Embed Size (px)
Citation preview

Can Respir J Vol 21 No 6 November/December 2014334
Tracheal Epstein-Barr virus-associated smooth muscle tumour in an HiV-positive patient
Giulio S Dominelli MD FRCPC1, Rachel Jen MD FRCPC1, Kirily Park MD PhD FRCPC2, Tawimas Shaipanich MD FRCPC1
1Department of Medicine, Respiratory Division, University of British Columbia, Vancouver; 2Department of Medicine, Nanaimo Regional General Hospital, Nanaimo, British Columbia
Correspondence: Dr Giulio S Dominelli, Pacific Lung Health Centre, St Paul’s Hospital, 8B Providence Wing, 1081 Burrard Street, Vancouver, British Columbia V6Z 1Y6. Telephone 604-806-8818, fax 604-806-8839, e-mail [email protected]
CASE PRESENTATIONA 38-year-old woman was referred to her respirologist for evaluation of a two-month history of worsening exertional dyspnea. She had been seen by otolaryngology several months earlier for a right tonsilar mass and an incidental tracheal lesion 8 mm in size. The tonsil was biopsied, with pathology showing benign features that were managed conserva-tively. Unfortunately, she was lost to follow-up. Her current presenta-tion was associated with a productive cough, occasional dysphagia and scant hemoptysis. Although there were no associated fever or chills, the patient reported a 4.5 kg weight loss over the previous two months. There were remote tuberculosis contacts, although work-up at that time proved negative. Her medical history was significant for HIV diagnosed six years previously. There was no history of AIDS-defining illness or previous opportunistic infections. She was not currently on antiretroviral therapy (CD4 count 2.20×109/L). Other comorbidities included hepatitis C and a remote 10 pack-year smoking history.
Physical examination in the seated position revealed a respiratory rate of 16 breaths/min and oxygen saturation of 96%. There was good air entry bilaterally, with no stridor, wheeze or other adventious sounds. However, when supine, there was significant cough, associated with the development of loud stridor and a minor oxygen saturation drop to 92%. Head and neck examination revealed an enlarged right
tonsil and no palpable cervical lymph nodes. The remainder of the cardiovascular and abdominal examination was unremarkable.
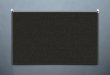
Given the concern for airway obstruction, a computed tomography (CT) scan of the neck, chest and abdomen was performed (Figure 1). Compared with a scan performed several months earlier, there was significant interval increase in the polypoid tracheal mass from 8 mm to 1.5 cm in diameter, an increase in the right tonsil mass to 1.1 cm and a left upper lobe nodule measuring 11 mm. Flexible bronchoscopy was performed in an intensive care unit setting. It revealed a near-obstructing lesion with no distal central airway narrowing or lesions (Figure 2A). Given its size and location, the decision was made to resect via rigid bronchoscopy in the operating room. The tracheal tumour was successfully removed via rigid bronchoscopy using loop electrocautery and retrievable basket through a flexible bronchoscope. The patient tolerated the procedure well and examination of the distal airways following removal showed no abnormalities. Pathology from the resection demonstrated a well-circumscribed mass com-posed of tightly packed fascicles of mildly atypical short spindle cells with numerous mitotic figures (up to 20 mitoses per 10 high-power fields). There was no necrosis present and lymphocytes were scattered throughout the tumour. According to immunohistochemistry, the tumour was strongly positive for smooth muscle actin and myosin and was negative for desmin, keratin, p63, S100, CD34, human herpes-virus 8 and epithelial membrane antigen. The CD45 stain was nega-tive in tumour cells, but highlighted the interspersed lymphocytes.
CLiNiCO-pATHOLOgiC CONfERENCES
©2014 Pulsus Group Inc. All rights reserved
GS Dominelli, R Jen, K Park, T Shaipanich. Tracheal Epstein-Barr virus-associated smooth muscle tumour in an HIV-positive patient. Can Respir J 2014;21(6):334-336.
Epstein-Barr virus-related smooth muscle tumours (EBV-SMTs) are a rare but well recognized non-AIDS-defining malignancy that can also be found in several other immunosuppressed states. Pulmonary involvement of EBV-SMTs is not uncommon, but it can present with multifocal lesions in any anatomical site. The present article describes an HIV-positive woman with dyspnea who was found to have a large tracheal EBV-SMT. The authors discuss their approach to diagnosis and management, and present unique follow-up bronchoscopic imaging.
Key Words: Epstein-Barr virus; HIV; Intervention bronchoscopy; Tracheal tumour
Une tumeur du muscle lisse de la trachée associée au virus d’Epstein-Barr chez une patiente positive au VIH
Les tumeurs des muscles lisses associées au virus d’Epstein-Barr (TML-VEB) sont des cancers non définis par le sida qui sont rares, mais bien connus. On peut les observer dans plusieurs autres états d’immunosuppression. L’atteinte pulmonaire des TML-VEB n’est pas inhabituelle, mais peut présenter des lésions multifocales dans tout foyer anatomique. Le présent article décrit une femme positive au VIH faisant de la dyspnée en raison d’une grosse TML-VEB de la trachée. Les auteurs présentent leur approche du diagnostic et de la prise en charge ainsi qu’une imagerie unique du suivi bronchoscopique.
Learning objectives• Tolearnwhichimmunosuppressedstatesplacepatientsatriskfor
Epstein-Barr virus-related smooth muscle tumours (EBV-SMTs).• Todevelopadifferentialdiagnosisforpulmonarymalignancyin
HIV patients.
Can Meds Competency: Medical Expert
Pretest• Whatarethecommonmalignantpulmonarymanifestations
of HIV?• What immunosuppressed states can be associated with
EBV-SMT?
Figure 1) Computed tomography scan with representative axial images showing the 1.5 cm polypoid tracheal tumour and left upper lobe nodule
Tracheal EBV-SMT in an HIV-positive patient
Can Respir J Vol 21 No 6 November/December 2014 335
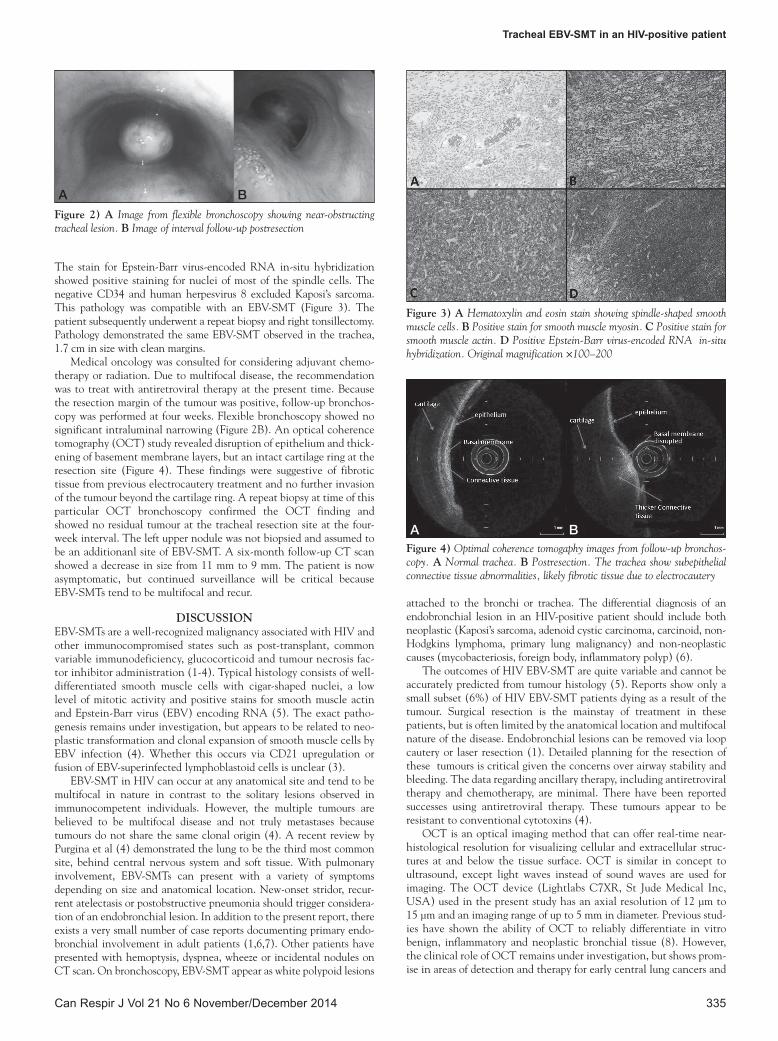
The stain for Epstein-Barr virus-encoded RNA in-situ hybridization showed positive staining for nuclei of most of the spindle cells. The negative CD34 and human herpesvirus 8 excluded Kaposi’s sarcoma. This pathology was compatible with an EBV-SMT (Figure 3). The patient subsequently underwent a repeat biopsy and right tonsillectomy. Pathology demonstrated the same EBV-SMT observed in the trachea, 1.7 cm in size with clean margins.
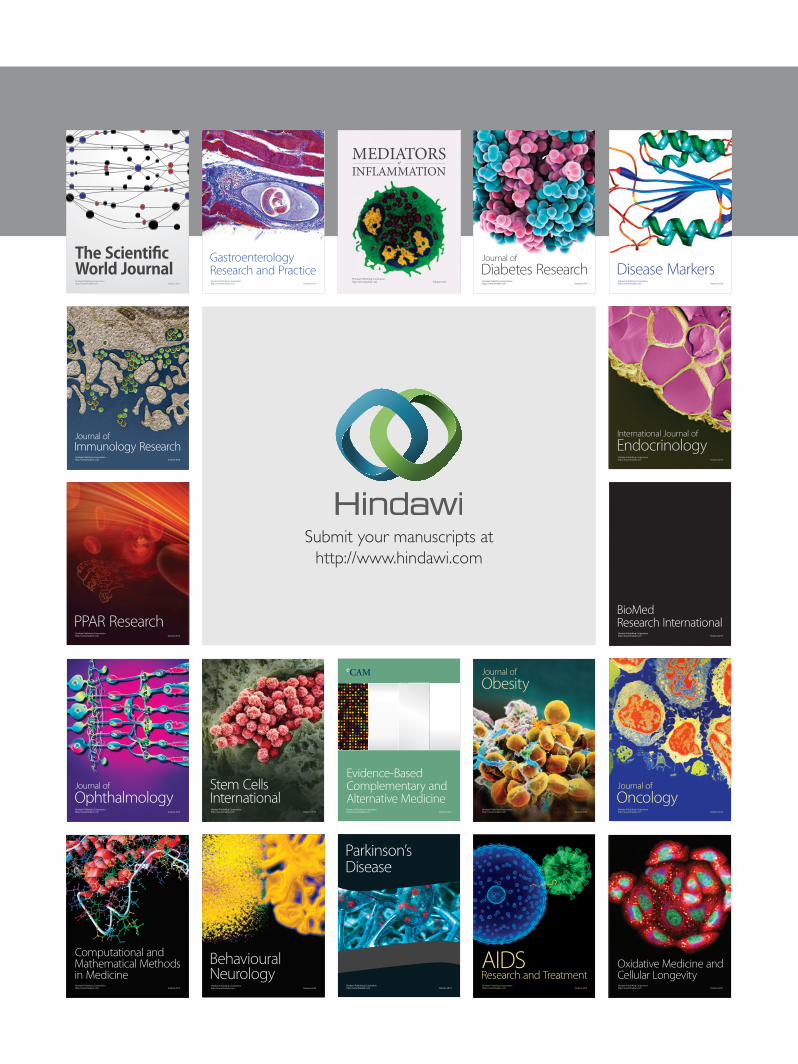
Medical oncology was consulted for considering adjuvant chemo-therapy or radiation. Due to multifocal disease, the recommendation was to treat with antiretroviral therapy at the present time. Because the resection margin of the tumour was positive, follow-up bronchos-copy was performed at four weeks. Flexible bronchoscopy showed no significant intraluminal narrowing (Figure 2B). An optical coherence tomography (OCT) study revealed disruption of epithelium and thick-ening of basement membrane layers, but an intact cartilage ring at the resection site (Figure 4). These findings were suggestive of fibrotic tissue from previous electrocautery treatment and no further invasion of the tumour beyond the cartilage ring. A repeat biopsy at time of this particular OCT bronchoscopy confirmed the OCT finding and showed no residual tumour at the tracheal resection site at the four-week interval. The left upper nodule was not biopsied and assumed to be an additionanl site of EBV-SMT. A six-month follow-up CT scan showed a decrease in size from 11 mm to 9 mm. The patient is now asymptomatic, but continued surveillance will be critical because EBV-SMTs tend to be multifocal and recur.
DISCUSSIONEBV-SMTs are a well-recognized malignancy associated with HIV and other immunocompromised states such as post-transplant, common variable immunodeficiency, glucocorticoid and tumour necrosis fac-tor inhibitor administration (1-4). Typical histology consists of well-differentiated smooth muscle cells with cigar-shaped nuclei, a low level of mitotic activity and positive stains for smooth muscle actin and Epstein-Barr virus (EBV) encoding RNA (5). The exact patho-genesis remains under investigation, but appears to be related to neo-plastic transformation and clonal expansion of smooth muscle cells by EBV infection (4). Whether this occurs via CD21 upregulation or fusion of EBV-superinfected lymphoblastoid cells is unclear (3).
EBV-SMT in HIV can occur at any anatomical site and tend to be multifocal in nature in contrast to the solitary lesions observed in immunocompetent individuals. However, the multiple tumours are believed to be multifocal disease and not truly metastases because tumours do not share the same clonal origin (4). A recent review by Purgina et al (4) demonstrated the lung to be the third most common site, behind central nervous system and soft tissue. With pulmonary involvement, EBV-SMTs can present with a variety of symptoms depending on size and anatomical location. New-onset stridor, recur-rent atelectasis or postobstructive pneumonia should trigger considera-tion of an endobronchial lesion. In addition to the present report, there exists a very small number of case reports documenting primary endo-bronchial involvement in adult patients (1,6,7). Other patients have presented with hemoptysis, dyspnea, wheeze or incidental nodules on CT scan. On bronchoscopy, EBV-SMT appear as white polypoid lesions
attached to the bronchi or trachea. The differential diagnosis of an endobronchial lesion in an HIV-positive patient should include both neoplastic (Kaposi’s sarcoma, adenoid cystic carcinoma, carcinoid, non-Hodgkins lymphoma, primary lung malignancy) and non-neoplastic causes (mycobacteriosis, foreign body, inflammatory polyp) (6).
The outcomes of HIV EBV-SMT are quite variable and cannot be accurately predicted from tumour histology (5). Reports show only a small subset (6%) of HIV EBV-SMT patients dying as a result of the tumour. Surgical resection is the mainstay of treatment in these patients, but is often limited by the anatomical location and multifocal nature of the disease. Endobronchial lesions can be removed via loop cautery or laser resection (1). Detailed planning for the resection of these tumours is critical given the concerns over airway stability and bleeding. The data regarding ancillary therapy, including antiretroviral therapy and chemotherapy, are minimal. There have been reported successes using antiretroviral therapy. These tumours appear to be resistant to conventional cytotoxins (4).
OCT is an optical imaging method that can offer real-time near-histological resolution for visualizing cellular and extracellular struc-tures at and below the tissue surface. OCT is similar in concept to ultrasound, except light waves instead of sound waves are used for imaging. The OCT device (Lightlabs C7XR, St Jude Medical Inc, USA) used in the present study has an axial resolution of 12 µm to 15 µm and an imaging range of up to 5 mm in diameter. Previous stud-ies have shown the ability of OCT to reliably differentiate in vitro benign, inflammatory and neoplastic bronchial tissue (8). However, the clinical role of OCT remains under investigation, but shows prom-ise in areas of detection and therapy for early central lung cancers and
Figure 2) A Image from flexible bronchoscopy showing near-obstructing tracheal lesion. B Image of interval follow-up postresection
Figure 3) A Hematoxylin and eosin stain showing spindle-shaped smooth muscle cells. B Positive stain for smooth muscle myosin. C Positive stain for smooth muscle actin. D Positive Epstein-Barr virus-encoded RNA in-situ hybridization. Original magnification ×100–200
Figure 4) Optimal coherence tomogaphy images from follow-up bronchos-copy. A Normal trachea. B Postresection. The trachea show subepithelial connective tissue abnormalities, likely fibrotic tissue due to electrocautery
A B
A B

Dominelli et al
Can Respir J Vol 21 No 6 November/December 2014336
tracheal stenosis. To our knowledge, the present report is the first to describe OCT as part of postresection surveillance for EBV-SMT. The noninvasive nature and real-time ability of this technology makes it ideal for future research in the area of postresection surveillance.
ACKNOWLEDGEMENTS: GSD, RJ, KP and TS identified the case, managed the patient and contributed to the writing and editing of the manuscript. The authors thank Dr H Masoudi for providing the histopa-thology images.
Post-test• Whatarethecommonmalignantpulmonarymanifestationsof
HIV?EBV-SMT are a rare malignant complication of HIV infection. The more frequent malignant manifestations that one should consider are: Kaposi’s sarcoma, lymphoma, bronchogenic carcinoma and metastasis (9). Both Kaposi’s and non-Hodgkin’s lymphoma are considered to be AIDS-defining malignancies (9).• What immunosuppressed states can be associated with
EBV-SMT?Case reports have identified EBV-SMT related to several immuno-suppressed states. These include, but are not limited to: HIV/AIDS, post-transplant, common variable immunodeficiency, glucocorti-coid and tumour necrosis factor inhibitor administration (2-4).
REFERENCES1. Bluhm JM, Yi ES, Diaz G, Colby TV, Colt HG. Multicentric
endobronchial smooth muscle tumors associated with the Epstein-Barr virus in an adult patient with the acquired immunodeficiency syndrome: A case report. Cancer 1997;80:1910-3.
2. Mierau GW, Greffe BS, Weeks DA. Primary leiomyosarcoma of brain in an adolescent with common variable immunodeficiency syndrome. Ultrastruct Pathol 1997;21:301-5.
3. Moore Dalal K, Antonescu CR, Dematteo RP, Maki RG. EBV-associated smooth muscle neoplasms: Solid tumors arising in the presence of immunosuppression and autoimmune diseases. Sarcoma 2008;2008:859407.
4. Purgina B, Rao UN, Miettinen M, Pantanowitz L. AIDS-related EBV-associated smooth muscle tumors: A review of 64 published cases. Patholog Res Int 2011;2011:561548.
5. Deyrup AT, Lee VK, Hill CE, et al. Epstein-Barr virus-associated smooth muscle tumors are distinctive mesenchymal tumors reflecting multiple infection events: A clinicopathologic and molecular analysis of 29 tumors from 19 patients. Am J Surg Pathol 2006;30:75-82.
6. Metta H, Corti M, Redini L, Dure R, Campitelli AM, Narbaitz M. Endobronchial leiomyoma: An unusual non-defining neoplasm in a patient with AIDS. Rev Inst Med Trop Sao Paulo 2009;51:53-5.
7. Sharif M, Seelall V. Endobronchial Epstein Barr virus-associated leiomyoma: An unusual finding in an adult. AIDS Chest 2011;140 (4 Meeting Abstracts):80A.
8. Whiteman SC, Yang Y, Gey van Pittius D, Stephens M, Parmer J, Spiteri MA. Optical coherence tomography: Real-time imaging of bronchial airways microstructure and detection of inflammatory/ neoplastic morphologic changes. Clin Cancer Res 2006;12:813-8.
9. White DA. Pulmonary complications of HIV-associated malignancies. Clin Chest Med 1996;17:755-61.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com