Embed Size (px)
Citation preview

J Clin Pathol 1993;46:931-935
Epstein-Barr virus in normal, pre-malignant, andmalignant lesions of the uterine cervix
R J Landers, J J O'Leary, M Crowley, I Healy, P Annis, L Burke, D O'Brien, J Hogan,W F Kealy, F A Lewis, C T Doyle
AbstractAim-To detect the presence or absenceof Epstein-Barr virus (EBV) in cervicallesions ranging from normality to inva-sive malignancy.Methods-Eighteen randomly selectedcases of invasive squamous cell carcino-mas of the uterine cervix were examinedas well as 25 cases each of normal cer-vices and those showing cervical intra-epithelial neoplasia (CIN) I, II, and III.DNA-DNA in situ hybridisation, using abiotinylated probe to the Bam Hl "W"fragment of EBV, was carried out inaddition to the polymerase chain reac-tion using specific primer sequences thatflank a 153 base pair segment of the BamHl "W" region of the EBV genome andwhich do not cross-amplify other DNAherpes viruses. Positive control materialincluded paraffin wax embedded P3 HR1lymphoblastoid cells (containing highcopy numbers of EBV) and two naso-pharyngeal carcinomas positive forEBV.Results-Neither normal nor CIN I tissuewas positive. Eight per cent of CIN II tis-sue was positive; 8% of CIN III, and 43%of carcinomas were positive for EBV.Conclusion-The study shows that thevirus is present in some cases of cervicalcarcinoma and to a lesser degree in somepremalignant lesions of the cervix, butthe exact association between it and cer-vical oncogenesis, be it causative or inci-dental, remains to be determined.
Department ofPathology, UniversityCollege Cork, Cork,IrelandR J LandersJJ O'LearyM CrowleyI HealyJ HoganC T DoyleDepartment ofHistopathology,Regional Hospital,Wilton, CorkP AnnisL BurkeD O'BrienW F KealyDepartment ofPathology, Universityof Leeds, LeedsF A LewisCorrespondence to:Dr R J LandersAccepted for publication22 April 1993
(C Clin Pathol 1993;46:931-935)
Epstein-Barr virus (EBV) is a ubiquitoushuman herpes virus causing widespread andlargely asymptomatic infection. Onceinfected, individuals become lifelong carriers.EBV efficiently immortalises B lymphocytesto perpetual growth. The virus is associatedwith three lymphoproliferative diseases of Bcell origin: (i) infectious mononucleosis; (ii)Burkitt's lymphoma; (iii) lymphomas in theimmunocompromised.
This B cell tropism of EBV, however, isnot consistent with the growing body of evi-dence linking EBV with epithelial cells. Theassociation between EBV and undifferenti-ated nasopharyngeal carcinoma is well docu-mented.12 Certain other carcinomas of, forexample, tonsil,3 tongue,4 larynx,5 parotid,6and thymus7 also show an association with
EBV. In these, however, the evidence is lessconclusive and the consistency of the associa-tion has yet to be established.
Invasive carcinoma of the cervix is one ofthe commonest malignant tumours of thefemale genital tract. Much controversy sur-rounds its aetiology. The possibility of a sexu-ally transmissible infectious carcinogen in thegenesis of cervical neoplasia has receivedwidespread attention. Possible agents includethe herpes viruses, Chlamydia trachomatis, thehuman papillomaviruses (HPV), especiallytypes 16 and 18, and cytomegalovirus.The association between EBV and the
human uterine cervix is, as yet, not very welldefined. Sixbey et al showed that culturedectocervical epithelial cells can be infectedwith EBV.' These authors also showed lateviral antigens and EBV DNA in the exfoliat-ing cells but not in the attached epithelialmonolayer, thus suggesting an associationbetween viral replication and epithelial differ-entiation. Infectious EBV capable of trans-forming B lymphocytes has been isolatedfrom cervical washings from women recover-ing from infectious mononucleosis and fromEBV seropositive women who had no clinicalor serological evidence of acute EBV infec-tion.9 This suggests that the cervix could be asite for chronic viral shedding in a mannersimilar to that which occurs in the nasophar-ynx. These studies show both in vitro and invivo evidence for EBV replication in thecervix. In contrast to the nasopharynx, wherethere is a close association between epithelialand lymphoid tissues, no such associationexists in the cervix, suggesting that cervicalepithelium may be a primary site of EBVinfection.
MethodsEighteen cases of cervical squamous cell car-cinoma as well as 25 cases each of normalcervices and those showing CIN I, II, and IIIwere examined. All cases consisted of forma-lin fixed, routinely processed, and paraffinwax embedded surgical specimens retrievedfrom the archives, over a six year period(1985-1990). The only criterion used forblock selection was that those blocks with theleast amount of tissue necrosis were used tominimise possible problems with polymerasechain reaction (PCR) inhibitors. No attemptwas made to select tumours according to thedegree of differentiation, or to select casesfrom specific age groups. As positive controlmaterial, cells from a lymphoblastoid cell
931

Landers, O'Leary, Crowley, Healy, Annis, Burke, O'Brien, Hogan, Kealy, Lewis, Doyle
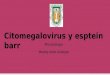
Figure1 Formalin-fixed and paraffin-embedded P3HRl lymphoblastoid cell lineshowing positive in situ hybridisation staining pattern for EBV.
P3HR1, which contains high copy numbersof EBV, were used in both studies (fig 1).
PCR TECHNIQUEDNA was extracted from tissues by dewaxingand then boiling two 5 ,um sections at 100°Cfor 20 minutes. The resultant solution (30 pl)was then taken for subsequent amplification.All reactions were carried out in sterile 0 5 mlmicrocentrifuge tubes in a Perkin-ElmerCetus DNA thermal cycler. The primers usedflank a 153 base pair segment of the Bam Hl"W" region of the EBV genome and give noamplification when tested with cells infectedwith other human herpes viruses. Primersequences (from published data)10 are asfollows:Primer 1: CACTTTAGAGCTCTGGAGGA;Primer 2: TAAAGATAGCAGCAGCGCAG.
These primers do not differentiate betweenEBV types A and B. Each PCR was carriedout in total volumes of 100 ,ul as follows:10 /u1 of 10 x reaction buffer (10 mM TRIS-HC1, 50 mM KC1, 1 5 mM MgCl,, 0-01%gelatin, 0-1% Triton X 100); 30 ,1 ofextracted DNA; 16 ,ul of dNTP mix, 0 55 ,ulof Taq polymerase (Promega); primers 1 and2 (in concentrated ammonia with no volumecorrection required); and 4345 pl of highpower liquid chromatography water. A totalof 50 amplification cycles was carried out oneach sample using the following cycling vari-ables: denaturation at 94°C for 1 minute;primer annealing at 60°C for 30 seconds; andprimer extension at 72°C for 1 minute. Allreactions were covered by mineral oil to pre-vent evaporation.
Tissue sections from a paraffin waxembedded P3HR1 lymphoblastoid cell line,and from a case of nasopharyngeal carci-noma, were used as positive controls, andsamples containing no template DNA wereused as negative controls. The primers werealso tested against fragments of whole CMVto ensure that no cross-amplification was tak-
ing place. The amplified products were thenvisualised using 2% agarose gel electrophore-sis, stained with ethidium bromide, andviewed under an ultraviolet transilluminator.
IN SITU HYBRIDISATIONPre-treatmentAll hybridisation reaction procedures werecarried out in three stages using nick trans-lated DNA probes. Pre-treatment stepsincluded the placement of 5,um sections onAPES coated single-well slides. Tissue sec-tions were baked overnight at 60°C to acquiremaximum section adherence. Sections weredewaxed in xylene for 30 minutes and werethen hydrated through graded alcohols to dis-tilled water over 30 minutes, and thenimmersed in phosphate buffered saline (PBS)for 5 minutes. The slides were immersed in0-02 M hydrochloric acid for 10 minutes,washed in PBS for 10 minutes, immersed inPBS containing 0-01% Triton X 100 for 90seconds, and then washed in PBS for 10 min-utes. Slides were then incubated in a pro-teinase K solution (50 mM TRIS-HCl(pH7-6), 5 mM EDTA, and proteinase K(0 5 mg/ml) at 37°C for 10 minutes. Theslides were washed twice in PBS containing2 mg/ml glycine and were immersed in 20%acetic acid in water for 15 seconds at 40C,washed through several changes of PBS, andpost-fixed in 4% paraformaldehyde in PBSfor 5. minutes. Sections were then washed inPBS for 5 minutes, dehydrated throughgraded ethanols, and stored in absoluteethanol before the hybridisation mixture wasapplied.
DNA probesThe DNA probes used were plasmid pBR322(Gibco BRL) as a negative control probe,human placental DNA (Oncor) as a totalDNA probe, and a Bam Hl "W" fragment ofEBV contained in pBR322. The probes werebiotinylated using biotin 1 1-dUTP (Sigma),using a nick translation kit (Gibco BRL) andfollowing the recommended protocol.Unincorporated dNTPs were separated fromthe biotinylated DNA by the spun columntechnique on Sephadex G 50 (Pharmacia).The biotinylated probes were prepared at aconcentration of 200 ng/ml in a hybridisationbuffer containing 2 x sodium nitrate andsodium sulphate (SSC), 5% dextran sulphate,0-2% dried milk powder (pure containing novegetable extracts), and 50% formamide.
HybridisationExcess absolute alcohol was drained from thetissue sections. Hybridisation mixture (75 ,ul)containing the probes were pipetted onto theprepared sections. The slide wells werecovered with a piece of gel-bond (FMCBioproducts), hydrophobic side down, andsealed with clear nail varnish. The slides wereheated at 90°C for 10 minutes to denaturecellular and probe DNA and were then trans-ferred to an incubator at 42°C in a humidi-fied box. The incubation was allowed toproceed over 18 hours at 42°C. After this the
932

EBVin the cemix
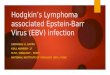
*il53bp.
M M
Figure 2 2% Agarose gel electrophoresis ofPCR products of cases and controls stainedwith ethidium bromide. M = (pX174 Hae III digest.
Figure 3 Invasive cervical squamous ceUl carcinomashowing positive in situ hybridisation signals for thepresence ofEBV.
gel-bond covering the wells was removedcarefully and the slides immersed in 2 x SSCfor 10 minutes. Sequentially, the slides were
washed in 2 x SSC at 60°C with agitationfor 20 minutes, 0-2 x SSC for 10 minutes,0-2 x SSC at 42'C for 20 minutes, 0-1 x
SSC for 10 minutes, and finally 2 x SSC for2 minutes the hybridisation signal was
detected.
Detection of signalThe slides were processed using a DNAdetection kit (Dako) with some modificationsto the recommended protocol. Briefly, theslides were immersed in buffer 2 (5% bovineserum albumin in 01 M TRIS-HCG (pH7-5), 0-1 M NaCl, 2 mM MgCl,, 0-05%
Triton X-100), to block non-specific strepta-vidin binding sites. The slides were drained ofexcess buffer and placed in a humidity cham-ber. An aliquot of streptavidin (10 ,il/ml) inbuffer 1 (01 M TRIS-HCG (pH 7.5), 0 1 MNaCl, 2 mM MgCl,, 005% Triton X-100)was added to each slide and incubated atroom temperature for 10 minutes. The slideswere washed for 5 minutes twice with agita-tion to remove excess buffer and were thenreturned to the humidified chamber. A solu-tion of biotinylated polyalkaline phosphatase(10 ,ul/ml) in buffer 1 was applied to theslides and incubated for a further 10 minutesat room temperature. The slides were washedfor 5 minutes twice in buffer 1 with agitationand immersed in buffer 3 (0 1 M TRIS-HCI(pH9 5), 0.1 M NaCl, 50 mM MgCl,) for 1hour. The slides were returned to the humidi-fied box and development reagent wasapplied. The development reagent, which wasmade fresh before use, was prepared byadding 44 ,ul of nitroblue tetrazolium NBT(Gibco BRL) solution to 10 ml of buffer 3and gently mixed by inverting the tube. 5-Bromo-4-chloro-3-indolyl phosphate (BCIP)(Gibco BRL) (33 pl) was then addedfollowed by gentle mixing. An appropriatevolume, equal to about 2 ml a slide wasapplied. The slides were incubated in sub-dued light for 30 minutes, and colour devel-opment was then monitored at 15 minuteintervals during incubation until full develop-ment had been attained. After developmentthe slides were immersed in PBS for 5 min-utes, rinsed in three changes of PBS, andfinally in water. Counterstaining was per-formed with 2% methyl green, then finallyrinsed in distilled water and coverslipmounted with glycerine jelly."
ResultsOf those cases in which positive results wereobtained, the in situ signals consisted pre-dominantly of perinuclear staining withintranuclear and cytoplasmic staining visiblein some malignant squamous epithelial cells.
All.cases positive by in situ hybridisationwere confirmed by PCR except for threecases in the group with carcinoma. Theresults for the different groups are shown inthe table (see also figs 2 and 3).
Results
NormalPCR 0%ISH 0%
CIN IPCR 0%ISH 0%
CIN IIPCR 8%ISH 8%
CIN IIIPCR 8%ISH 8%
CarcinomasPCR 43%ISH 28%
PCR = polymer chain-reaction.ISH = in situ hybridisation.
933

Landers, O'Leary, Crowley, Healy, Annis, Burke, O'Brien, Hogan, Kealy, Lewis, Doyle
Figure 4 Peritumoural lymphocytes in a case of cervical carcinoma showing positivehybridisation signals for EBV.
An interesting feature noted was that peri-tumoural lymphocytes in some cases of inva-sive carcinoma also gave positive signals forEBV (fig 4).
DiscussionUsing two molecular pathological techniques,this study has shown a previously undes-cribed association between Epstein-Barrvirus and squamous cell carcinoma of thecervix. The fact that the virus was shown ineight out of 18 cases by DNA amplificationusing PCR and in five out of 18 cases usingdirect in situ hybridisation is significant(p < 0001).The absence of infection in normal cervices
and the low levels of infection in pre-malig-nant lesions suggests that infection occurs latein cervical oncogenesis. It may well be thatthe virus is acting as a cofactor along withanother carcinogenic agent(s), possiblyhuman papillomaviruses, in the final progres-sion to invasive malignancy. These findings,however, only show the presence of EBVDNA in carcinomas of the cervix and in somecases of CIN and provide little insight intothe possible oncogenic role of the virus ininitiating or promoting tumour development.
Direct in situ hybridisation has in somecases shown the presence of viral DNA withinthe nucleus of the malignant cells. Thisstrongly suggests that the virus has integratedinto the host genome making an oncogeniceffect possible if not probable. It is wellrecognised that the virus appears to have anoncogenic role in the development of othermalignancies.9 Human seminal plasma acti-vated EBV in a lymphoblastoid cell line andalso had a synergistic effect on the activationof EBV when combined with culture fluids ofbacteria from the uterine cervix in patientswith cervical carcinoma."2 This raises the pos-sibility that human semen may activate latentEBV in vivo in the uterine cervix. Womenhave a three-fold increased risk of developing
cervical cancer if they partner a man whoseprevious wife had cervical carcinoma.12 It islikely that EBV, in a manner similar to otherherpes viruses and some types of HPV, canbe transmitted sexually, although it is notknown whether EBV can replicate in the malegenital tract. The close association betweenEBV and nasopharyngeal carcinoma clearlyindicates that the virus has oncogenic poten-tial within an epithelial cell. Thus the virusmay have a part to play in the aetiology orpathogenesis of cervical squamous cell carci-noma.No correlation between patient age or
tumour differentiation and the presence ofvirus was found.The discrepancy in results between the two
methods of virus detection has two possibleexplanations. First, DNA amplification usingPCR is a more sensitive technique than thedetection of viral DNA with in situ hybridisa-tion using, non-radiolabelled probes, andtheoretically even one particle of viral DNAin the tissue section should be detectable byPCR. It is possible that the three tumoursnegative in the in situ hybridisation study, butwhich gave positive results on PCR, may nothave had adequate copy numbers of the virusto permit detection. Second, as has beenshown, lymphocytes infiltrating the tumourson some tissue sections gave positive in situhybridisation signals for the presence of virusand thus would give a positive result on PCReven though the tumour cells themselves maynot contain any virus.
This last point emphasises the need forvery careful interpretation of results obtainedusing PCR on tissue sections. Ideally PCRcombined with in situ hybridisation is to berecommended as PCR results on their ownmerely indicate the presence of the virus inthe tissues but not necessarily in the cell ofinterest.The study, however, leaves many questions
unanswered: what exactly is the role, if any,of EBV in the development of cervical car-cinoma? How does the virus initially infectcervical tissues? Does the virus integrate intothe host genome and promote malignantchange? Is the virus, as we have detected, inan active or latent phase in these malignantcells? Such questions and others remain to beanswered by future work directed towardsestablishing whether the virus can directlytransform epithelial cells, and the precisemechanism(s) of EBV infection, either sexu-ally haematogenously, or both.
In summary, ubiquitous though humaninfection with EBV is, this study shows a newassociation between the virus and cervicalsquamous cell carcinoma. The exact associa-tion, be it causative or incidental, remains tobe determined.
1 Zur Hausen H, Schulte-Holthauzen H, Klein G, et al.EBV DNA in biopsies of Burkitt tumours and anaplasticcarcinomas of the nasopharynx. Nature 1970;228:1956-8.
2 Nonoyama M, Huang CH, Pagona JS, Klein G, Singh S.DNA of Epstein-Barr virus detected in tissues ofBurkitt's lymphoma and nasopharyngeal carcinoma.Proc Nad Acad Sci USA 1973;70:3265-8.
934

EBVin the cervix
3 Brickacek B, Hirsch I, Sibl 0, Vilikusova E, Vonka V.Presence of Epstein-Barr virus DNA in carcinomas ofthe palatine tonsil. JNCI 1984;72:809-15.
4 Raab-Traub N, Flynn K, Klein C. EBV DNA structureand oncogene expression in EBV associated malignan-cies. In: Ablashi DV, Glaser R, Levine PH, NonoyamaM, Pearson GR, eds. Second international symposium onEBVand associated malignant diseases. London: HumanaPress, 1987:423-8.
5 Brickacek B, Hirsch I, Sibl 0, Vilikusova E, Vonka V.Association of some supraglottic layrngeal carcinomaswith EB virus. IntJCancer 1983;32:193-7.
6 Saemundsen AK, Albeck H, Hansen JPH, et al. Epstein-Barr virus in nasopharyngeal and salivary gland carcino-mas in Greenland Eskimoes. Br Jf Cancer 1982;46:721-8.
7 Leyvraz S, Henle W, Chahinian AP, et al. Association ofEpstein-Barr virus with thymic carcinoma. N EnglMed 1985;312:1296-9.
8 Sixbey JW, Vesterinen EH, Nedrud JG, Raab-Traub N,
Walton LA, Pagano JS. Replication of Epstein-Barrvirus in human epithelial cells infected in vitro. Nature1983;306:480-3.
9 Sixbey JW, Lemon SM, Pagano JS. A second site forEpstein-Barr virus shedding: the uterine cervix. Lancet1986;ii:1 122-4.
10 Coates PJ, d'Ardenne AJ, Khan G, Kangro HO, Slavin G.Simplified procedures for applying the polymerase chainreaction to routinely fixed paraffin wax sections. ClinPathol 1991;44:115-8.
11 Zeng Y, Gi ZW, Ito Y. Epstein-Barr virus activation byhuman semen principle: Synergistic effects of culturefluids of bacteria isolated from patients with carcinomaof the uterine cervix. Cancer Lett 1985;28:311-5.
12 Lewis FA, Griffiths S, Ducliffe R, Wells M, Dudding N,Bird C. Sensitive in situ hybridisation technique usingbiotin-streptavidin-polyalkaline phosphatase complex.Clin Pathol 1987;40:163-6.
13 Kessler II. Etiological concepts in cervical carcinogenesis.Gynecol Oncol 1981;12:S7-24.
935