Embed Size (px)
DESCRIPTION
Equine Neurologic Examination - What Do I Really Look For?
Citation preview

Equine Neurologic Examination - What Do I Really Look For? Joe Mayhew
Massey University NEW ZEALAND
A description of all the manipulations that can be performed, and observations that can be made, when undertaking a neurologic examination often doesn’t give the sense of efficiency and flow that is necessary to effectively perform such examinations in practice. This presentation aims to assist the practitioner to develop a flow to the equine neurologic examination without detracting from the clinical dictum that “it is easy to look, but harder to see”; one has to know what one is looking for.
A. OVERVIEW
Traditionally, a detailed neurologic examination follows the collection of information on a patient’s signalment and history, an evaluation of the environment, and a complete physical examination 1-10. However, during evaluation of a horse suspected of having a neurologic disorder, most busy practitioners include several components of a neurologic examination during the general physical examination. These should include observation of behavior, mental status, head posture, vision, pupillary light reflexes, structures of the eye, and inspection for facial symmetry, and inspection of the oral cavity. A laryngeal adductor response or slap-test should be performed and evaluation of posture and gait while walking, trotting, and turning quickly ought to be included. Inspection and palpation for muscle mass, bony integrity, and patches of sweating over the body and limbs (horse) are also easily incorporated into this examination. Tail and anal tone and reflexes can be evaluated when the rectal temperature is recorded.
Usually, this examination [Table 1] allows the practitioner to decide whether a more detailed neurologic examination, as outlined below, is required.
Sometimes enough evidence is available from this examination alone to make a fairly accurate anatomic diagnosis. Thus, a differential diagnosis and initial plan can be developed. If this cannot be done, especially if a thorough case work-up is indicated, then a complete neurologic examination should be undertaken, which will probably uncover further neurologic findings helpful to case work-up.
B. SIGNALMENT
The age, breed, gender, use, and value of a patient all are important considerations in the diagnosis and prognosis of many neurologic conditions. Several diseases are age-dependent. Certain diseases are associated with particular breeds. Only a few neurologic diseases depend upon gender. Certain uses to which animals are put can be associated with certain diseases, and this impacts considerably on the prognosis that accompanies the diagnosis. The value of the patient must always be kept in mind with respect to the depth of evaluation, cost of therapy, and future performance and productivity; the survival of herd mates must also be considered. C. HISTORY
In addition to taking a general history of the patient, questioning of the client should focus on the primary complaint. Information concerning the precise circumstances of the environment, other animal contacts, and the nature of the first signs observed ought to be sought first. Further questioning is aimed at defining a relationship between the severity of the syndrome and the passage of time.
Most congenital and familial diseases begin early in life and signs usually progress relentlessly. Syndromes resulting from physical causes, particularly external injury, have a sudden onset and then often stabilize or improve. Signs caused by infectious agents can be acute or chronic, and frequently fluctuate in severity. Immune-mediated diseases often result in fulminant signs that can improve dramatically,
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

particularly with therapy. Progression of metabolic, toxic, and nutritional disorders is variable. Finally, signs due to neoplastic involvement of the nervous system may begin abruptly, but most often are progressive.
Historical data can give clues as to how widespread or focal the disease process is in the nervous system, whether there was evidence of asymmetry, and how severe the signs have been. These aspects of pathogenesis of diseases can also be helpful in the etiologic diagnosis. D. PROCEDURE FOR THE NEUROLOGIC EXAMINATION
The primary aim of a neurologic examination is to confirm whether or not a neurologic abnormality exists. Because omission of parts is the most common mistake made during the neurologic examination, the order in which the examination is performed becomes important. I give here a precise practical format that is logical in sequence, easy to remember with practice, and emphasizes the need for an anatomic diagnosis [Where is the lesion?] to be made before an etiologic diagnosis [What is the cause of the condition?] is made. The rationale for the sequence of this examination is: firstly, it starts at the head and proceeds caudally to the tail; secondly, it is used for patients of all sizes and whether the patient is ambulatory or recumbent; thirdly, it considers the anatomic location of lesions as the examination proceeds. Even if parts of the examination must be omitted because of the nature of the patient, suspicion of fracture, or financial constraints, the sequence ought to be followed through mentally. Frequently, the presence of a neurologic lesion[s] cannot be deduced until the end of a thorough neurologic examination.
An outline of the recommended format for neurologic examination of horses is given in Table 2 and an example of a recording form to record the results of the neurologic examination is given in Figure 1. Some comment as to differences important to recall when evaluating neonates also are indicated.
I encourage those readers who are not reasonably well practiced in performing neurologic examinations, and in recording the variety of responses obtained with direct observations, reflex testing and response induction in normal patients, to practice on a friendly, neighborhood, mid-sized dog. The approach for such an examination will be used for young foals and miniature horses. Should the practice dog or such patient be small enough, the close aspects of the procedure used are readily performed by sitting with the patient on one’s knees or standing above and behind the patient for restraint and comfort.
Below is given an overview of the practicalities of performing an efficient neurologic examination. This is then followed by interpreting the findings to determine the presence, site(s) and extent of any neurologic lesion.
1. Head
For the routine equine examination, I evaluate what I can from a distance, preferably before the patient is disturbed, for the first observations of behavior, mentation and head, neck, trunk and limbs. Head and neck deviations need to be assessed closely by straightening the neck along the midline to determine what asymmetry may be present. I allow the patient to smell my [often peppermint-tainted] hand for introduction and observe the face, particularly eyes and associated structures, for an expressional response. Then I examine the parts of the head and neck for evaluation of cranial nerve function [Table 3].
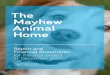
At this stage I will make sure I have the patient’s attention by tapping lightly once or twice above the eye with my finger tips on a cupped hand to induce a combined visual and facial response of palpebral closure, proceeding to a menace response [Figure 2] from nasal and temporal fields.
This is followed by observation of eye position and pupil size and symmetry using a bright pen torch from 12-24 inches. Swinging the light quickly from the fundus of one eye to the other and pausing for about 3s at each pupillary aperture as the light source is brought closer in front of each eye, allows the immediate pupillary response to be observed, unencumbered by blinking. Any asymmetry or suspected deficit means that a dazzle response must be performed and the tests need to be reperformed in dim and bright light, but not direct sunlight. With practice, the central fundus and optic disc can be directly inspected by looking directly along the shaft of light from a pen torch; otherwise an ophthalmoscope should be used. Evidence of
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

optic atrophy, peripapillary retinal lesions, globe position and trembling and ataxic eye movements and nystagmus all can all be detected.
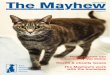
Eyeball position in the bony orbit, along with the size of the palpebral aperture and angle of the dorsal eyelashes then can be determined and both ventral movement and induced, normal, horizontal nystagmus of the globe then can be evaluated by first slowly raising the mandible to horizontal and then rotating the head to both sides through an arc of 60-90 degrees. Facial symmetry, reflexes, movement and especially muscle tone, all can then be observed as well as the bulk of the temporalis [Figure 3], masseter and pterygoid muscles being compared. During facial reflex testing with a blunt pair of needle holders sensation in the form of cerebral perception and resentment is evaluated from the nasal septum on each side. During this testing, any increased temperature and presence of sweat at the base of an ear will be evident. Nasal, oral, laryngeal, pharyngeal and hyoid region inspection and particularly palpation are performed and the thoracolaryngeal responses felt for. 2. Body
a. Neck & Thoracic Limbs Attention is immediately moved to the neck where bone and muscle symmetry is assessed by close
palpation and the local cervical and cervico-facial responses seen and felt. A solid blunt instrument such as 6-12 inch artery forceps or needle holders are best for performing this and other cutaneous testing although on occasion, with a very frightened patient, the tip of a rigid index finger may have to suffice as being more tolerated. A very firm vertical stimulus is required to be applied over sites at the level of and 10-15cm dorsal to the articular processes of cervical vertebrae.
b. Trunk & Pelvic Limbs Testing can continue caudally to transfer to the thorax testing the cutaneous trunci reflex over the mid
third of the lateral thorax, again with forceful stimuli. There is a variable region over the point of the shoulder, about the C7-T3 dermatomal region, where neither responses are obtained and the cutaneous trunci reflex usually fades in the caudal thoracic region. Flexion, extension and lateral bending of the thoracolumbosacral vertebral column then is conveniently tested with the instrument used to firmly stroke the lateral dorsum from the withers to the caudal gluteal region. Two-pinch technique is used to test dorsal dermatomes and limb autonomous zones for areas of hypalgesia if there is any evidence whatsoever of a reflex or lower motor neuron spinal cord lesion. Regional loss of muscle bulk, bony asymmetry and areas of sweating also should invoke detailed scrutiny.
c. Rectum, Bladder, Anus, Tail Coccygeal extension and flexion is evaluated during anal reflex and perineal sensory testing. A strong,
blunt-probe stimulus applied to the anal ring results in its brisk contraction and flexion [clamping] of the tail, whereas a light stimulus results in an anal reflex and with a stroking stimulus results in tail extension.
3. Gait & Posture
The minimal components of evaluation of posture and gait consist of the following. Walking in straight line viewed from the side as well as from behind and in front. Pulling laterally on the tail with the patient standing still and while walking forward, assessing
stride length and trajectory and placement of all four limbs. Trotting away from and back toward the examiner. Watching the patient walking in circles and turning tightly in circles in both directions. Taking the patient oneself and by walking backwards lead the patient in a serpentine path to
observe limb placement and lead in a manner such that the direction of each forefoot in turn is required to change direction during its swing phases.
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

Leading the patient to walk in circles and to turn tightly in circles in both directions, continuing these maneuvers while pulling on the lead rope and the tail simultaneously assessing strength of resistance.
Releasing the tail abruptly and stopping turning tightly to observe for adoption of and standing with abnormal limb positions. Manually placing the limbs in abnormal positions and placing them with the dorsum of the hoof resting on the ground are not useful in detecting neurologic motor or proprioceptive abnormalities.
Hopping the patient on at least the thoracic limbs [Figure 4].
Defining the presence and severity of gait and postural abnormalities Table 4], along with an interpretation of evidence of upper and lower motor neuron abnormal reflexes and function [Table 5] can assist in determining the site(s) of lesions in the nervous system.
A patient that is or can be placed in recumbency can be tested for classical limb reflexes. In practical terms these simply consist of the flexor reflexes in thoracic and pelvic limbs and the extensor or patellar reflex in the pelvic limbs. A reflex is regarded as present or hyperactive in a limb if such a response is detected in the recumbent while the limb is uppermost OR is dependent. All other reflex testing really does not usefully contribute to a neuroanatomic diagnosis and results of such additional limb reflex testing should not be used to alter a neuroanatomic diagnosis achieved by interpretation of the remainder of the examination.
At the conclusion of the gait evaluation, any issue that is unclear can be returned to for further evaluation and confirmation, and further testing can be considered as appropriate. This will frequently include reassessing the menace and pupillary responses and nasal septal sensation, observing the patient for facial weakness and head deviation while it is resting quietly and undisturbed, blindfolding and, for the smaller patients, hemi-walking, hoping on pelvic limbs, wheel barrowing on thoracic limbs with head and neck held extended.
For documentation, further study and possible consultation purposes, taking a video of any possible neurologic signs displayed by a patient is worth considering. It must be recalled however that a badly produced video clip is likely to be worse than a verbal or written description. At best, video sequences of neurologic movement abnormalities, particularly involving the gait, are less precise and accurate than in real life. E. FINAL INTERPRETATION; WHERE AND WHAT IS THE LESION?
Results of the neurologic examination should be documented and not left to memory [Figure 1]. After completion of the neurologic examination, the examiner may be able to decide if and where any
possible lesion exists. Sites include the basic areas of the: 1. Cerebrum 2. Brain stem 3. Peripheral cranial nerves 4. Cerebellum 5. Spinal cord 6. Peripheral spinal nerves 7. Neuromuscular junctions 8. Muscles 9. Autonomic nervous system Often the exact location of a lesion or lesions within these divisions will be able to be defined more
precisely. If the location of a lesion is not clear, then it is often worthwhile returning to the patient and performing an even more critical evaluation. Thus if facial weakness is suspected but not clearly seen the examiner can return to observe the horse for facial asymmetry while it is standing quietly in its stall without any
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

stimulation. Also, a blindfold may be applied to exaggerate evidence of vestibular disease. Finally, a very fractious or a very excited horse suspected of having a degree of weakness in the limbs may be exercised before a re-evaluation for evidence of weakness is made.
The presence of lameness can undoubtedly interfere with the interpretation of a horse’s gait and posture. If this is suspected then appropriate regional analgesia or the use of short acting synthetic opioid drugs (analgesics) may help to resolve the matter. With more chronic lameness cases, non steroidal anti-inflammatory drugs may be given at relatively high doses for several days or weeks, the horse’s gait can then be re-evaluated when any confounding lameness will have been reduced or eliminated.
At some time or other, all equine clinicians will come across cases that have some indication of a morbid nervous system lesion but no definitive proof can be obtained. Often, such cases are suspected to be suffering from conditions such as a painful musculoskeletal disorder, a peripheral neuromuscular movement disorder, a behavioural problem such as belligerency or laziness or back disease. Such patients may show one or more of the signs listed in Table 6. Examples of other forms of frantic behavior have been associated with a strong suspicion of exposure to nettles or poison ants, but in these situations the signs usually abate with time. A few of these unusual syndromes are discussed in latter sections.
F. INITIAL PLAN
Following consideration of anatomic and etiologic diagnoses, an initial plan must be devised. This will include use of ancillary aids to help rule in and rule out certain disease processes, a therapeutic plan, and a plan for client education, including economic advice, herd health management, and prognostic considerations. REFERENCES 1. de Lahunta A. Veterinary Neuroanatomy and Clinical Neurology. 2nd ed. W.B. Saunders Company. 1983. 2. Oliver JE, Hoerlein BF and Mayhew IG. Veterinary Neurology. WB Saunders. 1987; 7-56. 3. Palmer AC. Introduction to Animal Neurology. 2nd Ed ed. Blackwell Scientific Publications. 1976; 91-113. 4. Reed SM, Bayly WM and Sellon DC. Equine Internal Medicine. 2nd ed. W. B. Saunders. 2004; 1680. 5. Reed SM, Saville WJ and Schneider RK. Neurologic Disease: Current Topics In-Depth. 49th Ann Conv Amer Assoc Equine
Pract; 2003. 6. Ronéus M and Gustafsson K. Use of neurologic examination with focus on aetiologies in horses. 2000, SVA: Bålsta. 173-185. 7. Blythe LL and Engel HN. Back problems. Neuroanatomy and neurological examination. Vet Clin North Am Equine Pract
1999; 15:71-85, vi. 8. Adams R and Mayhew IG. Neurologic diseases. Vet Clin North Am Equine Pract 1985; 1:209-234. 9. Furr M and Reed SM. eds. Equine Neurology. 2008, Blackwell. 412 10. Mayhew IG. Large Animal Neurology. 2nd ed. Wiley-Blackwell. 2008.
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

TABLE 1: Neurologic tests and criteria evaluated in a physical examination.
Mental attitude / awareness Symmetry of neck, trunk and limbs Normal behavior patterns Tail and anal tone Menace tests Anal reflex Pupillary light reflexes Rectal examination Funduscopic examination Postures adopted at rest Symmetry of parts of the head Gait at walk and trot Inspection of the tongue Gait while turning Absence of nasal discharge Faster gaits External thoracolaryngeal (slap) reflex
TABLE 2: Outline of recommended format for the neurologic examination. Region Evaluation Division General Comment Neonate
Behavior Forebrain History important Seizures; especially mild and focal
Adjustment over 2-7 days
Mentation / Sensorium Thalamus Cerebrum Midbrain
Response to environment Adjustment - 24 hours
Head Posture & Movement Physical causes Forebrain – turn Vestibular – tilt Tremor – check eyeballs
Head tilt verses head turn Flexed head posture Jerky movements
Head
Cranial Nerves CN II - XII Brainstem Cervical sympathetic supply
Evaluate regions of head Subtle asymmetry in menace response & nasal sensation
Menace deficit <7 days Eye posture
Neck & Forelimbs C1-T2 Particularly asymmetry Flexor reflex only Hopping
All reflexes Hyperreflexia Crossed extension
Trunk & Hindlimbs T3-S2 L4 – femoral n. L5 – cranial gluteal n.
Particularly asymmetry Flexor & patellar reflexes only
All reflexes Hyperreflexia Crossed extension Extensor thrust
Rectum, Bladder, Anus, Perineum
S1-5
S1-2 is common fracture site
Body
Tail Co1- Extension & flexion ORTHOPEDIC PROBLEMS!
Shoulder & gluteal atrophy common Possible analgesic trial
SEPSIS!
Positional deficits All CNS-PNS Placing feet non-contributory Prematurity Extensor weakness Brain stem, spinal cord, PNS Especially LMN Dominant extensor strength Flexor weakness Brain stem, spinal cord, PNS
Spinal ataxia Irregular position & placement Cerebellar ataxia Hypermetria characteristic; F > H Normal to degree
Gait &
Posture
Ataxia
Vestibular gait Crouched posture Deliberate [predictable] stepping Wide based, staggering gait
Wide based to degree
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

FIGURE 1 NEUROLOGICAL EVALUATION Massey University -- Veterinary Teaching Hospital – IVABS
HISTORY:
Case No. ………………………………. Owner's Name:………………………….. Tel. No: ……………………......…………. Animal's Name…………………………… Species…………………………………… Breed…………………………………… Ref. Vet. …………………………………. VTH Clinician……………………………. *********Affix label here********** PHYSICAL EXAMINATION:
NEUROLOGICAL EXAMINATION VIDEO?
Behaviour, seizures Head Posture [tilt, turn] HEAD
Mental Status Head, Neck & Trunk Movement & Coordination
Cranial Nerves
Eyes LEFT RIGHT Vestibular/Ear LEFT RIGHT
Ophthalmic Exam Eye drop, normal/abnormal
Vision; II Nystagmus; normal vestibular
Menace; II-VII, cerebellum Abnormal
Pupils, PLR; II-III, Symp. Blindfold
Horners; Symp. Tongue
Strabismus; III, IV, VI, VIII Mass & use; XII, cerebrum
Face Pharynx, Larynx
Sensation; Vs, cerebrum Voice; IX, X
Muscle mass/jaw tone; Vm Swallow; IX, X, cerebrum
Ear, eye, nose, lip reflex; V-VII Endoscopy
Expression; VII, cerebrum T-L reflex
Sweating; Symp.
LEFT RIGHT GAIT & POSTURE
Thoracic limb / Neck
Pelvic Limb / Trunk Thoracic limb / Neck Pelvic Limb / Trunk
Paresis
Ataxia
Hypometria
Hypermetria
Posture
Postural Responses [hop, hemi, knuckle]
Lameness
LOCALISING SIGNS [reflexes, sensation etc] LEFT RIGHT
Thoracic limb / Neck
Pelvic Limb / Trunk
Tail, Anus, Bladder & Rectum
General [circle]: cerebrum brainstem peripheral CNs cerebellum spinal cord peripheral nerve muscle skeleton
ASSESSMENT Site of lesion[s]
Specific:
Cause of lesion[s]
PLAN Diagnostic
Therapeutic
Prognostic
KEY: 0 = absent; 1+ = hyporeflexic; 2+ = normal; 3+ = hypereflexic; 4+ = hypereflexic & clonus
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

TABLE 3: Assessment of cranial nerve function
CRANIAL NERVE MAJOR FUNCTION REFLEX/RESPONSE/ASSESSMENT I Olfactory Sense of smell Challenge II Optic Afferent pathway for vision and light Menace response
Pupillary light reflex Swinging light test
III Oculomotor Pupillary constriction Extra-ocular muscles
Pupillary light reflex Medial movement of globe
IV Trochlear Extraocular muscle (dorsal oblique) Ventrolateral rotation of globe
Sensory Sensory to head and face Ear, eyelid and lip (facial) reflexes Pain perception: head, nasal septum
V Trigeminal
Motor Motor to muscles of mastication Chewing, jaw tone, muscle mass (temporalis, masseter, pterygoid)
VI Abducens Extra-ocular muscle (retractor oculi) Extra-ocular muscle (lateral rectus)
Eyeball retraction (corneal reflex) Lateral movement of globe
VII Facial Motor to muscles of facial expression
Ear, eyelid and lip (facial) tone, reflexes, and movement Facial symmetry
Vestibular
Afferent branch of vestibular system Head posture Induced eyeball movement Normal vestibular nystagmus Normal gait Blindfold test
VIII
Cochlear Hearing Response to noise IX Glosso-pharyngeal Sensory / motor to pharynx X Vagus Sensory / motor to pharynx and larynx XI Accessory
Swallowing (observation and palpation) Gag reflex (nasal tube) Endoscopy
XII Hypoglossal Motor to tongue Tongue size and symmetry
FIGURE 2
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

FIGURE 3
FIGURE 4
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil

TABLE 4: Gait and postural abnormalities present with neurologic lesion at different locations.
GAIT AND POSTURAL ABNORMALITIES
LESION
LOCATION POSTURAL DEFICITS
PARESIS ATAXIA HYPOMETRIA HYPERMETRIA
Cerebrum +++ O O O O
Brain Stem ++ ++ ++ ++ ++
Vestibular +++ O ++ ++ O
Cerebellum ++ O +++ + +++
Spinal Cord / UMN ++ ++ ++ ++ ++
Peripheral Nerve / LMN ++ +++ + (++)* (+++)*
Musculo-Skeletal + ++ O + O
O = not usually expected + = mild if present ++ = usually present +++ = quite characteristically present * = usually only with selection sensory fiber involvement
TABLE 5: The common clinical features of Upper and Lower Motor Neuron Defects
DEFECT FUNCTION UPPER MOTOR NEURON LOWER MOTOR NEURON
Paralysis Normo- to hypertonic Hypotonic to flaccid Muscle atrophy None or disuse* Significant Muscle fasciculations NOT present Present Reflexes Normo- to hyperactive Hypoactive to absent
* becomes evident quickly in proximal muscles with lameness and disuse TABLE 6: Syndromes in which neurologic lesions may be suspected but usually not proven.
Prominent toe dragging Prominent sinking with dorsal lumbar pressure Intermittent & unusual lameness Throwing to the ground when saddle applied Shivering Rearing violently when first ridden Stringhalt-like movements Extreme difficulty in rising Hyperreflexic movements Localized hypertonia & tremor
Published in IVIS with the permission of the WEVA Close this window to return to IVIS
Proceedings of the 11th International Congress of World Equine Veterinary Association, 2009 - Guarujá, SP, Brazil