Embed Size (px)
Citation preview
Abnormal placentation: multidisciplinary
challenges
Universitätsklinik für Frauenheilkunde
Certified Gynecological Oncology
Center (DKG)
Certified Breast Cancer Center (DKG)
Certified Endometriosis Center (EEL)
Andrea Papadia M.D., Ph.D
Universitätsklinik für Frauenheilkunde, Inselspital
Obstetrics is a bloody
business
DISCLOSURE
Universitätsklinik für Frauenheilkunde, Inselspital
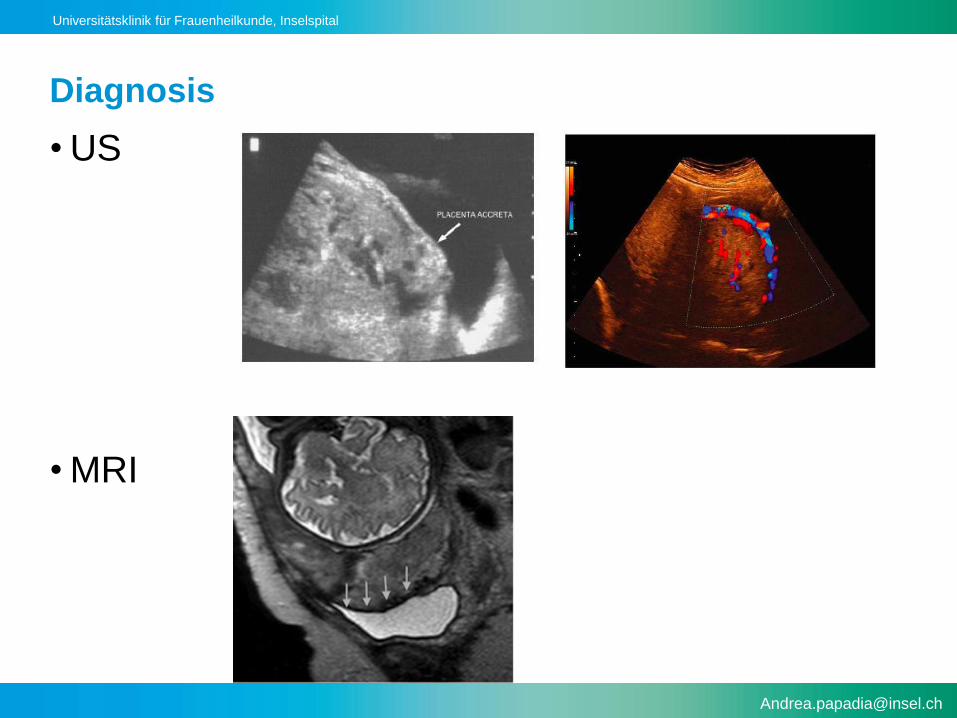
Placenta accreta
• The most common indication for cesarean hysterectomy in
developed countries
• Average blood loss is 3,000–5,000 mL
• 90% of patients with placenta accreta require blood
transfusion,
• 40% require more than 10 uPRBCs
• Maternal mortality is as high as 7%
• Maternal death may occur despite optimal planning,
transfusion management and surgical care
Hudon L, Belfort MA, Broome DR. Diagnosis and management of placenta percreta: a review. Obstet Gynecol Surv 1998;53:509–17.
O’Brien JM, Barton JR, Donaldson ES. The management of placenta percreta: conservative and operative strategies.Am J Obstet Gynecol
1996;175:1632–8.
Universitätsklinik für Frauenheilkunde, Inselspital
Massive bleeding
disseminated intravascular coagulopathy
multiorgan failure
death
Universitätsklinik für Frauenheilkunde, Inselspital
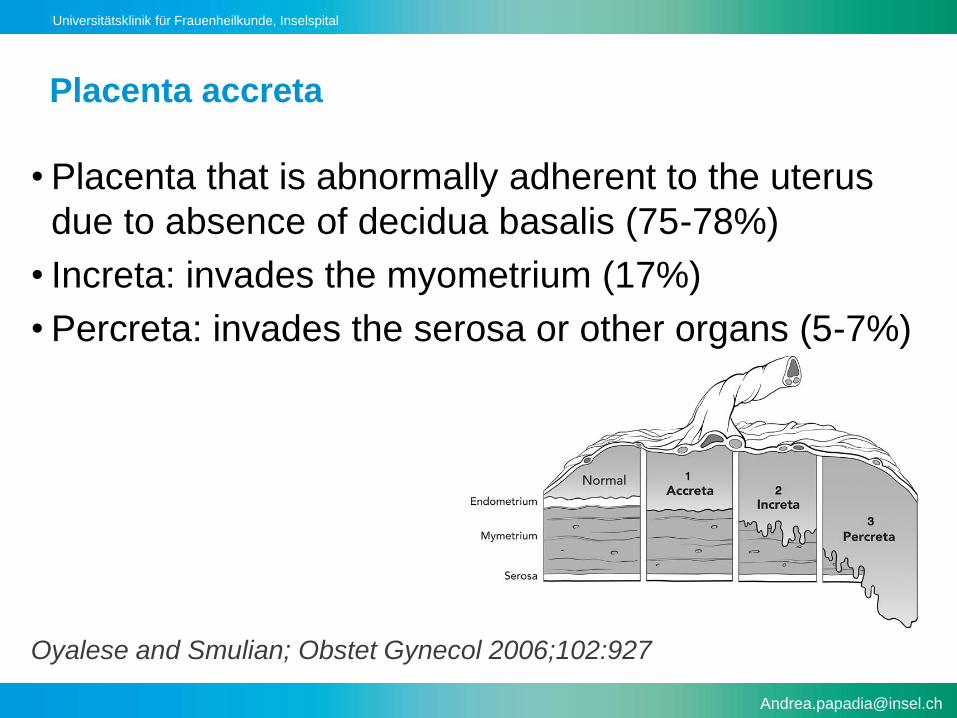
Placenta accreta
• Placenta that is abnormally adherent to the uterus
due to absence of decidua basalis (75-78%)
• Increta: invades the myometrium (17%)
• Percreta: invades the serosa or other organs (5-7%)
Oyalese and Smulian; Obstet Gynecol 2006;102:927
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta – rates increasing
• Approximate rates
–1960s 1 in 30,000 deliveries
–1985 – 1994 1 in 2,510 deliveries
–1982 – 2002 1 in 533 deliveries
Wu S et al: Abnormal placentation: 20 year analysis. AJOG 2005
Miller et al., AJOG 1997
Universitätsklinik für Frauenheilkunde, Inselspital
Risk factors
• Cesarean section
• Cesarean section
• Cesarean section
• Cesarean section
• Cesarean section
• Cesarean section
• Cesarean section
• Cesarean section
• Cesarean section
• Cesarean section
Universitätsklinik für Frauenheilkunde, Inselspital
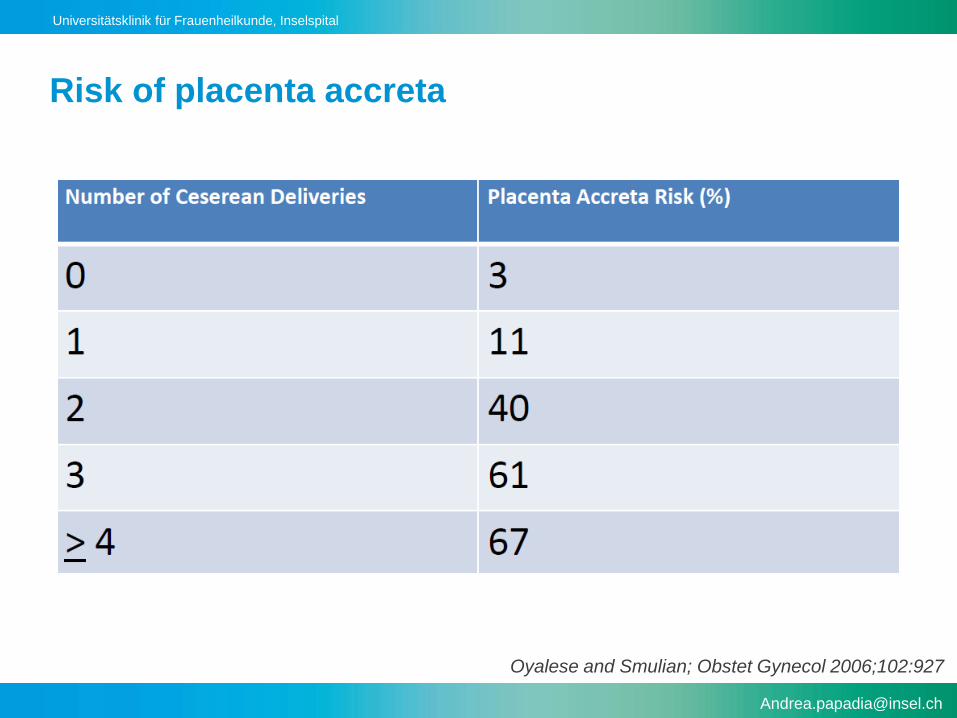
Risk of placenta accreta
Oyalese and Smulian; Obstet Gynecol 2006;102:927
Universitätsklinik für Frauenheilkunde, Inselspital
Clinical relevance
• Clinically, placenta accreta becomes problematic during
delivery when the placenta does not completely separate
from the uterus and is followed by massive obstetric
hemorrhage

Universitätsklinik für Frauenheilkunde, Inselspital
Maternal complications
• ICU admission
• Thromboembolism
• Acute renal failure
• Respiratoy insufficiency
• Pyelonephritis
• Pneumonia
• Wound infection
• Need for additional surgery to treat or control bleeding
• Operative injury/Fistula formation
• Death – mortality 7%
Universitätsklinik für Frauenheilkunde, Inselspital
Neonatal morbidity
• The mean gestational age for scheduled deliveries of
liveborn infants among women with antenatally suspected
placenta accreta was 35.4 weeks (range 33.6–37.9 weeks)
and 50% of infants were admitted to the neonatal intensive
care unit (NICU).
• The mean gestational age for emergency deliveries among
those with antenatally suspected placenta accreta was 2.2
weeks (range 25.6–37 weeks) and 94% of these neonates
required NICU admission.Eller AG et al, BJOG 2011

Universitätsklinik für Frauenheilkunde, Inselspital
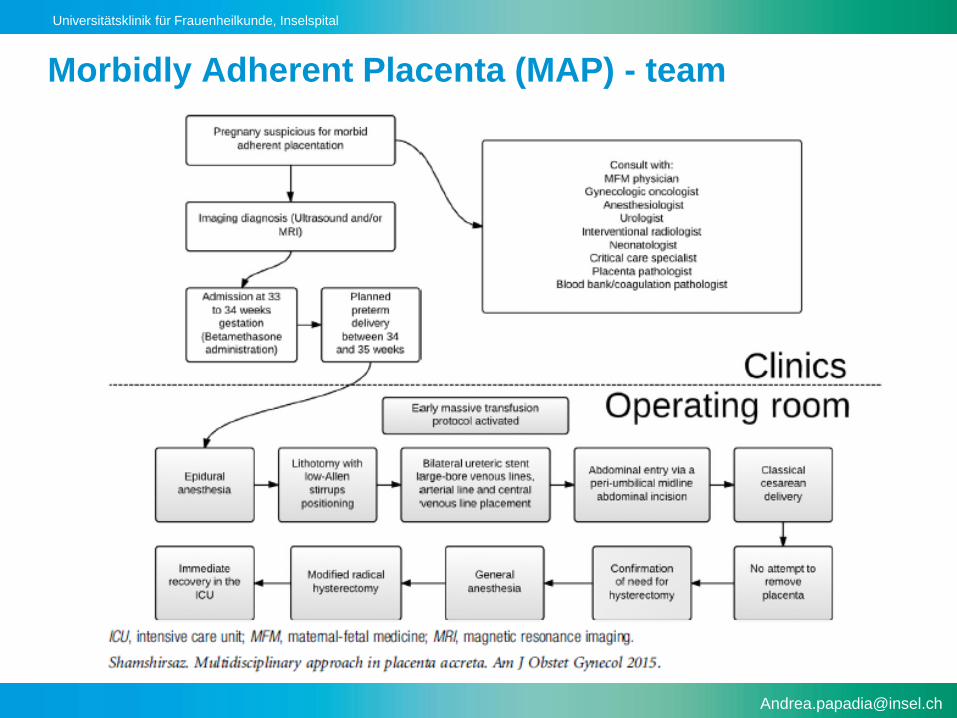
Multidisciplinary approach
• Obstetrician (MFM)
• Gynecologic oncologist
• Anesthesiologist / Criticalc care specialist
• Interventional radiologist
• Neonatologist
• Blood bank
• Urologist
• Vascular surgeon
Universitätsklinik für Frauenheilkunde, Inselspital
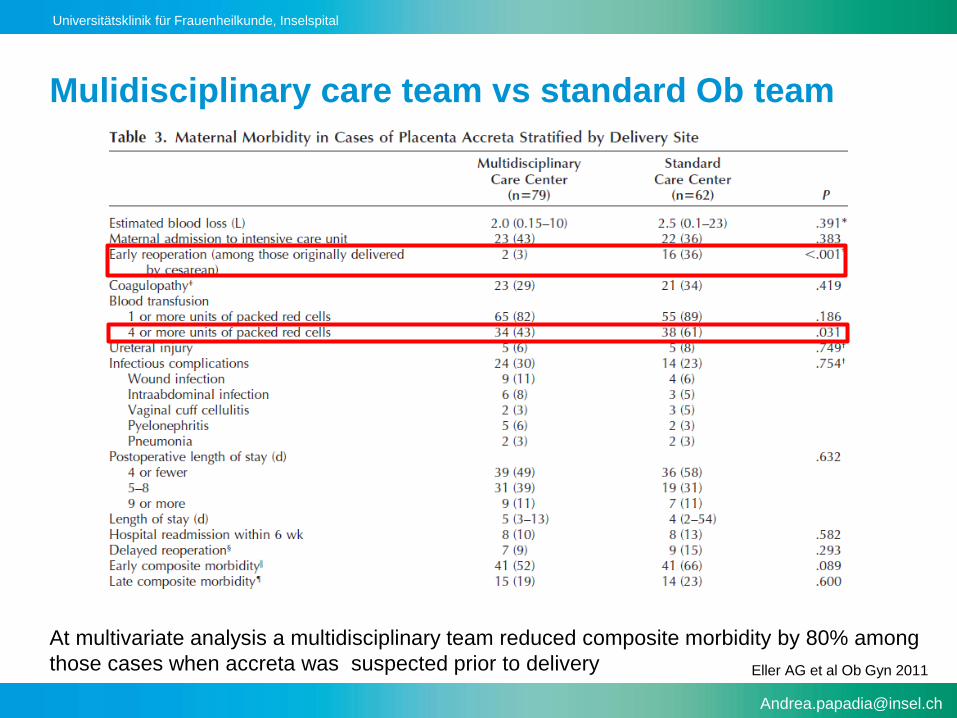
Mulidisciplinary care team vs standard Ob team
At multivariate analysis a multidisciplinary team reduced composite morbidity by 80% among
those cases when accreta was suspected prior to delivery Eller AG et al Ob Gyn 2011
Universitätsklinik für Frauenheilkunde, Inselspital
Morbidly Adherent Placenta (MAP) - team
Universitätsklinik für Frauenheilkunde, Inselspital
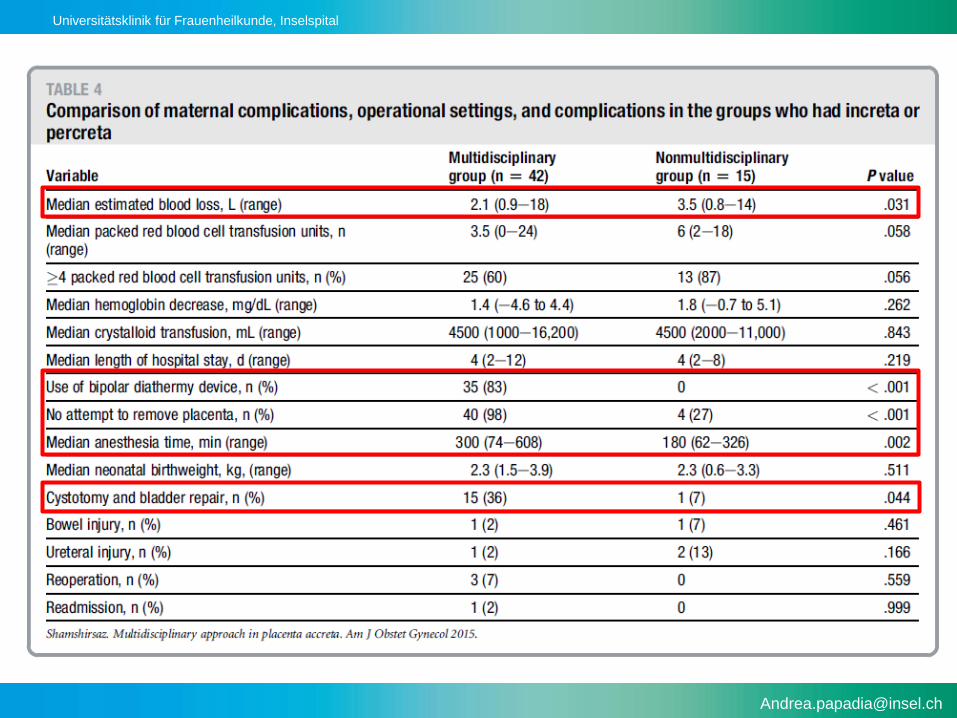
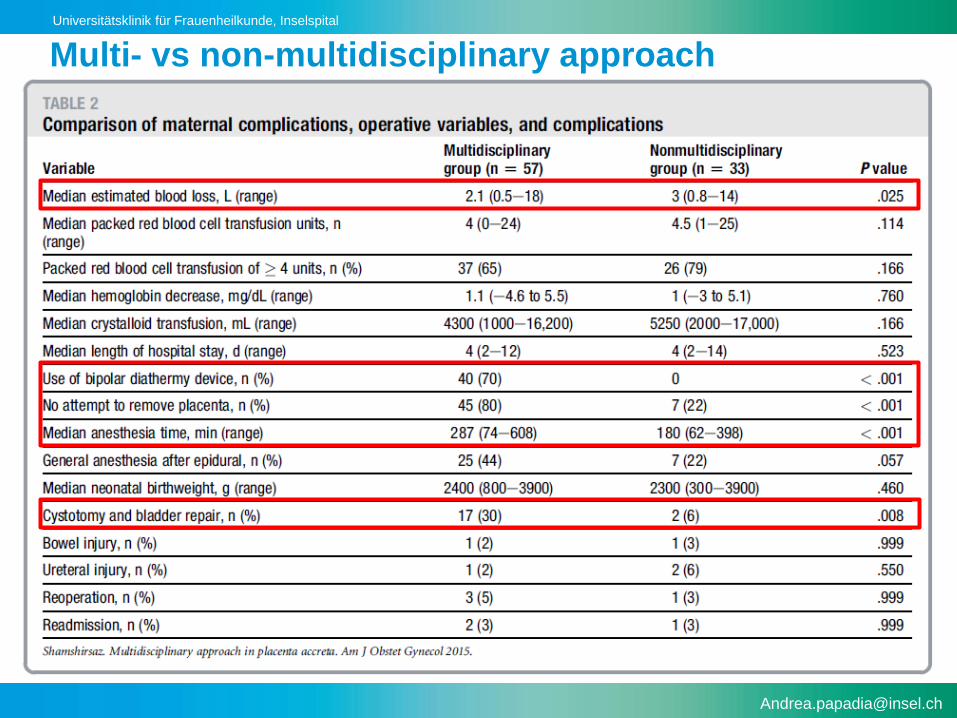
Multi- vs non-multidisciplinary approach
Universitätsklinik für Frauenheilkunde, Inselspital
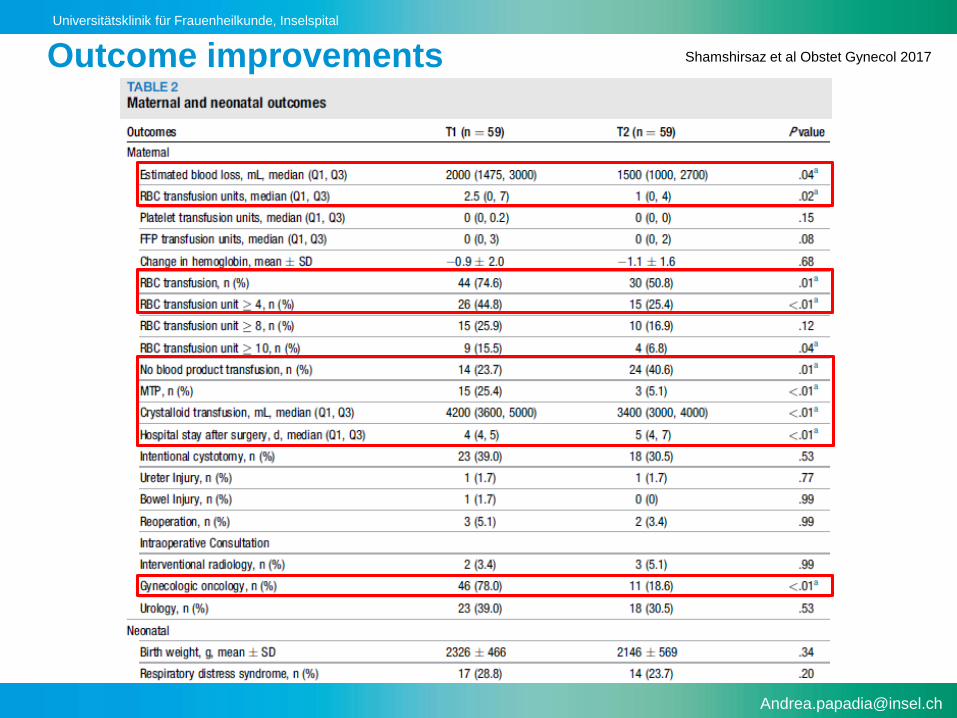
Outcome improvements Shamshirsaz et al Obstet Gynecol 2017
Universitätsklinik für Frauenheilkunde, Inselspital
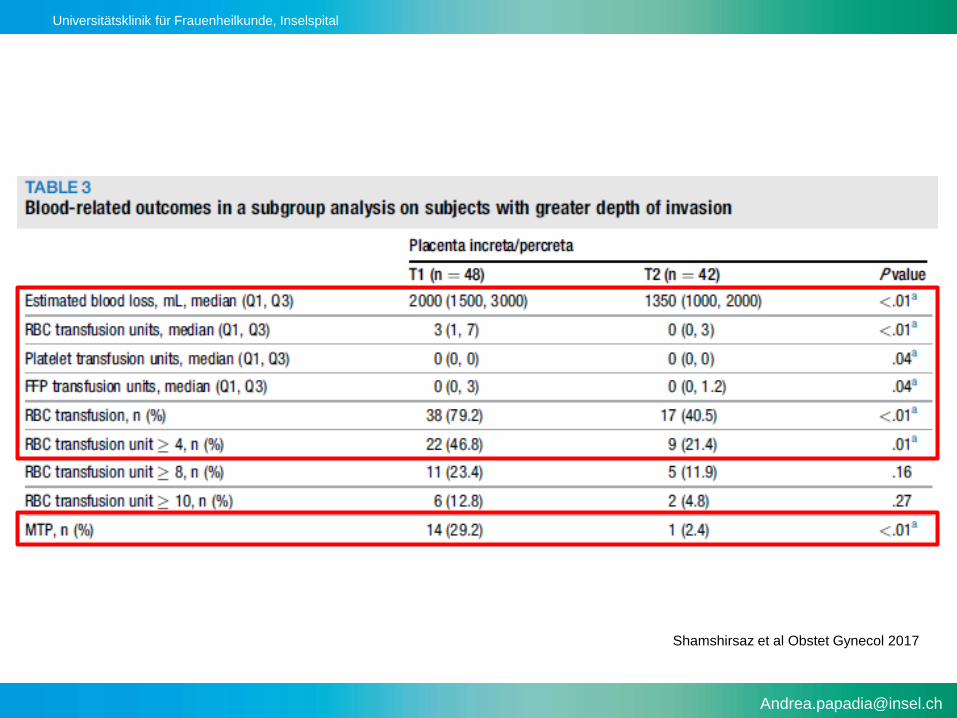
Shamshirsaz et al Obstet Gynecol 2017
Universitätsklinik für Frauenheilkunde, Inselspital
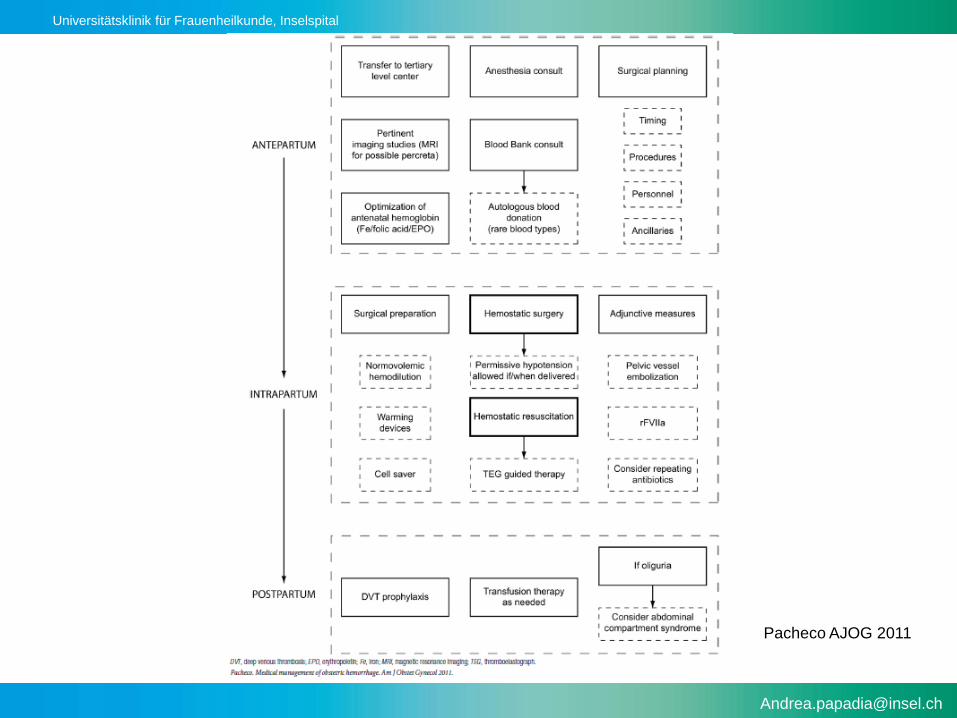
Antepartum interventions
• Once the diagnosis is suspected, patients should receive
iron and/or folic acid as needed to maintain normal
hemoglobin values.
• Occasionally, patients may require recombinant
erythropoietin as adjuvant therapy.
• Occasionally, patients at risk for severe hemorrhage may
benefit from preoperative autologous blood donation.
Pacheco et al AJOG 2011
Catling Int J Obstet anesthesia 2007

Universitätsklinik für Frauenheilkunde, Inselspital
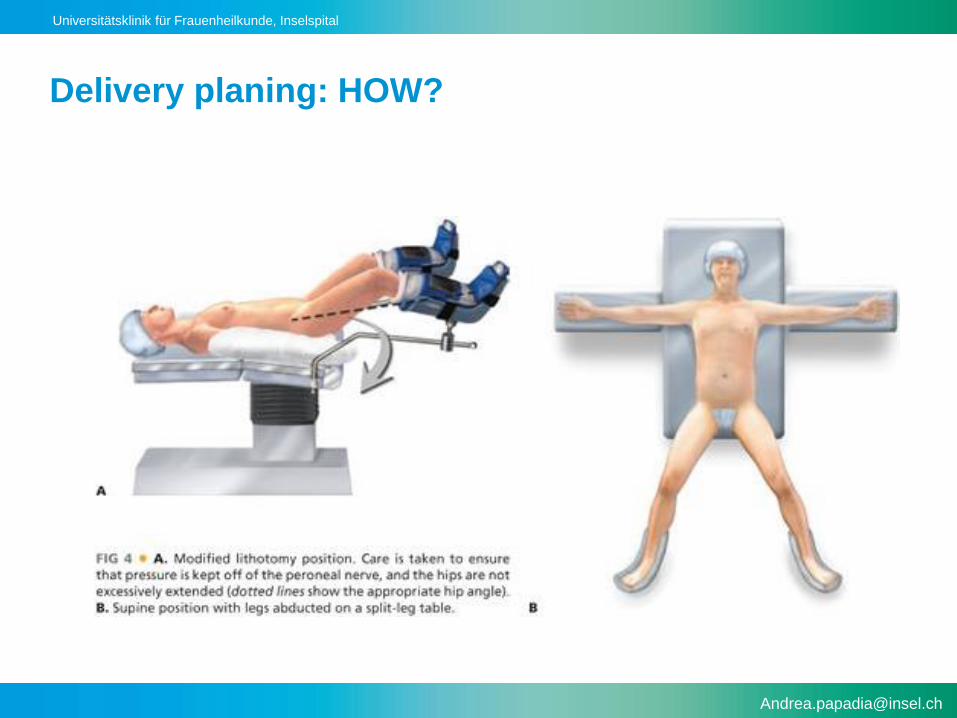
Delivery planning: WHEN?
• Timing should be individualized
• Joint decision (pt, obstetrician, neonatologist)
• Planned delivery reduces EBL and complications!!!
• Develop a contingency plan!
• Antenatal corticosteroids to induce fetal lung maturation
• Optimization of maternal and neonatal outcomes in stable
pts with delivery at 34 WKS
Chestnut DH, Dewan DM, Redick LF, Caton D, Spielman FJ. Anesthetic management for obstetric hysterectomy: a multi-institutional
study. Anesthesiology 1989;70:607–10.
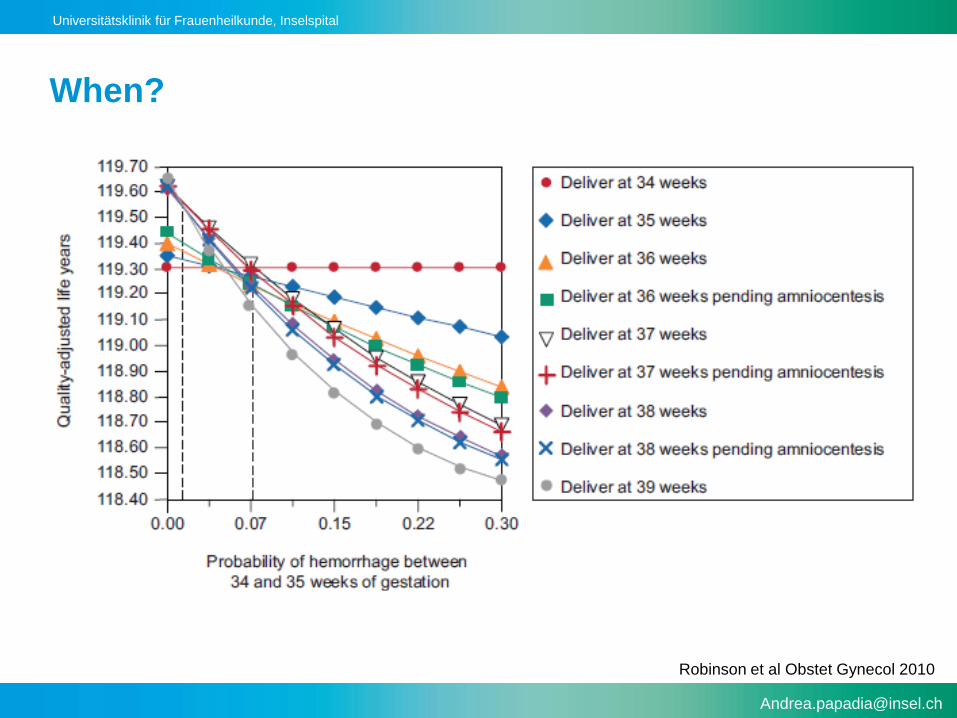
Robinson BK, Grobman WA. Effectiveness of timing strategies for delivery of individuals with placenta previa and
accreta. Obstet Gynecol 2010;116:835–42.
Universitätsklinik für Frauenheilkunde, Inselspital
When?
Robinson et al Obstet Gynecol 2010
Universitätsklinik für Frauenheilkunde, Inselspital
Delivery planing: WHERE?
• The delivery should be performed in an operating
room with the personnel and support services
needed to manage potential complications.
• Interventional radiologist Hybrid OR
• Neonatologists
• Blood bank
• ICU
• Other surgical subspecialties available
Universitätsklinik für Frauenheilkunde, Inselspital
Delivery planing: WHO?
• Experienced multidisciplinary team:
–Obstetrics (MFM)
–Gynecologic onology
–Anesthesist
–Critical care
–Transfusion Medicine
–Interventional radiologist
–Neonatology
–Urology
–Vascular Surgery
Universitätsklinik für Frauenheilkunde, Inselspital
Intrapartum interventions
• Avoid complete sympathectomy
• General anesthesia
• Regional anesthesia with continuous epidural technique
• Acute Normovolemic Hemodilution (ANH)
• Preoperative bilateral common iliac artery catheter?
• CellSaver®
• Recombinant factor VIIa
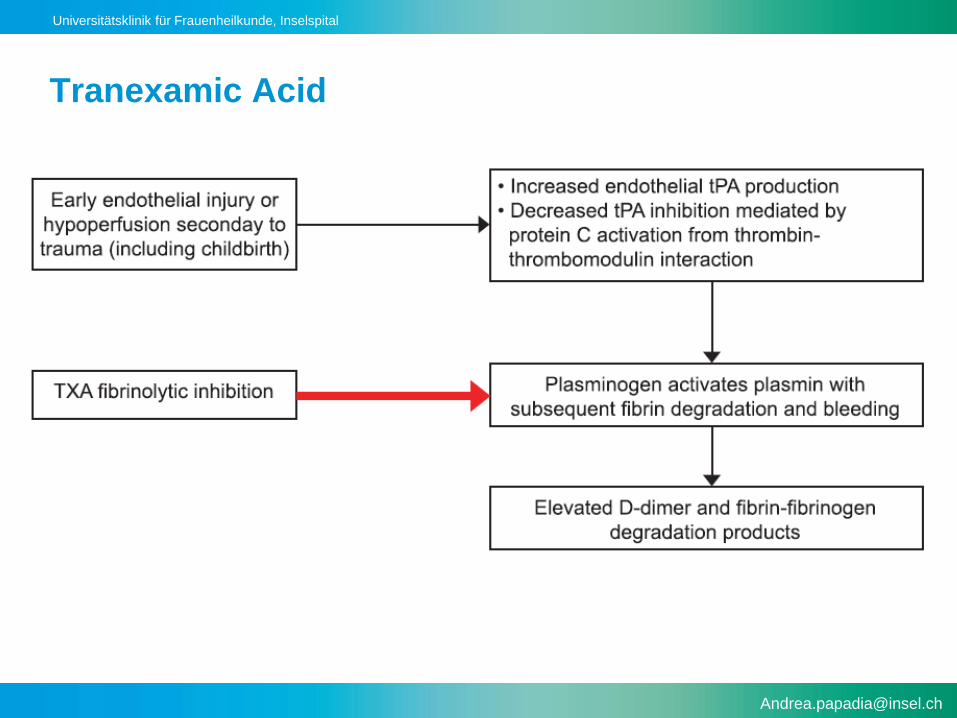
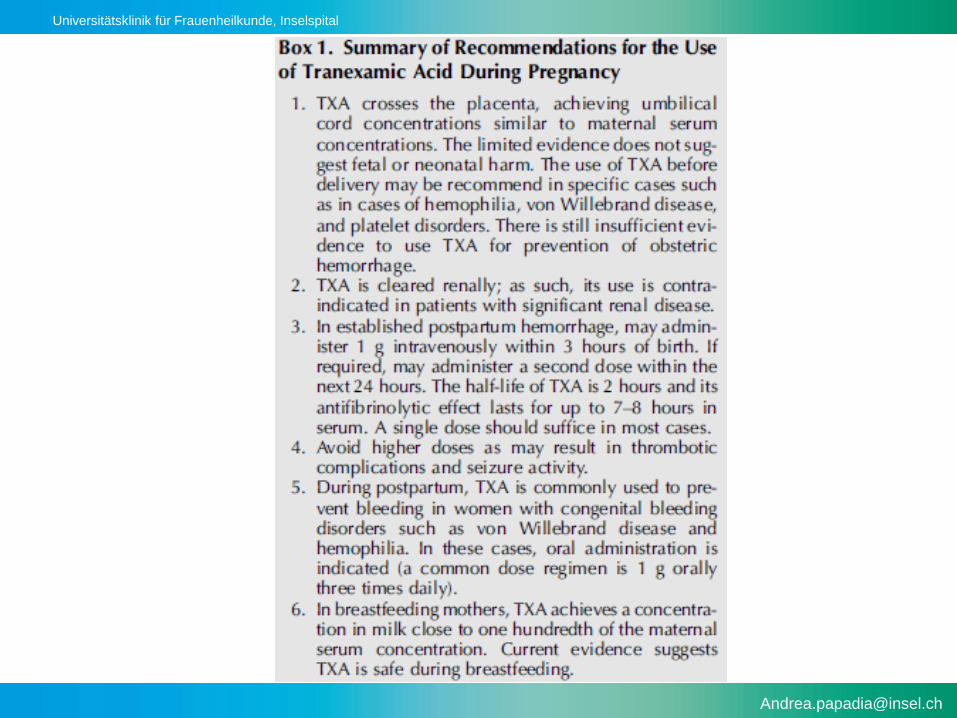
• TXA
Catling Inter J Obstet Anesthesia 2007
Tawes Semin Vasc Surg 1994
Rainaldi Br J Anaesthet 1998

Universitätsklinik für Frauenheilkunde, Inselspital
Effect of TXA on bleeding realted mortality
WOMAN trial. Lancet 2017
Universitätsklinik für Frauenheilkunde, Inselspital
Hemostasis monitoring
• Conventional plasma-based coagulation analyses like PT,
aPTT and international normalized ratio (INR) are poor
predictors of transfusion requirements
• Thromboelastograph (TEG) is an easy test that provides
information on specific components of the coagulation
process
Universitätsklinik für Frauenheilkunde, Inselspital
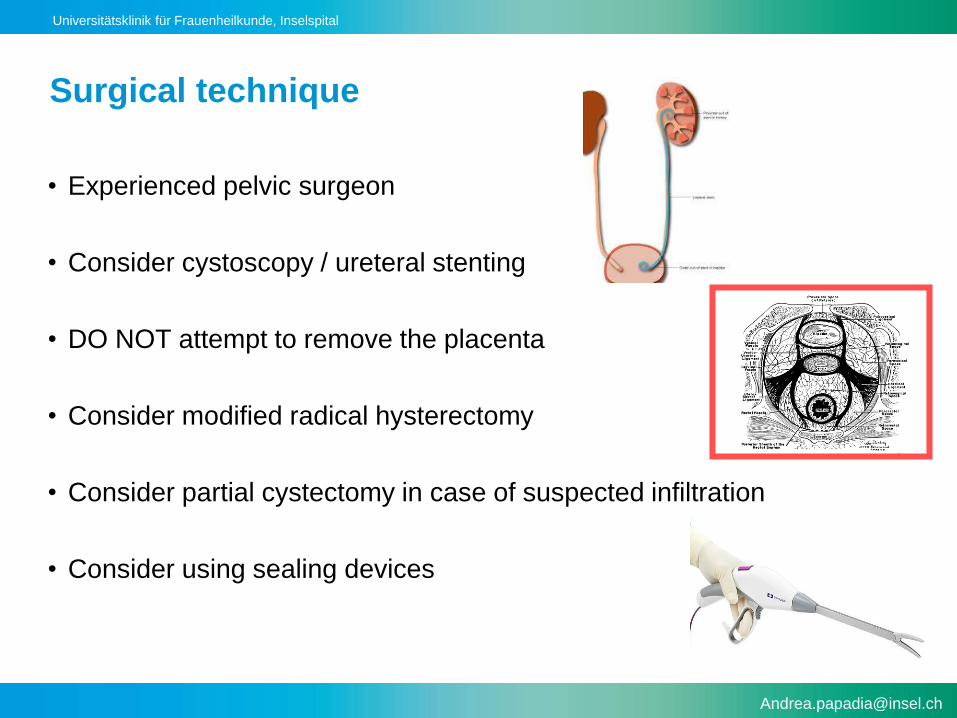
Surgical technique
• Experienced pelvic surgeon
• Consider cystoscopy / ureteral stenting
• DO NOT attempt to remove the placenta
• Consider modified radical hysterectomy
• Consider partial cystectomy in case of suspected infiltration
• Consider using sealing devices
Universitätsklinik für Frauenheilkunde, Inselspital
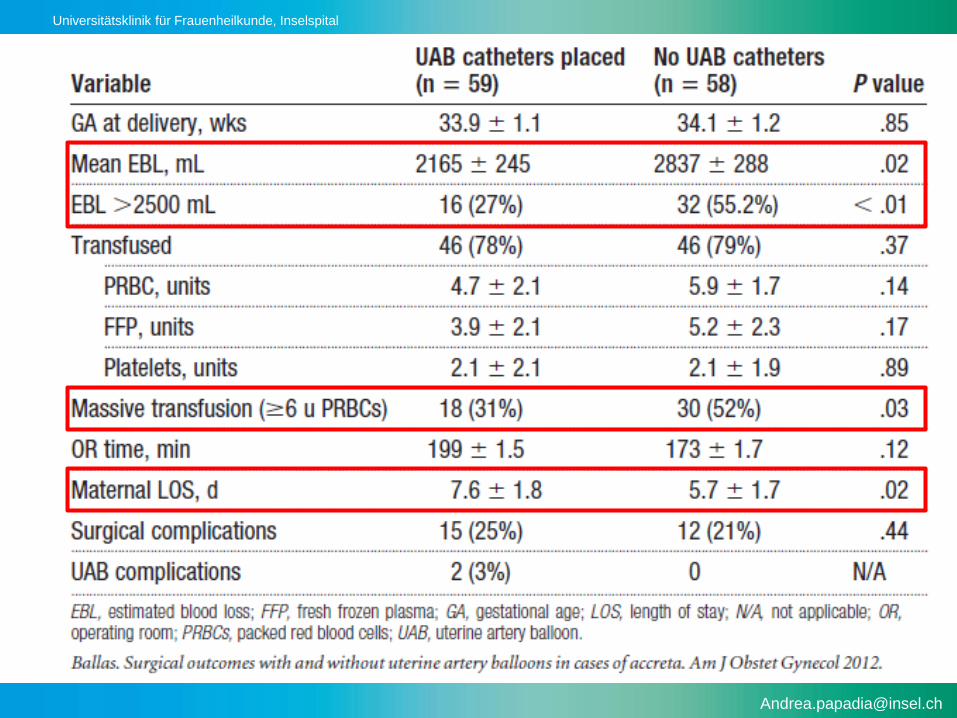
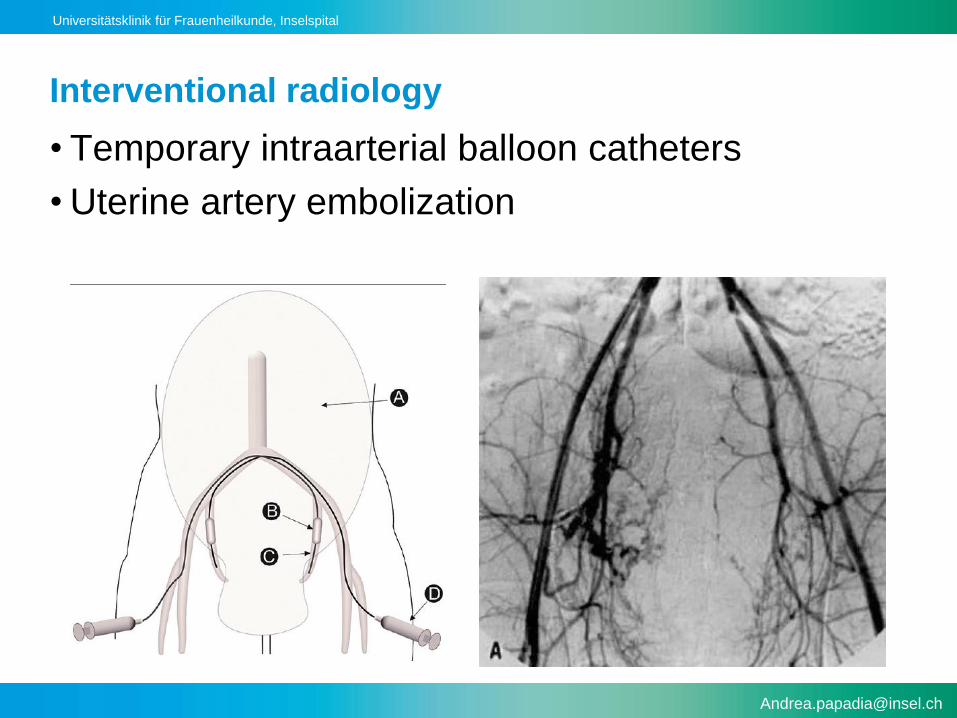
Interventional radiology
• Temporary intraarterial balloon catheters
• Uterine artery embolization
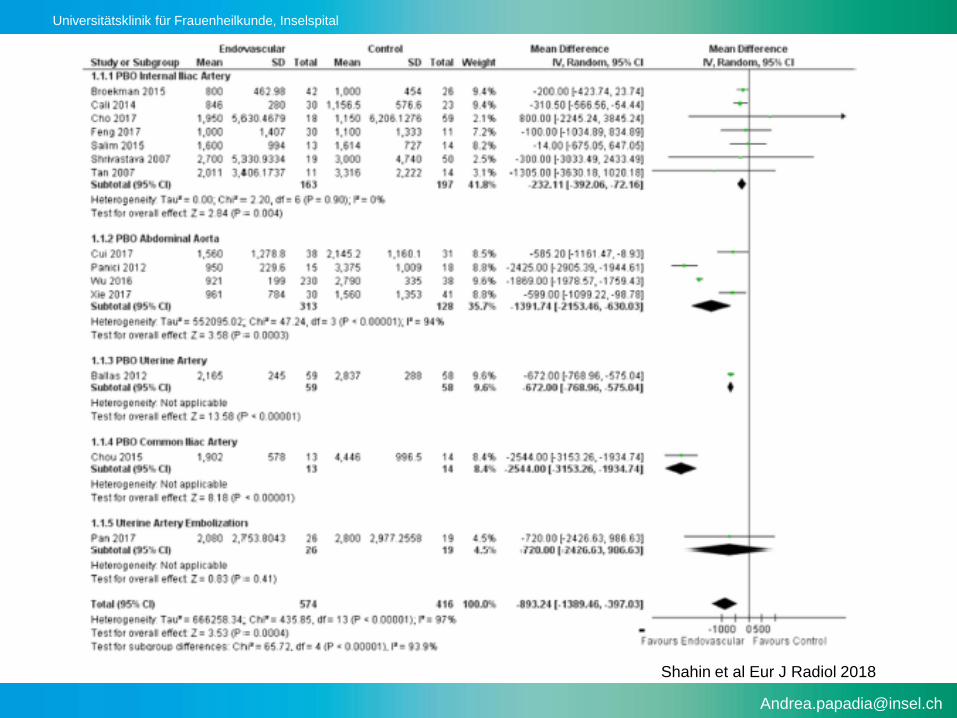
Universitätsklinik für Frauenheilkunde, Inselspital
Shahin et al Eur J Radiol 2018
Universitätsklinik für Frauenheilkunde, Inselspital
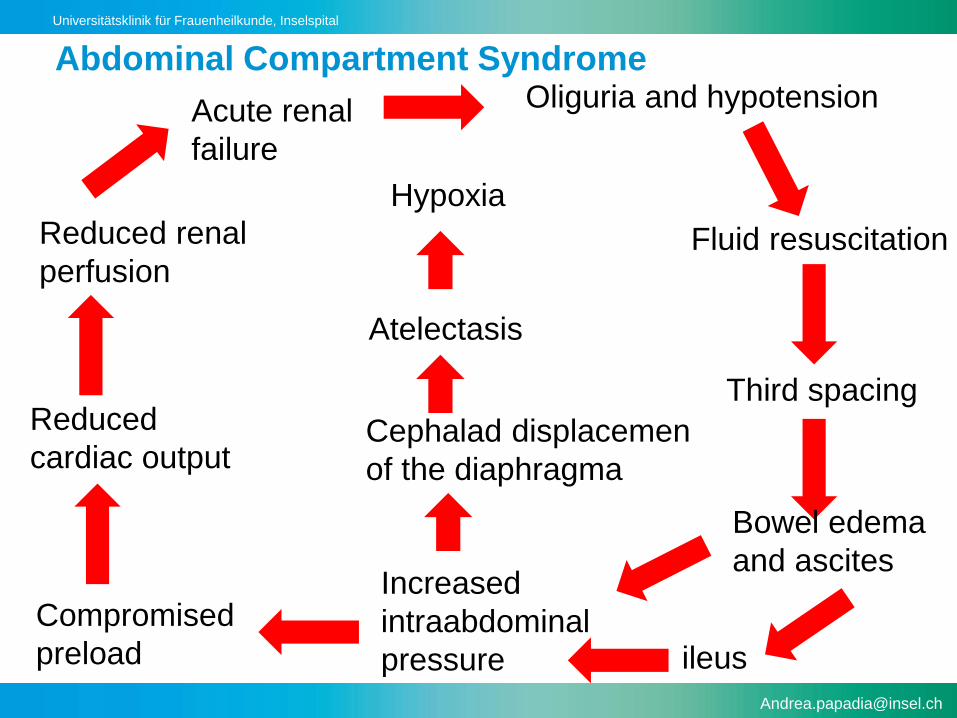
Oliguria and hypotension
Fluid resuscitation
Third spacing
Bowel edema
and ascites
ileus
Increased
intraabdominal
pressure
Compromised
preload
Reduced
cardiac output
Reduced renal
perfusion
Cephalad displacemen
of the diaphragma
Atelectasis
Hypoxia
Acute renal
failure
Abdominal Compartment Syndrome
Universitätsklinik für Frauenheilkunde, Inselspital
The multidisciplinary approach in the
management of a morbidly adherent placenta is a
bundel of interventions
Universitätsklinik für Frauenheilkunde, Inselspital
Conservative management of MAP
• Leave placenta in situ
• Required:
–Hemodinamic stability
–Normal coagulation status
–Willing to accept risks
Universitätsklinik für Frauenheilkunde, Inselspital
Perioperative Outcomes
• PPH: 51.5%
–17.4% controlled medically
–66.2% UAE
–20.9% hysterectomy
• Severe maternal morbidity: 0.6%
–Sepsis
–Vescico-uterine fistula
–Bladder injury during primary hysterectomy
–Thromboembolism
–Death from complications of MTS
Sentilhes et al Obstet Gynecol 2010
Universitätsklinik für Frauenheilkunde, Inselspital
• If there is a strong suggestion of the presence of abnormal placental invasion,
health care providers practicing at small hospitals or at institutions with
insufficient blood bank supply or inadequate availability of subspecialty and
support personnel should consider patient transfer to a tertiary perinatal care
center.
• To enhance patient safety, it is important that the delivery be performed by an
experienced obstetric team that includes an obstetric surgeon, with other
surgical specialists, such as urologists, general surgeons, and gynecologic
oncologists, available if necessary.
Universitätsklinik für Frauenheilkunde, Inselspital
Postpartum considerations
• Increased thromboembolic risk
–Mechanical prophylaxis (SCDs)
–Pharmacologic prophylaxis
• Oliguria and hypotension
–IV fluid administration / boluses
–Third spacing with bowel edema and ascites
– ileus
–Abdominal compartment syndrome
Universitätsklinik für Frauenheilkunde, Inselspital
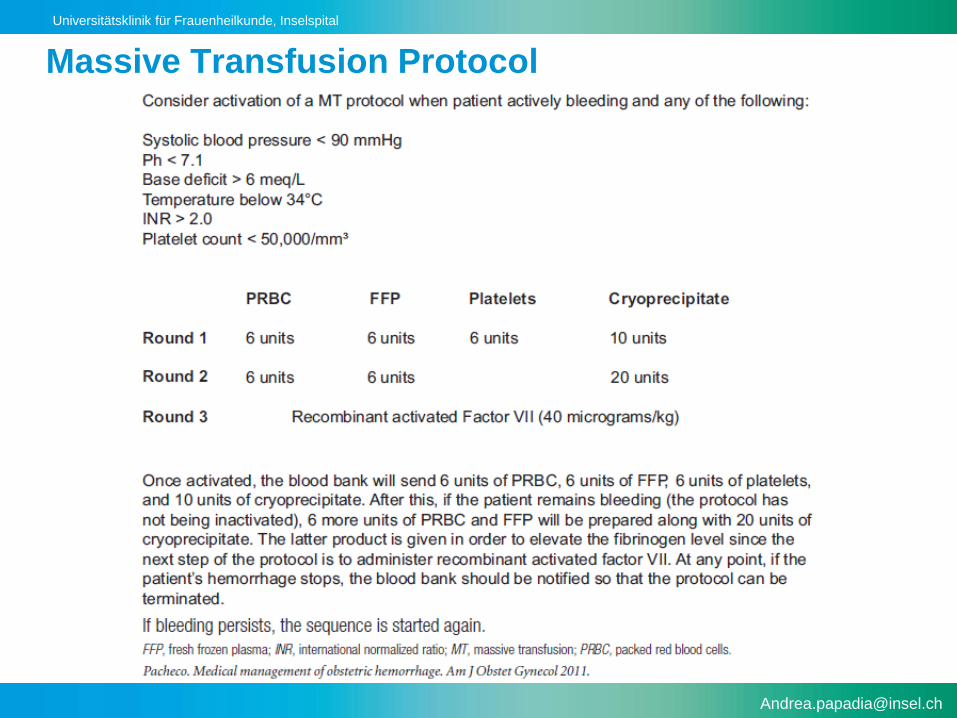
Massive transfusion protocol
• Activated by Obstetrician
–Concerned for massive bleeding
• Managed by anesthesiologist in the OR
–2 large bore I.V. accesses
–Central line
–Arterial line
Universitätsklinik für Frauenheilkunde, Inselspital
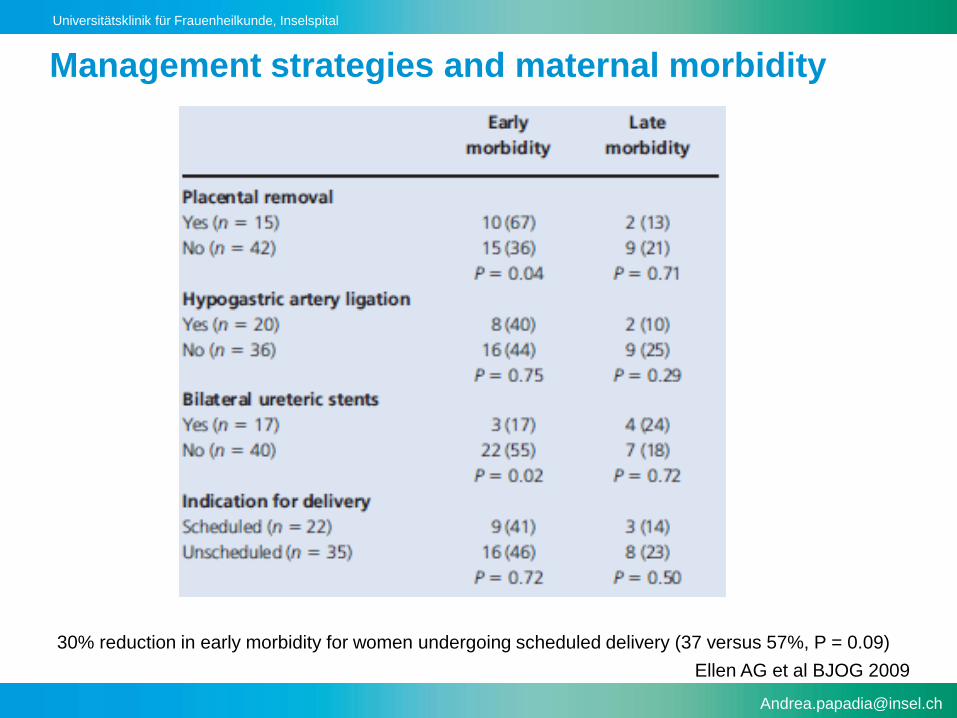
Management strategies and maternal morbidity
Ellen AG et al BJOG 2009
30% reduction in early morbidity for women undergoing scheduled delivery (37 versus 57%, P = 0.09)
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta –
perinatal morbidity
–Placenta accreta associated with increased
perinatal morbidity
–most cases due to PTD
•prompted by vaginal bleeding
OR
•desire to avoid vaginal bleeding and optimize
surgical conditions
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta –
perinatal morbidity
–In fact, iatrogenic preterm birth is advised for
antenatally diagnosed cases of accreta
– In some cases, bleeding may precipitate
abruption and compromise of fetal blood flow
Oyelese Y, Smulian JC: Placenta previa, placenta accreta, and vasa previa. Obstet
Gynecol 2005
Eller AG, Porter TF et al: Optimal management strategies for placenta accreta.
BJOG 2009
Bauer ST, Bonanno C: Abnormal placentation. Semin Perinatol 2009
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta
research summary
(cont)
Outcomes were
improved with
antenatal
diagnosis and
specialized care
Bauer ST, Bonanno C:
Abnormal placentation.
Semin Perinatol 2009
Universitätsklinik für Frauenheilkunde, Inselspital
• Clinically, placenta accreta becomes problematic during
delivery when the placenta does not completely separate
from the uterus and is followed by massive obstetric
hemorrhage
• , leading to
• disseminated intravascular coagulopathy;
• the need for hysterectomy;
• Surgical injury to the ureters, bladder, bowel, or
neurovascular structures;
• adult respiratory distress syndrome;
• acute transfusion reaction;
• electrolyte imbalance;
• and renal failure.
Universitätsklinik für Frauenheilkunde, Inselspital
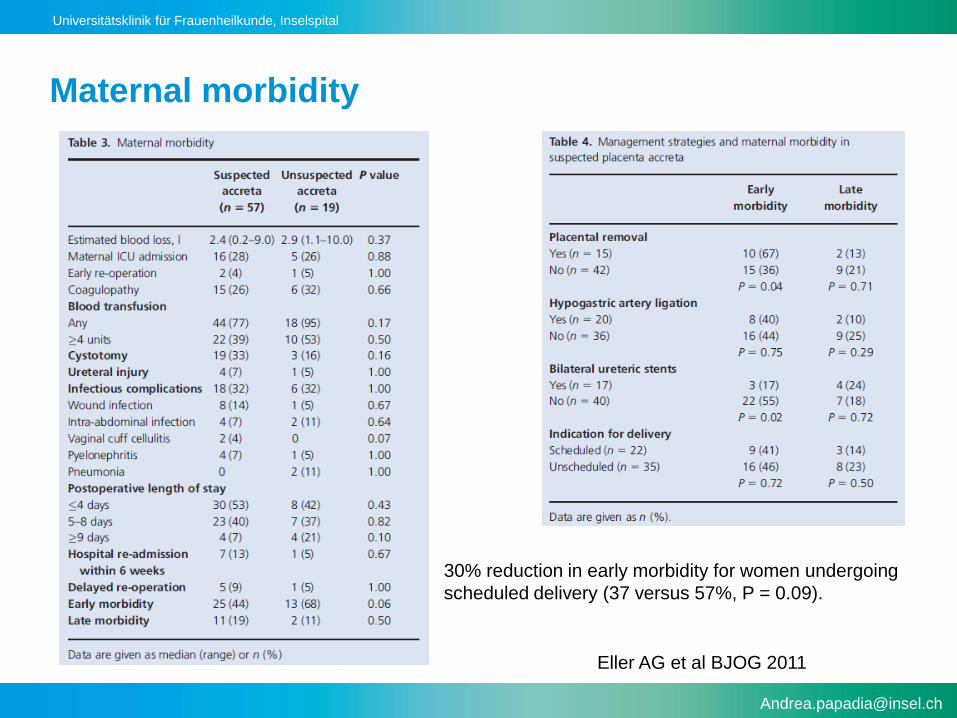
Maternal morbidity
Eller AG et al BJOG 2011
30% reduction in early morbidity for women undergoing
scheduled delivery (37 versus 57%, P = 0.09).
Universitätsklinik für Frauenheilkunde, Inselspital
Anestesiology
• Assessment by the anesthesiologist should occur
as early as possible before surgery.
• Both general and regional anesthetic techniques
have been shown to be safe in these clinical
situations;
• The judgment of which type of technique to be
used should be made on an individual basis.
• Fluid resuscitation and management of
hemorrhagic shock
Universitätsklinik für Frauenheilkunde, Inselspital
Benefit derived from a multidisciplinary approach
• Women managed by a multidisciplinary care team
are less likely to:
–Require large volume transfusion ( 4 uPRBCs)
• 43% vs 61%, p= 0.031
–Reoperation within 7 days of delivery
• 3% vs 36%, p> 0.001
–Experience morbidity (prolonged maternal admission to
ICU, large volume blood transfusion, coagulopathy,
ureteral injury, early reoperation)
• 47% vs 74%, p= 0.26
Eller AG et al 2011
Universitätsklinik für Frauenheilkunde, Inselspital
Blood bank
• Alert the blood bank for a potential massive hemorrhage.
• Current recommendations for blood replacement in trauma
situations suggest a 1:1 ratio of PRBCs to FFP.
• PRBCs and thawed FFP should be available in the
operating room.
• Additional units of blood and coagulation factors should be
infused quickly and as necessitated by the patient’s vital
signs and hemodynamic stability.
Universitätsklinik für Frauenheilkunde, Inselspital
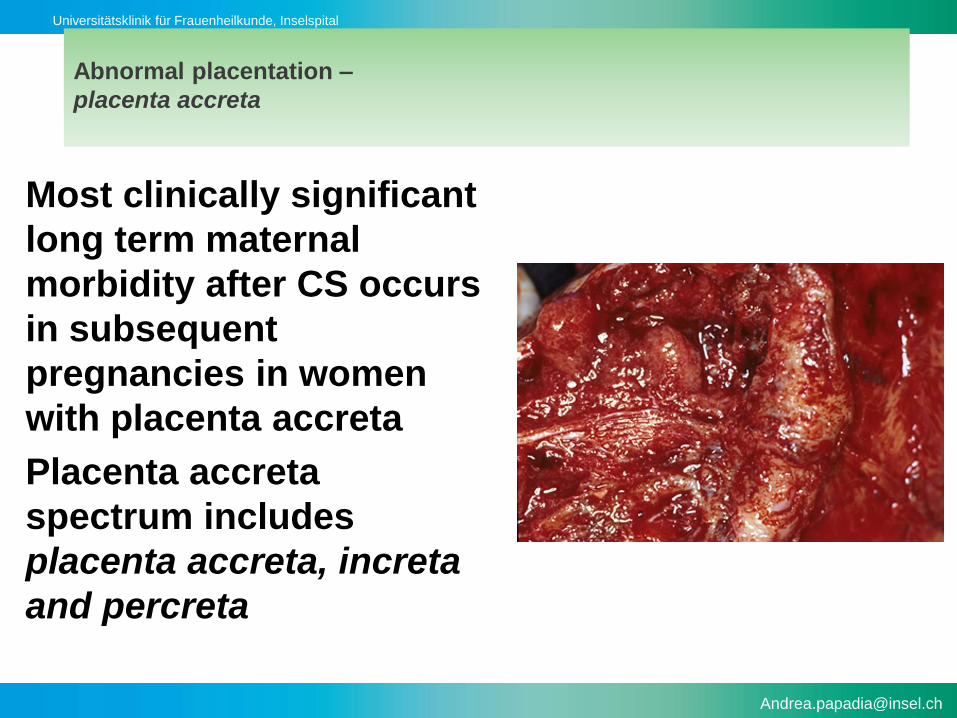
Abnormal placentation –
placenta accreta
Most clinically significant
long term maternal
morbidity after CS occurs
in subsequent
pregnancies in women
with placenta accreta
Placenta accreta
spectrum includes
placenta accreta, increta
and percreta
Universitätsklinik für Frauenheilkunde, Inselspital
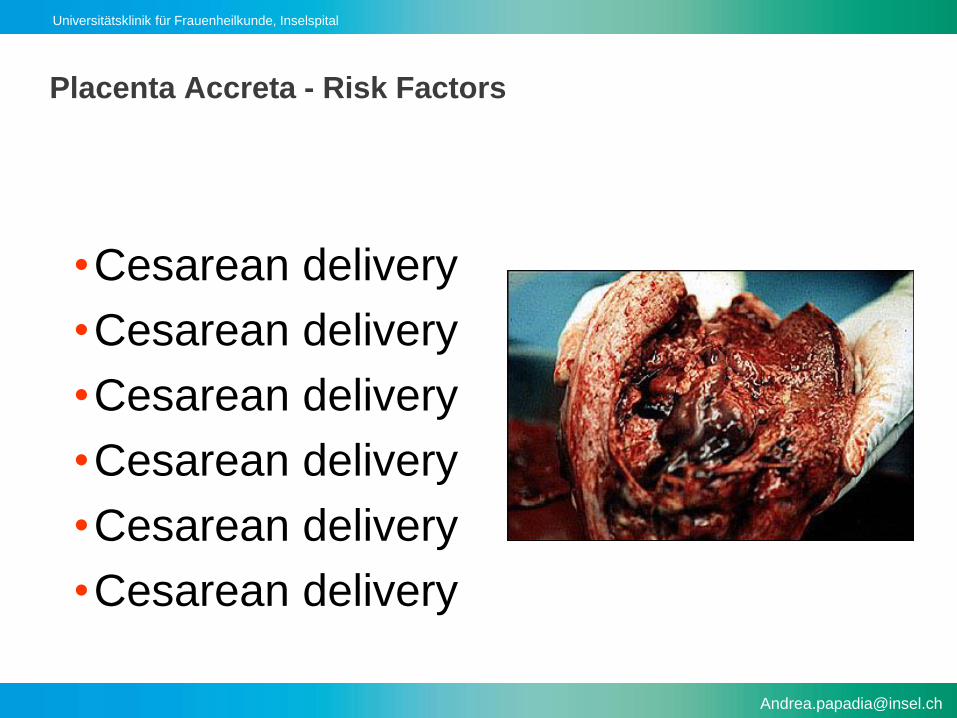
Placenta Accreta - Risk Factors
•Cesarean delivery
•Cesarean delivery
•Cesarean delivery
•Cesarean delivery
•Cesarean delivery
•Cesarean delivery
Universitätsklinik für Frauenheilkunde, Inselspital
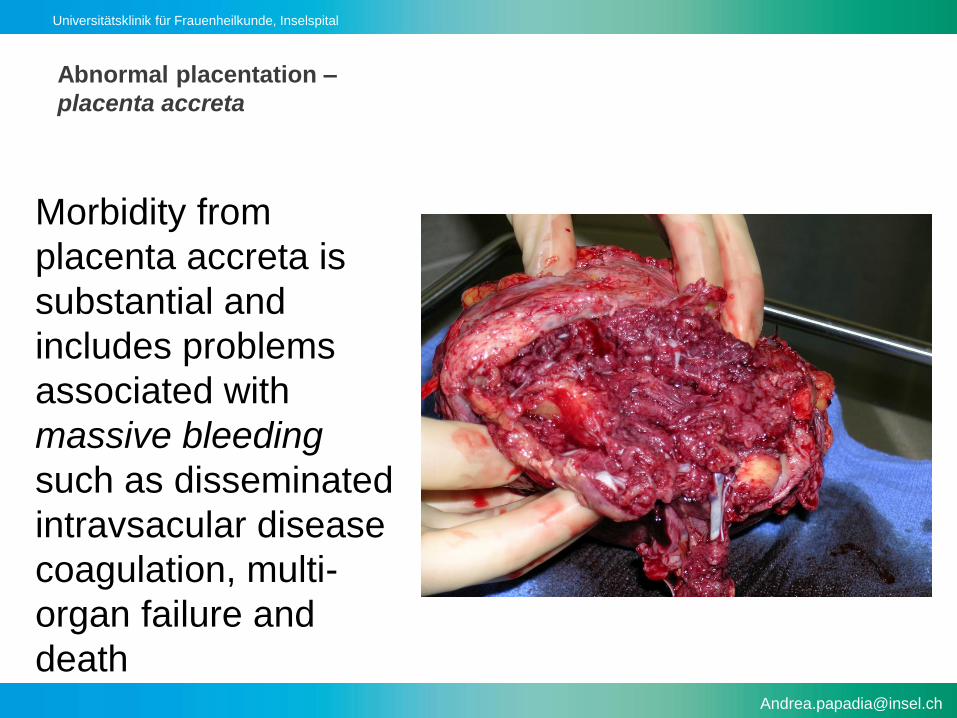
Abnormal placentation –
placenta accreta
Morbidity from
placenta accreta is
substantial and
includes problems
associated with
massive bleeding
such as disseminated
intravsacular disease
coagulation, multi-
organ failure and
death
Universitätsklinik für Frauenheilkunde, Inselspital
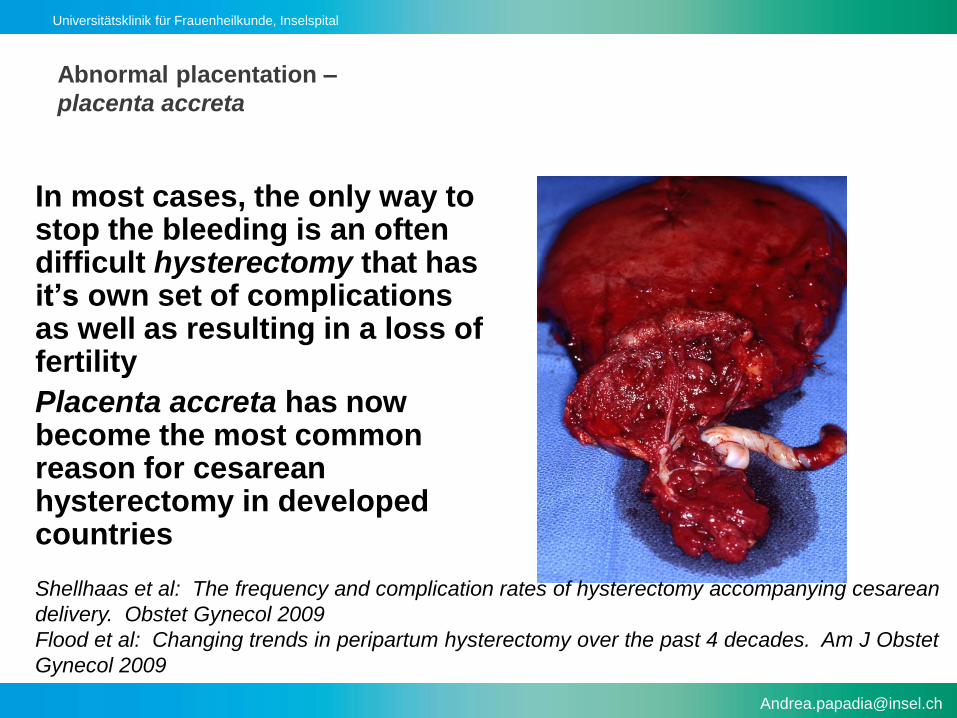
Abnormal placentation –
placenta accreta
In most cases, the only way to stop the bleeding is an oftendifficult hysterectomy that has it’s own set of complications as well as resulting in a loss of fertility
Placenta accreta has nowbecome the most commonreason for cesareanhysterectomy in developedcountries
Shellhaas et al: The frequency and complication rates of hysterectomy accompanying cesarean
delivery. Obstet Gynecol 2009
Flood et al: Changing trends in peripartum hysterectomy over the past 4 decades. Am J Obstet
Gynecol 2009
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta
research summary
•Case series (n=76)
Blood transfusion required in over 80%
Transfusion of 4 units of packed red blood
cells in over 40% of cases
Eller et al: Optimal management strategies for placenta accreta. BJOG 2009
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta
research summary (cont)
• Literature review
–Average blood loss 3,000 – 5,000 mL at the time of delivery
–Most common surgical complication cystotomy(often intentional)
–Ureteral injury in 10 – 15% of cases
–Less common injuries to bowel, pelvic nerves and large vessels and vesico-vaginal fistulas
Hudon L et al: Diagnosis and management of placenta percreta: a review. Obstet GynecolSurv 1998
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta
research summary (cont)
• Prospective cohort study 1999-2002 from NIH/MFM Cesarean Registry Study
– 19 Academic medical centers
– 378,168 births• 57,068 CS• 30,132 CS no labor
– Daily ascertainment of CS
– Trained study nurses
Silver RM,al: Maternal morbidity associated with multiple cesarean deliveries. Obstet Gynecol 2006
Universitätsklinik für Frauenheilkunde, Inselspital
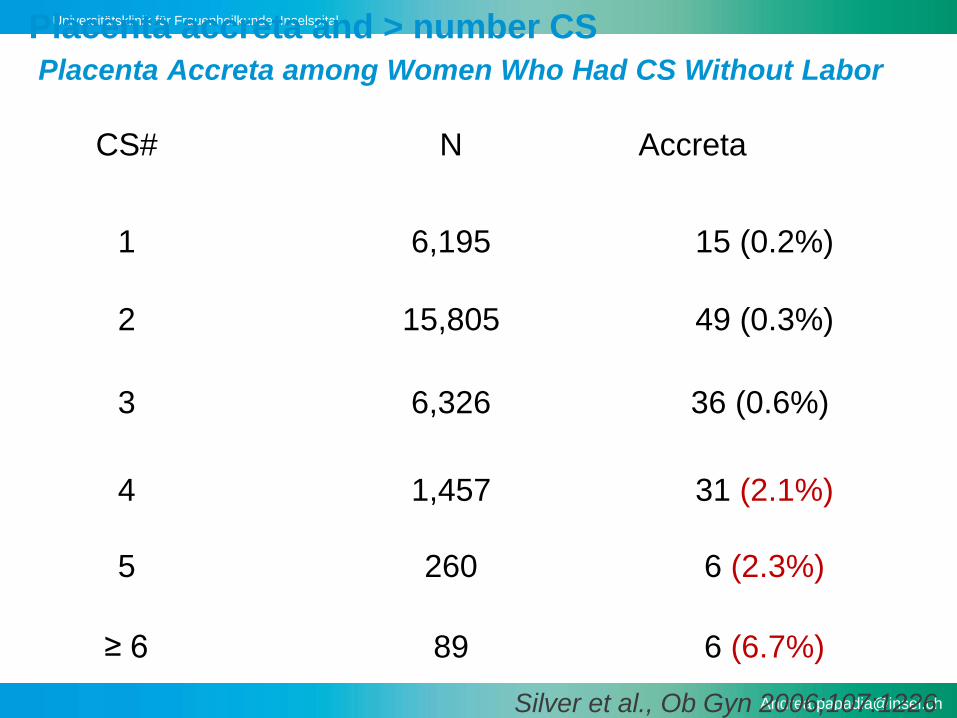
Placenta accreta and > number CS
Placenta Accreta among Women Who Had CS Without Labor
CS# N Accreta
1
2
3
4
6,195
15,805
6,326
260
15 (0.2%)
49 (0.3%)
36 (0.6%)
6 (2.3%)5
1,457 31 (2.1%)
≥ 6 89 6 (6.7%)
Silver et al., Ob Gyn 2006;107:1226
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta and > number CS
research summary
• Combination of placenta previa and prior cesarean
delivery dramatically increases the risk for placenta
accreta
Silver et al: Maternal morbidity associated with multiple cesarean deliveries.
Obstet Gynecol 2006
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta and > number CS
research summary
• In the 723 women in the cohort with placenta previa
– accreta occured in 3%, 11%, 40%, 61% and 67% in
those having their first, second, third, fourth, and fifth
or greater CS respectively
Silver et al: Maternal morbidity associated with multiple cesarean deliveries. Obstet
Gynecol 2006
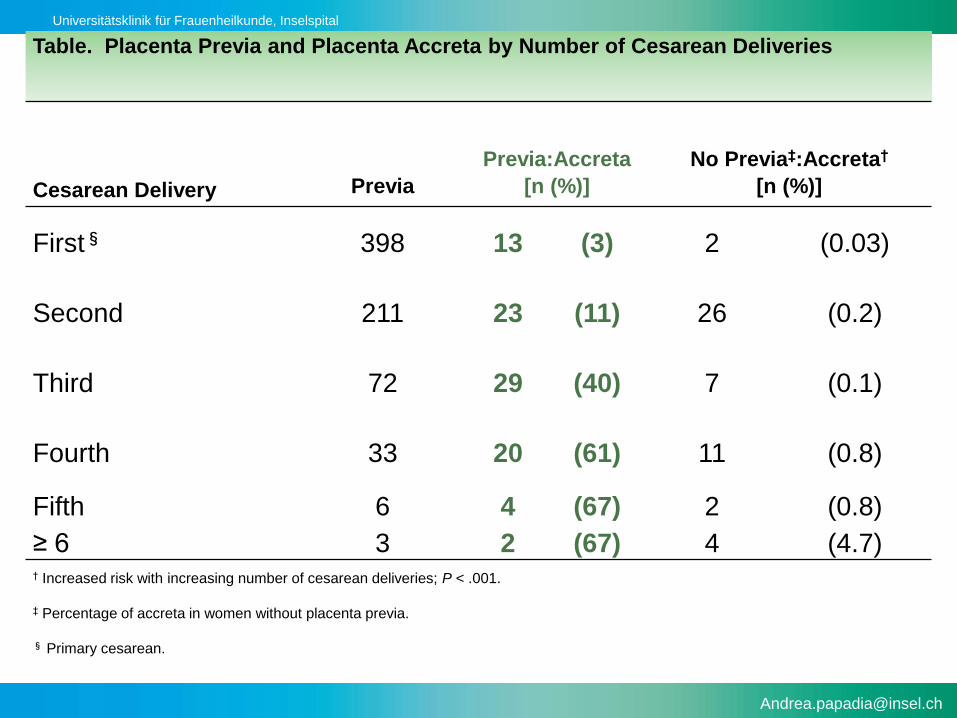
Universitätsklinik für Frauenheilkunde, Inselspital
Table. Placenta Previa and Placenta Accreta by Number of Cesarean Deliveries
Previa:Accreta No Previa‡:Accreta†
Cesarean Delivery Previa [n (%)] [n (%)]
First§ 398 13 (3) 2 (0.03)
Second 211 23 (11) 26 (0.2)
Third 72 29 (40) 7 (0.1)
Fourth 33 20 (61) 11 (0.8)
Fifth 6 4 (67) 2 (0.8)
≥ 6 3 2 (67) 4 (4.7)† Increased risk with increasing number of cesarean deliveries; P < .001.
‡ Percentage of accreta in women without placenta previa.
§ Primary cesarean.
Universitätsklinik für Frauenheilkunde, Inselspital
Placenta accreta –
maternal comorbidity
research summary (cont)
–25 to 50% of women required admission to an intensive care
–Increased risk of thromboembolism, pyelonephritis, pneumonia, wound and pelvicinfections, need for a second operation to control bleeding or treat infection
Silver et al: Maternal morbidity associated with multiple cesarean deliveries. Obstet Gynecol 2006
Universitätsklinik für Frauenheilkunde, Inselspital
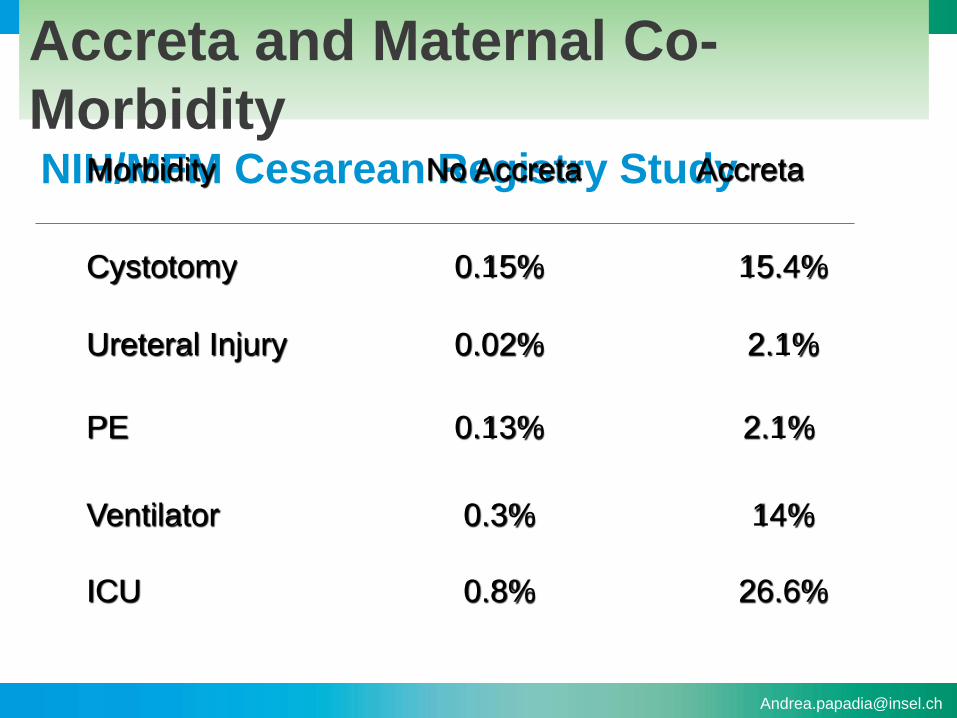
Accreta and Maternal Co-
MorbidityNIH/MFM Cesarean Registry StudyMorbidity No Accreta Accreta
Cystotomy
Ureteral Injury
PE
Ventilator
0.15%
0.02%
0.13%
0.8%
15.4%
2.1%
2.1%
26.6%ICU
0.3% 14%
Universitätsklinik für Frauenheilkunde, Inselspital
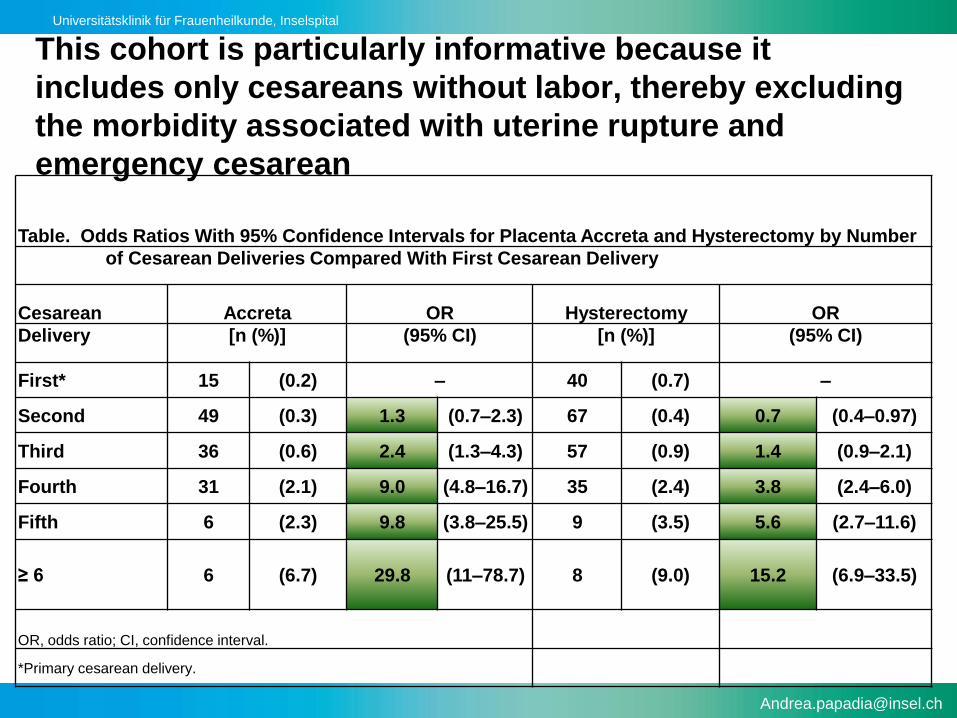
Table. Odds Ratios With 95% Confidence Intervals for Placenta Accreta and Hysterectomy by Number
of Cesarean Deliveries Compared With First Cesarean Delivery
Cesarean Accreta OR Hysterectomy OR
Delivery [n (%)] (95% CI) [n (%)] (95% CI)
First* 15 (0.2) – 40 (0.7) –
Second 49 (0.3) 1.3 (0.7–2.3) 67 (0.4) 0.7 (0.4–0.97)
Third 36 (0.6) 2.4 (1.3–4.3) 57 (0.9) 1.4 (0.9–2.1)
Fourth 31 (2.1) 9.0 (4.8–16.7) 35 (2.4) 3.8 (2.4–6.0)
Fifth 6 (2.3) 9.8 (3.8–25.5) 9 (3.5) 5.6 (2.7–11.6)
≥ 6 6 (6.7) 29.8 (11–78.7) 8 (9.0) 15.2 (6.9–33.5)
OR, odds ratio; CI, confidence interval.
*Primary cesarean delivery.
This cohort is particularly informative because it
includes only cesareans without labor, thereby excluding
the morbidity associated with uterine rupture and
emergency cesarean
Universitätsklinik für Frauenheilkunde, Inselspital
Abnormal placental attachment
• First described in 1937 by Irving and Hertig
–Placenta accreta is the «abnormal adherence, either in whole
or in part of the afterbirth to the underlying uterine wall»
• Placenta accreta (75-78%): Abnormal attachment of the
placental villi directly to the myometrium due to an absence
of decidua basalis and an incomplete development of the
fibrinoid layer