Embed Size (px)
Citation preview

10/8/2018
1
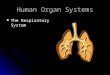
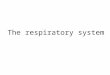
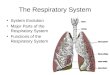
Respiratory System
• Major functions of respiratory system: supply body with O2 for cellular respiration and dispose of CO2, a waste product of cellular respiration
• Respiratory and circulatory system are closely coupled
• Also functions in olfaction and speech
Respiratory System
• Respiration involves four processes1. Pulmonary ventilation
(breathing): movement of air into and out of lungs
2. External respiration: exchangeof O2 and CO2 between lungs and blood
3. Transport of O2 and CO2 in blood
4. Internal respiration: exchange ofO2 and CO2 between systemic blood vessels and tissues
Circulatory
system
Respiratory
system
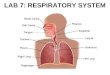
The Major Respiratory Organs
Nasal cavity
Nostril
Larynx
Trachea
Carina of trachea
Right main (primary) bronchus
Right lungDiaphragm
Left lung
Left main (primary) bronchus
Oral cavity
Pharynx
Conducting ZoneRespiratory Zone

10/8/2018
2
Anatomical Relationships Of Organs In The Thoracic Cavity
Trachea
Thymus
Apex of lung
Right superior lobe
Horizontal fissure
Right middle lobe
Oblique fissure
Right inferior lobe
Heart(in mediastinum)
Diaphragm
Base of lung Cardiac notch
Anterior view. The lungs flank mediastinal structures laterally.
Left inferiorlobe
Obliquefissure
Leftsuperior lobe
Visceral pleura
Pleural cavity
Parietal pleura
Rib
Intercostal muscle
Lung
Hilum of the LungApex of lung
Pulmonary artery
Left mainbronchus
Pulmonaryvein
Cardiacimpression
Obliquefissure
Lobules
Aorticimpression
Hilum of lung
Left inferiorlobe
Obliquefissure
Leftsuperior lobe
Photograph of medial view of the left lung.
Anatomical relationships of organs in the thoracic cavity
PosteriorVertebra
Right lung
Parietal pleura
Visceral pleura
Pleural cavity
Pericardial membranes
Anterior mediastinum
Anterior
Heart (in mediastinum)
Pulmonary trunk
Thoracic wall
Left lung
• Left pulmonary vein
• Left pulmonary artery
• Left main bronchus
Root of lungat hilum
Esophagus(in mediastinum)
Sternum
Transverse section through the thorax, viewed from above. Lungs, pleural membranes, and major organs in the mediastinum are shown.

10/8/2018
3
Nasal Cavity Posteriornasalaperture
Sphenoidalsinus
Frontal sinus
Nasal cavity
• Nasal conchae(superior, middle and inferior)
• Nasal meatuses(superior, middle, and inferior)
• Nasal vestibule
• Nostril
Hardpalate
TongueSoftpalate
Uvula
Cribriformplate ofethmoid bone
• Passageway• Moistens and warms entering air• Filters and cleans• Resonating chamber for speech• Location of olfactory receptors
• Vibrissae• Mucus membranes
• Pseudostratified ciliated epithelium• Goblet cells• Cilia – directed toward
pharynx• Seromucous glands: lysozyme• Defensins
Conchae:• Increase
surface area of mucosa
• Increase air turbulence
Pharynx, Larynx, and Upper Trachea
(b) Structures of the pharynx and larynx
Nasopharynx
Oropharynx
Larynx
Posterior nasalaperture
• Pharyngeal tonsil
• Opening ofpharyngotympanictube
• Palatine tonsil
• Isthmus of thefauces
Esophagus
Laryngopharynx
Trachea
Hard palate
Soft palate
Tongue
Lingual tonsil
Hyoid bone
• Epiglottis
• Vestibular fold
• Thyroid cartilage
• Vocal fold
• Cricoid cartilage
Thyroid gland
Air or Air and food passageway
‘Eustachian’ tube
Unencapsulatedlymphoid nodules
Epiglottis (elastic cartilage) protects airway (glottis) from food/drink during swallowing
The Larynx
Body of hyoid bone
Thyroid cartilage
Laryngeal prominence(Adam’s apple)
Cricothyroid ligament
Cricoid cartilage
Trachealcartilages
Anterior view
Thyrohyoidmembrane
Epiglottis
• Location of vocal folds typically known as the true vocal cords
• Airway – in and out – return to pseudostratified ciliated epithelium
• Voice production

10/8/2018
4
Epiglottis
Vestibular fold (false vocal cord)
Vocal fold (true vocal cord)
Glottis
Inner lining of trachea
Cuneiform cartilage
Corniculate cartilage
Movements of the vocal folds.
Vocal folds in closed position;closed glottis
Vocal folds in open position;open glottis
https://youtu.be/9Tlpkdq8a8c
Tissue Composition Of The Tracheal Wall
Esophagus
Trachealis
Posterior
Lumen of trachea
Anterior
Submucosa - glandular
Hyaline cartilage
Adventitia
Seromucous glandin submucosa
Mucosa – pseudostratified ciliated epithelium
• ‘Windpipe’• Supported by C – shaped rings of hyaline
cartilage – prevents closing even when thoracic pressure changes and food in esophagus pushes
• Carina
Tissue composition of the tracheal wall
Goblet cell
Mucosa
Pseudostratifiedciliated columnarepithelium
Lamina propria(connective tissue)
•
•
Submucosa
Seromucous glandin submucosa
Photomicrograph of thetracheal wall (320 )
Hyaline cartilage

10/8/2018
5
Conducting Zone Passages
Superior lobe of left lung
Lobar (secondary)bronchus
Left main(primary) bronchus
Segmental(tertiary)bronchus
Inferior lobeof left lung
Inferior lobe of right lung
Middle lobe of right lung
Superior lobe of right lung
Trachea
At level of T7
• Three lobes on right; two lobes on left• Segments• Lobules
• C-rings replaced by hyaline plates• Elastic tissue present - stroma• Pseudostratified ciliated eventually replaced by columnar• Smooth muscle in walls increases
Respiratory Zone Structures
Alveolar ductAlveoli
Alveolar duct
Alveolarsac
Terminalbronchiole
Respiratorybronchioles
• Terminal bronchioles <0.5 mm in diameter• No cartilage involvement• Smooth muscle dominates• Epithelium now non-ciliated cuboidal in the smallest tubes• Mucus production limited then ends
Respiratory Zone Structures
Respiratorybronchiole
Alveolarduct
Alveolarpores
Alveoli
Alveolarsac
Alveolar surface area = 90 m2 or 969 ft2 in healthy lungs of adult male

10/8/2018
6
Alveoli And The Respiratory Membrane
Respiratory bronchiole
Terminal bronchiole
Smoothmuscle
Elasticfibers
Alveolus
Capillaries
Respiratory membrane is combination of alveolar squamous cells and capillary endothelial cells • 0.5 µm thick blood-air barrier
Alveoli And The Respiratory Membrane
Alveolus
Capillary
Nucleus of type Ialv eolar cell
Alv eolar pores
Alv eolar epithelium
Endothelial cell nucleus
Respiratorymembrane
Alveolus
CapillaryO2
CO2
Fused basement membranesof alv eolar epithelium andcapillary endothelium
Capillary endothelium
Macrophage
Type Ialv eolar cell
Type II alv eolar cell(secretes surfactant)
Red blood cellin capillary
Alv eoli (gas-filledair spaces)
Detailed anatomy of the respiratory membrane
Red blood cell
• Type I alveolar cells = simple squamous supported by thin basement membrane, dominate• Type II alveolar cells = scattered surfactant-producing cuboidal cells, produce antimicrobials also.
Surfactant decreases cohesiveness (surface tension) of water on surface, reducing tendency to collapse
• Alveolar pores share air between adjacent alveoli• Alveolar macrophages move along surface eventually being swept out
Pulmonary Ventilation• Boyle’s law: relationship between pressure and
volume of a gas• Gases always fill the container they are in
• If amount of gas is the same and container size is reduced, pressure will increase
• So pressure (P) varies inversely with volume (V)
• Mathematically:• P1V1 = P2V2
When atmospheric pressure and intrapulmonary pressure are the same, no air moves• muscles acting on the lungs change the intrapulmonary
pressure

10/8/2018
7
Parietal pleura
Atmospheric pressure (Patm
)0 mm Hg (760 mm Hg at sea level)
Thoracicwall
Visceral pleura
Pleural cavity containing pleural fluid
Transpulmonarypressure4 mm Hg (the difference between 0
mm Hg and 4 mm Hg)
Must be maintained or lung collapses
Intrapleuralpressure (P
ip)
4 mm Hg(756 mm Hg)
Intrapulmonarypressure (P
pul)
0 mm Hg(760 mm Hg)
4
0
Diaphragm
LungStrong adhesive forces between visceral and parietal pleurae keeps Pip
negative
Sequence of eventsChanges in anterior-posterior and
superior-inferior dimensions
Changes in lateral dimensions(superior view)
Insp
ira
tio
nE
xp
ira
tio
n
Ribs areelev ated and sternum flaresas externalintercostals
contract.
Externalintercostalscontract.
Diaphragm movesinferiorly duringcontraction.
Ribs andsternum aredepressed asexternalintercostals
relax.
Externalintercostalsrelax.
Diaphragmmov essuperiorlyas it relaxes.
Inspiratory muscles contract(diaphragm descends; rib cagerises).
1
Thoracic cavity volumeincreases.2
Lungs are stretched;intrapulmonary volume increases.3
Intrapulmonary pressuredrops (to 1 mm Hg).4
Air (gases) flows into lungsdown its pressure gradient untilintrapulmonary pressure is 0(equal to atmospheric pressure).
5
Inspiratory muscles relax(diaphragm rises; rib cagedescends due to recoil of costalcartilages).
1
Thoracic cavity volumedecreases.2
Elastic lungs recoilpassively; intrapulmonaryv olume decreases.
3
Intrapulmonary pressure rises(to 1 mm Hg).4
Air (gases) flows out of lungsdown its pressure gradientuntil intrapulmonary pressure is 0.
5
• Normal inspirational muscle contractions lead to 500 ml change in volume
• Diaphragm is dominant inspirational muscle
Forced inspirations recruit the scalenes, sternocleidomastoids, pectoralis minors, and erector spinae
Normal expiration is passive
Gas Exchange:Basic Properties of Gases
• Dalton’s law of partial pressures• Total pressure exerted by mixture of gases is equal to sum of
pressures exerted by each gas
• Partial pressure• Pressure exerted by each gas in mixture
• Directly proportional to its percentage in mixture
• Henry’s law• For gas mixtures in contact with liquids:
• Each gas will dissolve in the liquid in proportion to its partial pressure
• At equilibrium, partial pressures in the two phases will be equal
• Amount of each gas that will dissolve depends on: • Solubility: CO2 is 20 more soluble in water than O2, and little N2 will
dissolve
• Temperature: as temperature of liquid rises, solubility decreases

10/8/2018
8
Partial Pressure Gradients Promoting Gas Movements In The Body
Inspired air: Alveoli of lungs:
External
respiration
Pulmonary
veins (PO2
100 mm Hg)
PO2
PCO2
160 mm Hg
0.3 mm Hg
PO2
PCO2
104 mm Hg
40 mm Hg
Pulmonaryarteries
Alveoli
PO2
PCO2
40 mm Hg
45 mm Hg
Blood leavingtissues and
entering lungs:
Blood leavinglungs and
entering tissuecapillaries:PO2
PCO2
100 mm Hg
40 mm Hg
Heart
Systemicveins
Systemicarteries
Internal
respiration
O2 CO2
CO2 O2 O2 CO2
O2 CO2
O2 CO2 O2 CO2
CO2 O2
Tissues:
PO2 less than 40 mm Hg
greater than 45 mm HgPCO2
Oxygen Transport
• Association of oxygen and hemoglobin• Each Hb molecule is composed of four polypeptide
chains, each with a iron-containing heme group• So each Hb can transport four oxygen molecules
• Oxyhemoglobin (HbO2): hemoglobin-O2
combination
• Reduced hemoglobin (deoxyhemoglobin) (HHb): hemoglobin that has released O2
The oxygen-hemoglobin dissociation curve will
help you understand how the properties of
hemoglobin (Hb) affect oxygen binding in the
lungs and oxygen release in the tissues. In the lungs, where PO
2is high
(100 mm Hg), Hb is almostfully saturated (98%) with O2. This axis tells you how much
O2 is bound to Hb. At 100%,each Hb molecule has 4 boundoxygen molecules.
If more O2 is present,more O2 is bound.Howev er, because ofHb’s properties (O2
binding strengthchanges with saturation),this is an S-shaped curve.
This axis tells you the relativeamount (partial pressure) ofO2 dissolv ed in the fluidsurrounding the Hb. In the tissues of other organs,
where PO2 is low (40 mm Hg), Hbis less saturated (75%) with O2.
Hemoglobin
Oxygen
100
80
60
40
20
0 0 20 40 60 80 100
PO2
(mm Hg)
Pe
rce
nt
O2sa
tura
tio
n o
f h
em
oglo
bin

10/8/2018
9
Oxygen Transport
Influence of other factors on hemoglobin saturation
• 2,3-bisphosphoglycerate (BPG) is produced by RBCs during glycolysis• BPG levels rise when oxygen levels are low
• Increasing BPG binding to Hb: release more O2
• As tissues metabolize glucose, they use O2, causing:• Increases in PCO2
and H+ in capillary blood
• Declining blood pH (acidosis) and increasing Pco2 cause Hb-O2 bond to weaken
• Referred to as Bohr effect
• O2 unloading occurs where needed most
• Heat production in active tissue directly and indirectly decreases Hbaffinity for O2
• Allows increased O2 unloading to active tissues
Changing Delivery of Oxygen by Hemoglobin
• At rest, hemoglobin carries more oxygen than it actually delivers to tissues• Only 23% of what is carried is delivered
• Tissue Po2 determines % liberated
• Hemoglobin saturation (all hemes carrying oxygen) changes with changing conditions• temperature and pH-related conformational shift in
hemoglobin, ↑BPG reduces its capacity to carry

10/8/2018
10
100
80
60
40
20
0
10°C
20°C38°C
43°C
Normal bodytemperature
Pe
rce
nt
O2
sa
tura
tio
n o
f h
em
og
lob
in
20 40 60 80 100
PO2(mm Hg)
100
80
60
40
20
0
Normal arterialcarbon dioxide(PCO2
40 mm Hg)
or H (pH 7.4)
20 40 60 80 100
PO2(mm Hg)
Pe
rce
nt
O2
sa
tura
tio
n o
f h
em
og
lob
in
Increased carbon dioxide(PCO2
80 mm Hg)or H (pH 7.2)
Decreased carbon dioxide(PCO2
20 mm Hg) or H (pH 7.6)
Carbon Dioxide Transport
• Occurs primarily in RBCs, where enzyme carbonicanhydrase reversibly and rapidly catalyzes this reaction
• In systemic capillaries, after HCO3– is created, it quickly
diffuses from RBCs into plasma• Outrush of HCO3
– from RBCs is balanced as Cl– moves into RBCs from plasma • Referred to as chloride shift

10/8/2018
11
Carbon Dioxide Transport
Encouraging CO2 exchange at tissues and at lungs
• Haldane effect - amount of CO2 transported is affected by PO2• The lower the PO2
and Hb O2 saturation, the more CO2 Hbcan carry
• Unsaturated Hb buffers H+ and forms carbaminohemoglobin more easily
• Bohr effect - at tissues, as more CO2 enters blood, more oxygen dissociates from hemoglobin • As HbO2 releases O2, it more readily forms
carbaminohemoglobin
Transport and Exchange of CO2 and O2 at Tissues
Oxygen release and carbon dioxide pickup at the tissues
Tissue cell Interstitial fluid
CO2
CO2
CO2
CO2
CO2
CO2 (about 20%)
CO2
O2
O2
CO2 (dissolved in plasma 7-10%)
CO2 H2O H2CO3 HCO3 H
Slow
Fast
Cl
Cl
HCO3
HCO3 H H2CO3CO2 H2O
CO2 Hb HbCO2
HbO2 O2 HbRed blood cell
Carbonic
anhydrase
(Carbamino-
hemoglobin)
HHb
Chlorideshift(in) viatransportprotein
Binds toplasmaproteins
O2 (dissolved in plasma) Blood plasma
Partially saturated, fully saturatedHb Affinity for O2 varies with the extent of oxygen saturationRate of Hb binding/releasing oxygen dependent on PO2, temperature, blood pH, PCO2, and BPG (2,3 bisphosphoglycerate)
oxyhemoglobin
deoxyhemoglobin
As bicarbonate ion 70%
Transport and exchange of CO2
and O2 at lungsCO2
CO2
CO2
CO2
Alveolus
O2
O2
Fused basement membranes
CO2 (dissolved in plasma)
CO2 H2O H2CO3
Slow
Cl
HCO3
Chlorideshift(out) viatransportprotein
Blood plasmaO2 (dissolved in plasma)
Cl
HCO3 H H2CO3CO2 H2O
Carbonicanhydrase
Fast
CO2 Hb HbCO2(Carbamino-hemoglobin)
HbO2 H O2 HHbRed blood cell
HCO3 H
Oxygen pickup and carbon dioxide release in the lungs

10/8/2018
12
Respiratory centers in the brain stem Pons
Medulla
Pons
Medulla
Intercostal
nerves
External intercostalmuscles
Diaphragm
Dorsal respiratory group (DRG)
integrates peripheral sensory
input and modifies the rhythmsgenerated by the VRG.
Phrenic nerve (from C3, C4, C5) innervates the diaphragm.
Ventral respiratory group (VRG)
contains rhythm generators
whose output drives respiration.
Pontine respiratory centers
interact with the medullary
respiratory centers to smooththe respiratory pattern.
Changes in PCO
2regulate ventilation by a negative feedback mechanism
Arterial PCO2
PCO2decreases pH
in brain extracellular
fluid (ECF)
Central chemoreceptorsin brain stem respond toH in brain ECF (mediate70% of the CO2 response)
Peripheral chemoreceptorsin carotid and aortic bodies
(mediate 30% of the CO2
response)
Afferent impulses
Efferent impulses
Medullary
respiratory centers
Respiratory muscle
Ventilation(more CO2 exhaled)
Arterial PCO2and pH
return to normal
Initial stimulus
Physiological response
Result
Neural and chemical influences on brain stem respiratory centers
Higher brain centers(cerebral cortex—voluntarycontrol over breathing)
Respiratory centers(medulla and pons)
Stretch receptorsin lungs
Centralchemoreceptors
Peripheralchemoreceptors
Other receptors (e.g., pain)and emotional stimuli actingthrough the hypothalamus
Irritantreceptors
Receptors inmuscles and joints
O2,CO2,H
CO2,H

10/8/2018
13
Responding to Changing Conditions
• What causes change?
• Responses:• Reserve capacity built in
• In volume – structure of conducting passages, muscular involvement, lung involvement
• Dilation
• Recruitment
• In blood flow – adjustment in heart rate and lung involvement
• In hemoglobin – changes in affinity for O2
• In respiratory rate – stimulation from the brain
Respiratory Volumes And Capacities
6000
5000
4000
3000
2000
1000
0
Mil
lili
ters
(m
l)
Inspiratoryreserve volume
3100 ml
Tidal volume 500 ml
Expiratoryreserve volume
1200 ml
Residual volume1200 ml
Functionalresidualcapacity2400 ml
Inspiratorycapacity3600 ml Vital
capacity4800 ml
Total lungcapacity6000 ml
Spirographic record for a male

10/8/2018
14
Respiratory Volumes And Capacities
Respiratory
volumes
Respiratory
capacities
Summary of respiratory volumes and capacities for males and females
MeasurementAdult male
average value
Adult female
average value Description
Tidal volume (TV)
Inspiratory reservevolume (IRV)
Expiratory reservevolume (ERV)
Residual volume (RV)
Total lung capacity (TLC)
Vital capacity (VC)
Inspiratory capacity (IC)
Functional residualcapacity (FRC)
500 ml 500 ml
3100 ml 1900 ml
1200 ml 700 ml
1200 ml 1100 ml
6000 ml 4200 ml
4800 ml 3100 ml
3600 ml 2400 ml
2400 ml 1800 ml
Amount of air inhaled or exhaled with each breath under restingconditions
Amount of air that can be forcefully inhaled after a normal tidalvolume inspiration
Amount of air that can be forcefully exhaled after a normal tidalvolume expiration
Amount of air remaining in the lungs after a forced expiration
Maximum amount of air contained in lungs after a maximuminspiratory effort: TLC = TV IRV ERV RV
Maximum amount of air that can be expired after a maximuminspiratory effort: VC = TV IRV ERV
Maximum amount of air that can be inspired after a normal tidalvolume expiration: IC = TV IRV
Volume of air remaining in the lungs after a normal tidal volumeexpiration: FRC = ERV RV



![Respiratory system roadmap.pptx [Repaired] - Loginanatomical-sciences.health.wits.ac.za/roadmaps/Respiratory system... · DIVISION OF THE RESPIRATORY SYSTEM CONDUCTING PORTION Nasal](https://img.pdfslide.net/doc/110x75/5a78c3d87f8b9ae6228c9db0/respiratory-system-repaired-loginanatomical-scienceshealthwitsaczaroadmapsrespiratory.jpg)
![Respiratory System [โหมดความเข้ากันได้] · PATHOLOGY OF RESPIRATORY SYSTEM นพ. อรรณพ นาคะป ท Respiratory system U it](https://img.pdfslide.net/doc/110x75/5fa578efd4e80f055f6b3401/respiratory-system-aaaaaaaaaaaaaaaaaa-pathology.jpg)













![Anatomy and Physiology Respiratory System [Tab 2] Respiratory System](https://img.pdfslide.net/doc/110x75/56649ebd5503460f94bc631f/anatomy-and-physiology-respiratory-system-tab-2-respiratory-system.jpg)