Embed Size (px)
DESCRIPTION
JOURNAL
Citation preview

Hypertension in Pregnancy, 31:79–90, 2012Copyright © Informa Healthcare USA, Inc.ISSN: 1064-1955 print/1525-6065 onlineDOI: 10.3109/10641955.2010.525277
LHIP1064-19551525-6065Hypertension in Pregnancy, Vol. 1, No. 1, Sep 2010: pp. 0–0Hypertension in PregnancyStandardized Mississippi Protocol Treatment of 190 Patients with HELLP Syndrome: Slowing Disease Progression and Preventing New Major Maternal MorbidityMississippi Protocol Management of HELLP SyndromeMartin et al.
James N. Martin Jr. MD, Michelle Y. Owens MD, MS, Sharon D. Keiser MD, MS, Marc R. Parrish DO, Kiran B. Tam Tam MD, Justin M. Brewer MD, Julie L. Cushman RN, and Warren L. May PhD
Division of Maternal–Fetal Medicine, Department of Obstetrics and Gynecology, and the Biostatistics Center, University of Mississippi Medical Center, Jackson, MS, USA
Objective. To evaluate the effectiveness of the Mississippi Protocol (MP) to treatHELLP (hemolysis, elevated liver enzymes, and low platelets) syndrome. Methods.Uniform early initiation of MP (corticosteroids, magnesium sulfate, systolic blood pres-sure control) was studied prospectively in patients admitted with severe preeclampsia/class 1 or class 2 HELLP syndrome. Results. One hundred and ninety patients between2000 and 2007 received MP without suffering maternal death, stroke, or liver rupture.Only 39 of 163 patients (24%) not class 1 when MP began progressed to class 1 disease;only 18.2% of class 1 and 2.4% of class 2 subsequently developed major maternalmorbidity. Conclusion. Early initiation of MP inhibits HELLP syndrome diseaseprogression and severity.
Keywords HELLP syndrome, Hypertension, Preeclampsia, Thrombocytopenia.
INTRODUCTIONOne of the most feared presentations within the pantheon of preeclampsia-related disease affecting the obstetric patient is the development of HELLP(hemolysis, elevated liver enzymes, and low platelets) syndrome, a form ofsevere preeclampsia/eclampsia manifested by laboratory evidence of hepaticdysfunction and damage, microangiopathic hemolytic anemia, and thrombocy-topenia (1–4). The risk of serious morbidity correlates in general with increas-ingly severe signs, symptoms, and laboratory abnormalities. This isfundamental to the development and clinical utilization of the Mississippithree-class system for patient management with HELLP syndrome pregnan-
Presented at the Central Association of Obstetricians and Gynecologists 76th Annual Meeting, Wailea, Maui, Hawaii, October 25–28, 2009.Address correspondence to James N. Martin Jr., Division of Maternal–Fetal Medicine, Department of Obstetrics and Gynecology, and the Biostatistics Center, University of Mississippi Medical Center, Jackson, MS 39216, USA. E-mail: jnmartin@ob-gyn. umsmed.edu
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

80 Martin et al.
cies (2,4). Because maternal morbidity is greatest and maternal mortality ismost likely when HELLP syndrome deteriorates to a class 1 designation, afundamental tenet of management is a protocol to prevent disease progressiononce diagnosed. Delivery is the cornerstone of therapy because it removes theplacenta from the mother’s uterus and eliminates placental production offactors important in the pathogenesis of the disorder. During the inductionand delivery process as well as the early puerperium, magnesium sulfate isgiven intravenously to the patient to reduce systemic vascular resistance andto prevent eclamptic seizures, and antihypertensives are utilized to preventstroke and other complications related to severe systolic and/or diastolichypertension (4–6).
Retrospective case–control studies and small prospective randomized trialsin the early 1990s suggested that use of certain corticosteroids, in addition toseizure prevention and blood pressure control, appeared to benefit both perin-atal and maternal care of patients with HELLP syndrome (4). Havingwitnessed ongoing evidence of apparent intravenous dexamethasone efficacywhile caring for hundreds of HELLP syndrome patients managed from theearly 1990s onward, in addition to being aware of the high morbidity andmultiple complications of HELLP syndrome patients managed in the 1980swithout corticosteroid administration, the senior investigator increasinglyintegrated the routine use of intravenous dexamethasone into the care of allpatients developing evidence of HELLP syndrome after 1994 at the Universityof Mississippi Medical Center. In combination with magnesium sulfate andefforts to minimize severe systolic hypertension, these three therapies wereincorporated into a uniform, aggressively applied protocol of HELLP syndromemanagement that was initiated at the beginning of 2000 as “the MississippiProtocol” (MP). The rationale and literature evidence to support this manage-ment approach was summarized only recently (4). This report is the first sum-mary of our experience with this expanded approach to further improvingpatient outcomes with this form of severe preeclampsia.
The purpose of this report is to evaluate maternal and perinatal outcomeswith MP management of patients with a final diagnosis of complete class 1 orclass 2 HELLP syndrome who received tertiary care in our regional medicalcenter after 1999.
MATERIALS AND METHODSAll pregnant patients diagnosed with HELLP syndrome at the Winfred L.Wiser Hospital for Women & Infants, University of Mississippi MedicalCenter in Jackson after January 1, 2000, were prospectively managed by theMP and considered for study inclusion. Data were entered into a much moredetailed and expanded database from that used (Mississippi HELLPSyndrome Database) for prior studies (2,7). For this report, only patients whosatisfied all criteria to merit a final diagnosis of class 1 or class 2 HELLP syn-drome were included. Patients with class 1 HELLP exhibited severe thromb-ocytopenia with a perinatal platelet nadir ≤50,000/μL, a total serum lactatedehydrogenase (LDH) of ≥600 IU/L, and serum transaminase level of ≥70 IU/Las aspartate aminotransferase (AST) and/or alanine aminotransferase (ALT).
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

Mississippi Protocol Management of HELLP Syndrome 81
Evidence of red cell hemolysis was present with regard to abnormal cell forms orfragments and the presence of urinary bilirubin or increased indirect biliru-bin. Patients with class 2 HELLP syndrome had similar laboratory thresholdsto class 1, except for less profound thrombocytopenia (platelet nadir between>50,000 and ≤100,000/μL). All patients also had signs, symptoms, and labora-tory findings that were consistent with a diagnosis of preeclampsia/eclampsiaduring their antepartum/postpartum course. Patients who satisfied all crite-ria to merit a final diagnosis of class 3 HELLP syndrome (mild thrombocy-topenia with platelet nadir >100,000 but ≤150,000, total LDH ≥600 IU/L, andAST or ALT ≥40 IU/L) or incomplete HELLP syndrome (only two of threeplatelet/LDH/AST criteria present) are excluded from this report. We empha-size that a patient’s HELLP classification is dynamic and can change overtime; the most advanced class developed is the final diagnosis coded. If apatient was originally considered to exhibit probable HELLP syndrome butwas subsequently determined to have a different disease process (HELLPlaboratory parameters developed secondary to thrombotic thrombocytopenicpurpura (TTP), disseminated intravascular coagulation (DIC), acute fattyliver of pregnancy, connective tissue disease flare, vasoocclusive sickle cell cri-sis, severe placental abruption, or sepsis-initiated hypoxic/hypovolemic shocktissue injury particularly to the kidney), she was excluded from this reportand included in a separate publication for these uniquely complex patients (8).
Major maternal morbidity incurred by any study patient includes any ofthe following by category: cardiopulmonary complications of pulmonary edema,pleural or pericardial effusion, required intubation with ventilator support, con-gestive heart failure, myocardial infarction or arrest; hematologic/coagulationcomplications of DIC (partial thromboplastin time ≥40 s and fibrinogen <200mg/dL) or transfusion of blood products; central nervous system/visual compli-cations of stroke, cerebral edema, hypertensive encephalopathy, or vision loss;hepatic complications of subcapsular liver hematoma or rupture; and renalcomplications if serum creatinine >1.2 mg/dL with acute tubular necrosis oracute renal failure. Major perinatal morbidity includes any of the following:respiratory distress syndrome, hyaline membrane disease, intraventricularhemorrhage, 5-min Apgar ≤3, or arterial cord gas pH ≤7.0 at birth. Standarddiagnostic criteria for each entity were used and evaluated for accuracy foreach study subject.
The MP for management of HELLP syndrome (MPRx) includes three majorcomponents: (i) magnesium sulfate by intravenous infusion primarily foreclampsia seizure prophylaxis and reduction of systemic vascular resistance,through delivery and up to 24 h postpartum with duration dependent on dis-ease acuity and whether HELLP syndrome is first-evidenced postpartum; (ii)blood pressure control using oral or intravenous medication (hydralazine orlabetalol) to sustain systolic blood pressure <160 mmHg and diastolic bloodpressure <100 mmHg; and (iii) intravenous dexamethasone 10 mg at 12-hintervals until platelet normalization is trending toward 100,000/μL at whichtime 5 mg dexamethasone at 12-h intervals is administered twice intrave-nously before cessation to minimize the risk of rebound thrombocytopenia.Intravenous dexamethasone for patients with HELLP syndrome is initiated inthe following circumstance(s): (i) a diagnosis of class 1 or class 2 HELLP
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

82 Martin et al.
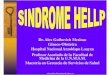
syndrome is made ante- or postpartum; or (ii) a diagnosis of class 3 HELLPsyndrome is made in association with one of the following complications: (a)eclampsia, (b) difficult to control severe systolic hypertension, (c) severe epi-gastric pain, and/or (d) evidence of significant system/multiorgan compromiseinvolving the heart, lungs, kidneys, or central nervous system (4). This isdepicted in Figure 1. Intravenous dexamethasone for HELLP syndrome treat-ment purposes is adequate for fetal lung maturation treatment purposes if fetallung immaturity is present. Once a diagnosis of class 1 or class 2 HELLP syn-drome is made, the MP is begun with planned delivery to occur within 48–72 hto enable fetal lung maturation corticosteroid benefit to be achieved and formaternal laboratory parameters of HELLP syndrome to begin a normalizingtrend. With rare exception and not in this series, the so-called expectantmanagement is not undertaken even if gestational age is <23–24 weeks. Oncecompleted, the findings in patients with final diagnoses of class 3 HELLPsyndrome or incomplete HELLP syndrome during the same time interval areplanned for later publication.
Implementation of the MP has five goals of therapy: (i) to prevent thedevelopment of class 1 HELLP syndrome from class 2 or complicated class 3HELLP syndrome; (ii) to minimize the development of major maternal mor-bidity as defined; (iii) to prevent maternal mortality; (iv) to shorten the course
Figure 1: Intravenous dexamethasone for patients with HELLP syndrome.
Preeclampsia/Eclampsia/HELLP Syndrome>16 weeks gestation
Class 1 or 2 HELLP Syndrome?(PLT <100K/uL, LDH>600AST/ALT>70, +Schistocytes,Ind. Bili >1.2)
NO
Class 3 or PartialHELLP
Syndrome?
NO
NO
INITIATE IVDEXAMETHASONE
10mg IV q 12HOURS
CONSIDER IVDEXAMETHASONE
10mg IV q 12 HOURS
NO
Severe HypertentionDifficult to Control,or CNS Symptoms?
SevereEpigastric Pain?
Continue CurrentManagement without
IV Dexamethasone
End-Organ Injury (renal,hepatic, CVS, CNS) and/orabruption-DIC?
NO
NO
YES
YES Eclampsia?
YES
YES
YES
YES
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

Mississippi Protocol Management of HELLP Syndrome 83
of disease and the length of hospitalization; and (v) to minimize perinatalmortality and major morbidity.
Data were collected and analyzed by appropriate tests for continuous (inde-pendent samples t-tests, Mann–Whitney) or categorical (chi-square, Fisher’sexact test) outcomes with differences considered significant if p < 0.05.
RESULTSDuring the 8-year span between 2000 and 2007, 27,494 live births occurred inthe University of Mississippi Medical Center (Winfred L. Wiser Hospital forWomen & Infants) including 190 patients who met the study inclusion criteriaand were treated with the MP (1 every 145 live births; 0.7%). No maternaldeaths, strokes, or liver ruptures occurred among 66 patients with class 1(34.7%) and 124 patients with class 2 (65.3%) HELLP syndrome. Demographicand delivery details are shown in Table 1 for the two class groups, and theprofile of presentation indicating disease severity in each group is detailed inTable 2. Details of laboratory findings including the LDH to AST ratio areshown in Table 3. Placental abruption occurred in 15.2% of class 1 and 8.1% ofclass 2 HELLP patients (p = 0.14). Most of the 190 patients in the series hadantepartum-onset disease (85%).
Approximately 40% of the patients who developed complete class 1 HELLPsyndrome (27 of 66 or 40.9%) had met criteria for the most advanced stage ofdisease at the time of transfer and/or hospital admission. Following the initia-tion of MP, only 39 of the other 163 patients with class 2 HELLP syndromeprogressed to class 1 (23.9%). Major maternal morbidity was present atadmission in 33.3% versus 9.7% of the class 1 and class 2 groups, respectively(p < 0.001); following admission and MP initiation, only 18.2% of class 1 versus2.4% of class 2 HELLP patients (p < 0.001) developed new onset major mater-nal morbidity (see Table 4).
Table 1: Maternal demographics and delivery data for patients with a FINAL diagnosis ofclass 1 or class 2 HELLP syndrome.
Final diagnosis ofClass 1 HELLP
syndromeClass 2 HELLP
syndrome p-Value
N 66 patients 124 patientsMaternal age at delivery (years) 24.6 ± 5.6 24.2 ± 6.1 NSMaternal weight at admission (lbs) 183 ± 57 189 ± 47 NSMaternal BMI at admission 32 ± 9 32 ± 7 NSRace/ethnicity (% African-American) 74% 78% NSNulliparous 47% 58% NSMultiparous 59% 52% NSGestational age at delivery (weeks) 30.7 ± 4.5 31.2 ± 5.1 NSCesarean delivery 67% 60% NSPrior cesarean delivery 15% 15% NSPatient transfer to UMMC for care 86% 84% NS
Note: Means are ±1 SD; NS, Non-Significant difference with p > 0.05.
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

84 Martin et al.
With regard to interventions, 47% of patients in class 1 received bloodproduct transfusions of some type versus 11.3% in class 2 (p < 0.001); afteradmission and initiation of MP, only 4.6% of patients in class 1 requiredplatelet transfusions versus 22.7% who had received them before transfer andinitiation of MP. One patient who developed criteria to merit a final diagnosisof class 2 HELLP group had a subcapsular liver hematoma noted before hospital
Table 2: Admission signs and symptoms before initiating Mississippi Protocol (MP) treatment.
Final diagnosis ofClass 1 HELLP
syndromeClass 2 HELLP
syndrome p-Value
N 66 patients 124 patientsSystolic blood pressure (mmHg) 150 ± 21 154 ± 19 NSDiastolic blood pressure (mmHg) 90 ± 18 94 ± 15 NSMean arterial pressure (mmHg) 110 ± 18 114 ± 15 NSDipstick proteinuria (1+ or 2+) 24% 13% NSDipstick proteinuria (3+ or 4+) 53% 55% NSHematuria (micro/macro) 32% 23% NSNausea/vomiting 33% 15% 0.0041Epigastric pain 30% 14% 0.006Headache 50% 51% NSVisual impairment 12% 15% NSFacial edema 14% 13% NSEclampsia 6% 4% NSUric acid >5.5 mg/dL (%) 76% 69% NSLDH ≥600 IU/L 100% 89% 0.0026AST ≥70 IU/L 68% 49% 0.0142ALT ≥70 IU/L 44% 23% 0.0034Creatinine > 1.2 mg/dL 12% 9% NSPlatelet count ≤50,000/μL 41% 0% <0.001Platelet count >50,000 – ≤100,000/μL 24% 53% <0.001Platelet count >100,000 – ≤150,000/μL 21% 24% NSPlatelet count >150,000/μL 14% 23% NS
Note: The values reported above are the ADMISSION values for patients who eventuallyachieved a FINAL diagnosis of class 1 HELLP syndrome or class 2 HELLP syndrome; NS,Non-Significant difference with p > 0.05.
Table 3: Peak severity of laboratory values according to FINAL HELLP syndromeclassification.
Final diagnosis ofClass 1 HELLP
syndromeClass 2 HELLP
syndrome p-Value
N 66 patients 124 patientsPlatelet nadir (μL) 34,800 ± 12,500/μL 75,500 ± 14,200/μL <0.001Peak total LDH (IU/L) 5288 ± 4190 IU/L 2553 ± 3329 IU/L <0.001Peak AST (IU/L) 671 ± 743 IU/L 319 ± 695 IU/L 0.0014LDH: AST ratio (mean) 15.4 ± 15.4 17.3 ± 13.5 NSLDH: AST ratio (range) 1.1 – 88.4 1.6 – 62.2 NSUric acid (mg/dL) 7.5 ± 2 7.2 ± 2 NSCreatinine (mg/dL) 1.25 ± 0.9 0.99 ± 0.8 0.0396
Note: NS, Non-Significant difference with p > 0.05.
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

Mississippi Protocol Management of HELLP Syndrome 85
transfer and initiation of MP; at the time of diagnosis of the liver hematomathe patient met class 3 HELLP syndrome criteria. All patients in the seriesreceived intravenous dexamethasone; most patients (71.2% in class 1, 78.2%in class 2) had them initiated antepartum, the remainder intrapartum or post-partum with one exception (a patient barely meeting criteria for class 2HELLP syndrome). Magnesium sulfate was administered to 98.8% of patientsin this series; antihypertensives were required in 43.9% of class 1 patientsand 41.1% of class 2 to reduce systolic blood pressure to less than 160 mmHg,an insignificant difference. Length of hospitalization before delivery did not dif-fer between class 1 and class 2 groups (mean 12.5 vs. 14 h, p = 0.39); length ofhospitalization following delivery, however, was significantly longer in class 1patients than in class 2 (mean 108 vs. 96 h, 4.5 vs. 4 days, p < 0.001).
Important perinatal outcomes for class 1 and class 2 HELLP syndrome preg-nancies, respectively, included mean birthweights (1348 ± 691 g, 1531 ± 942 g),major perinatal morbidity (59.1%, 55.7%), and perinatal mortality (197 : 1000vs. 186 : 1000) based on 19.7% stillbirths and no neonatal deaths in the class1 group and 12.1% stillbirths and 6.5% neonatal deaths in the class 2 group.All stillbirths happened before hospital admission or during labor in a patientdeemed to be not a candidate for cesarean delivery for reasons of extremeprematurity. The high perinatal mortality rate for both groups was negativelyimpacted by the 17 mothers (6 in class 1 and 11 in class 2) who requireddelivery before 24-week gestation.
DISCUSSIONThe current investigation, adding emphasis on reducing systolic blood pres-sures to less than 160 mmHg in addition to intravenously infused magnesiumsulfate and dexamethasone, further expands upon the reported experience ofour institution with HELLP syndrome which previously spanned the yearsbetween the early 1980s and 2000. After the failure in 1999 of a proposal to
Table 4: Major maternal morbidity pre- and post-MP initiation.
Final diagnosis ofClass 1 HELLP
syndromeClass 2 HELLP
syndrome p-Value
N 66 patients 124 patientsPre-MP/hospital admission 22/66 (33.3%) 12/124 (9.7%) <0.001
Hematologic/coagulation 21 12Cardiopulmonary 3 1CNS/visual 0 0Renal 3 1Hepatic 0 1
During MP/hospitalization 12/66 (18.2%) 3/124 (2.4%) <0.001Hematologic/coagulation 10 2Cardiopulmonary 1 1CNS/visual 0 0Renal 2 0Hepatic 0 0
Note: MP, Mississippi Protocol treatment.
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

86 Martin et al.
NIH to fund a 26-center prospective randomized and placebo-blinded trialinvolving 1000+ patients with class 1 and class 2 HELLP syndrome to com-pare intravenous dexamethasone versus placebo administration uponantepartum–postpartum, preterm–term, and disease progression issues with/without major maternal morbidity, we initiated the present single institutionseries to explore how well an expanded MP might help achieve the five goalsof HELLP syndrome therapy in a variety of clinical circumstances. Uniform,early, and aggressive application of the MP as described for the managementof patients with HELLP syndrome usually resulted in successful maternaloutcomes. Only patients with a final diagnosis of class 1 or class 2 HELLPsyndrome as severe preeclampsia were considered in this report, and the pro-tocol therapy was begun quickly as soon as a diagnosis was made; 85% ofcases had treatment initiated before delivery. This series achieved four of fivegoals: absence of maternal mortality, a reduction of major maternal morbidityto <20% in class 1 and <5% in class 2, a low rate of class 3 or class 2 HELLPsyndrome disease progression to the most advanced disease class 1 HELLPsyndrome in patients managed with this protocol, and a mean length of hospi-talization following delivery of only 4–4.5 days. A fifth goal of improved perin-atal outcome was not clearly achieved; poor perinatal outcome because ofextreme prematurity remains a significant concern with this disease entityregardless of treatment(s) employed. The overall value of the clinical strategyusing corticosteroids (intravenous dexamethasone) as an early and integralcomponent of care for patients with HELLP syndrome is again affirmed inthis latest series of 190 patients among more than 400 patients so managed inthis tertiary care center since the early 1990s.
Between the initiation and conclusion of the present 8-year observationaltrial, two large prospective randomized clinical trials using intravenous dex-amethasone versus placebo in patients with HELLP syndrome have beenreported. The first, undertaken in Columbia by Fonseca and colleagues with132 patients, has been severely criticized for multiple shortcomings that ren-der untenable their conclusion that dexamethasone treatment does notimprove the outcome of women with HELLP syndrome (9). Indeed, closeinspection of the data demonstrated that patients with class 1 HELLPsyndrome who received intravenous dexamethasone recovered significantlyfaster than the untreated control group, suggesting that the sickest patientsbenefit the most from this treatment (4,10). The second trial, undertaken inBrazil by Katz et al. in 105 patients, likewise is seriously flawed because ofinclusion of HELLP syndrome patients who were not class 1 or class 2, alack of stratification of case outcome into classes of disease so that class 1disease response to therapy could be evaluated, delay of drug initiation untilpostpartum after most disease morbidity is already established, smallpatient numbers, and inclusion of patients in the control group that hadrecently received corticosteroids for fetal lung maturation purposes (11).Moreover, their complication rates for transfusion, renal failure, and mater-nal death in both treatment and placebo groups were substantially higherthan those witnessed in the present or prior series reported from our mater-nal–fetal unit. In the absence of a single, very large, well-constructed multi-center prospective blinded and placebo-controlled clinical trial undertaken
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

Mississippi Protocol Management of HELLP Syndrome 87
in the United States with CONSORT guidelines and a professional externaltrial monitoring group to assure compliance and accuracy, debate about theclinical value of this third component to care of the patient with HELLP syn-drome will continue and divide the subspecialty of maternal–fetal medicineinto the users and nonusers of this treatment modality (12). Clearly, the con-clusion stated by the authors of these two trials that intravenous dexam-ethasone offers no benefit to patients with HELLP syndrome is invalidatedby weak data.
The principle of limiting HELLP syndrome progression with the MP is animportant concept to emphasize. A strength of the Mississippi classification ofHELLP syndrome is its assignment of patients into three classes of progres-sively worsening disease from class 3 (mild) to class 1 (most severe) (4). Use ofthis classification allows the clinician to better appreciate the magnitude ofillness and the peril to a particular patient, analogous to systems in place tostratify disease severity for patients with diabetes mellitus or hypertension.In addition, it allows the clinician and the investigator to better appreciate theimpact of any therapeutic intervention(s) upon the course and progression ofdisease. Following initiation of MP, only 18.2% of patients who developedclass 1 HELLP syndrome had evidence of new major maternal morbidity, com-pared with 33.3% present on admission. Similarly, the numbers were 2.4%versus 9.7% for patients in class 2. A substantial number of patients did notprogress beyond class 2 HELLP to class 1, likely in part because of Protocolmanagement. The highest maternal morbidity, particularly in the cardiopul-monary system, occurs in patients with class 1 HELLP syndrome (2,4). Hence,arrest of disease progression to prevent the development of class 1 HELLPsyndrome is a major therapeutic goal of treating any patient with HELLP syn-drome. Early initiation of intravenous dexamethasone, especially when usedin association with the other components of MP, provides the clinician with atool to interdict HELLP syndrome disease progression until removal of theplacenta and associated pregnancy decidua from the mother through timelydelivery can be accomplished.
As emphasized recently by Vigil-deGracia, “developing HELLP syndromeplaces any woman at significant risk of mortality” (13). In both of the majorpublished reviews on maternal mortality related to HELLP syndrome (13,14),maternal death had major contributing factors of cerebral hemorrhage andother serious multisystem disease developing typically in clinical circum-stances of delayed diagnosis of HELLP syndrome, absence of early intrave-nous dexamethasone initiation, and absence of successful prevention of severeelevations of blood pressure (systolic, diastolic, mean arterial). Central ner-vous system hemorrhage is the single most common cause of maternal deathin patients with HELLP syndrome pregnancies. As demonstrated recently in28 patients with stroke and severe preeclampsia/eclampsia, the prevention ofsevere systolic hypertension is likely very important to the possible preven-tion of these deaths and residual disabilities (6). The absence of maternaldeath in the present 8-year, 190-patient series stands in stark contrast to thefive largest, most recent published series of patients with HELLP syndromesince 2005 in which there were 21 maternal deaths among 215 patientstreated by other protocols of management (15–19).
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

88 Martin et al.
Importantly, excluded from this study were patients that exhibited laboratorycriteria of a HELLP-like syndrome that developed secondary to a variety of othermedical [TTP, DIC, prolonged hypoxemia/hypotension with unsuccessful intuba-tion for general anesthesia, systemic lupus erythematosus (SLE)/scleroderma,sickle cell crisis with complications] and obstetrical (catastrophic placentalabruption with fetal demise and renal insult, acute fatty liver of pregnancy) com-plications apart from severe preeclampsia/eclampsia. Between 1994 and 2008 wetreated 11 patients as described. In each instance, plasma exchange therapy dur-ing the postpartum period was initiated to facilitate maternal recovery and inmost cases (8/11) the mother survived (20). Another patient excluded from thisinvestigation was reported in 2006 to have either HELLP syndrome or TTP mas-querading as HELLP syndrome (8). Because the ADAMTS13 activity level <5%was not drawn until postmortem, it is now known to be invalid for differentialdiagnosis; the patient suffered a cardiopulmonary arrest and sudden renal dete-rioration before plasma exchange could be initiated.
It is conceptually erroneous to assume that almost all serious maternalmorbidity with HELLP syndrome does not develop until the motherprogresses through class 3 and class 2 to the stage of class 1 HELLP syndrome(4). It appears that both hepatic and renal morbidity are initiated well inadvance of the mother evidencing severe thrombocytopenia and other criteriafor class 1 or class 2 HELLP syndrome – it is instead more likely that thesecomplications arise subsequent to adverse action on tissue by pathogenic fac-tors released from the placenta, which subsequently produce the laboratoryand clinical information we require presently to make the diagnosis (21). Thisseries is again illustrative of this inasmuch as the only patient to reveal evi-dence of a liver hematoma did so while her platelet count was >100,000/μL; itis possible that initiation of the corticosteroid component of MP was instru-mental in stabilizing hepatic tissue deterioration and preventing progressionof the hematoma to the stage of rupture. Given the large number of casereports of hepatic rupture with HELLP syndrome in the absence of earlyintravenous dexamethasone initiation that have appeared in the recentobstetric literature (more than 20 reports in the last 5 years) and the recentpublication of two case series of liver transplantation for patients withHELLP syndrome (22,23), the avoidance of liver rupture in the present seriesof 200 patients is very significant.
Perinatal outcome with HELLP syndrome remains very problematicbecause many patients present with disease requiring delivery prior to a ges-tational age that is highly likely to produce intact perinatal survival.Although utilization of MP appears to greatly benefit the mother and lessenher morbidity and mortality risks, a perinatal benefit is less likely to beclearly achieved as long as delivery cannot be safely postponed for a pro-tracted period of time to attain greater fetal maturation. The next majormilestone in the improvement of HELLP syndrome pregnancy managementawaits the availability of therapeutic agents to prevent the development ofHELLP syndrome altogether or, failing that, significant postponement ofdisease onset until well into the third trimester.
The authors recognize the limitations of this prospective observational studywhich combines three-component management pieces into one protocol. The
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

Mississippi Protocol Management of HELLP Syndrome 89
intravenous dexamethasone protocol used was empiric and might have producedbetter results if higher doses had been used in the most severe cases as advo-cated by others (24). Better results in our series compared with others could bedue to years of provider education to referring physicians in Mississippi thatresulted in earlier referrals of patients and earlier treatment initiation of MP.
Declaration of InterestThe authors report no conflicts of interest. The authors alone are responsiblefor the content and writing of the paper.
REFERENCES1. Sibai BM, Ramadan MK, Usta I, et al. Maternal morbidity and mortality in 442 pregnancies
with hemolysis, elevated liver enzymes, and low platelets (HELLP syndrome). Am J ObstetGynecol 1993; 169:1000–1006.
2. Martin JN Jr, Rinehart BK, May WL, et al. The spectrum of severe preeclampsia: Compara-tive analysis by HELLP (hemolysis, elevated liver enzyme levels, and low platelet count)syndrome classification. Am J Obstet Gynecol 1999; 180:1373–1384.
3. Sibai BM. Diagnosis, controversies, and management of the syndrome of hemolysis, elevatedliver enzymes, and low platelet count. Obstet Gynecol 2004; 103:981–991.
4. Martin JN Jr, Rose CH, Briery CM. Understanding and managing HELLP syndrome: Theintegral role of aggressive glucocorticoids for mother and child. Am J Obstet Gynecol 2006;195:914–934.
5. Altman D, Carroli G, Duley L, et al. Magpie Trial Collaboration Group. Do women withpre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: Arandomized placebo-controlled trial. Lancet 2002 Jun 1; 359(9321):1877–1890.
6. Martin JN Jr, Thigpen BD, Moore RC, et al. Stroke and severe preeclampsia and eclampsia:A paradigm shift focusing on systolic blood pressure. Obstet Gynecol 2005; 105:246–254.
7. Martin JN Jr, Thigpen BD, Rose CH, et al. Maternal benefit of high-dose intravenouscorticosteroid therapy for HELLP syndrome. Am J Obstet Gynecol 2003; 189:830–834.
8. Rehberg JF, Briery CM, Hudson WT, Bofill JA, Martin JN Jr. Thrombotic thrombocytopenicpurpura masquerading as hemolysis, elevated liver enzymes, low platelets (HELLP) syn-drome in late pregnancy. Obstet Gynecol 2006; 108:817–820.
9. Fonseca JE, Mendez F, Catano C, Arias F. Dexamethasone treatment does not improve theoutcome of women with HELLP syndrome: A double blind, placebo-controlled, randomizedclinical trial. Am J Obstet Gynecol 2005; 193:1591–1598.
10. O’Brien JM. Dexamethasone, HELLP syndrome and study design. Am J Obstet Gynecol2006 Dec; 195(6):e13–e14.
11. Katz L, de Amorim MM, Figueiroa JN, Pinto e Silva JL. Postpartum dexamethasone forwomen with hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome:A double-blind, placebo-controlled, randomized clinical trial. Am J Obstet Gynecol 2008 Mar;198(3):283.e1–e8.
12. Norwitz ER, Bahtiyar MO, Sibai BM. Can postgraduate courses in maternal-fetal medicinechange clinical attitude? J Matern Fetal Neonatal Med 2005 Nov; 18(5):311–317.
13. Vigil-deGracia P. Maternal deaths due to eclampsia and HELLP syndrome. Int J GynecolObstet 2009; 104:90–94.
14. Isler CM, Rinehart BK, Terrone DA, et al. Maternal mortality associated with HELLP(hemolysis, elevated liver enzymes, and low platelets) syndrome. Am J Obstet Gynecol 1999;181(4):924–928.
15. Yucesoy G, Ozkan S, Bodur H, et al. Maternal and perinatal outcome in pregnancies compli-cated with hypertensive disorder of pregnancy: A seven year experience of a tertiary carecenter. Arch Gynecol Obstet 2005; 273:43–49.
16. Demir SC, Evruke C, Ozgunen FT, et al. Factors that influence morbidity and mortality insevere preeclampsia, eclampsia and hemolysis, elevated liver enzymes, and low plateletcount syndrome. Saudi Med J 2006; 27:1015–1018.
17. Osmanagaoglu MA, Osmanagaoglu S, Ulusoy H, Bozkaya H. Maternal outcome in HELLPsyndrome requiring intensive care management in a Turkish hospital. Sao Paulo Med J2006; 124:85–89.
18. Cavkaytar S, Ugurlu EN, Karaer A, Tapisiz OL, Danisman N. Are clinical symptoms morepredictive than laboratory parameters for adverse maternal outcome in HELLP syndrome?Acta Obstet Gynecol 2007; 86:648–651.
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.

90 Martin et al.
19. Gasem T, al Jama FE, Burshaid S, et al. Maternal and fetal outcome of pregnancy compli-cated by HELLP syndrome. J Mat Fet Neo Med 2009; 22:1140–1143.
20. Owens MY, Martin JN Jr, Keiser SD, et al. Postpartum multiorgan microangiopathicsyndrome (PMMS): A recognizable clinical scenario common to multiple uncommon diseasesrequiring plasma exchange to enable recovery. Am J Perinatology 2010 (submitted forpublication).
21. Venkatesha S, Toporsian M, Lam C, et al. Soluble endoglin contributes to the pathogenesisof preeclampsia. Nat Med 2006 Jun; 12(6):642–649.
22. Shames BD, Fernandez LA, Sollinger HW, et al. Liver transplantation for HELLP syndrome.Liver Transpl 2005 Feb; 11(2):224–228.
23. Zarrinpar A, Farmer DG, Ghobrial RM, et al. Liver transplantation for HELLP syndrome.Am Surg 2007 Oct; 73(10):1013–1016.
24. O’Brien JM, Milligan DA, Barton JR. Impact of high-dose corticosteroid therapy for patientswith HELLP (hemolysis, elevated liver enzymes, and low platelets) syndrome. Am J ObstetGynecol 2000; 183:921–924.
Hyp
erte
ns P
regn
ancy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yor
k U
nive
rsity
Lib
rari
es o
n 06
/30/
14Fo
r pe
rson
al u
se o
nly.