Embed Size (px)
Citation preview

i
Web Annex 6. Decision-making table, PICO question on children and adolescents In: Guidelines for the care and treatment of persons diagnosed with chronic hepatitis C virus infection
July 2018

ii
WHO/CDS/HIV/18.40 © World Health Organization 2018 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. Web Annex 6. Decision-making table, PICO question on children and adolescents. In: Guidelines for the care and treatment of persons diagnosed with chronic hepatitis C virus infection. Geneva: World Health Organization; 2018 (WHO/CDS/HIV/18.40). Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris. Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing. Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
This publication forms part of the WHO guideline entitled Guidelines for the care and treatment of persons diagnosed with chronic hepatitis C virus infection. It is being made publicly available as supplied by those responsible for its development for transparency purposes and information, as required by WHO (see the WHO handbook for guideline development, 2nd edition (2014)).

iii
Acknowledgement The World Health Organization (WHO) wishes to express its appreciation to the following individuals, who contributed to the development of this document: Marc Bulterys, WHO, Geneva, Switzerland; Roger Chou, Oregon Health and Science University, Portland, United States of America (USA); Philippa Easterbrook, WHO, Geneva, Switzerland.

1
PICO question 1a and 2a: ADOLESCENTS AND CHILDREN When to start? What is the optimal timing to start treatment for chronic hepatitis C infection in adolescents and children?
Which drug to use? Which DAA regimen should be used for treatment of chronic hepatitis C infection in adolescents and children?
PICOT1a question Population: adolescents (12–18 years) and children (3–12 years) from 3 to 18 years with chronic hepatitis C infection Intervention: treatment in adolescents only >12 years
Comparison: initiation of treatment using direct-acting
antiviral (DAA)- or interferon (IFN)-based regimen in all
adolescents and children >3 years
Outcomes: viral cure (sustained virological response
[SVR]12), adverse events, discontinuation, drug resistance,
clinical outcomes, quality of life, pharmacokinetic (PK)
equivalence, transmission, costs, cost–effectiveness
PICOT2a question Population: adolescents and children from 3 to 18 years with chronic hepatitis C infection Intervention: initiation of treatment using specific DAA-based
regimens
Comparison: treatment using non-DAA IFN-based regimens
Outcomes: viral cure (SVR12), adverse events, discontinuation, drug resistance, clinical outcomes, quality of life, PK equivalence, transmission, costs, cost–effectiveness Subanalysis: by specific DAA regimen
A. BACKGROUND Epidemiology and burden
It is estimated that around 3.5 million children aged 1–19 years are living with chronic HCV worldwide. Nineteen countries account for the majority of infections.
Mother-to-child transmission is the leading source of HCV infection in children, although other modes of acquisition may also occur, including nosocomial transmission (e.g. through blood transfusions or unsafe injections) and injecting drug use in adolescents.
While well more than a million HCV-infected people have been treated globally, few of these are adolescents or children. There are concerns that children are being left behind in the HCV treatment revolution (as occurred with HIV antiretroviral (ARV) treatment scale up).
Natural history
Around 7–20% of children will experience spontaneous viral clearance, but most HCV-infected children will become chronically infected, based on European studies (Bortolotti, 2008; European Paediatric HCV network, 2005; Casetellino, 2004).
Progression of liver fibrosis to cirrhosis is infrequent in children (around 2–3%) and few will experience end-stage liver disease during childhood, based on prospective studies (Bortolotti, 2008). There are isolated case reports of children with cirrhosis aged as young as 3 or 4 years, and rare cases of hepatocellular carcinoma (HCC) in adolescence (Gonzalez-Peralta, 2009).
However, hepatic fibrosis may progress during childhood: among 44 children with repeated liver biopsies in the PEDS-C trial (mean 6 years interval), around one third showed an increase in the severity of hepatic fibrosis, and the proportion with bridging fibrosis/cirrhosis doubled from 11% to 20% (Mohan, 2013).
Groups at increased risk of more rapid disease progression include children with thalassaemia major, where hepatic iron overload contributes to progression of fibrosis (Elalfy, 2013), children with HIV coinfection (Claret-

2
Teruel, 2011) and childhood cancer survivors (Castellino, 2004).
Although few children will experience end-stage liver disease during childhood, they are at risk of cirrhosis and HCC in early adulthood, given that development of liver fibrosis directly correlates with increasing age and duration of infection (Guido, 2003).
Extrahepatic manifestations: knowledge is limited of the medium- to long-term impact of HCV-related inflammation on extrahepatic manifestations in children. Development of non-organ-specific autoantibodies and subclinical hypothyroidism are common, and present in young children (Indolfi, 2008).
Other aspects of living with chronic HCV include the fact that the infection may confer a stigma, which can impact on quality of life.
Current treatment options
Despite new DAAs for adults having been available for some time (sofosbuvir was approved in 2013), there has been significant delay in evaluating their use in treating children with chronic HCV infection and, until recently, DAAs had not been licensed for adolescent or paediatric use. The only options for treating children and adolescents were the less effective and more toxic IFN-based therapies.
In 2017, the US Food and Drug Administration (FDA) (April) and European Medicines Agency (EMA) (June/July) approved the fixed-dose combination of sofosbuvir/ledipasvir and combination of sofosbuvir and ribavirin for use in treatment-naive and -experienced adolescents >12 years or weighing >35 kg with chronic HCV genotypes 1, 4, 5 and 6, and genotypes 2 and 3 infection, respectively.
For children less than 12 years, DAAs are still not licensed for use. For children aged 3–12 years, IFNs (IFN α, pegylated [PEG]-IFN α-2a and -2b) and ribavirin (RBV) are still currently the only drugs approved for the treatment of chronic HCV infection. Based on registration trials, a PEG-IFN α-2a/RBV combination was approved by EMA and FDA in December 2009 and December 2008, respectively; and PEG-IFN α-2b/RBV by EMA and FDA in March 2013 and December 2009, respectively. Children with HCV genotype 1 or 4 infection should be treated for 48 weeks and those with genotype 2 or 3 for 24 weeks.
However, results are now also becoming available from clinical studies using DAAs in children aged 6–12 years, showing comparably high rates of sustained virological response (SVR).
Current guidelines based on access to IFN treatment from the North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition recommend that the majority of children can be followed without treatment until adulthood. IFN/RBV treatment should be considered only for the few children with persistently elevated liver enzymes and/or evidence of liver fibrosis (Mack, 2012).
A target product profile for paediatric regimens was established at WHO Paediatric ARV Drug Optimization (PADO) meeting in December 2016 and included: acceptable safety profile; tolerability; efficacy in adult trials with SVR12 >90–95%; palatability and age-appropriate formulations.
DRAFT RECOMMENDATIONS: [to be discussed at Guidelines Development meeting]
ADOLESCENTS ≥12 years
In treatment-naive and -experienced cirrhotic and non-cirrhotic adolescents aged 12 years and above or weighing at least 35 kg with chronic hepatitis C infection we recommend:
o use of sofosbuvir/ledipasvir for 12 weeks for those infected with HCV genotypes 1, 4, 5, or 6 (Strong recommendation, very low quality of evidence)
o use of sofosbuvir and weight-based
CHILDREN <12 years
In children aged less than 12 years with chronic hepatitis C infection we recommend:
o deferral of treatment until aged 12 years prior to approval of DAA regimens for those in age groups less than 12 years (Conditional recommendation, very low, quality of evidence)
o treatment with IFN-based regimens should no longer be used (Strong

3
ribavirin for 12 weeks for those infected with HCV genotype 2, and 24 weeks for genoptype 3 (Strong recommendation, very low quality of evidence)
o Treatment with IFN-based regimens should no longer be used (Strong recommendation, very low quality of evidence)
Note: other DAA regimens can be considered following regulatory approval for use in adolescents or children.
recommendation, very low, quality of evidence)
Note: prior to approval and availability of DAAs for children aged <12 years of age, exceptional treatment with IFN + ribavirin may be considered for those children with genotype 2 or 3 infection, and severe liver disease. This may include children at higher risk of progressive disease, including those with HIV coinfection, thalassaemia major and childhood cancer survivors.

4
B. SUMMARY AND QUALITY OF EVIDENCE
Systematic review and meta-analysis of DAA vs PEG-IFN in adolescents and children A systematic literature search and meta-analysis were performed using MEDLINE and Embase from 1 June 2007 to 1 June 2017. PEG-IFN and ribavirin: eleven trials reporting on combined treatment with PEG-IFN and ribavirin were included. Overall, the efficacy of this combination therapy was higher for children infected with HCV genotypes 2 and 3 (90%) than for those infected with genotypes 1 and 4 (48%). Relapse rate, independent of genotype and treatment duration, was 6%. Treatment discontinuation was reported in 17% of the children treated. Discontinuation due to severe adverse events occurred in 2%. DAA: two trials published as full-length articles and three as abstracts were included. The overall efficacy of the different DAA combinations tested was very high (98%). Relapse rate was low (0.7%) and no treatment discontinuation was reported.
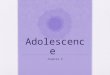
Random-effects proportional meta-analysis for children treated with pegylated interferon and ribavirin (predominantly adolescents)
Outcome Percentage (95% confidence interval)
Number of arms
Sustained virological response
genotypes 1 and 4 48.6 (44.1–53.1) 11
genotypes 2 and 3 90.9 (84.2–95.9) 7
Relapse 6.1 (2.8–10.5) 10
Virological breakthrough 3.4 (0.8–7.7) 8
Treatment discontinuation 17.7 (6.4–33.2) 9
due to lack of virological response
14.9 (15.3–29.3) 9
due to an adverse event 2.4 (1.1–4.3) 11
Random-effects proportional meta-analysis for children treated with direct-acting antivirals (predominantly adolescents)
Outcome Proportion (95% confidence interval)
Number of arms
Sustained virological response 98.1 (96.2–99.3) 5
genotypes 1 and 4 98.2 (96.2–99.5) 4
genotypes 2 and 3 96.9 (90.9–99.8) 2
Relapse 0.7 (0.08–1.9) 5
Virological breakthrough Not calculable 5
Treatment discontinuation Not calculable 5
due to lack of virological response
0 0
due to an adverse event 0 0
Meta-analysis results for SVR in children infected with hepatitis C virus genotypes 2 and 3 (panel A), and 1 and 4 (panel B) treated with pegylated interferon and ribavirin
Meta-analysis results for SVR in children infected with hepatitis C virus (all genotypes) treated with direct-acting antivirals
□ High
□ Moderate
□ Low
X Very low

5
ADDITIONAL TRIAL DATA IN ADOLESCENTS >12 YEARS Sofosbuvir/ledipasvir with genotype 1 The use of fixed-dose combination sofosbuvir/ledipasvir was approved in children aged 1–17 years and ≥35 kg, infected with HCV genotype 1 by the FDA in April 2017, and EMA in June 2017. Study design: this was based on an open-label study of 100 GT1 HCV-infected treatment-naive and -experienced adolescents in the UK, US and Australia. Initial PK lead-in of the first 10 patients was done to confirm the dose (90 mg ledipasvir and 400 mg sofosbuvir once daily). Study population: the median age was 15 (range 12–17) years, median BMI 21 (range 13–37) kg/m
2, infected with genotype 1 (81% 1a, 19% 1b), infected by perinatal transmission
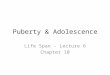
(84%), rate of disease (42% no cirrhosis, 1% yes cirrhosis, 57% unknown) Balistreri et al. 2017). 80 patients were treatment-naive and 20 were treatment-experienced. One out of 42 had cirrhosis. Results: overall, there were high rates of SVR12 (98%, 98/100 patients) (Fig. 1) and good tolerability profiles and satisfactory PK profiles. The AUCtau and Cmax for sofosbuvir, GS-331007, and ledipasvir in adolescents were within the predefined PK equivalence boundaries (50–200%) found in adults in clinical trials. Two patients did not attend the post-treatment follow-up visit after achieving end-of-treatment response and were defined as lost to follow up (LTFU). The most common adverse events were headache (27%), diarrhoea (14%) and fatigue (13%). No serious adverse effects leading to treatment discontinuation were reported. All PK parameters were within the predefined equivalence boundaries when compared to adults from phase 2 and phase 3 trials of the same medications in adults. The same trial is ongoing in children aged 3–12 years. Fig. 1. SVR12 in adolescents with HCV GT1 treated with LDV/SOF FDC
Sofosbuvir/ribavirin with genotypes 2 + 3 The use of sofosbuvir/ribavirin was approved by the FDA for use in children aged 12–17 years and ≥35 kg, infected with HCV genotype 2 or 3 in April 2017.

6
Study design: this was based on an open-label study of the PK, safety and efficacy of sofosbuvir (400 mg) and weight-based dosing (WBD) of ribavirin in 52 treatment-naive and -experienced adolescents aged 12–17 years old (NCT 02175758) at 28 sites in Australia, Germany, Italy, New Zealand, Russiathe Russian Federation, the United Kingdom of Great Britain and Northern IrelandK and the USA (Wirth, 2017). Study population: the median age was 15 (range 12–17) years, median BMI was 22 (range 16–32) kg/m
2, infected with genotype 2 (12%), 2b (10%), 2a/2c (4%), 4 (2%), 3a (71%),
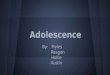
infected by vertical transmission (73%), rate of disease (42% no cirrhosis, 60% unknown as did not have an assessment of stage of liver disease). Results: SVR12 was 98% in the 52 adolescents treated (Fig. 2). The single patient (GT3) who did not obtain SVR12 was LTFU but did achieve SVR4. Nausea (27%) and headache (23%) were the most common adverse events reported. More than 10% of patients also experienced upper abdominal pain, diarrhoea, asthenia and dizziness. Seven patients (19%) experienced a grade 3–4 adverse event, but none discontinued treatment due to this. A small minority experienced transient, mild reductions in haemoglobin, consistent with the toxicity profile of RBV. All PK parameters were within the predefined equivalence boundaries when compared to adults from phase 2 and phase 3 trials of the same medications in adults. The same trial is ongoing in children aged 3–12 years. Fig. 2. SVR12 in adolescents with HCV GT2 and GT3 treated with SOF+RBV
Use of SOF/LED plus RBV in adolescents for treatment-naive non-cirrhotic hepatitis C GT3:
In registration trial (NCT 02249182), only 2 patients with HCV genotype 3 infection were treated with SOF/LED for 12 weeks and achieved SVR12.
The EMA EPARfor Harvoni unclear – “ Harvoni can be used for some patients with genotype 3”. So apparently licensed also for adolescents with HCV genotype 3 infection even though only two have been treated so far.
Published trials in adults (not adolescents or children) (Feld JJ et al. Clin Infect Dis. 2017 May 23. doi: 10.1093/cid/cix289).
PRELIMINARY TRIAL DATA IN CHILDREN <12 YEARS (refer to summary document and presentation at meeting)

7
C. BENEFITS/HARMS
ADOLESCENTS ≥12 years and CHILDREN <12 years
Benefits
Elimination of viral hepatitis as a public health threat in many high-burden
countries will be possible only if children and adolescents can also access highly
effective DAA regimens for treatment and cure.
Highly effective DAA treatment achieves cure rates >97%. Children may have
even better SVR rates than adults.
Early treatment may prevent the development of liver-related complications.
Cognitive functioning, educational attainment and well-being may improve, even if
there are no liver-related symptoms. Both physical and psychosocial health and
cognitive functioning are reduced significantly in infected children compared with
children without HCV (Nydegger, 2008; Rodrigue, 2009; Younossi, 2016), and
may improve with DAAs.
Treatment would reduce horizontal transmission in childhood and adolescence
before the onset of risk behaviours (injecting drug use/sexual transmission).
Treatment would enable a child to live free of a socially stigmatizing infection.
Adults with HCV acquired in childhood are at higher risk of cirrhosis and HCC
than those who acquire infection in adulthood, as liver fibrosis development
directly correlates with increasing age and duration of infection (Guido, 2003).
There was a 26-fold increased risk of liver-related death among HCV-infected
adults with childhood-acquired HCV (Omland, 2010).
It will reduce costs – as it will avoid higher costs of care and treatment associated
with more advanced liver disease in adults.
Although the same dose is used in adolescents as for adults, dosing in children
will be lower, which will reduce costs.
Recommendation and opportunity for treatment in adolescents and children will
encourage testing and case-finding.
It will simplify general population and focused testing strategies as everyone will
be eligible for testing regardless of age.
Inclusion of the recommendation would enable treatment of adolescents to be
included in health insurance cover.
Harms
Some adolescents and children will be diagnosed and treated for an infection that
is currently causing no symptoms, which may create anxiety.
x Benefits clearly outweigh
harms
□ Benefits and harms are
balanced
□ Potential harms clearly
outweigh potential benefits
Are the desirable anticipated
effects large?
x No
□ Probably
□ Uncertain
□ Yes
□ Varies
ADOLESCENTS >12 years for use of
SOF/LED and SOF/RBV
Harms
Existing recommended regimens
are not pangenotypic and
therefore genotyping still required
RBV: use of RBV-based regimen
is suboptimal, requiring
haematological monitoring
RBV: unknown safety in
CHILDREN <12 years: deferral of treatment until DAAs approved for 6–12 years age group
Benefits of deferral
Significant liver disease rare in childhood
Therapeutic superiority of DAA
regimens for all GTs and better safety
profile, when compared to IFN-based
regimens

8
pregnancy and in age group more likely to have unplanned pregnancies
Only one IFN-free option for GT 2/3 and SOF/RBV not a good regimen for GT 3 plus cirrhosis and GT2
Consider SOF/LED plus RBV for GT3. EMA European public assessment reports (EPAR) for Harvoni unclear – “ Harvoni can be used for some patients with genotype 3”. So licensed also for adolescents with HCV genotype 3 infection.
Only available and approved regimen for this age group is PEG-IFN and RBV, which has well-known toxicities (including growth deficits in children), inconvenient administration route via subcutaneous IFN injections, poor efficacy and requires long duration of treatment, i.e. 6–12 months.
Burdensome on-therapy and after-therapy safety profile of PEG-IFN and RBV. On-therapy side-effects include flu-like symptoms, e.g. fever, decreased appetite, asthenia and fatigue, and haematological complications such as anaemia, leukopenia and neutropenia. Potential irreversible after-therapy side-effects, such as thyroid disease, diabetes, ophthalmological complications and (including growth deficits in children), impairment of growth (Wirth, 2005; Jara, 2008; Narkewicz, 2010; Kelly, 2012; Jonas, 2012) means low benefit–risk ratio for treatment in children.
General deferral of treatment until adulthood is current norm in paediatric treatment guidelines from Europe and United States.
Recommended deferral now only until 12 years, minimizing time for disease progression and transmission.
Potentially avoid current need for liver biopsy with use of non-invasive tests (NITs) for staging in adolescence. Harms from deferral
Progression of liver fibrosis may occur during childhood: approximately one third of children with repeat biopsies showed an increase in severity of fibrosis and in the proportion with bridging fibrosis/cirrhosis (11–20%) (Mohan, 2013).
In some children, development of advanced liver disease can be fast and unpredictable (Badizadegan, 1998; Bortollotti, 2008).
Physical and psychosocial health and cognitive function of even asymptomatic HCV-infected children is significantly reduced compared with children without HCV (Nydegger, 2008; Rodrigue, 2009; Haber, 2017) and would likely benefit from early therapy.
D. ACCEPTABILITY, VALUES AND PREFERENCES
Parental support for early treatment. Views of adolescents uncertain, but with short-course treatment likely to be highly acceptable.
xNo major variability
□ Major variability
Is the option acceptable
to key stakeholders?

9
Children supported by their parents generally have excellent compliance with treatment.
□ No
x Probably
□ Uncertain
□ Yes
□ Varies
E. EQUITY, ETHICS AND HUMAN RIGHT IMPLICATIONS Will the recommendation raise questions around equity?
With more than 1 million adults who have received new HCV treatment, it is important that children and adolescents are now able to benefit from this curative treatment as quickly as possible, and enable discontinuation of less effective and more toxic IFN-based therapies. Are there ethical implications to this recommendation?
Ensure that children and adolescents are fully informed. The consent of parent or legal
guardian and assent of adolescent or child is required.
□ Less equitable
x More equitable
F. RESOURCE USE AND FINANCIAL IMPLICATIONS
The costs are decreasing in high-, middle- and low-income countries (cite WHO
HCV Treatment access report 2018 for current costs)
Costs of care and treatment in children are lower as reduced dose, fewer
comorbidities, fewer cases of cirrhosis and potentially shorter treatment.
Cost effective – as will avoid higher costs of care and treatment associated with
more advanced liver disease in adults
Are the resources required
small?
□ No
□ Probably
□ Uncertain
□ Yes
x Varies
G. FEASIBILITY AND CONSTRAINTS TO IMPLEMENTATION
Majority of those infected are undiagnosed. Very few adolescents or children are being tested and diagnosed. In a recent US study (HCV prevalence in children 0.2–0.4%, only 1 in 7 children with HCV were identified and <2% were offered treatment (Delgado-Borrego, 2012). Reasons include lack of awareness about opportunities for HCV cure among adolescents in the population, and among health-care workers.
Few low- or middle-income countries have included testing or treatment of adolescents or children in their national guidelines.
Low- and middle-income countries with already significant financial constraints on treatment scale up may be unwilling to extend treatment to adolescents in the initial phase of scaling up.
1. RELEVANCE TO DIFFERENT SETTINGS/POPULATIONS
Are any major barriers expected for the implementation of this recommendation?
Will this recommendation be most relevant for particular settings (e.g. endemicity)?
Relevant to all high-burden settings. About 19 countries account for 80% of the
burden. Highest-burden countries for paediatric infection include Pakistan, Egypt,
Nigeria, China, Russia, Indonesia and Ukraine.
In a large number of LMICs, including those with a high HCV prevalence, almost
half of the population is under 25 years of age. Therefore, even if prevalence is
low, they constitute a significant proportion of the infected population.
Is the option feasible to
implement?
□ No
x Probably
□ Uncertain
□ Yes
□ Varies

10
H. DRAFT RECOMMENDATIONS:
ADOLESCENTS ≥12 years
In adolescents aged 12 years and above or weighing at least 35 kg with chronic hepatitis C infection (treatment-naive and -experienced cirrhotic and non-cirrhotic) we recommend:
o use of sofosbuvir/ledipasvir for 12 weeks for those infected with HCV genotypes 1, 4, 5 or 6 (Strong recommendation, very low quality of evidence)
o use of sofosbuvir and weight-based RBV for 12 weeks for those infected with HCV genotype 2 and 24 weeks for those infected with genoptype 3 (Strong recommendation, very low quality of evidence)
o Treatment with IFN-based regimens should no longer be given (Strong recommendation, very low quality of evidence)
CHILDREN <12 years
In children aged less than 12 years with chronic hepatitis C infection we recommend: o deferral of treatment until aged 12 years prior to approval of DAA regimens for those in age
groups less than 12 years (Conditional recommendation, very low, quality of evidence) o Treatment with IFN-based regimens should no longer be given (Strong recommendation, very
lowquality of evidence)
Note. Prior to approval and availability of DAAs for children <12 years of age, exceptional treatment with IFN + RBV may be considered for those children with genotype 2 or 3 infection and severe liver disease. This may include children at higher risk of progressive disease, including those with HIV coinfection, thalassaemia major and childhood cancer survivors. Note. Other DAA regimens can be considered following regulatory approval for use in adolescents or children. I. STRENGTH OF RECOMMENDATION
As above, and see GRADE tables below and attached.
J. RATIONALE FOR RECOMMENDATION:
Both ADOLESCENTS ≥12 years and CHILDREN <12 years
Goal of treatment in childhood is prevention of HCV-associated liver damage and extrahepatic disease, and to achieve an HCV-free generation of children
On the basis of adult clinical trials of DAA regimens, there is a potential to cure paediatric HCV in the vast majority of children treated.
Elimination of viral hepatitis as a public health threat will be possible only if adolescents and children with chronic hepatitis C can also benefit from treatment and cure. Viral eradication means that a child can live free of a socially stigmatizing infection.Will align with forthcoming US and European recommendations (AASLD/IDSA and European Society for Pediatric Gastroenterology, Hepatology and Nutrition).
Overall benefits of treatment of all infected adolescents and children outweigh the risks, as costs continue to
decrease in high-, middle- and low-income countries.
ADOLESCENTS ≥12 years or weighing at least 35
kg: SOF/LED or SOF/RBV
Comparable outcomes in adolescents to adults in two published trials: comparable high SVR rates (98% for GT1/4; 100% for GT2 and 97% for GT3). No serious adverse events or significant laboratory abnormalities with SOF/LED and SOF/RBV.
European Medicines Agency (EMA) and the Food and Drug Administration (FDA) approval in 2017 of two regimens for treatment of adolescents (12–17 years, weighing more than 35 kg: (fixed-dose combination SOF/LED and combination of SOF/RBV)
CHILDREN <12 years: recommendation for deferral until
12 years and not use IFN-based regimens
Overall low efficacy, prolonged treatment duration of IFN-based treatments (24–48 weeks), and significant side-effect profile, including growth deficits that are unique to children), inconvenient administration route via subcutaneous IFN injections, and high cost.
IFN increasingly less available, especially in LMICs
Current approach is to defer treatment until aged 12 years or until the new highly effective short-course oral DAA regimens become available.

11
for GTs 1, 4, 5 and 6, and GTs 2 and 3 infections, respectively.
SOF/LED and SOF/RBV fulfil criteria for TPP identified at PADO meeting (December 2016)
- Acceptable safety profile - Tolerability - Efficacy SVR12 >95%
Only a small number of children have significant liver disease that would benefit from early treatment.
K. IMPLEMENTATION CONSIDERATIONS 1. Need for adoption of 2017 WHO testing guideline recommendations for adolescents and children in
national testing and treatment guidelines. As all adolescents and children, regardless of age, stage of disease, risk group, become potential candidates for treatment with approved effective DAA regimens, there is a need to scale up testing to identify undiagnosed cases.
2 Includes those who are either part of a population with higher seroprevalence (e.g. some mobile/migrant populations from high/intermediate endemic countries, and certain indigenous populations) or who have a history of exposure or high-risk behaviours for HCV infection (e.g. PWID, people in prisons and other closed settings, MSM and sex workers, and HIV-infected persons, children of mothers with chronic HCV infection, especially if HIV-coinfected).
2. Future drug development and approval Opportunity to accelerate evaluation and approval of future paediatric drug regimens through revised EMA approach to registration of DAA regimens for paediatric use (EMA Expert meeting on the clinical investigation of medicines for the treatment of paediatric hepatitis C (www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/events/2014/12/event_detail_001074.jsp&mid=WC0b01ac), such that regimens Drugs can now be approved on the basis of phase I/II clinical studies of 30–40 children. Uncertain whether FDA will follow the same path. Given the expected high efficacy of the multiple DAA regimens approved in adults and in development, comparative trials are unrealistic and may be unnecessary. Can extrapolate data from adult clinical trials and define what criteria should be applied in selecting the most promising regimens for treating children. Base approval on pre-authorization phase I/II clinical studies of 30–40 children, with PK and limited tolerability and efficacy data. Post-licensure and approval, safety and efficacy studies can collect longer-term and more detailed data.
3. Palatability and age-appropriate formulations need to be prioritized and developed.
L. RESEARCH GAPS
Ongoing studies with DAAs in children and adolescents with chronic HCV infection (last update August 2017)
Combined regimens Genotype Identifier Expected completion
glecaprevir/pibrentasvir 1–6 NCT 03067129 May 2022
ombitasvir/paritaprevir/ritonavir ± dasabuvir ± ribavirin
1, 4 NCT 02486406 September 2019
sofosbuvir + daclatasvir 4 NCT 03080415 June 2018
ledipasvir/sofosbuvir * 1, 4 NCT 02868242 April 2019
ledipasvir/sofosbuvir ± ribavirin 1, 4, 5, 6 NCT 02249182 July 2018

12
References
Badizadegan K, Jonas MM, Ott MJ, Nelson SP, Perez-Atayde AR (1998). Histopathology of the liver in children with chronic hepatitis C viral infection. Hepatology. 28:1416–23. Balistreri WF, Murray KF, Rosenthal P, Bansal S, Lin CH, Kersey K et al. (2017). The safety and effectiveness of ledipasvir-sofosbuvir in adolescents 12-17 years old with hepatitis C virus genotype 1 infection. Hepatology. 66(2):371–-378. doi: 10.1002/hep.28995. Epub 2017 Jun 19. Bortolotti F, Verucchi G, Camma C, Cabibbo G, Zancan L, Idolfi G et al. (2008). Long-term course of chronic hepatitis C in children: from viral clearance to end-stage liver disease. Gastroenterology. 134:1900–7. [PubMed] Castellino S, Lensing S, Riely C, Rai SN, Davila R, Hayden RT et al. (2004). The epidemiology of chronic hepatitis C infection in survivors of childhood cancer: an update of the St Jude Children's Research Hospital hepatitis C seropositive cohort. Blood. 103:2460–6. [PubMed] Claret-Teruel G, Noguera-Julian A, Esteva C, Munoz-Almagro C, Sanchez E, Jiminez R et al. (2011). Impact of human immunodeficiency virus coinfection on the progression of mother-to-child transmitted hepatitis C virus infection. Pediatr Infect Dis J. 30:801–4. [PubMed] Delgado-Borrego A, Smith L, Jonas MM, Hall CA, Negre B, Jordan SH et al. (2012). Expected and actual case ascertainment and treatment rates for children infected with hepatitis C in Florida and the United States: epidemiologic evidence from statewide and nationwide surveys. J Pediatr. 161:915– 21. [PubMed] Elalfy MS, Esmat G, Matter RM, Abdel Aziz HE, Massoud WA et al. (2013). Liver fibrosis in young Egyptian beta-thalassemia major patients: relation to hepatitis C virus and compliance with chelation. Ann Hepatol. 12:54– 61. [PubMed] European Paediatric Hepatitis C Virus Network (2005). Three broad modalities in the natural history of vertically acquired hepatitis C virus infection. Clin Infect Dis. 41:45– 51. [PubMed] Gonzalez-Peralta RP, Langham MR Jr, Andres JM, Mohan P, Colombani PM, Alford MK et al. (2009). Hepatocellular carcinoma in 2 young adolescents with chronic hepatitis C. J Pediatr Gastroenterol Nutr. 48:630–5. [PubMed] Guido M, Bortolotti F, Leandro G, Jara P, Hierro L, Larrauri J et al. (2003). Fibrosis in chronic hepatitis C acquired in infancy: is it only a matter of time? Am J Gastroenterol. 98:660–3. [PubMed] Haber B, Alonso E, Pedreira A, Rodriguez-Baez N, Ciocca M, Lacaille F et al. (2017). Long-term follow-up of children treated with peginterferon and ribavirin for hepatitis C virus infection. J Pediatr Gastroenterol Nutr. 64:89–94.
sofosbuvir + ribavirin 2, 3 NCT 02175758 April 2018
sofosbuvir/velpatasvir 1–6 NCT 03022981 December 2019
Note: * Egyptian children undergoing cancer chemotherapy
1. Sofosbuvir plus ledipasvir and weight-based RBV for use in treatment-naive non-cirrhotic genotype 3 infection
(currently only adult published data) 2. Long-term follow-up studies for 2–3 years in those treated to examine impact on growth, cognitive function,
educational attainment. No long-term study (beyond 24 weeks after the end of treatment) is currently available for DAAs in children.
3. Potential shortening of treatment regimen to 8 weeks 4. Need for more IFN-free options for GT 2/3 5. Future trials should include children whose DAA regimens have failed and genotype coverage should reflect
that of adult studies. should reflect that of adult trials 6. Future studies are needed to identify the best combinations for treating adolescents and children, when to
initiate treatment, and management of those with treatment failure. 7. Cost–effectiveness studies on treating children with DAAs, including acceptability and quality of life 8. Prioritization of DAA regimens for paediatric development, using a strategy of extrapolating data from adult
clinical trials and then applying criteria to select the most promising regimens for treating children 9. Need for paediatric formulations (granules) for those less than 6 years 10. Address knowledge gaps in epidemiology/burden and natural history of chronic HCV infection acquired
vertically or in childhood and in adolescence. These include the longer-term clinical outcomes of chronic HCV acquired vertically or in childhood and the extent of undiagnosed paediatric/adolescent HCV infection.

13
Harvoni: ledipasvir 90 mg/sofosbuvir 400 mg. In: European Medicines Agency (http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/003850/human_med_001813.jsp&mid=WC0b01ac058001d124, accessed 12 February 2018). Indolfi G, Stagi S, Bartolini E, Salti R, de Martino M, Azzari C et al. (2008). Thyroid function and anti-thyroid autoantibodies in untreated children with vertically acquired chronic hepatitis C virus infection. Clin Endocrinol (Oxf). 68:117–21. [PubMed] Jara P, Hierro L, de la Vega A, Diaz C, Camarena C, Frauca E et al. (2008). Efficacy and safety of peginterferonalpha2b and ribavirin combination therapy in children with chronic hepatitis C infection. Pediatr Infect Dis J. 27(2):142–8. Jonas MM, Balistreri W, Gonzalez-Peralta RP, Haber B, Lobritto S, Mohan P et al. (2012). Pegylated interferon for chronic hepatitis C in children affects growth and body composition: results from the pediatric study of hepatitis C (PEDS-C) trial. Hepatology. 56(2):523–31. Kelly DA, Haber B, González-Peralta RP, Murray KF, Jonas MM, Molleston JP et al. (2012). Durability of sustained response shown in paediatric patients with chronic hepatitis C who were treated with interferon alfa-2b plus ribavirin. J Viral Hepat. 19(4):263–70. Mack CL, Gonzalez-Peralta RP, Gupta N, Leung D, Narkewicz MR, Roberts ER et al.; North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (2012). NASPGHAN practice guidelines: diagnosis and management of hepatitis C infection in infants, children, and adolescents. J Pediatr Gastroenterol Nutr. 54:838–55. [PubMed] Mohan P, Barton BA, Narkewicz MR, Molleston JP, Gonzalez-Peralta RP, Rosenthal P et al. (2013). Evaluating progression of liver disease from repeat liver biopsies in children with chronic hepatitis C: a retrospective study. Hepatology. 58:1580–6. [PMC free article] [PubMed] Narkewicz MR, Rosenthal P, Schwarz KB, Drack A, Margolis T, Repka MX; PEDS-C Study Group (2010). Ophthalmologic complications in children with chronic hepatitis C treated with pegylated interferon. J Pediatr Gastroenterol Nutr. 51(2):183–6. doi: 10.1097/MPG.0b013e3181b99cf0. PubMed PMID: 20512062; PubMed Central PMCID: PMC2910798. Nydegger A, Srivastava A, Wake M, Smith AL, Hardikar W et al. (2008). Health-related quality of life in children with hepatitis C acquired in the first year of life. J Gastroenterol Hepatol. 23(2):226–30. Omland LH, Krarup H, Jepsen P, Georgsen J, Harritshoj LH, Riisom K et al. (2010). Mortality in patients with chronic and cleared hepatitis C viral infection: a nationwide cohort study. J Hepatol. 53:36–42. [PubMed] Rodrigue JR, Balistreri W, Haber B, Jonas MM, Mohan P, Molleston JP et al. (2009). Impact of hepatitis C virus infection on children and their caregivers: quality of life, cognitive, and emotional outcomes. J Pediatr Gastroenterol Nutr. 48(3):341–7. Serranti D, Indolfi G, Nebbia G, Cananzi M, D’Antiga L, Ricci S, Stagi S, Azzari C, Resti M et al. (2017). for the Italian Study Group for Treatment of Chronic Hepatitis C in Children. Transient hypothyroidism and autoimmune thyroiditis in children with chronic hepatitis C treated with pegylated-interferon-α-2b and ribavirin. Pediatr Infect Dis J. Sept 22. doi: 10.1097/INF.0000000000001791 (in press).
Sokal EM, Bourgois A, Stephenne X, SIlveira T, Porta G, Gardovska D et al. (2010). Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection in children and adolescents. J Hepatol. 52(6):827–31. Wirth S, Pieper-Boustani H, Lang T, Ballauf A, Kullmer U, Gerner P et al. (2005). Peginterferon alfa-2b plus ribavirin treatment in children and adolescents with chronic hepatitis C. Hepatology. 41(5):1013–18. Wirth S, Ribes-Koninckx C, Calzado MA, Bortolotti F, Zancan L, Jara P et al. (2010). High sustained virologic response rates in children with chronic hepatitis C receiving peginterferon alfa-2b plus ribavirin. J Hepatol. 52(4):501–7.
Wirth S, Rosenthal P, Gonzalez-Peralta RP, Jonas MM, Balistreri WF, Lin CH et al. (2017). Sofosbuvir and ribavirin in adolescents 12-17 years old with hepatitis C virus genotype 2 or 3 infection. Hepatology. 66:1102–10. doi: 10.1002/hep.29278.
Younossi ZM, Stepanova M, Balistreri W, Schwarz KB, Murray KF, Rosenthal P et al. (2016). High efficacy and significant improvement of quality of life (QoL) in adolescent patients with hepatitis C genotype 1 (GT1) treated with sofosbuvir (SOF) and ledipasvir (LDV). Hepatology. 64(S1): abstract 709. OR Hepatology. 63(1 Supplement 1): 351A–352A. Date of publication: 1 Oct 2016

14
Summary of judgements Judgement
Problem No Probably no Probably yes yes varies
Certainty of evidence Very low Low Moderate High
Balance of benefits and harms
Potential harms clearly outweigh potential benefits
Benefits and harms are balanced
Benefits clearly outweigh harm
Large desirable effects No Uncertain Probably Yes Varies
Are required resources small?
No Uncertain Probably Yes Varies
Equity Less equitable More equitable
Acceptability No Uncertain Probably Yes Varies
Feasibility No Uncertain Probably Yes Varies

15