Embed Size (px)
Citation preview

NO DIRECT ROLE FOR EPSTEIN-BARR VIRUS IN ORAL CARCINOGENESIS:A STUDY AT THE DNA, RNA AND PROTEIN LEVELS
Isabel CRUZ1,2, Adriaan J.C. VAN DEN BRULE
1, Antoinette A.T.P. BRINK1, Peter J.F. SNIJDERS
1, Jan M.M. WALBOOMERS1,
Isaac VAN DER WAAL2 and Chris J.L.M. MEIJER
1*1Unit of Molecular Pathology, Department of Pathology, University Hospital Vrije Universiteit, Amsterdam, The Netherlands2Department of Oral and Maxillofacial Surgery/Oral Pathology/ACTA, University Hospital Vrije Universiteit, Amsterdam,The Netherlands
Reports on the association of EBV with oral squamous-cellcarcinomas (OSCCs) are scarce and inconclusive. To deter-mine the potential role of EBV in oral carcinogenesis, weinvestigated 36 EBV DNA PCR-positive OSCCs for the ex-pression of EBV transcripts and proteins. From these EBVDNA-positive OSCCs, 13 were analysed for the presence ofEBV products, either at RNA and/or protein level. EBERtranscripts were investigated by RNA in situ hybridisation.EBNA-1, EBNA-2, LMP-1, LMP-2, BHRF1 and BARF0 tran-scripts were investigated by RT-PCR and/or NASBA.EBNA-1, LMP-1 and ZEBRA protein expressions were inves-tigated by immunohistochemistry. All 36 OSCCs were posi-tive for EBV DNA, using the highly sensitive BamHI W PCR,and 18 of these (50%) were positive using the less-sensitivePCR, which targets BNLF-1. However, virtually all OSCCstested failed to reveal EBV transcripts, including EBERs andEBNA-1 transcripts. No ZEBRA and LMP-1 proteins werefound in the neoplastic or any other cells of the OSCCsinvestigated. Immunohistochemistry using a monoclonal an-tibody (MAb) raised against EBNA-1 (2B4) resulted in posi-tive staining in some cases of OSCCs, but these results werenon-specific, since EBV-negative epithelial tissues showed ex-tensive non-specific staining and no EBNA-1-specific tran-scripts were detected by RT-PCR or NASBA. The absence ofexpression of EBV encoded transcripts and proteins indicatethat, with the present knowledge on EBV, an active role inoral carcinogenesis for this virus is unlikely. Int. J. Cancer 86:356–361, 2000.© 2000 Wiley-Liss, Inc.
Epstein-Barr virus (EBV) is the most highly transforming virusknown to date, as seen by the efficiency of production of lympho-blastoid cell lines (LCLs) uponin vitro infection of B lymphocyteswith EBV (Farrell et al., 1997). Paradoxically, this virus infects90% of the world population without causing disease in the ma-jority of individuals. In healthy immunocompetent individuals, thestrong control exerted by cytotoxic T cells (CTLs) prevents theexpression of the majority of viral proteins (Stevenet al., 1997).
After primary infection, EBV establishes lifelong (latent) infec-tion in the human body (Anagnostopoulos and Hummel, 1996;Farrellet al.,1997). The most accepted view concerning the sitesof viral persistence is that EBV latently infects a small proportionof long-lived (memory) B lymphocytes and periodically replicatesin the oropharynx, allowing infection of new hosts (Farrellet al.,1997).
The EBV receptor, CD21, is mainly found in B lymphocytes.However, other cells (e.g.,epithelial cells) are also permissive forEBV infection, either by use of a viral receptor (Talackoet al.,1991) or by IgA-mediated internalisation of the virus (Sixbey andYao, 1992). Accordingly, EBV has been associated not only withlymphoid but also with epithelial malignancies (Anagnostopoulosand Hummel, 1996) . Undifferentiated nasopharyngeal carcinoma(UNPC) and undifferentiated (“lympho-epithelioma-like”) gastriccarcinoma (UGC) are epithelial tumours that are strongly associ-ated with EBV DNA presence, and viral expression has beendemonstrated in the majority of neoplastic cells (Anagnostopoulosand Hummel, 1996; Osato and Imai, 1996). EBV DNA has beendetected in a smaller proportion of other epithelial malignancies
such as gastric adenocarcinoma (Osato and Imai, 1996), breastcancer (Labrecqueet al.,1995) and OSCC (Mao and Smoth, 1993;Lewensohn-Fuchset al., 1994; Horiuchiet al., 1995; Thomasetal., 1995), although there are conflicting results. Cautionary noteson interpretation of EBV-specific PCR data and the need to con-firm these data by morphological techniques and RNA expressionwere addressed previously (van den Bruleet al., 1995).
Three main patterns of EBV latency have been described so far(Oudejanset al., 1995; Niedobiteket al., 1997), depending par-tially on cell type and promoter used. EBERs and BARF0 RNAsare usually expressed in high copy numbers in the 3 types oflatency, but their functions remain obscure (Farrellet al., 1997).EBNA-1 is involved in episome maintenance and viral replication,possibly explaining its consistent presence in all types of virallatency so far described. In addition, EBNA-1 may have otherunidentified functions (Snuddenet al., 1995; Niedobiteket al.,1997), with possible oncogenic properties being suggested bystudies in transgenic mice (Wilsonet al.,1996). The ORF-encod-ing EBNA-1 is located in theBamHI Kregion of the viral genome.The size of the protein varies (69–96 kDa) according to the size ofits internal glycine/alanine repeat.
We and others (Mao and Smoth, 1993; Lewensohn-Fuchset al.,1994; Horiuchiet al.,1995; Thomaset al.,1995; Cruzet al.,1997)have detected EBV DNA in OSCC samples but, with the exceptionof 2 reports (Horiuchiet al.,1995; Thomaset al.,1995), EBV wasneither demonstrated in the neoplastic cells (Mao and Smoth,1993; Lewensohn-Fuchset al., 1994; Cruzet al., 1997) nor wasviral expression detected when this was attempted (Lewensohn-Fuchset al., 1994). The possibility that contaminating saliva orcells present in the specimen other than the neoplastic cells (e.g.,B lymphocytes and/or minor salivary glands) might be the sourceof viral DNA was not excluded. To clarify the possible involve-ment of EBV in oral carcinogenesis, we investigated the viralexpression at the RNA and protein levels in EBV DNA-positiveOSCCs.
MATERIAL AND METHODS
Patients and tissuesThirty-six frozen OSCC specimens from patients who were
examined at the Department of Oral and Maxillofacial Surgery andOtorhinolaryngology, University Hospital Vrije Universiteit, Am-sterdam, The Netherlands, have been previously analysed for thepresence of EBV DNA by polymerase chain reaction with 2 primerpairs (EBV 14/EBV 20 and LMP 1.1/LMP 1.3, which amplify,respectively, a fragment within the major internal repeat,BamHIW, and a fragment within the single copy gene,BNLF-1) (Cruzetal., 1997). From these we have selected 9 cases with relativelyhigh viral load and 4 cases with relatively low viral load. In the
*Correspondence to: Unit of Molecular Pathology, Department of Pa-thology, University Hospital Vrije Universiteit, De Boelelaan 1117, 1081HV Amsterdam, The Netherlands. Fax:131-20-4442964.E-mail: [email protected]
Received 23 June 1999; Revised 26 August 1999
Int. J. Cancer:86, 356–361 (2000)© 2000 Wiley-Liss, Inc.
Publication of the International Union Against Cancer
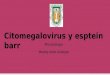
present study, we have analysed the expression of viral-specifictranscripts and/or proteins in these 13 cases (Fig.1). In 2 of these,the limited material available prevented analysis of EBERs andLMP-1, ZEBRA and EBNA-1 proteins.
Detection of EBV transcriptsEBERs RNAin situ hybridisation (RISH).Paraffin-embedded
tissue obtained from 11 EBV DNA containing OSCC as previ-ously determined by PCR (Cruzet al., 1997) were subjected toEBER 1/2 RNA in situ hybridisation (RISH) as previously de-scribed (Jiwaet al., 1993). EBV-positive Hodgkin’s lymphomaand nasopharyngeal carcinoma were used as positive controls.Negative controls included a tonsil specimen (EBV-negative) andOSCC samples hybridised with EBERs sense probes.
Reverse transcriptase-polymerase chain reaction (RT-PCR) forEBV transcripts.RNA was isolated from five 10-mm sections from10 snap-frozen biopsies of EBV DNA containing OSCC, using theRNAzol B method (Cinna/Biotecx, Houston, TX) (Brinket al.,1997). Reverse transcription was performed on 1mg of extractedRNA. For EBNA-1 detection, 10 pmol of the K antisense primerwere used, as previously described (Brinket al., 1997). Twogroups of alternative transcripts of EBNA-1 were analysed: thosederived from the C/W promoter and detected by the Y3-K pair, andthose derived from the F/Q promoter and detected by the Q-Kprimer pair (Oudejanset al.,1995; Brinket al.,1997). In addition,we investigated transcripts of BARF0 in 10 OSCCs, transcripts ofLMP-1 and BHRF1 in 9 OSCCs and transcripts of EBNA-2 andLMP-2 in 4 OSCCs using RT-PCR (Brinket al.,1997). For PCR,1.6 ml of the cDNA was used in a final volume of 50ml of PCR
solution as previously described (Brinket al.,1997). Samples weresubjected to 40 cycles of PCR. PCR products were analysed byelectrophoresis on 1.5% agarose gels and then transferred toQiabrane filters (Qiagen, Chatsworth, CA) by alkaline Southernblotting. To confirm the specificity of the PCR products generated,filters were hybridised with a specific gamma-32P end-labelledinternal oligo probe (U-probe) for EBNA-1 (Oudejanset al.,1995)and relevant probes for the other transcripts investigated (Brinketal., 1997).
Nucleic acid sequence-based amplification (NASBA) forEBNA-1 transcripts.Purified RNA (10 ng) was subjected toNASBA as previously described for EBV transcriptional analysis(Brink et al., 1998). NASBA reactions were carried out using theEBNA-1 1.2/EBNA-1 2.1 primer set, allowing the detection of awide array of EBNA-1 transcripts, including putative transcriptsfrom novel promoters (Brinket al.,1998). Reaction products wereevaluated by gel electrophoresis, transferred to nylon filters andhybridised to specific gamma-32P-ATP end-labelled oligonucleo-tide probe, as previously described (Brinket al., 1998).
Controls for RNA analysisQuality control for the isolated RNA from each individual
sample tested was performed by gel electrophoresis in which thepresence of 18S/28S ribosomal RNA served as a marker for properRNA quality (Brink et al.,1997). RT-PCR for the cellular snRNP-U1A transcripts (Brinket al.,1997) was performed in the tumourstested to allow detection of putative inhibitors of the RT-PCRreaction in individual samples. RNA extracted from JY cell line,Burkitt’s lymphoma, Hodgkin’s lymphoma and nasopharyngealcarcinoma were included as positive controls of the RT-PCR andNASBA reactions.
Immunohistochemical detection of EBV proteinsFour-mm sections from formalin-fixed, paraffin-embedded tis-
sues were mounted on poly-L-lysine-coated slides. Consecutivesections were used as negative control of the immunohistochem-ical (IHC) reaction and for H&E staining to confirm diagnosis.
The streptavidin-biotin complex immunoperoxidase techniqueused has previously been described in detail (Cruzet al., 1998).Antigen retrieval was performed by immersing slides in citrate ina microwave (600 W) at 100°C (33 5 min) for LMP1 and ZEBRAand in an autoclave (10 min) for EBNA-1 IHC. Primary antibodieswere incubated at room temperature for 1 hr: a. 2B4 (1:200), a ratMAb that was raised against bacterially expressed EBNA-1-lamb-da-cro/lacZ fusion protein that is devoid of the glycine/alanineEBNA-1 repeats (Gra¨sseret al.,1994); b. S12 (Organon, Teknika,Boxtel, The Netherlands) (1:100), a sensitive mouse MAb that wasraised against EBV LMP1-b-galactosidase fusion protein (Jiwaetal., 1995); c. BZ-1 (DAKO,Glostrap, Denmark)(1:100), a mouseMAb that recognises ZEBRA (Younget al., 1991). For EBNA-1IHC, the secondary antibody used was biotinylated rabbit anti-rat(1:100). After the secondary antibody, all cases were incubatedwith streptavidin-biotin complex horseradish peroxidase (1:200)for 1 hr. The catalysed reporter deposition (CARD) method wasused for amplification of EBNA-1 IHC.
In addition, frozen material obtained from 4 OSCCs were alsoinvestigated for EBNA-1 expression by IHC with the 2B4 anti-body.
Controls for IHCAs a positive control for EBNA-1, LMP-1 and ZEBRA IHC, we
used the JY cell line, which is a well-known EBV-transformedlymphoblastoid cell line expressing these viral products amongothers (Brinket al., 1997).
As negative controls for IHC, we used PBS instead of theprimary antibody. In addition, to test the specificity of the 2B4antibody, we performed immunohistochemistry in several biopsiesof normal human tissue using both the 2B4 antibody and anantibody raised against the non-EBV part of the fusion protein
FIGURE 1 – Schematic representation of EBV DNA status of 36OSCCs previously analysed by PCR. In this study, a proportion ofcases containing both relatively high (EBV1 1 1) and low (EBV1)viral load was selected to study viral expression (viral transcriptsand/or proteins). EBV1 1 1: EBV DNA detected in agarose gelscontainingBNLF-1 PCR products (confirmed by Southern blot andhybridisation of PCR products); EBV1: EBV DNA detected byBamHI WPCR but not byBNLF-1PCR; *EBV1 1: EBV sequencesfrom the BNLF-1 viral gene only detected after Southern blot andhybridisation of PCR products.
357EBV DNA AND VIRAL EXPRESSION IN OSCC

used to produce the 2B4 antibody (trpE, kindly provided by Dr. F.Grasser, Hamburg, Germany).
RESULTS
Presence of EBV DNA in OSCC as detected by PCR with 2pairs of primers
All 36 OSCCs previously analysed for EBV DNA using PCR(Cruzet al.,1997) and included in this study contained EBV DNAwhen the primers for the major internal repeat of the EBV genome(BamHI W) were used (Fig. 1). The presence of EBV was notdetected in 18 of these cases (50%) when PCR was performed withprimer pairs that amplify a fragment within the single copy gene ofthe viral genome (BNLF-1), indicating relatively low viral load(1) in the samples (Fig. 1). In 8 OSCCs (22.2%), EBV DNA wasdemonstrated when using primers for the single copy gene, butthese were only detected after Southern blot of the PCR productsand hybridisation with a radioactive internal probe. These caseswere classified as containing moderate levels of EBV DNA (11).The remaining 10 cases (27.8%) showed EBV DNA after PCRwith primers for the single copy gene,BNLF-1, and this wasalready detected when PCR products were run on an agarose geland the fragments were visualised by U.V. light. These cases wereclassified as containing relatively high amounts of EBV DNA(111) (Fig. 1).
RNA in situ hybridisation for EBERsRISH for EBER 1/2 was performed in the formalin-fixed, par-
affin-embedded sections of 11 OSCCs (Table I). Seven of thesecases contained relatively high amounts of EBV DNA (111),while 4 cases contained relatively low viral load (1). EBERRISH-specific signal was not detected in any of the cases tested,neither in epithelial nor in any other cells (Fig. 2a). RadioactiveRISH was performed in 6 of these cases (RISH kindly performedby Dr. G. Niedobitek, Erlangen, Germany), and in 2 of themisolated EBER-positive lymphocytes were detected after pro-longed exposure (results not shown). The EBV containingHodgkin’s lymphoma and nasopharyngeal carcinoma (Fig. 2b) thatserved as positive controls showed nuclear positivity, validatingthe results obtained with RISH.
RT-PCR and NASBA for EBV transcriptsRT-PCR performed in RNA extracted from 10 OSCCs that
harboured EBV DNA as detected by PCR did not reveal EBNA-1transcripts. A representation of the RT-PCR results is depicted inFigure 3. NASBA for EBNA-1 transcripts was performed in 5 of
these samples since this technique can detect potential newEBNA-1 transcripts from novel promoters (Brinket al.,1998). Allcases tested were negative using NASBA, confirming the RT-PCRresults for EBNA-1 transcripts.
None of the other EBV transcripts investigated by RT-PCR(EBNA-2, LMP-1, LMP-2 BHRF1 and BARF0) could be demon-strated, with the exception of 2 cases (Table I, T6, T8), in whichvery weak signals were obtained for LMP-1 and BARF0 tran-scripts. In these cases, none of the other viral products investigatedwas demonstrated in the neoplastic cells, including the LMP-1protein.
The JY cell line and EBV-positive tumours that were includedas positive controls revealed the relevant transcripts using bothRT-PCR (Fig. 3) and NASBA assays.
U1A transcripts could be successfully amplified in all OSCCsamples tested (Fig. 3). All OSCCs investigated showed strongribosomal bands corresponding to 18S/28S rRNA with the excep-tion of 2 cases (Table I, T5, T13), in which weak signals wereapparent. The demonstration of 18S/28S rRNA in all samplesanalysed indicates good RNA quality.
IHC analysis of LMP-1 and ZEBRA protein expression inOSCCs
Eleven OSCCs were tested for LMP-1 and ZEBRA proteins, butno staining was apparent in neoplastic or in any other cells (sali-vary glands of the submucosa when present or inflammatory cells).The JY cell line included as a positive control showed expressionof both viral proteins, validating the IHC procedure.
IHC analysis for expression of EBNA-1 proteinThe positive control used for this analysis consisted of an
EBV-infected cell line, JY, which expresses EBNA-1 among otherviral products. Virtually all cells present in the specimen werestained with the 2B4 antibody.
As a negative control, we used PBS instead of the primaryantibody, and no staining was visualised in the OSCC specimens.
Nine OSCCs previously shown to contain EBV DNA by PCR [5showing strong EBV signals (111) and 4 weak signals (1)]were analysed for expression of EBNA-1 protein by means of IHCwith 2B4 MAb. These carcinomas showed nuclear and/or cyto-plasmatic staining in a proportion of the neoplastic cells. However,upon prolonged washing, virtually all staining was removed.
Since no EBNA-1 transcripts were identified, we included ad-ditional negative controls allowing us to test the specificity of the
TABLE I – PRESENCE OF EBV DNA IN OSCCs IN RELATION TO VIRAL RNA AND PROTEIN EXPRESSION
Tn EBV DNA EBERRNA
EBNA-1RNA
EBNA-2RNA
LMP-1RNA
LMP-2RNA
BHRF1RNA
BARF0RNA
LMP-1protein
ZEBRAprotein
T1 111 2 2 2 2 2 2 2 2 2T2 111 2 2 ND 2 ND 2 2 2 2T3 111 2 2 ND 2 ND 2 2 2 2T4 111 2 2 2 2 2 2 2 2 2T5 111 22 2 2 2 2 2 2 2 2T61 111 ND 2 ND 1/2 ND 2 1/2 ND NDT71 111 ND 2 ND 2 ND 2 2 ND NDT8 111 2 2 ND 1/2 ND 2 1/2 2 2T9 111 2 2 ND 2 ND 2 2 2 2T10 1 22 ND ND ND ND ND ND 2 2T11 1 2 ND ND ND ND ND ND 2 2T12 1 2 ND ND ND ND ND ND 2 2T13 1 2 2 2 ND 2 ND 2 2 2HL 111 1 ND ND 1 1 ND ND ND NDNPC 111 1 ND ND ND ND ND ND ND NDBL 111 ND 1 ND ND ND ND ND ND NDJY 111 ND 1 1 1 1 1 1 1 1
EBV DNA (PCR): 111, positive at the gel level after PCR for EBV single copy gene (BNLF-1); 1, positive after PCR for EBV majorinternal repeat (BamHI W) (specificity confirmed using Southern blot of PCR products and hybridisation with internal probe). Controls: HL,Hodgkin’s lymphoma; NPC, nasopharyngeal carcinoma; BL, Burkitt’s lymphoma; JY, EBV-infected cell line. ND, not done.–1 Tissue notavailable for all analyses.–2 Isolated EBER-positive lymphocytes were seen after prolonged exposure when radioactive RISH was attempted.
358 CRUZ ET AL.

2B4 MAb. These consisted of surgical biopsies of normal epithe-lium of the aero-digestive tract (e.g.,oesophagus, stomach, colon,lung, salivary glands) obtained from individuals at the operatingroom. Several of these tissues showed broad staining with the 2B4antibody, localised mainly in the cytoplasm. Similar results wereobtained when we tested these tissues with the trpE MAb raisedagainst the non-EBV part of the fusion protein used to raise the2B4 MAb. This indicates that the 2B4 MAb cross-reacts withepithelia of the aero-digestive tract, preventing reliable interpreta-tion of the staining observed in OSCCs.
DISCUSSION
A role for EBV in OSCC has been suggested, but evidence forviral expression of transcripts and proteins is lacking. Our aims
were to determine which cellular compartment in OSCC samplesharbours EBV and to ascertain the possible role that the virusmight play in oral carcinogenesis. Accordingly, we investigatedseveral viral products that are commonly found in a variety ofEBV-associated malignancies, some of which have a knownpathogenic function. Even though all OSCCs harboured EBVDNA as detected by PCR and 28% of these appeared to have aconsiderable viral load, no viral products were demonstrated in theneoplastic cells.
None of the EBV transcripts investigated here were detected inthe OSCC samples, with the exception of 2 cases in which veryweak signals were obtained for LMP-1 and BARF0, after RT-PCR. These findings were particularly intriguing with regard toEBNA-1, EBERs and BARF0 transcripts. Indeed, EBNA-1 is
FIGURE 2 – (a) EBV DNA-positive OSCC as determined by PCR. EBER RNAin situ hybridisation did not reveal any transcripts in theneoplastic cells, Scale bar5 30 mm. (b) EBV-positive nasopharyngeal carcinoma that served as a positive control for EBER RNAin situhybridisation. Strong positive signals can be observed in virtually all nuclei of the neoplastic cells, Scale bar530 mm.
359EBV DNA AND VIRAL EXPRESSION IN OSCC

consistently expressed in all forms of latency described so far, andit is considered as being essential for viral persistence. Althoughthe function of EBERs and BARF0 is presently unknown, thesetranscripts are expressed in high amounts in the majority of ma-lignancies so far described that show an association with EBV.Some reports concerning epithelial malignancies have shown EBVor its products in neoplastic (Labrecqueet al., 1995; Sugawaraetal., 1999) or pre-neoplastic cells (Yanaiet al., 1997) using mor-phological techniques, while EBERs was not detected. However,these reports are rare and matter of debate.
The fact that no viral transcripts were demonstrated using highlysensitive techniques such as RT-PCR and NASBA suggests thatthe viral genomes detected by PCR in these samples are mainlytranscriptionally inactive. The weak LMP-1 and BARF0 transcrip-tion detected in 2 cases by RT-PCR is likely to reflect transcrip-tional activity in sporadic EBV-infected non-neoplastic cells (e.g.,tumour-infiltrating lymphocytes).
We also investigated ZEBRA and LMP-1 protein expression ina proportion of OSCCs containing EBV DNA, but none could bedemonstrated in the samples. This indicates that EBV productiveinfection is not present in OSCC samples, since the absence ofZEBRA precludes lytic infection (Anagnostopoulos and Hummel,1996). The absence of LMP-1, a viral protein with known trans-forming capacity (Wanget al.,1985; Anagnostopoulos and Hum-mel, 1996), confirms the results obtained with RT-PCR for theLMP-1 transcripts.
Although 9 samples tested by the EBNA-1 MAb (2B4) exhib-ited positive signals in neoplastic cells, upon prolonged washingvirtually all staining was abolished. In addition, by testing severalnormal tissues from the human aero-digestive tract, with either the2B4 MAb or the antibody raised against the non-EBV part of thefusion protein, extensive cytoplasmatic staining was observed,indicating that the 2B4 MAb cannot be reliably used for immu-nohistochemistry. Gra¨sseret al. (1994) tested this antibody againsta panel of EBV-negative cell lines, mainly of lymphoid origin, anddid not report non-specific staining in these cells but noted cross-reaction with endothelial cells. Moreover, in another study, EBV-negative epithelial cells showed non-specific cross-reactivity with2B4 (Murray et al., 1996), confirming our results on normalepithelial cells of the aero-digestive tract.
Previously, we did not find EBV DNA in the oral mucosa ofhealthy individuals using the same PCR protocol as for OSCCs(results not shown; Cruzet al.,1997). This suggested that EBV isnot commonly found at detectable amounts in samples of oralmucosa in the healthy population, even when sensitive techniquessuch as PCR are employed. There is, however, evidence that theimmune system of OSCC patients is often partially suppressed,and the possibility remains that EBV might be shed in higheramounts in the oropharynx of these patients without being causallyassociated with OSCCs. The possibility that infiltrating lympho-cytes might be the source of EBV DNA in these samples waspartly excluded by our present results, since EBV was only dem-onstrated occasionally in few cells and this was not even consis-tently found in all tumours analysed.
EBV DNA has been detected in OSCCs using PCR, but fewstudies attempted to determine the viral transcriptional programand/or the cellular localisation of the virus. Talackoet al. (1991),using sensitive ISH, could not demonstrate EBV in OSCCs, andLewensohn-Fuchset al. (1994) did not detect BHLF-1 or EBERtranscripts using RISH, nor ZEBRA by IHC, in any of the EBVDNA PCR-positive OSCCs analysed. In contrast, Horiuchiet al.(1995) observed EBV DNA and EBER-1 in the neoplastic cells of53% of EBV DNA PCR-positive OSCCs but no LMP-1 protein inthe tumours. Thomaset al. (1995) detected EBER and LMP-1protein in the neoplastic cells of OSCC developed in an immuno-suppressed individual who underwent renal transplantation, high-lighting the potential importance of the patient immune status as adeterminant for EBV-associated pathology in the oral mucosa, aspreviously noted for oral hairy leukoplakia (Greenspanet al.,1985).
In conclusion, the conflicting published data may be partiallyexplained by the methodology employed (e.g.,relative sensitivitiesand specificity of the tests used and the types of viral productsinvestigated) and/or by the patient population analysed (e.g., rel-ative competence of the immune system). Our results were ob-tained using several different techniques (i.e., EBER ISH, RT-PCR, NASBA and immunohistochemistry) and show that with thepresent knowledge of EBV latency patterns and using the availablemethodology, there is no evidence suggesting that EBV plays acausal role in oral carcinogenesis in individuals who do not sufferfrom severe immunosuppression. The presence of EBV DNA infrozen specimens of OSCC from these patients, as detected byPCR (Cruzet al., 1997), is likely to reflect increased shedding ofthe virus in the saliva.
ACKNOWLEDGEMENTS
The authors thank Drs. J. van der Wal and K.P. Schepman forhelpful collaboration in collecting clinical material and patientdata, Ms. T. Tadema for laboratory facilities, Ms. M. Vervaart andMs. I. Pronk for performing RNA analysis and IHC in frozentissue and Dr. G. Niedobitek for helpful discussions. Part of thiswork (I.C.) was supported by the Portuguese National Agency forResearch and Technology (JNICT)(PRAXIS XXI Programme).
FIGURE 3 – Representation of the RT-PCR results for EBV tran-scripts (EBNA-1 and BARF0) and for U1A, which served as qualitycontrol for RNA. 1, 2, 3, 4 (Table I cases T13, T1, T5, T4, respec-tively): OSCCs containing EBV DNA in relatively low (1) or high (2,3, 4) copy numbers;1: positive control. Lane 1: EBNA-1 transcriptsderived from the Q promoter and amplified by the Q-K primer pair.Only the positive control (Burkitt’s lymphoma) revealed a band of theexpected size (237 bp); OSCCs are negative. Lane 2: EBNA-1 tran-scripts derived from the C/W promoter and amplified with the Y3-Kprimer pair. The positive control (JY cell line) revealed a band of theexpected size (266 bp), while OSCCs (1–4) are negative. Lane 3:BARF0 transcripts. Only the positive control (JY cell line) shows aband of the expected size (232 bp); OSCCs (1–4) are negative. Lane4: RT-PCR for the U1A transcript. All OSCCs analysed (1–4) and thepositive control (JY cell line) revealed a band of the expected size (226bp), indicating presence of good-quality RNA.
360 CRUZ ET AL.

REFERENCES
ANAGNOSTOPOULOS, I. and HUMMEL, M., Epstein-Barr virus in tumours.Histopathology, 29, 297–315 (1996).BRINK, A.A.T.P., OUDEJANS, J.J., JIWA, M., WALBOOMERS, J.M.M., MEIJER,C.J.L.M. and VAN DEN BRULE, A.J.C., Multiprimed cDNA synthesis fol-lowed by PCR is the most suitable method for Epstein-Barr virus transcriptanalysis in small lymphoma biopsies.Mol. cell. Probes,11,39–47 (1997).BRINK, A.A.T.P., VERVOORT, M.B.H.J., MIDDELDORP, J.M., MEIJER,C.J.L.M. and VAN DEN BRULE, A.J.C., Nucleic acid sequence-based ampli-fication, a new method for analysis of spliced and unspliced Epstein-Barrvirus latent transcripts, and its comparison with reverse transcriptase PCR.J. clin. Microbiol., 36, 3164–3169 (1998).CRUZ, I., VAN DEN BRULE, A.J.C., STEENBERGEN, R.D.M., SNIJDERS, P.J.F.,MEIJER, C.J.L.M., WALBOOMERS, J.M.M., SNOW, G.B. and VAN DER WAAL,I., Prevalence of Epstein-Barr virus in oral squamous cell carcinomas,premalignant lesions and normal mucosa—a study using the polymerasechain reaction.Oral Oncol.,33, 182–188 (1997).CRUZ, I.B., SNIJDERS, P.J., MEIJER, C.J., BRAAKHUIS, B.J., SNOW, G.B.,WALBOOMERS, J.M. and VAN DER WAAL, I., P53 expression above the basalcell layer in oral mucosa is an early event of malignant transformation andhas predictive value for developing oral squamous cell carcinoma.J. Pathol.,184,360–368 (1998).FARRELL, P.J., CLUDTS, I. and STUHLER, A., Epstein-Barr virus genes andcancer cells.Biomed. Pharmacother.,51, 258–267 (1997).GRASSER, F.A., MURRAY, P.G., KREMMER, E., KLEIN, K., REMBERGER, K.,FEIDEN, W., REYNOLDS, G., NIEDOBITEK, G., YOUNG, L.S. and MUELLER-LANTZSCH, N., Monoclonal antibodies directed against the Epstein-Barrvirus encoded nuclear antigen 1 (EBNA-1): immunohistological detectionof EBNA-1 in the malignant cells of Hodgkin’s disease.Blood, 84, 3792–3798 (1994).GREENSPAN, J.S., GREENSPAN, D., LENNETTE, E.T., ABRAMS, D.I., CONANT,M.A., PETERSEN, V. and FREESE, U.K., Replication of Epstein-Barr viruswithin the epithelial cells of oral “hairy” leukoplakia, an AIDS associatedlesion.N. Engl. J. Med.,313,1564–1571 (1985).HORIUCHI, K., MISHIMA, K., ICHIJIMA, K., SUGIMURA, M., ISHIDA, T. andKIRITA, T., Epstein-Barr virus in the proliferative diseases of squamousepithelium in the oral cavity.Oral Surg. Oral Med. Oral Pathol.OralRadiol. Endod.,79, 57–63 (1995).JIWA, N.M., KANAVAROS, P., VAN DER VALK , P., WALBOOMERS, J.M.M.,HORSTMAN, A., VOS, W., MULLINK , H. and MEIJER, C.J.L.M., Expression ofc-myc and bcl-2 oncogene products in Reed Stenberg cells independent ofthe presence of Epstein-Barr virus.J. clin. Pathol.,46, 211–217 (1993).JIWA, N.M., OUDEJANS, J.J., DUKERS, D.F., VOS, W., HORSTMAN, A., VANDER VALK, P., MIDDLEDORP, J.M., WALBOOMERS, J.M.M. and MEIJER,C.J.L.M., Immunohistochemical demonstration of different latent mem-brane protein-1 epitopes of Epstein-Barr virus in lymphoproliferative dis-eases.J. clin. Pathol.,48, 438–442 (1995).LABRECQUE, L.G., BARNES, D.M., FENTIMAN, I.S. and GRIFFIN, B.E., Ep-stein-Barr virus in epithelial cell tumours: a breast cancer study.CancerRes.,55, 39–45 (1995).LEWENSOHN-FUCHS, I., MUNCK-WIKLAND , E., BERKE, Z., PALLESEN, G.,LINDE, A., WIMAN , K.G. and DALIANIS , T., Detection of human papillo-mavirus, Epstein-Barr virus and elevated p53 expression in squamous cellcarcinomas of the head and neck.In: M.A. Stanley (ed.),Immunology ofhuman papillomaviruses,pp. 15–20, Plenum Press, New York (1994).MAO, E.-H., SMOTH, C.J., Detection of Epstein-Barr virus (EBV) DNA by
the polymerase chain reaction in oral smears from healthy individuals andpatients with squamous cell carcinoma.J. oral Pathol. Med.,22, 12–17(1993).MURRAY, P.G., NIEDOBITEK, G., KREMMER, E., GRASSER, F., REYNOLDS,G.M., CRUCHLEY, A., WILLIAMS , D.M., MULLER-LANTZSCH, N. and YOUNG,L.S., In situ detection of the Epstein-Barr virus encoded nuclear antigen 1in oral hairy leukoplakia and virus-associated carcinomas.J. Pathol.,178,44–47 (1996).NIEDOBITEK, G., YOUNG, L.S. and HERBST, H., Epstein-Barr virus infectionand the pathogenesis of malignant lymphomas.Cancer Surv.,30,143–162(1997).OSATO, T. and IMAI , S., Epstein-Barr virus and gastric carcinoma.Semin.Cancer Biol.,7, 175–182 (1996).OUDEJANS, J.J., VAN DEN BRULE, A.J.C., JIWA, N.M., DE BRUIN, P.C.,OSSENKOPPELE, G.J., VAN DER VALK , P., WALBOOMERS, J.M.M. and MEIJER,C.J.L.M., BHRF1, the Epstein-Barr virus (EBV) homologue of the bcl-2proto-oncogene, is transcribed in EBV-associated B-cell lymphomas and inreactive lymphocytes.Blood, 86, 1893–1902 (1995).SIXBEY, J.W. and YAO, Q.-Y., Immunoglobulin A-induced shift of Epstein-Barr virus tissue tropism.Science,255,1578–1579 (1992).SNUDDEN, D.K., SMITH, P.R., LAI, D., NG, M.-H. and GRIFFIN, B.E.,Alterations in the structure of the EBV nuclear antigen, EBNA1, inepithelial cell tumours.Oncogene, 10, 1545–1552 (1995).STEVEN, N.M., ANNELS, N., KUMAR, A., LEESE, A., KURILLA , M.G. andRICKINSON, A.B., Immediate early and early lytic cycle proteins are fre-quent targets of the Epstein-Barr virus-induced cytotoxic T cell response.J. exp. Med.,185,1605–1617 (1997).SUGAWARA, Y., MIZUGAKI , Y., UCHIDA, T., TORIJ, T., IMAI , S., MAKUUCHI,M. and TAKADA , K., Detection of Epstein-Barr virus (EBV) in hepatocel-lular carcinoma tissue: a novel EBV latency characterised by the absenceof EBV-encoded small RNA expression.Virology, 256,196–202 (1999).TALACKO, A.A., TEO, C.G., GRIFFIN, B.E., JOHNSON, N.W., Epstein-Barrreceptors but not viral DNA are present in normal and malignant oralepithelium.J. oral Pathol. Med.,20, 20–25 (1991).THOMAS, D.W., RAMSAHOYE, B., JASANI, B. and LIM, S.H., Epstein-Barrvirus in squamous cell carcinoma after renal transplant.Transplantation,60, 390–392 (1995).VAN DEN BRULE, A.J.C., WALBOOMERS, J.M.M. and MEIJER, C.J.L.M.,Epstein-Barr virus infection as a co-factor in cervical carcinogenesis?J. Pathol.,176,219–220 (1995).WANG, D., LIEBOWITZ, D. and KIEFF, E., An EBV membrane proteinexpressed in immortalised lymphocytes transforms established rodentcells.Cell, 43, 831–840 (1985).WILSON, J.B., BELL, J.L. and LEVINE, A.J., Expression of Epstein-Barr virusnuclear antigen-1 induces B cell neoplasia in transgenic mice.EMBO J.,15, 3117–3126 (1996).YANAI , H., TAKADA , K., SHIMIZU , N., MIZUGAKI , Y., MASAHIRO, T. andOKITA , K., Epstein-Barr virus infection in non-carcinomatous gastric epi-thelium.J. Pathol.,183,293–298 (1997).YOUNG, L.S., L R., ROWE, M., NIEDOBITEK, G., PACKHAM , G., SHANAHAM ,F., ROWE, D.T., GREENSPAN, D., GREENSPAN, J.S., RICKINSON, A.B. andFARRELL, P.J., Differentiation-associated expression of the Epstein-Barrvirus BZLF1 transactivator protein in oral hairy leukoplakia.J. Virol., 65,2868–2874 (1991).
361EBV DNA AND VIRAL EXPRESSION IN OSCC