-
Median_ Nerve Displacement Throughthe Carpal Canal
Robert M. Szabo, MD, Brian K.. Bay, PhD, Nell A. Sharkey,
PhD,Chris Gaut, MD, Davis, CA
We determined the direct relationships between wrist position
and displacement of the mediannerve during active contraction of
the flexor tendons at the wrist with an intact,
transectedtransverse carpal ligament (TCL). Nine fresh cadavers
were mounted in an apparatus to allow
variable wrist position. Excursions of the tendons and
displacement of the median nerve weremeasured by tracking markers
with a video camera. Each limb was tested at 0°, 30°, and 60°
of wrist extension before and after release of the TCL.
Excursion of the flexor tendons required
for full finger flexion ranged from 2.3 to 3.I cm (mean, 3 cm).
Median nerve displacementranged from 0.9 to I .4 cm (mean, I cm).
The relationship between median nerve and flexortendon excursion
was consistently linear. Finger motion alone allows for median
nerve dis-
placement after surgery in the carpal tunnel. (J Hand Surg 1994~
19A:901-906,
path of the median nerve lies anteriorcenterg\of rotation of the
joints of the hand,of the ,fist and fingers will shorten the
bed
nerve, it to side proximally. Simi-of the wrist and fingers
lengthens
the median nerve in the hand, causing~slide distally.
Distal-proximal sliding of the me-
"re at the wrist in response to hand motion.)bserved in live
subjects1 and in cadavers.:"xtent that the normal sliding of the
mediart
restricted, for example, as a result of adhe--or compressive
entrapments, lengthening the
in response to joint motion must be ac-by local elongation of
the nerve. Nerw~
or traction of this type can result in tern-
or permanent disruption of action potentialation, causing
impairment of sensory and
hypothesize that altered kine-
Department of Orthopaedics, University of Califor-School of
Medicine, Davis, CA.for publication Dec. 15, 1993; accepted in
revise, d
II, 1994.any form have been received or will be receiw,~d
party related directly or indirectly to the sub-this
article.
uests: Robert M. Szabo, MD, Dep~.rtment of Ortho-University of
California. Davis, 2230 Stockton Biwl.,
CA 95817.
matics may be an etiologic element in nerve entrap-
ment syndromes, such as carpal tunnel syndrome.The purpose of
this study is to describe the normal
motion of the median nerve at the wrist in relationto stimulated
active finger flexion, with the wristimmobilized in a neutral
position or in extension.
Methods
Nine fresh cadaver forearms disarticulated at theelbow were
used. Each was rigidly mounted-in a jigby means of three Steinmann
pins, one each in theradius and ulna proximally and one distal,
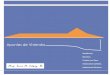
traversingboth radius and ulna (Fig. 1). Two 3-ram externalfixation
half-pins in the index metacarpal were at-tached to the jig by a
pivoting clamp that allowedimmobilization of the wrist in any
desired position offlexion or extension. Each finger was
independentlyloaded with a 75-gram counterweight attached to
thefinger tip with a heavy suture to extend the finger.
The forearm was superficially dissected to exposethe median
nerve, transverse carpal ligament, andflexor digitorum
superficialis (FDS) tendons. Theflexor digitorum profundus (FDP)
tendons were ex-posed by deeper dissection in the mid-forearm.
Carewas taken not to disrupt the natural tendon-nervepositional
relationship, and all fascia was left intact..Stainless steel
sutures were attached to the FDS andFDP tendons at the
muscle-tendon junctiom
The Journal of Hand Surgery
-
.902 S~zabo et al. / Median Nerve Displacement Through the
Carpal Canal
VideoCamera
FixationPins
Wrist SupportLoadCell
Stepper Motor
2. Exampledisplacemenand throughing markers z
ne e/tendon :
FingerCounterweights
Figure 1. Experimentalmodel and data collection system.
proximally along the muscle bellies, and attachedto a load cell
in series with a computer-controlledstepper motor. The stepper
motor simulated slowmuscle contraction by producing 12.5 mm/min
offlexor displacement and was positioned to maintainthe normal line
of action of the flexor muscles. Eachkinematic study was initiated
with the fingers fullyextended, and the stepper motor was used to
flexthe fingers until they reached the palm.
Excursion of the FDS tendons and displacementof the median nerve
relative to the transverse carpalligament was measured by tracking
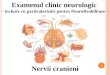
the positions ofmarkers attached to each structure (Fig. 2).
Steelsphere marke~s 0.5 mm in diameter were placed inthe substance
of the.tendon of the flexor digitorumsuperficialis of the ring
finger and within the sub-stance of the median nerve. With this
placement,markers moved with the nerve or tendon, and notwith the
overlying fascia, Reference markers wereplaced in the transverse
carpal ligament. As the fin-gers were actively flexed, positions of
the markerswere recorded with a Pulniz CDC video camera(Pulnix
America, Sunnyvale, CA) placed directlyabove the wrist. Images were
recorded with the fin-gers extended and at each 5-ram increment of
flexortendon motion proximally, as determined by dis-placement at
the stepper motor. Marker positionswere measured in each captured
frame usingIMAGE software (Wayne Rasband, Research Ser-vices
Branch, National Institute of Mental Health),
and displacements of the flexor tendons andnerve at the wrist
were calculated.
Each limb was tested in three positions:30° wrist ex~:ension,
60° wrist extension. Th.positions selected reflect a sequential
incretension that parallel increasing carpal tunnel)sures noted
’with increasing wrist extensionple with and without carpal tunnel
sylowing these tests, the transverse carpal liwas surgicalb)
sectioned to simulate a release~to treat carpal tunnel syndrome,
and the kineexperiments were repeated.
For each specimen, the FDS tendonwas plotted against
displacement of the cortesing median nerve, and this
relationshiplyzed by linear regression. A three-fa~of variance was
then conducted with theline slopes to ,determine the significance
ofsvariation, wrist position, and surgicaltransverse carpal
ligament. This wasa two-factorial blocked design analysis(ANOVA)
with specimen as blockingwrist position and surgical release as the
extal factors.
ResultsExcursion of the FDS tendons required
finger flexion ranged from 2.3 to 3.1 cmcm). Corresponding
displacement of the
ranged fro~betv,
median nervregardlessverse carpa
of r2 for netvaried fr
,f the con.’and tendc
;sion was u:dis
,we3. Ptot e#" :" :tigame: :
-
The Journal of Hand Surgery / Vol. 19A No. 6 November 1994
903
2. Example of video frames used to measure median nerve (MN) and
flexor digitorum supevficialis (FDS-ringdisplacement. Measurements
are references to a line drawn parallel to the edge of the
transverse carpal ligament:,~,~,d through a marker placed within
the substance of the ligament. At the beginning of loading (A), the
MN and
-ri:= markers are approximately equidistant from the TCL. At the
end of the test (B), both have moved proximallynerve/tendon ratio
of approximately 0.4 . Palmaris longus (PL) is labelled for
reference.
ranged from 0.9 to 1.4 cm (mean, 1 cm). The~ between excursion
of the FDS tendons
median nerve displacement was consistently lin-regardless of
wrist position or whether the
asverse carpal ligament was intact (Fig. 3). Val-or r2 for nerve
displacement versus tendon ex-
varied from 0.893 to 0.998 (mean, 0.96). Be-of the consistently
linear relationship betweenand tendon displacement, slope of the
linear.sion was used to characterize each test. These
.placement ratios were used for sta-
tistical comparison of the experimental groups (Fig.4).
The ANOVA revealed significant differences be-tween specimens (p
= .002 I), but differences owingto surgical release of the
transverse carpal ligament(p = .142) and wrist position (p = .349)
were significant. The effect of ligament release and wristposition
remained insignificant and had similar p-values when eliminating
the effect of specimen vari-ability With the: two-way blocked
ANOVA.
Load versus motor displacement data were ap-
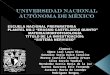
1.5
slope = 0.43
R2 = 0.992
1.0
0.0 0.5 1.0 1.5 ,,.0 2.5 3.0Tendon Displacement (cm)
Plot of nerve displacement versus tendon displacement. This
sample i:s in the neutral position with the transverseligament
intact. Range of nerve and tendon motion and the linear
relationship are typical.
-
904 S.zabo et al. / Median Nerve Displacement Through the Carpal
Canal
0olm
Neutral 30° Extensiono
60 Extension
~ Pre Release [~ Post ReleaseFigure 4. The nerve/tendon
displacement ratio (slope of the nerve versus tendon displacement)
for the three(wrist in neutral, 30° extension, and 60° extension)
and the two conditions (transverse carpal ligament intact and
proximately linear; r 2 = 0.95 by regression analysison compiled
data from all experiments. Loads neverexceeded 45 N. No slipping at
the tendon-suture wasnoted.
Passive flexion of the fingers at each wrist posi-tion resulted
in bunching up of the nerve and tendondistal to the transverse
carpal ligament, with littleevidence of sliding.
DiscussionCarpal tunnel iyndrome (CTS) has classically
been considered a nerve compression injury; how-ever, it is
clearly multifactorial in origin. 5 CTS isknown to be aggravated by
activities requiring pro-longed wrist flexion or repeated wrist or
finger flex-ion and power grip. 6 Using wick catheter
pressuremeasurements, we determined that hydrostaticpressure
increases in the carpal canal when the wristis held in either
flexion or extension.7 Furthermore,repetitive wrist flexion and
extension cause a sus-tained increase in intracarpal pressure.8
Recentmagnetic resonance imaging studies have demon-strated that in
flexion the finger flexor tendons areshifted anteriorly against the
transverse carpal liga-ment, while in extension they are aligned
more dot-.
sally. 9 In its interposed position between theriot row of
tendons and the transverse carpalment, the median nerve is subject
to shearincompression as the fingers are flexed. Thewhich these
shear forces result in tensilethe mediarr’nerve has not been
investigated.
A related problem concerns "spot-weldinthe me, dian nerve caused
by postoperativesions. Postoperative splinting regimens andtherapy
programs have been recommended tovent this problem without any
knowledge ofnerve mechanics. For instance, a lonebate concerns
whether splinting the wristpal tunnel surgery to prevent
bowstringingflexor tendons is harmful because of limitingnerve
displacement by adhesions.
Wilgis and Murphy2 observed longitudinalof the median nerve at
the wrist in response tosive motion of the hand in cadaver limbs.we
are concerned that passive motion of aarm may not accurately
reflect nervean active person, l° we simulated active fingerion in
cadaver preparations by pulling onflexor tendons with a motor.
Wedian nerve displacement with power grip inthe FDP and FDS act in
unison. The s
architect’~and flexorto justify t~
single motorof the medi.
such as typ}
range of.iaat we cfinger ticand Mu
ion/extensiwas note
who edeflections
In additi
:nt of the me~.9.~2 and rm
-~otion b,and ma’:_
One of the fcin re,~
ernal elastiis clean
cm, indic~being ~
:asured onnerve atd length
si~z~ is strai.tension. At.
motion ofuntil eq
In additionthe ne :
motion,con~
the rateacent tern
shear tWe k~
forces:prodm
ests that ’membran
fie,"of the:
Goldstein e~tendonsligamer
loadsexist b.
transversefinger fic
-
The Journal of Hand Surgery / Vol. 19A No. 6 November 1994
905
architecture of the flexor digitorum superfi-flexor digitorum
profundus muscles ap-
ustify tendodesis of their tendons and usele motor for finger
flexion. ~ The displace-the median nerve may be different in
activi-
as typing that require in-dependent FDS/.range of longitudinal
sliding of the median
tln::: we observed (9-14 mm) in response finger flexion is
similar to that observed by
is and Murphy2 in response to passive wristm/extension in
cadavers. A similar range of
was noted in live subjects by McLelland and~ who estimated nerve
sliding by observing
:flections of microelectrodes inserted in theIn addition to
longitudinal sliding, displace-
:of the median nerve in the palmar-dorsal direc-~.~-" and
radial-ulnar direction~3 in response tom, cion have been observed
in dynamic ultra-and magnetic resonance imaging studies.of the
forces causing the nerve to slide longi-
in response to hand motion is the nerve’s:rnal elastic tension.
Commonly if the median
is cleanly transected, the ends will retract 1indicating that
the nerve was under tension
being cut. Kwan et al.,~4 in a rabbit study,on 11% shortening in
segments of periph-
nerve after explanation. If we take the ex-iength as the gauge
length, then the nerve
~s strained 1 I%, and therefore is continuallyAny imbalance in
tensile forces causedof joints would result in sliding of the
until equilibrium is reestablished.addition to internal tension,
shear forces be-
the nerve and adjacent tissues may affectmotion. Our finding
that the flexor digitorum
consistently translocate at two to threethe rate of the median
nerve indicates that the
tendons exert proximally directed, fric-shear forces on the
nerve as the fingers are
verse carpal ligament, we may expect that similarshear forces
will affect the median nerve; thesewouM be aligned opposite to the
shear forces result-ing from friction with the proximally moving
ten-dons. We speculate that increased pressure in thecarpal tunnel
might amplify the relative role of shearforces in median nerve
motion. Such a pressure in-crease could result from abnormal
anatomy5 or sim-ply from forceful contraction of the flexor
digitorumprofundus muscle.~° Similarly, any adhesions be-tween
nerve and tendon or between nerve and trans-verse carpal ligament
or entrapment would be ex-pected to alter the normal nerve
kinematics.
The failure of surgical release of the transversecarpal ligament
to affect nerve and tendon excursionin this study is not
surprising. Disruption of normal:hydrostatic relations in a cadaver
hand would beexpected to alter carpal tunnel pressure dynamics;in
addition, there was no evidence that any of thesecadavers suffered
from carpal tunnel syndromewhen alive. Increasing wrist extension
caused atrend toward diminished sliding of the mediannerve. Wrist
flexion would be more likely to elicitkinematic abnormalities;~5
however, technical prob-lems with the wrist-flexed preparation
prevented usfrom collecting data in this position.
The observation that both flexor tendons and me-dian nerve
exhibit substantial translocation at thewrist in response to finger
motion when the wrist isrigidly immobitzed is significant with
respect to carefollowing surgical repair of nerve or tendon
injuries.It appears that active finger motion alone would pro-wide
:sufficient motion of the median nerve andflexor tendons in the
vicinity of the wrist to preventadhesf~n formation even if the
wrist is immobilized.Conw~rsely, if one desires complete
immobilizationof the: median nerve or finger flexor tendons
afterre.pair, digital motion must be prevented. --
ReferencesWe know of no published measurements ofi~’fix’~
~se forces; our observation that passive finger ~ cLelland DL,
Swash M. Longitudinal sliding of theproduced little motion of the
median nerve ~’t----~"median nerve during movements of the upper
limb. J
that they may be important. In addition,membranous connections
between the median
flexor tendons may contribute to the syn-of their movement.
et al. ~ measured strain in the digitaltendons proximal and
distal to the transverseligament in response to stepwise
increasing
loads and concluded that significant shearexist between the
finger flexor tendons and
se carpal ligament. Wrist flexion and ac-finger flexion
increased these traction effects.
median nerve passes adjacent to the ~rans-
d:’~eurol Neurosurg Psych 1977;39:566-70...~gilgis EFS, Murphy
The significance of longitudi-R." hal excursion in peripheral
nerves. Hand Clin 1986;
2:761-6.
9/~/Brown R, Pedowitz R, Rydevik B, et al. Effects ofacute
graded strain on efferent conduction propertiesin the rabbit tibial
nerve. Clin Orthop 1993;296:
,-~,~28:~-94.Q~lSunderland S. Stretch-compression neuropathy.
Clin~.~
Exp Neurol 1981;18:1-13.v/~i Szabo RM, Madison M. Carpal tunnel
syndrome. Or-
thop Clin North Am 1992;23:103-9.6. Masear VR, Hayes JM, Hyde
AG. An industrial cause
-
906 Szabo et al. / Median Nerve Displacement Through the Carpal
Canal
of carpal tunnel syndrome. J Hand Surg 1986;11A:222-7.
7. Gelberman RH, Szabo RM, Mortensen WW. Carpaltunnel pressures
and wrist position in patients withColles’ fracture. J Trauma
1984;24:747-9.
8. Szabo RM, Chidgey LK. Stress carpal tunnel pres-sures in
carpal tunnel patien’rs’ and normal patients. JHand Surg
1989;14A:624-7.
9. Skie M, Zeiss J, Ebraheim NA, Jackson WT. Carpaltunnel
changes and median nerve compression duringwrist flexion and
extension seen by magnetic reso-nance imaging. J Hand Surg
1990;15A:934-9.
I0. Smith EM, Sonstegard DA, Anderson WH. Carpaltunnel syndrome:
contribution of flexor tendons.Arch Phys Med Rehabil
1977;58:379-85.
11. Brand PW, Beach RB, Thompson DE.sion and potential excursion
of musctes inand hand. J Hand Surg 1981;6:209-16. ,
12. Zeiss J, Skie M, Ebraheim N, Jacksonrelations between median
nerve and flexor.the carpal tunnel. Am J Roentgenol 1989:
13. Nakamichi K, Tachibana S. Transverse s]median nerve beneath
the flexor retinacul
~. uwrg 1992;17B:213-6.an MK, Wall E J, Massie J, Garfin SR~
stress, and stretch of peripheral nerve. Ac
Scand 1992;63:262-72.15. Goldstein SA, Armstrong TJ, Chaffin
DB,
LS. Analysis of cumulative strain in tendonszdon sheaths. J
Biomech 1987;20:1-6.