” will minimize stiffnesswarm-up” will minimize stiffness muscle hypertrophy without weaknessmuscle hypertrophy without weakness grip and percussion myotonia; lid lag and grip and percussion myotonia; lid lag and
ocular myotoniaocular myotonia CK normal or mildly increasedCK normal or mildly increased

Fournier et al, 2006
Electrophysiology Electrophysiology HelpsHelps
routine NCS (routine NCS (± after potentials)± after potentials) EMG: myotonic potentialsEMG: myotonic potentials short exercise protocol with short exercise protocol with
repetition repetition ±± cold exposure cold exposure
more in the afternoon Neurophysiology session!!